Diagnosis and Treatment of Systemic Juvenile Idiopathic Arthritis (sJIA) in Pediatric Age Groups
- Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing strategies for the transfusion of blood components in pediatric age groups into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of nutritional care delivery, care gaps and current needs.
3. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
4. Identify barriers to, and facilitators of implementation.
5. Select an implementation framework and its component strategies.
6. Develop a step-by-step implementation plan:
▪️ Select the target populations and evaluate the outcome.
▪️ Identify the local resources to support the implementation.
▪️ Set timelines.
▪️ Distribute the tasks to the members.
▪️ Evaluate the outcomes.
7. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
▪️ Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
▪️ Educational materials: printed or electronic information (software).
▪️ Web-based education: computer-based educational activities.
▪️ A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
▪️ Reminders: the provision of information verbally, on paper or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
▪️ Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
▪️ Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
▪️ Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
▪️ Reminders: the provision of information verbally, on paper or electronically to remind a patient/consumer to perform a particular health-related behavior.
▪️ Mass media campaigns.
3. For Nurses
▪️ Educational meetings: lectures, workshops or training courses, seminars, and symposia.
▪️ Educational materials: printed.
▪️ A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
▪️ Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
▪️ Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
▪️ Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
▪️ Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
▪️ Administrative policies and procedures.
▪️ Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
▪️ International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
▪️ Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
➡️Guideline Implementation Tools
Educational materials based on this Adapted CPG for treatment of CAP in children have been made available in several forms including algorithms, pathways, tables, and parents’ educational health guide (in Arabic).
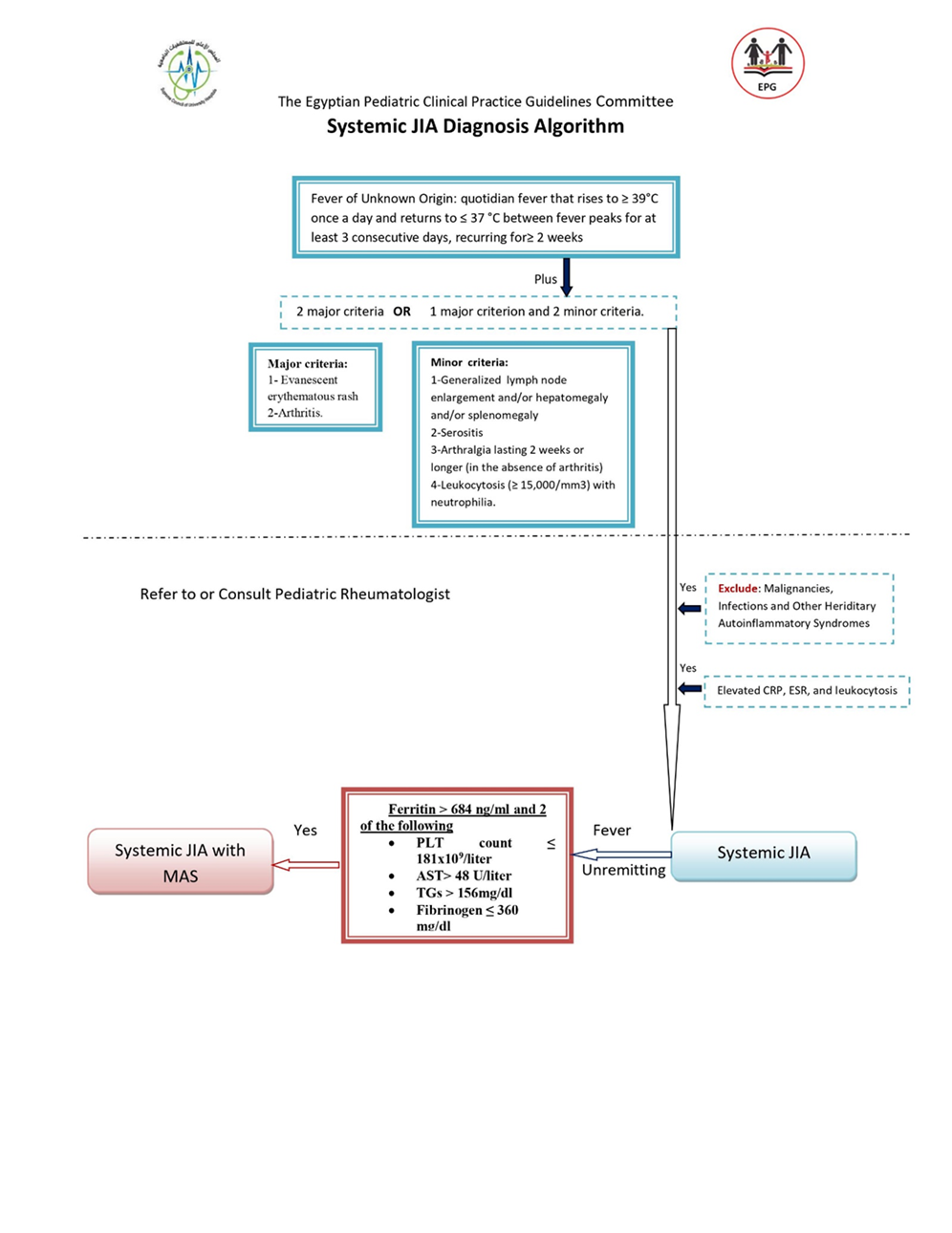
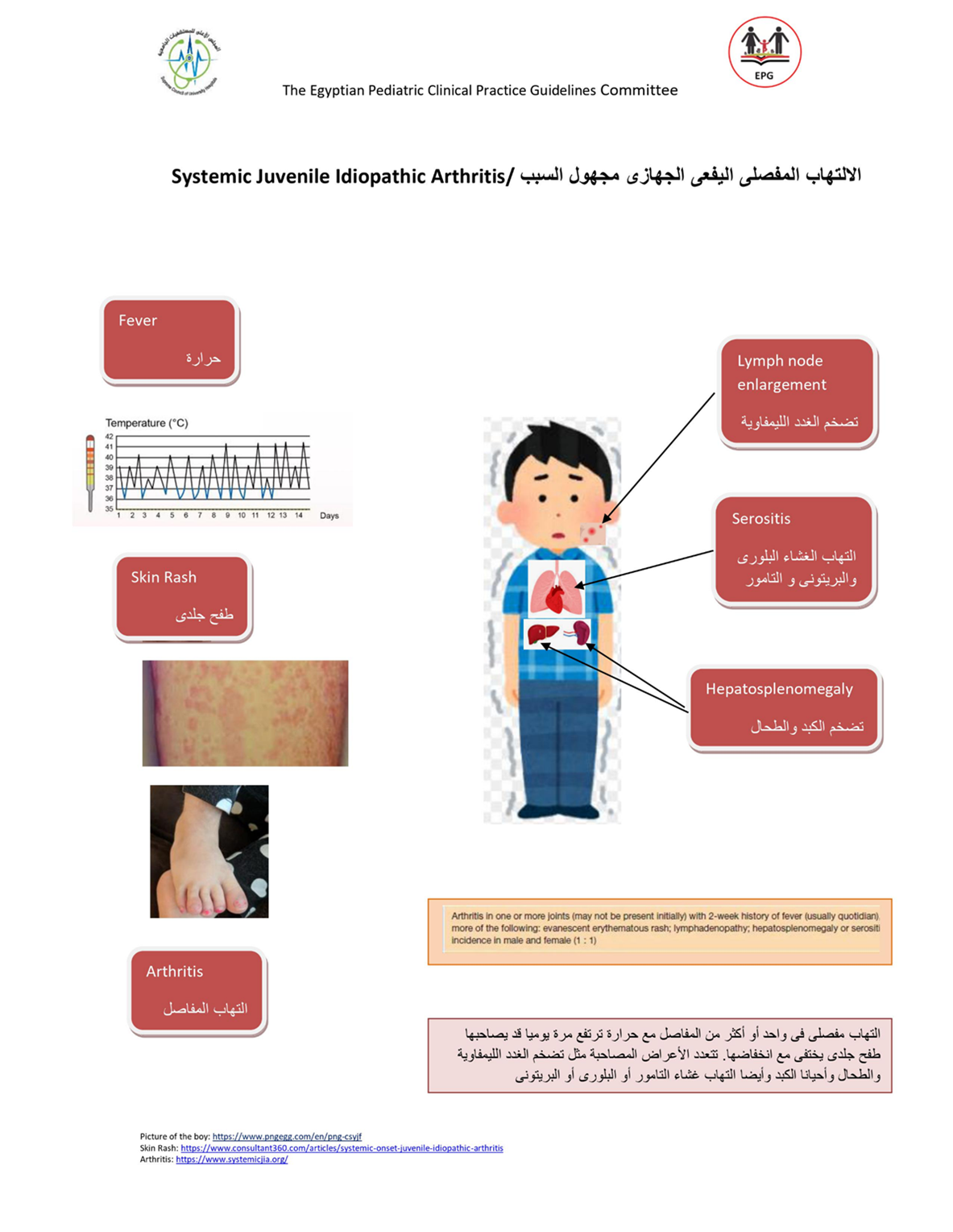
Table (7) : sJADAS10 composite score for assessment of sJIA activity
|
|
sJADAS 10 |
|
Physician global assessment |
0-10 VAS |
|
Parent/patient global assessment |
0-10 VAS |
|
Active joints count |
Simple 0-10 joints a |
|
Acute phase reactants (range) |
Normalized ESR b or CRP (0-10) c |
|
Modified systemic manifestations score (range) |
0-10 |
|
Total score range |
0-50 |
a : Up to 10 joints, irrespective of their type, censored at 10. b: According to the formula: (value in mm/h – 20)/10, where values 120 mm/h are converted to 120. c :According to the formula (value in mg/l – 10)/10, where values 110 mg/l are converted to 110. sJADAS 10: systemic Juvenile Arthritis Disease Activity Score in 10 joints (Adapted from Tibaldi et al., 2020)
