Bronchial Asthma Management in Children
- Recommendations
Table 3. Recommendations |
|
| |||
A. Diagnosis and management of asthma in children 5 years and younger Q1. For children 5years&younger What is the best practice in the diagnostic criteria of asthma? |
|
| |||
N | Health questions | Source Guideline | Recommendations | Quality of evidence | Strength of Recommendation |
1.a | - Is there clinical assessment for probability of asthma in children 5 years and younger |
Canadian thoracic society 2021
Japanese 2020
| Clinical assessment to assess for the initial probability of asthma is based on: • a history of recurrent episodes (3 attacks) of wheeze, cough, breathlessness and chest tightness that vary over time • recorded observation of wheeze heard by a healthcare professional • personal/family history of other atopic conditions (in particular, atopic eczema/dermatitis, allergic rhinitis) • no symptoms/signs to suggest alternative diagnoses.
Symptom improvement can be observed after beta-2 agonist inhalation. | intermediate
intermediate
| Strong
strong
(GPS)
|
1.b | Is assessing clinical improvement after using regular low-dose inhaled corticosteroids (ICS) and as-needed SABA within 2–3 months’ support diagnosis of asthma in children 5 years and younger?
| GINA 2024 | A trial of treatment for at least 2–3 months with as-needed SABA and regular low-dose ICS may provide some guidance about the diagnosis of asthma. Marked clinical improvement during treatment, and deterioration when treatment is stopped, support a diagnosis of asthma. | Very low | Weak (conditional) |
1.c | Is chest X-ray indicated for diagnosis of asthma? | GINA 2024 | Chest X-ray Radiographs are rarely indicated; except, if there is doubt about the diagnosis of asthma help to exclude other diagnoses. |
| GPS |
Q2. For children aged 5 years and younger: What is the best practice for assessing asthma severity? | |||||
2 | How to assess pulmonary function in children 5 years and younger? | GINA 2024 | Due to the inability of most children 5 years and younger to perform reproducible expiratory maneuvers, lung function testing, do not have a major role in the diagnosis of asthma at this age. However, by 5 years of age, many children are capable of performing reproducible spirometry if coached by an experienced technician and with visual incentives |
| GPS |
| Q3- For children aged 5 years and younger: What is the best practice for the initial asthma management based on asthma severity? | ||||
3.a | Which children should be initiated on regular low dose ICS as controller treatment? | GINA 2024 | If symptoms pattern is consistent with asthma, and asthma symptoms are not well controlled, or > 3 exacerbations per year.
| Very low | Weak (conditional) |
|
| GINA 2024 | If symptoms pattern is not consistent with asthma but wheezing episodes requiring SABA occur frequently e.g > 3 per year. Give diagnostic trial for 3 months | Very low | Weak
|
3.b | When to use double low dose ICS as controller therapy in children 5 years and younger | GINA 2024 | Doubling the initial low dose of ICS may be the best option if asthma is not well controlled on low dose ICS after checking inhaler technique and adherence | Low | Weak (conditional) |
3.c | What is the role of LTRA in asthma management? | Japanese 2020 | LTRA can be added to ICS for children whose asthma is not controlled well with ICS alone. | low | Weak (conditional) |
3.d | Can we use LABA in the management of asthma in children 5 years and younger? | GINA 2024 | There are insufficient data about the efficacy and safety of ICS in combination with a long-acting beta2 agonist (LABA) in children <4 years old to recommend their use. |
| GPS |
3.e | How often should a child be reviewed after initial treatment to review response and adjust treatment? | GINA 2024 | -Assessment at every visit (every 2-3 months) should include asthma symptom control and risk factors and side-effects. -If therapy is stepped-down or discontinued, schedule a follow-up visit 3–6 weeks later to check whether symptoms have recurred, as therapy may need to be stepped-up or reinstituted
The child’s height should be measured every year, or more often.
| Very low
Very low | Weak (conditional)
Weak (conditional) |
| For children aged 5 years and younger: when to refer to asthma specialist
| GINA 2024 | The child should be referred for expert assessment if symptom control remains poor and/or flare-ups persist, or if side-effects of treatment are observed or suspected | low | Weak
|
3.f | 4- Is self-management education, including a written personalized asthma action plan should be offered to parents of children 5 years and younger?
| British 2019 | All people with asthma (and/or their parents or carers) should be offered self-management education, which should include a written personalized asthma action plan and be supported by regular professional review. | High | Strong |
|
Table 4. Recommendations |
|
|
|||
|
B. Diagnosis and Management of asthma in children 6 years and older |
|
|
|||
|
N |
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
Q4 |
How is asthma diagnosed? |
GINA 2024
ERS 2021 |
The diagnosis of asthma is based on the history of characteristic symptom patterns and evidence of variable expiratory airflow limitation and reversibility by spirometry (appendix) or peak expiratory flow if available rather than relying on symptoms alone.
The task force recommends spirometry as part of the diagnostic work-up of children aged 5–16 years with suspected asthma |
Moderate |
GPS
Strong |
|
Q5 |
What are the characteristic symptom patterns of asthma? |
GINA 2024 |
Wheeze, shortness of breath, cough and/or chest tightness: • Often worse at night or in the early morning. • Vary over time and in intensity. • Triggered by viral infections, exercise, allergen exposure, changes in weather, laughter, or irritants such as car exhaust fumes, smoke or strong smells. |
|
GPS |
|
|
Stepwise approach for management of asthma for children 6 years and older |
||||
|
Q6.a |
In children 6 years and older, what is the criteria to start step 1 to control the symptoms and minimize future risk?
