Bronchial Asthma Management in Children
- Introduction
Asthma is a chronic inflammatory disease of the airways, characterized by recurrent episodes of wheeze, chest tightness, cough, and shortness of breath and airflow obstruction resulting from edema, bronchospasm, and increased mucus production. Commonly associated with seasonal allergies (allergic rhinitis) and eczema (atopic dermatitis), these three conditions form what is known as the atopic triad (1). There is a wide range in the frequency and severity of the symptoms, but uncontrolled asthma and acute exacerbations can lead to respiratory failure and death (2).
Poor asthma control has a significant impact on patients, their families, the healthcare system, and the community as a whole in terms of poor quality of life, frequent emergency department visits, hospitalizations, and deaths (3-5).
Asthma is a devastating global disease that affects people of all ages, with prevalence ranging from 1% to 21% in adults and up to 20% of children aged 6–7 years experiencing severe wheezing bouts within a year (6). The global prevalence of asthma ranges from 1% to 18% in different studies, with national prevalence estimates ranging from 1.7% to 53% in different countries and at different ages (7). The prevalence of asthma has increased dramatically in the last 20 years, indicating that environmental factors (allergens, infections, lifestyle, and food) play a significant role in the development of asthma (8). Bronchial asthma prevalence varies significantly by region, with industrialized countries having a higher frequency than developing countries (9).
Asthma is a leading cause of hospitalization in Egypt, and it is estimated that one out of every four children with asthma is unable to attend school on a regular basis due to poor asthma management (10).
The prevalence was 8.2 percent among Egyptian children aged 3 to 15 years. It was reported that asthma prevalence was 4.8% in Egyptian infants and children aged less than 4 years, from five governorates. Studies from Egypt reported that prevalence of asthma is 9.4% in 11– 15-year-old school in Cairo and 8.2% was reported in another study of children with age of 3–15 years (11).
➡️Pathophysiology of asthma:
Asthma is a chronic inflammatory airway disease that results in a narrow airway lumen. The airway narrowing is caused by smooth muscle contraction, bronchospasm, and increased mucus secretion as well as bronchial wall thickening due to edema, smooth muscle hypertrophy, and subepithelial fibrosis. The pathophysiological mechanisms that underlie these changes are diverse and heterogeneous. They are driven by a variety of cell types including immune cells; mainly T-helper cells (Th2, Th17, Th1), B-cells, mast cells, eosinophils, dendritic cells, and neutrophils; as well as structural bronchial cells such as epithelial cells, myofibroblasts, and smooth muscle cells (12). The mechanisms of asthma include the following: (figure 1) (13)
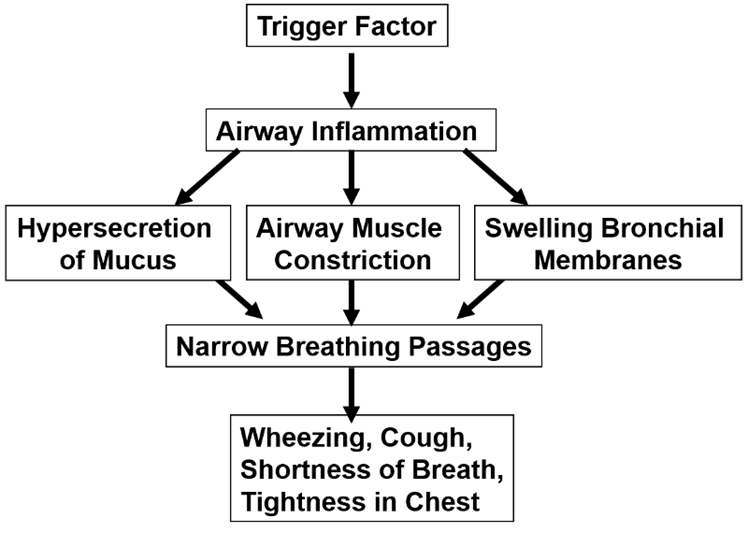
Figure 1: pathophysiology of asthma (Liu et al., 2021) (13).
Asthma Patterns in Childhood, Based on Natural History
1- Transient non atopic wheezing:
It is characterized by recurrent cough/wheeze that is primarily triggered by common respiratory viral infections and is most common in early preschool years. Usually resolves during the preschool and early school years, without increased risk for asthma in later life (14).
2- Persistent atopy-associated Asthma:
It starts in the early preschool years and is linked to atopy : either: Clinical (e.g., atopic dermatitis in childhood, allergic rhinitis, food allergy), or Biologic (e.g. elevated serum immunoglobulin E, increased blood eosinophils). Highest risk for persistence into later childhood and adulthood. Those who begin before the age of three have diminished airflow by the time they reach school age (15).
➡️Asthma with deteriorating lung function:
It is associated with hyperinflation in childhood and male gender. Children experience progressive airflow limitation (16).