d: Modified systemic manifestations score:
|
Clinical or laboratory feature |
Points |
|
Fever * 37.5–38⁰C >38–39⁰C >39–40⁰C >40⁰C |
1 2 3 4 |
|
Evanescent erythematous rash |
1 |
|
Generalized lymphadenopathy (enlargement of >3 lymph node stations) |
1 |
|
Hepatomegaly and/or splenomegaly |
1 |
|
Serositis (pleuritis, pericarditis or peritonitis) |
1 |
|
Anaemia (haemoglobin <9 gm/dl) |
1 |
|
Platelet count >600 109 /L or ferritin >500 ng/ml |
1 |
*:Fever is defined as the maximum temperature either in the past 24 h, 3 days or week. In the assessment of fever, the possible pharmacologic suppression of temperature by paracetamol, NSAIDs or glucocorticoids should be taken into
account. 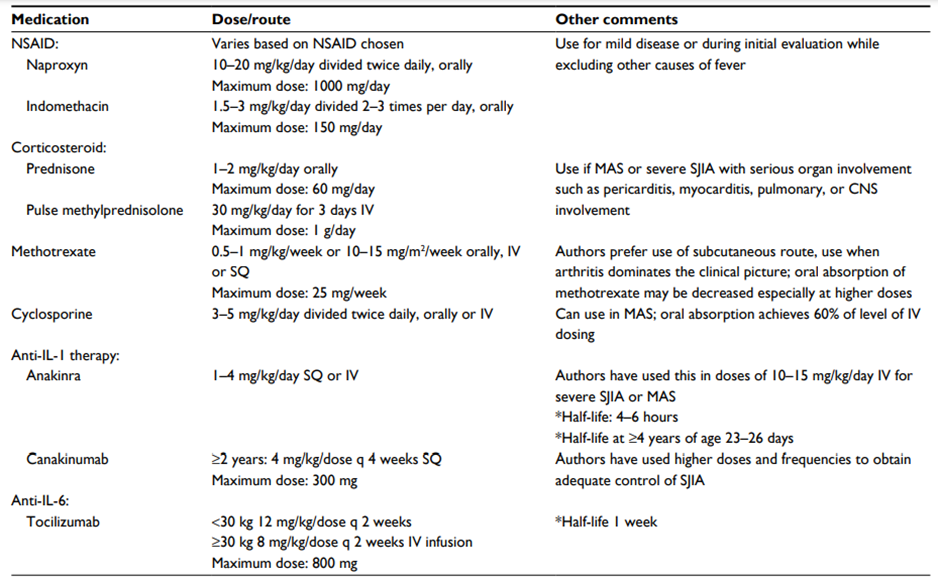
Table (8) Therapeutic agents commonly used for sJIA treatment
Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; SQ, subcutaneous; IV, intravenous; CNS, central nervous system; MAS, macrophage activation syndrome; q, every; sJIA, systemic juvenile idiopathic arthritis. Shenoi S, Wallace CA, 2016 (46)
➡️Parent and carer health educational guide (in Arabic)
الالتهاب المفصلي اليفعي الجهازي مجهول السبب
الالتهاب المفصلي اليفعي الجهازي مجهول السببsJIA يعد نوع مميز من أنواع الالتهاب المفصلي اليفعي مجهول السبب JIA,يتميزبوجود بعض الأعراض الأكلينيكية التى تميزه عن باقي الأنواع وكذلك المضاعفات وطرق التشخيص والخيارات العلاجية الخاصه به , و يمثل هذا النوع حوالي 10 ٪ إلى 20 ٪ من مجمل حالات JIA ، مع معدلات إصابة تتراوح من 0.4 إلى 0.8 طفل لكل 100.000 طفل.
