THE DIAGNOSIS, TREATMENT, AND PREVENTION OF THROMBOSIS IN PAEDIATRIC AGE GROUPS
- Implementation strategies or interventions
1. Leadership commitment, engagement, and support.
2. Local clinical and quality champions.
3. Dissemination (printed and electronic).
4. Regular training and education.
5. Regular audit and feedback (along with regular review and update promotes the concept of the ‘living CPGs’.
6. Networking with relevant existing projects.
7. Parents or carers as champions for changes.
➡️Implementation tools
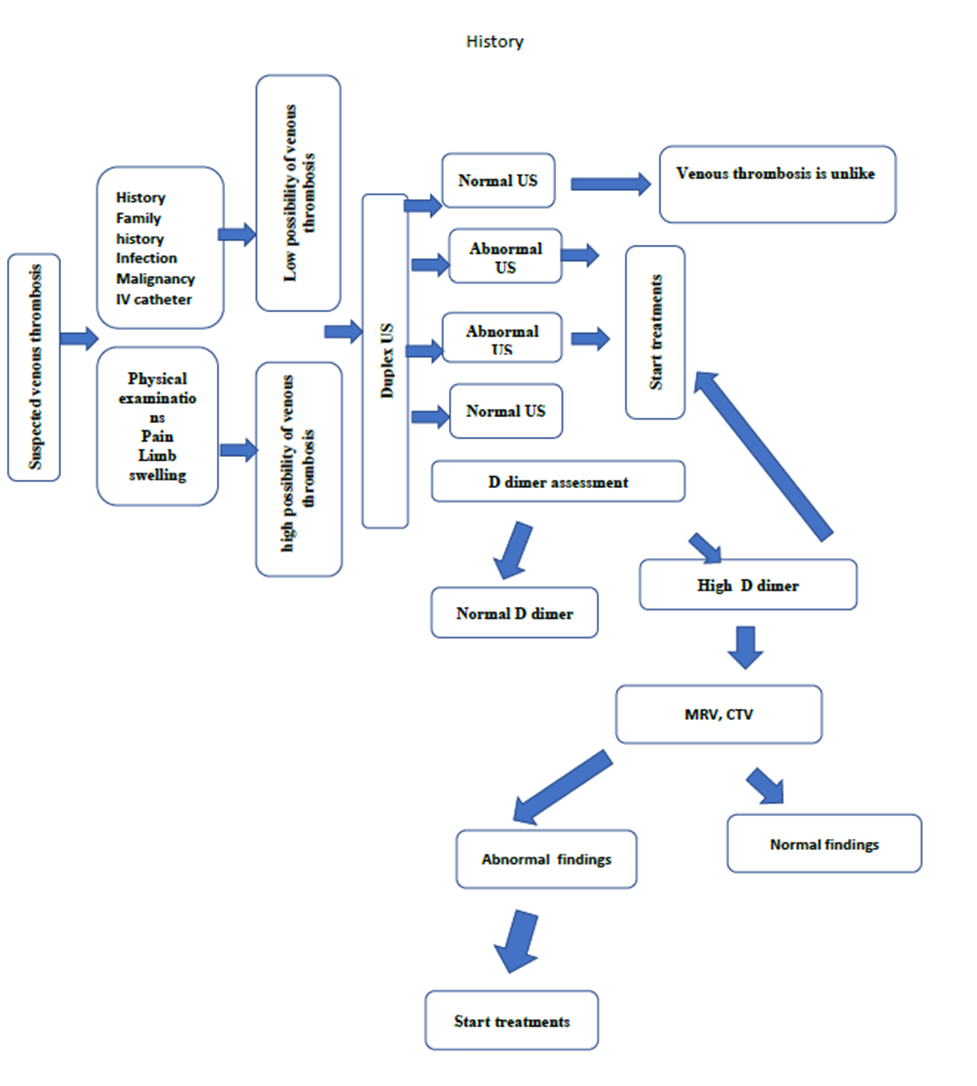
Figure1: Diagnostic
algorithm for Pediatric DVT