➡️Asthma triggers:
Asthma attacks commonly occur following exposure to one or several triggers. Viral respiratory infections remain the leading cause, but there are a number of other known triggers, including aeroallergens, second hand smoke exposure, or changes in ambient air temperature or humidity. Identification and documentation of specific asthma triggers should be part of routine care. Education on trigger recognition and avoidance is essential (17)
➡️Risk factors of asthma:
There are a number of risk factors that should be explored in the history of children who present with features of asthma. In symptomatic children, a personal or family history of atopic features, including asthma, eczema or rhinitis, supports a diagnosis of asthma. Education on modifiable risk factors, for example, exposure to secondhand smoke or air pollution and obesity, should be delivered routinely during consultations and asthma reviews. A range of social determinants that are linked to poverty impact on outcomes and the health of children with asthma (18).
➡️Clinical Presentation of asthma:
Children with asthma typically present with a symptom triad of wheeze, shortness of breath and cough. However, ‘asthma’ is an umbrella term used to describe this collection of symptoms and, when present, should prompt practitioners to ask, ‘What type of asthma is this?’ There are a number of asthma subtypes that present and respond to treatment differently. Identification of the features of asthma and modifiable or treatable traits should only be the start of the diagnostic journey (19). Asthma symptoms are normally intermittent in nature and may not be present at the time of clinical review, making the diagnosis challenging in some cases (20). Additionally, disease phenotypes are not fixed and may evolve over time, necessitating ongoing review of symptoms and treatment. Wheeze is a key feature of asthma and, if not present, a diagnosis of asthma in a child is unlikely (21).
The prevalence of ‘preschool wheeze’ is an additional challenge when diagnosing asthma in young children. In the first few years of life, many children will experience wheeze, but not all will go on to develop true asthma. The diagnosis of asthma should therefore be reviewed routinely to identify true asthma and alter treatment where necessary (22). Favorable response to an appropriate trial of asthma treatment is an important confirmatory piece of diagnostic evidence. Clinical examination may be normal in children and adolescents with asthma if they present during asymptomatic periods. During acute attacks, use of accessory muscles of respiration and widespread wheeze may be present (23). Chest hyperinflation may be identified in acute and chronic disease settings.
Many of children with asthma develop symptoms before five years of age, but the disease is frequently misdiagnosed or not suspected particularly in infants and toddlers. Evaluating the presence of asthma symptoms is an important first step in establishing a proper diagnosis. (Figure 2) (24).
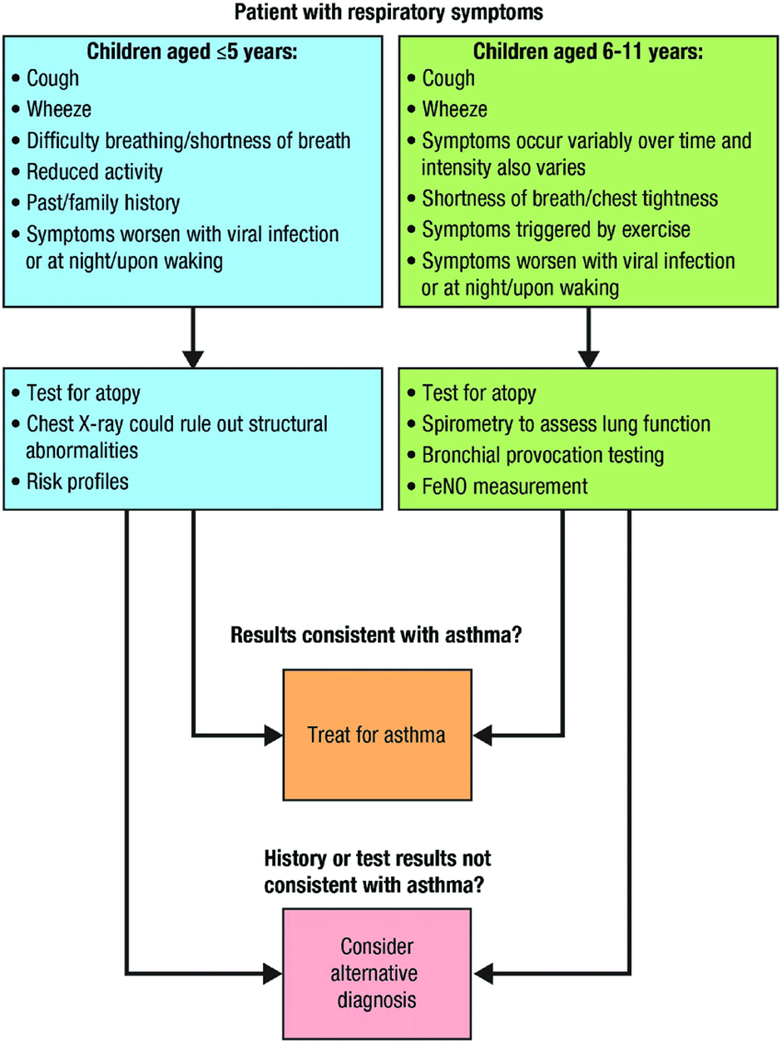
Figure 2: Diagnosis of asthma in children (Devani et al., 2022)(25)
➡️Asthma comorbidities:
Asthma is often associated with various comorbidities. The most frequently reported asthma comorbid conditions include:
I. Allergic rhinitis (26).
II. Sinusitis (27)
III. Gastroesophageal reflux disease (28).
IV. Allergic conjunctivitis (29).
V. Obesity (30).
VI. Obstructive sleep apnea (31).
VII. Eczema (31).
VIII. Food allergy (28).
➡️Differential diagnosis of asthma:
Table 1: Age-Related Differential Diagnosis for Wheezing (Kaplan et al., 2019) (32).

