Diagnosis, Management and Prevention of Acute Hemolytic Anemia in Infants, Children and Adolescents
- Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing AHA diagnosis, management, and prevention strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of health care delivery, care gaps and current needs.
3. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, management and prevention and adapt them to the local context or environment.
4. Identify barriers to, and facilitators of implementation.
5. Select an implementation framework and its component strategies.
6. Develop a step-by-step implementation plan:
▪️ Select the target populations and evaluate the outcome.
▪️ Identify the local resources to support the implementation.
▪️ Set timelines.
▪️ Distribute the tasks to the members.
▪️ Evaluate the outcomes.
7. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
▪️ Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
▪️ Educational materials: printed or electronic information (software).
▪️ Web-based education: computer-based educational activities.
▪️ A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
▪️ Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
▪️ Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
▪️ Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
▪️ Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
▪️ Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behavior.
▪️ Mass media campaigns.
3. For Nurses
▪️ Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
▪️ Educational materials: printed.
▪️ A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
▪️ Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
▪️ Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
▪️ Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
▪️ Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
▪️ Administrative policies and procedures.
▪️ Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
▪️ International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
▪️ Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
➡️Guideline Implementation Tools
Educational materials based on this Adapted CPG for treatment of AHA in children have been made available in several forms including:
1. Manual for physician for diagnosis and algorithm for management of acute hemolytic anemia
3. Arabic Educational materials for nurses and mothers
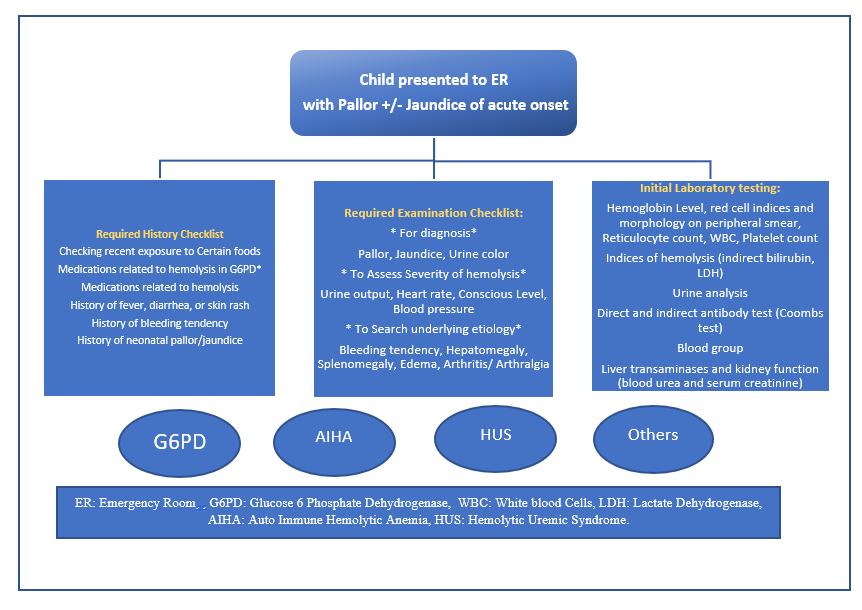
Figure 1. Diagnostic Approach to the child Presenting to the ER with acute Pallor +/- Jaundice
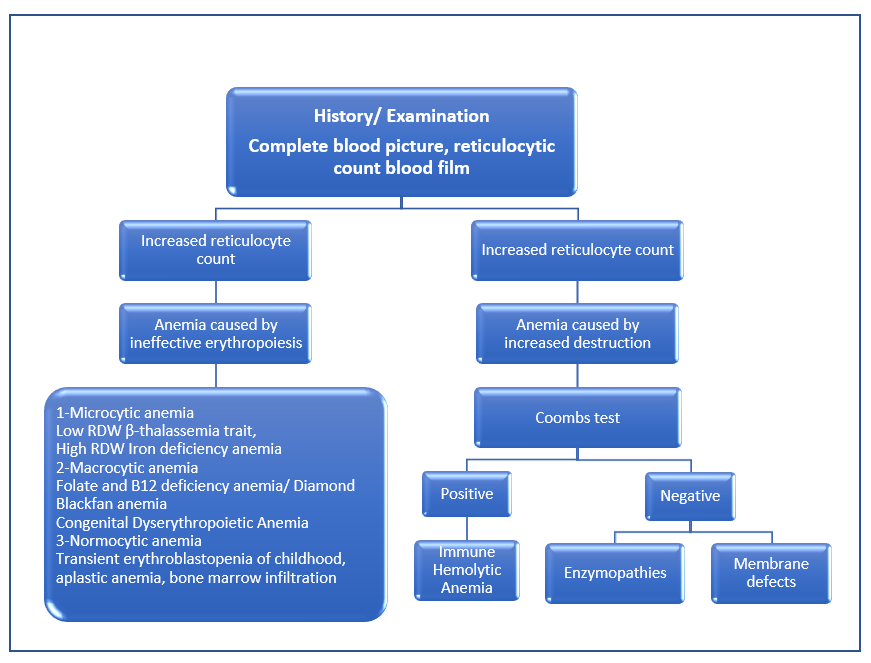
Figure 2. Diagnostic Approach to Child with Acute Pallor +/- Jaundice According to Reticulocyte count
Table 3: Health Questions used to develop this Adapted Clinical Practice Guideline:
|
Diagnosis |
History and clinical examination: (see figure 1 & 2) Laboratory diagnosis: 1.What is the initial laboratory panel for infants, children and adolescents presenting with AHA? 2.What is the best timing and test to diagnose G6PD deficiency in infants, children and adolescents presenting with AHA? 3.What are the indications of G6PD testing? 4.What is the best test to diagnose AIHA in infants, children and adolescents presenting with AHA? 5.What are the additional immunological tests before starting treatment in patients with AIHA? 6.What is the initial laboratory panel for patients with suspected post diarrheal hemolytic uremic syndrome? |