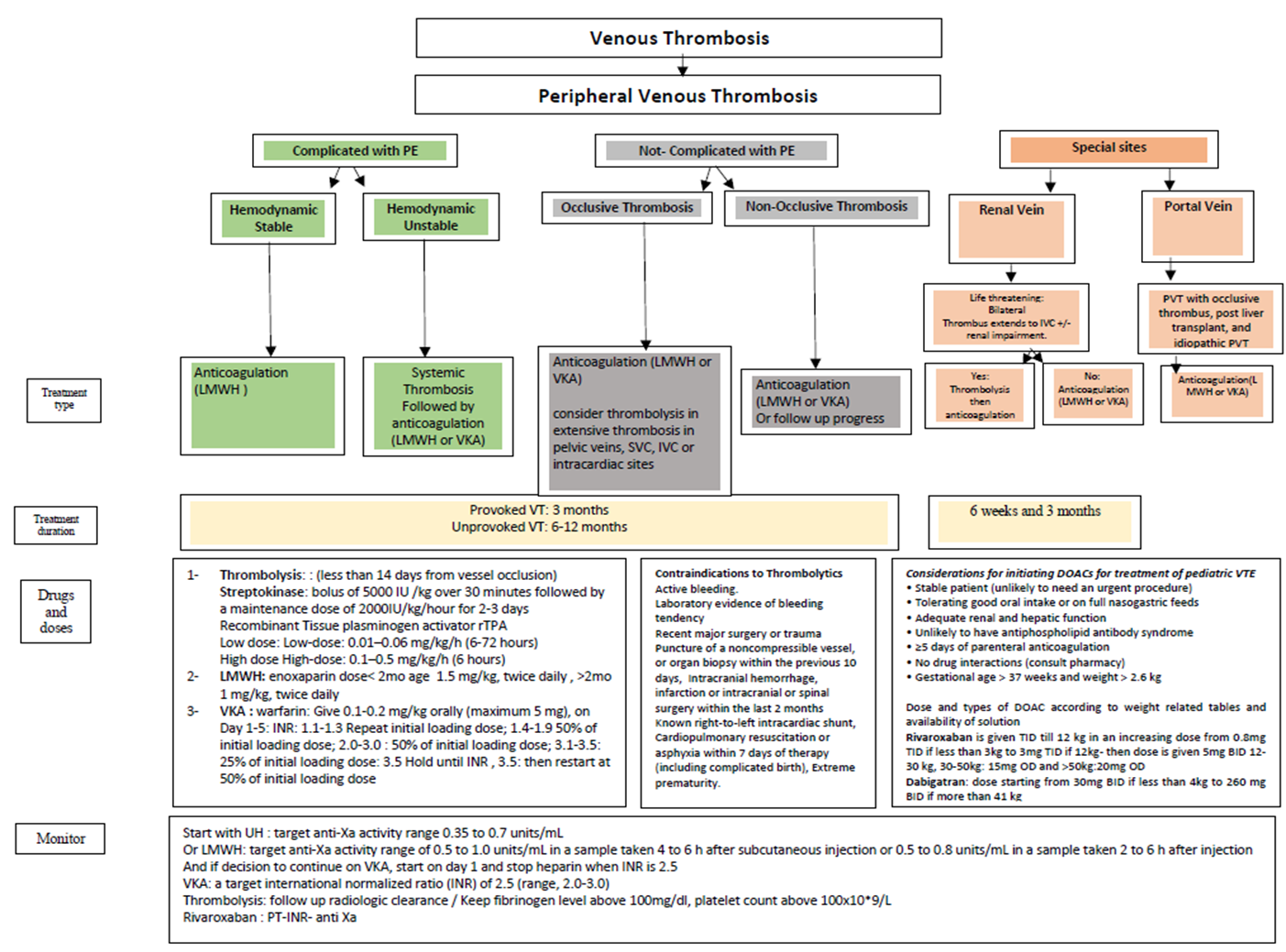
Figure 2: Algorithm
for management of venous thrombosis
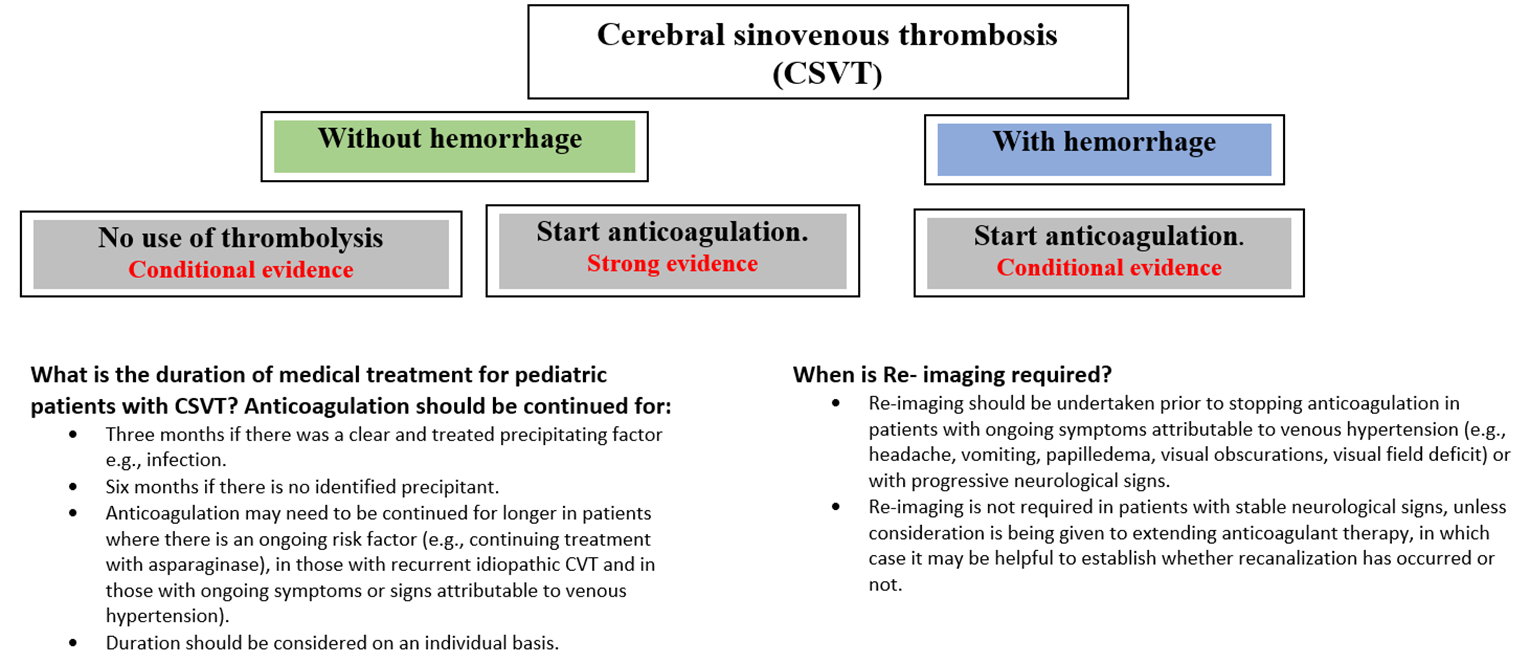
Figure 3: Management plan of cerebral sinovenous thrombosis
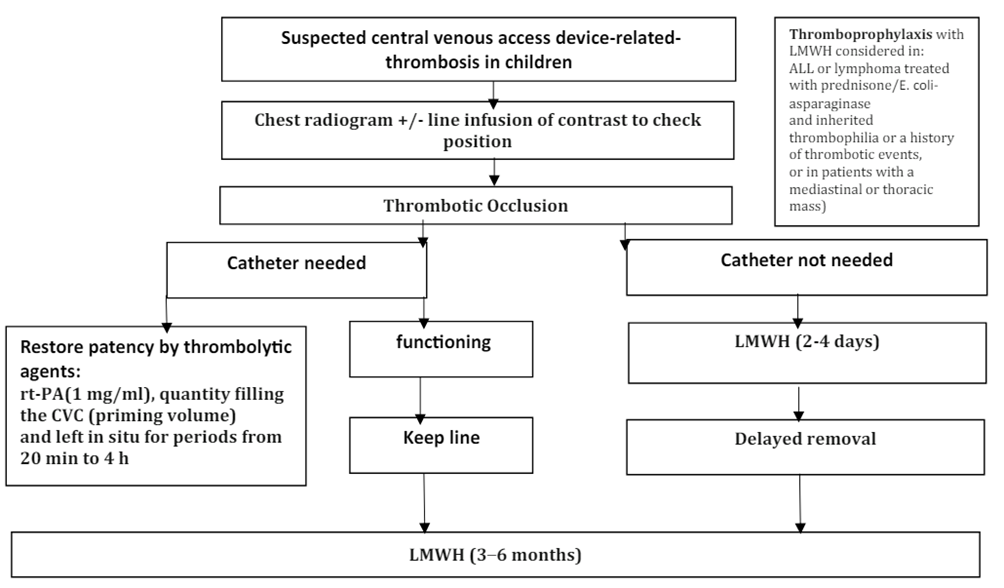
Figure 4: Pathway for management of acute CVAD-associated thrombosis in neonates and children.