➡️Assessment of asthma control:
Treatment should be designed to ensure the asthma is well controlled, this means:
▪️ The patient doesn’t have symptoms on more than 2 days a week.
▪️ The patient doesn’t need his reliever medication on more than 2 days a week.
▪️ Asthma doesn’t limit what the patient can do.
▪️ The patient doesn’t have symptoms at night or on wakening up.
▪️ Achieving good asthma control and control quality of life (33).
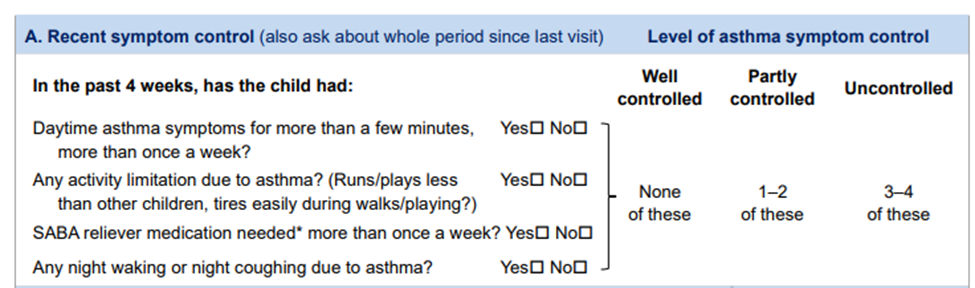
Assessment of level of asthma symptom control (34)
➡️Difficult-to-treat asthma:
It is asthma that is un controlled despite prescribing of medium or high-dose ICS with a second controller or with maintenance OCS, or that require high-dose treatment to maintain good symptoms control and reduce the risk of exacerbations. It doesn’t mean a ‘difficult patient’. In many cases, asthma may appear to be difficult because of modifiable factors such as incorrect inhaler technique, poor adherence, exposure to smoking or other irritants, presence of comorbidities, or because the diagnosis is in correct. (35)
➡️Severe asthma:
It is a subset of difficult-to-treat asthma. It means asthma that is un controlled despite adherence with maximal optimized high-dose controller treatment and management of contributory factors, or that worsen when high-dose treatment is decreased.
Asthma is not defined as severe if it markedly improves when contributory factors are addressed. (35)
➡️Prognosis of asthma:
Recurrent coughing and wheezing occur in 35% of preschool-age children. Of these, approximately one-third continue to have persistent asthma into later childhood, and approximately two-thirds improve on their own through their teen years (36).
Asthma severity by the ages of 7-10 year is predictive of asthma persistence in adulthood. Children with moderate to severe asthma and with lower lung function measures are likely to have persistent asthma as adults. Children with milder asthma and normal lung function are likely to improve over time, with some becoming periodically asthmatic (disease-free for months to years); however, complete remission for 5 years in childhood is uncommon (37).
➡️Asthma predictive index
3 or more wheezing episodes plus at least 1 major criteria or 2 minor criteria.
I. Major criteria
• Parental history of asthma
• Physician-diagnosed atopic dermatitis
• Inhalant allergen sensitization
II. Minor criteria
• Physician-diagnosed allergic rhinitis
• Wheezing without colds
• Blood eosinophil count ≥4%
• Food allergen sensitization
The role of these tools is to help identify children at
greater risk of developing persistent asthma symptoms not as criteria for the diagnosis of asthma in
young children(38).
➡️Prevention of asthma:
A hygiene hypothesis purports that naturally occurring microbial exposures in early life might drive early immune development away from allergic sensitization, persistent airways inflammation, and remodeling. If these natural microbial exposures truly have an asthma-protective effect, without significant adverse health consequences, then these findings may foster new strategies for asthma prevention (39).
Several non-pharmacotherapeutic measures with numerous positive health attributes—avoidance of environmental tobacco smoke (beginning prenatally), exclusive breastfeeding (>4 months), an active lifestyle, and a healthy diet—might reduce the likelihood of asthma development (40).
The vaccinations are safe and effective in asthma, may help prevent asthma development, and pneumococcal and annual influenza vaccination in particular should be offered to asthmatics. Vaccines against Respiratory Syncytial Virus (RSV), which are the main triggers for asthma exacerbation and have been linked to asthma inception, should help reduce asthma morbidity and mortality (41).
➡️Purpose & Scope
These guidelines have been developed to standardize the delivery of services and to implement the guidance on the prevention, diagnosis and management of bronchial asthma in children. It provides guidance to primary health care providers, pediatricians and specially trained nurses.
The guidelines aimed to improve early case detection and referral, case management of bronchial asthma. As a sequence, there will be an improvement in quality of life and medical condition for asthmatic children.
This version of the guideline includes recommendations and good practice statements for children suffering from bronchial asthma.