يمكن أن تظهرأعراضsJIA في أي وقت خلال الطفولة والمراهقة ، مع ذروة الإصابة عند عمر سنتين,يصاب به الأولاد والبنات على حد سواء, يحدث عند الأطفال من جميع الخلفيات العرقية ، مع معدل انتشار أعلى في الجنوب الشرقي واليابان.
▪️معايير التصنيف الالتهاب المفاصل البفعي مجهول السبب وفقا لرابطة الجمعيات الدولية للروماتيزم:
يتطلب تشخيص sJIA وجود التهابات في واحد من المفاصل أو أكثر، مع أو قد يسبقها ظهور حمى مستمرة لمدة أسبوعين على الأقل ، تحدث بشكل يومي (على الأقل3 أيام يومية) ، ويرافقها واحد أو أكثر من هذه الاعراض:الطفح الجلدي أحمر غير ثابت في مكانه , تضخم العقد اللمفاوية المنتشرة في الجسم, تضخم الكبد أو الطحال, التهاب في الاغشية المصلية. ولتشخيص الحالة انها sJIA فيجب استبعاد وجود :
- مرض الصدفية أواي تاريخ مرضي للاصابه بها لدى المريض أو أقاربه من الدرجة الأولى.
- ان تكون التهابات المفاصل في طفل ذكر عمره اكتر من ست سنوات ولديه HLA-B27ايجابي.
- مرض التيبس الفقاري المناعي ، التهاب المفاصل المرتبط بالتهاب ألأوتار ERA ، الالتهاب المفصلي العجزي الحرقفي المصاحب لالتهابات القولون المناعية ، التهاب القزحي الأمامي الحاد ، أو تاريخ أحد هذه الأمراض لدى المريض او أحد أقاربه من الدرجة الأولى.
- تحليل عامل الروماتويدي RF موجب مرتين يفصل بينهما ثلاثة أشهر علي الاقل.
▪️الاعراض الاكلينيكية:
§ حمى يومية ترتفع فيها الحرارة الي39-40 درجة مئوية مرة أو مرتين في اليوم ثم تنخفض سريعا إلى الطبيعي.
§ طفح جلدي بقعي أو لطاخي متحرك من مكان لمكان (غير ثابت)، غير مسبب للحكة، يظهر في الجذع والرقبة والجزء من الأطراف القريب من الجذع ,ومن المميز له ظهوره مع نوبات الحمى وتلاشيه عند زوال الحمى.
§ التهابات المفاصل تكون في أربع مفاصل أو أقل أو فد تكون متعددة الي أكثر من خمس مفاصل و المفاصل الأكثر التهابا (المعصمين, الركبتين, والكاحلين). ظهور التهاب المفاصل عادة يكون في خلال الأشهر الثلاثة الاولي من ظهور المرض، إلا أنه قد يتأخر في الظهور لأسابيع اوأشهرأو نادرًا الي سنوات.
§ تضخم العقد اللمفاوية المنتشرة في الجسم ويكون التضخم واضح مما يثير الشكوك من انه ورم خبيث.
§ تضخم الكبد والطحال.
§ التهاب في الأغشية المصلية والذي يكون عادة بدون أعراض ويمكن اكتشافه فقط بمخطط صدى القلب أو تصوير شعاعي للصدر.
▪️التشخيص
لا توجد تحاليل محددة لـتشخيص مرضsJIA)). التحاليل المعملية تعد داعمة للتشخيص وتعكس الطبيعة الألتهابية للمرض ولاستبعاد الحالات التي تسبب أعراض مماثلة.صورة الدم قد تشير الي وجود زيادة في عدد كريات الدم البيضاء والصفائح الدموية وانيميا فقر الدم,ويلاحظ وجود ارتفاع في معاملات الألتهاب مثل معدل ترسيب كرات الدم الحمراء (ESR) ، بروتين سي التفاعلي (CRP) ونسبة الفيرتين بالدم. اما الأجسام المضادة الذاتية مثل الأجسام المضادة الذاتية المضادة للنواة (ANA) والعامل الروماتويدي (RF) فتكون دائمًا سلبيًة ولا تفيد في التشخيص(لوحظ وجود ANA إيجابي في حوالي 4٪ إلى 6٪ من مرضى sJIA)).قد نحتاج الي نضح وخزعة نخاع العظام لاستبعاد الأورام الخبيثة في الدم.