|
Management |
Emergency management: 1.What is the emergency treatment for infants, children and adolescents presenting with AHA? 2.When is Packed red cells indicated? Sub-question: volume/ precautions needed? Medical Pharmacological treatment: 3.What is the medical treatment in infants, children, and adolescents with AIHA? What are the criteria of adequate /good response to treatment in infants, children, and adolescents with AIHA? Monitoring and Follow-up 4.For follow up after discharge, what are the laboratory tests needed in patients with G6PD and AIHA? |
|
Prevention |
1.What are the drugs to be avoided and the dietary modifications required to prevent the occurrence of AHA in patients with G6PD deficiency? 2.For prevention of HUS, when is empiric antibacterial treatment indicated for children with bloody diarrhea? |
Table 4. Differential Diagnosis of AIHA19:
|
Congenital forms |
Spherocytosis and other defects of the erythrocyte membrane proteins; erythrocyte enzyme deficiency; - dyserythropoietic anemia; - haemoglobinopathies; Wilson's disease. |
|
Hemolytic anemia from mechanical causes |
Synthetic heart valves; march hemoglobinuria; cardiopulmonary bypass. |
|
Hemolytic anemia due to vascular injury |
Microangiopathic anemia; thrombotic thrombocytopenic purpura; hemolytic-uremic syndrome; disseminated intravascular coagulation; arterio-venous malformations. |
|
Hemolytic anemia due to thermal damage |
Extensive burns. |
|
Hemolytic anemia from chemical causes |
Chemicals: solvents; methyl chloride; lead; arsenic and hydrogen; snake venom. |
|
Hemolytic anemia due to infectious agents |
Bacteria (Mycoplasma pneumoniae, Clostridium welchii); viruses (cytomegalovirus, herpes virus); protozoa (Plasmodium spp.). |
Table 5: Common drugs that patients with G6PD deficiency should avoid or use with caution23, 24:
|
Generic name |
Risk level |
Generic name |
Risk level |
|
Acetaminophen |
Low |
Moxifloxacin |
High |
|
Acetylsalicylic acid |
Variable* |
Naphthalen |
High |
|
Ascorbic acid (Vitamin C) |
High with high dose |
Nitric oxide |
High |
|
Chloramphenicol |
High |
Nitrofurantoin |
High |
|
Ciprofloxacin |
High |
Nitroglycerin |
High |
|
Colchicine |
Low |
Phenazopyridine (pyridium) |
High |
|
Dapsone |
High |
Primaquine |
High** |
|
Diphenhydramine |
Low |
Probenecid |
High |
|
Glimepiride |
High |
Rasburicase |
High*** |
|
Glipizide |
High |
Sodium nitroprusside |
High |
|
Glyburide |
Use with caution |
Streptomycin |
Low |
|
Hydroxychloroquine |
High |
Sulfacetamide |
High |
|
Isoniazid |
Low |
Sulfamethoxazole |
High**** |
|
Levofloxacin |
High |
Trimethoprim |
Low**** |
|
Methylene blue |
High |
Vitamin K |
Low to high† |
* Risk level low to none, use with caution
** Reduce dose with medical therapy if required
*** Prescribing modification required
**** Also, when in combination with the other drug
† High with vitamin K3 (menadione), low with vitamin K1 (phytomenadione)