|
Drug |
Route |
Dose |
Therapeutic monitoring |
|
UFH |
Continuous IV infusion |
Age < 12 mo: bolus 75 U/kg followed by 28 U/kg/h Age 1 to < 12 y: bolus 75 U/kg followed by 20 U/kg/h Age > 12 y: bolus 80 U/kg followed by 18 U/kg/h |
Target range: aPTT: 1.5-2.5 times control or Anti-Xa level 0.3-0.7 U/mL |
|
Enoxaparin (LMWH) |
Subcutaneous injection |
Age < 2 mo: 1.5-1.7 mg/kg q12 h Age > 2 mo: 1 mg/kg q12 h |
Target range: Anti-Xa 0.5-1.0 U/mL (Sample 3 to 4 h after third dose) |
|
Warfarin |
Oral |
Loading: 0.2 mg/kg x 1 (if INR < 1.3), max 10 mg Maintenance: adjust according to INR (Measure INR daily days 2 to 4) INR 1.1-1.3: repeat loading dose INR 1.4-1.9: 50% of loading dose INR 2.0-3.0: INR 3.1-3.5: 25% of loading dose INR >3.5: Hold until INR < 3.5, reinitiate at 50% of loading dose. |
Target range: INR 2.0 to 3.0 |
|
Rivaroxaban (DOAC) |
Oral |
According to weight 2.6 to < 3 kg:0.8 mg per dose TDS 3 to < 4 kg: 0.9 mg per dose TDS 4 to < 5 kg: 1.4 mg per dose TDS 5 to < 7 kg: 1.6 mg per dose TDS 7 to < 8 kg: 1.8 mg per dose TDS 8 to < 9 kg: 2.4 mg per dose TDS 9 to < 10 kg: 2.8 mg per dose TDS 10 to < 12 kg: 3 mg per dose TDS 12 to < 30 kg: 5 mg per dose BD 30 to < 50 kg: 15 mg OD ≥ 50 kg: 20 mg OD |
|
Table 2: Common anticoagulant therapies for use in pediatric VTE
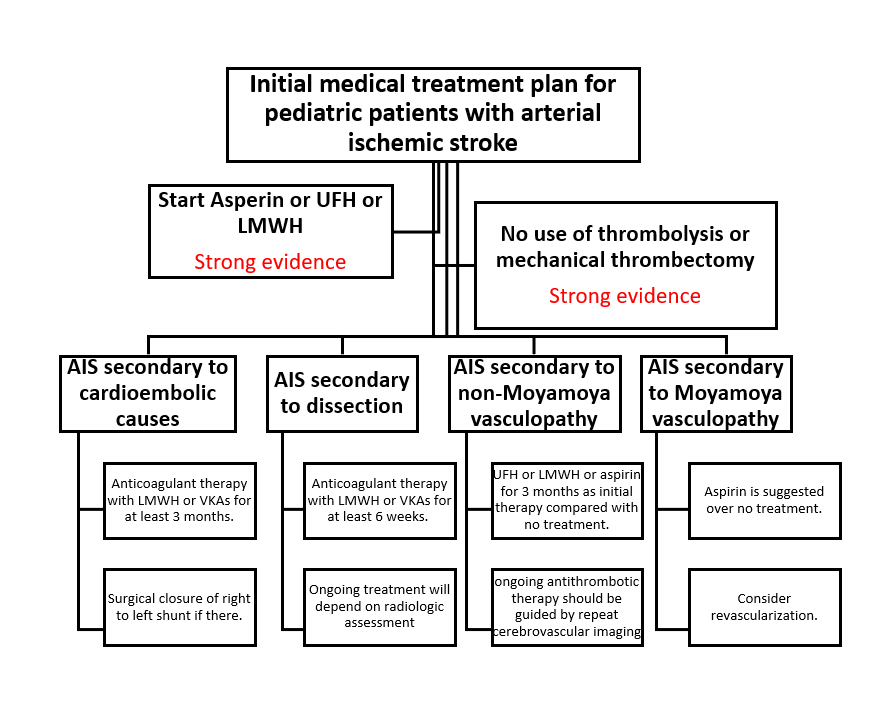
Figure 5: Management
plan of arterial ischemic stroke