الفحص الإشعاعي قد يبين تورم الأنسجة الرخوة وهشاشة في العظام.فقدان الغضاريف وتاكل العظام عادا ما يظهر في غضون عامين من ظهور المرض.
▪️المضاعفات
متلازمة تنشيط البلاعم MAS هي أحد مضاعفات التي تهدد حياةالأطفال المصابين بـ sJIA.حيث يعاني المريض من حمى شديدة غير مستجيبة وتدهور للحالة العامة للمريض, مع تضخم بالكبد والطحال، وخلل عصبي، ومظاهر نزفية, وفشل متعدد في وظائف أعضاء الجسم.تظهر التحاليل المعملية انخفاض بكريات الدم , وارتفاع في وظائف الكبد ونازعة هيدروجين اللاكتات والدهون الثلاثية والفيرتين بالدم ، مع انخفاض مستويات الفيبرينوجين وانخفاض نسبة سرعة الترسيب ESR بعد أن كانت مرتفعة سابقا ، مع استمرار ارتفاع البروتين التفاعلي CRP. قد نحتاج الي نضح وخزعة نخاع العظام للتأكد من تشخيص MAS.
التهاب المفاصل التآكلي المبكر من المضاعفات المتكررة في حالات المصابين بsJIA وتؤثر عادة علي الركبتين والكاحلين والرسغين. كذلك هشاشة العظام وتأخر النمو من المضاعفات المحتملة الي جانب المضاعفات الناتجة عن تناول الأدوية مثل عقار الكورتيزون لفترات طويلة والادوية المثبطة لجهازللمناعة والتى تزيد نسبة الإصابة بالعدوي والأورام الخبيثة.
المرضي المصابين ب sJIA لديهم احتمال أكبر لحدوث عجز وظيفي متوسط و شديد مقارنة بالأنواع الاخرى من JIA و قد يعزى هذا إلى عدد المفاصل واجهزة الجسم المتأثرة بالاصابة.
▪️العلاج
الهدف من العلاج هو السيطرة على الألتهاب النشط من أجل تخفيف الأعراض والوقاية من المضاعفات المرتبطة بالمرض.نظرًا لطبيعة مرض sJIA وتأثيره علي العديد من أجهزة الجسم، يجب أن تركز بروتوكولات العلاج على الطفل ككل وليس على جانب واحد فقط من المرض.يشمل العلاج الناجح كلا من التدخل الدوائي وغير الدوائي بما في ذلك التغذية العلاجية والعلاج الطبيعي والدعم النفسي والأجتماعي للمريض.
في البداية ، تستخدم مضادات الألتهاب غير الستيرويدية والكورتيزون للسيطرة على المرض, ولكن بسبب الآثار الجانبية غير المرغوب فيها والمرتبطة باستخدام هذه الأدوية فتهدف البروتوكولات الحديثة في العلاج إلى التقليل التدريجي أو التوقف التام عن استخدام هذه الأدوية بعد ان يتم إجراء التشخيص الدقيق للمرض.
تم استخدام العلاج البيولوجى مثل مثبطات TNF بشكل متكرر، ولكنها أظهرت فعالية منخفضة مقارنة بنتائجها في المرضى المصابين بالأنواع الأخرى من .JIAاما العلاجات المضادة لـ IL-1 و IL-6 اثبتت فعالية كبيرة في مرضي sJIA وكلما كان العلاج بهذه العقاقير مبكرا كلما اعطي فرصة افضل لتحسين النتايج.
الحالات المصابة ب MASتحتاج لجرعات كبيرة من الكورتيزون عن طريق الوريد اولا (ميثيل بريدنيزولون لمدة ثلاثة أيام متتالية) متبوعًا بالكورتيزون عن طريق الفم و يستخدم عقارالسيكلوسبورين وهو مثبط الكالسينيورين كعلاج ثانوي وكذلك العلاجات البيولوجية وخاصة مضادIL-1((Anakinraالذي يستخدم بنجاح في علاج كل من MAS و sJIA النشط ويعد مفيدًا في تحقيق التخفيض السريع لجرعة الكورتيزون.