|
GINA 2024 |
Start with step 1 in children with: Symptoms <twice / week As-needed low-dose ICS |
High |
Strong |
|
Q6.b |
What is the preferred controller in step 1? |
GINA 2024 |
Low dose ICS taken whenever SABA taken |
Intermediate |
Strong |
|
Q7.a |
In children 6 years and older, what is the criteria to start step2 to control the symptoms and minimize future risk? |
GINA 2024 |
Start with step 2 in children with: Symptoms ≥twice / week but not daily |
|
GPS |
|
Q7.b |
What is the preferred controller in step 2? |
GINA 2024 |
Daily low dose ICS |
High |
Strong |
|
Q7.c |
What is the other controller options in step 2? |
GINA 2024 |
Daily Leukotrienes receptor antagonist or low dose ICS taken whenever SABA taken |
High
Intermediate |
Strong
Strong |
|
Q8.a |
In children 6 years and older, what is the criteria to start step3 to control the symptoms and minimize future risk? |
GINA 2024 |
Start with step 3 in children with: Symptoms most days or waking from asthma once or more / week |
|
GPS |
|
Q8.b |
What is the preferred controller in step 3? |
GINA 2024 |
Low dose ICS-LABA OR Medium dose ICS or Very low dose ICS-LABA (MART) |
High
Intermediate |
Strong
Strong |
|
Q8.c |
What is the other controller options in step 3? |
GINA 2024 |
Low dose ICS+ LTRA |
|
GPS |
|
Q9.a |
In children 6 years and older, what is the criteria to start step4 to control the symptoms and minimize future risk?
|
GINA 2024 |
Start with step 4 in children with: Symptoms most days or waking from asthma once or more / week + low lung functions if available |
Very low |
Weak
|
|
Q9.b |
What is the preferred controller in step 4? |
GINA 2024 |
Medium dose ICS-LABA OR
Low dose ICS-LABA (MART) OR Refer for expert advice |
Intermediate
Very low |
Strong
Weak (conditional) |
|
Q9.c |
What is the other controller options in step 4? |
GINA 2024 |
Add-on tiotropium
or Add on LTRA |
High |
Strong
GPS |
|
Q10.a |
In children 6 years and older, what is the criteria to start step 5 to control the symptoms and minimize future risk?
|
GINA 2024 |
Start with step 5 in children not controlled with step 4 and refer to expert
|
Very low |
Weak (conditional) |
|
Q10.b |
What is the preferred expert controller in step 5? |
GINA 2024 |
Refer for phenotypic assessment ±higher dose ICS-LABA or Add-on therapy, e.g. anti-IgE,, anti- IL5, Add on long acting muscarinic antagonist (LAMA) (Tiotropium) or anti-IL4R |
High |
Strong
GPS |
|
Q10.c |
What is the other controller options in step 5? |
GINA 2024 |
Consider add on low dose OCS but consider side effects |
|
GPS |
|
|
Difficult to treat asthma |
||||
|
Q11 |
What is difficult to treat asthma? |
GINA 2024 |
It is asthma that is uncontrolled despite prescribing of medium- or high-dose ICS with a second controller (usually a LABA) or with maintenance OCS, or that requires high-dose treatment to maintain good symptom control and reduce the risk of exacerbations. It does not mean a ‘difficult patient’. In many cases, asthma may appear to be difficult to treat because of modifiable factors such as incorrect inhaler technique, poor adherence, smoking or comorbidities, or because the diagnosis is incorrect
|
|
GPS |
|
Q12 |
How to assess difficult to treat asthma?
|
British 2019
British 2019
GINA 2024
GINA 2024 |
Patients with difficult asthma should be systematically evaluated, including:
A. Confirmation of the diagnosis of asthma (refer to Q1 and Q4)
B. Clinician should consider poor adherence to maintenance therapy
C. Review history and examination for comorbidities These include anxiety and depression, obesity, deconditioning, chronic rhinosinusitis, inducible laryngeal obstruction, GERD, obstructive sleep apnea, bronchiectasis, cardiac disease, and kyphosis due to osteoporosis. Investigate according to clinical suspicion.
D. Modifiable risk factors and triggers: identify factors that increase the risk of exacerbations, e.g., environmental tobacco exposure, other environmental exposures (indoor and outdoor) air pollution, molds and noxious chemicals, and medications such as beta-blockers or nonsteroidal anti-inflammatory drugs (NSAIDs).
|
Very low
Low |
Weak (conditional)
Weak
GPS
GPS |
|
|
Asthma resistant to therapy |
||||
|
Q13 |
What is asthma resistant to therapy? |
GINA 2024 |
Severe asthma is a subset of difficult-to-treat asthma. It means asthma that is uncontrolled despite adherence with maximal optimized high-dose ICS-LABA treatment and management of contributory factors, or that worsens when high-dose treatment is decreased |
|
GPS |
|
Q14 |
When to refer patients with asthma resistant to therapy? |
GINA 2024 |
In Children 6 years and older Children with persistent asthma symptoms or exacerbations despite correct inhaler technique and good adherence with Step 4 treatment and in whom other controller options have been considered, should be referred to a specialist with expertise in investigation and management of severe asthma, if available |
Very low |
Weak (conditional) |
|
Q15 |
How to assess asthma resistant to therapy?
|
GINA 2024 |
In Children 6 years and older -Further assessment and management should be done by a specialist, preferably in a multidisciplinary severe asthma clinic if available -Additional investigations may be appropriate for identifying less-common comorbidities and differential diagnoses contributing to symptoms and/or exacerbations and should be based on clinical suspicion -Assess the severe asthma phenotype |
|
GPS |
|
|
Immunotherapy (IT) |
||||
|
Q16 |
What about the role of allergy testing for severe asthma? |
(GINA) 2024 |
• Consider skin prick test (SPT) or specific IgE if not done before
|
|
GPS |
|
Q17 |
What is the role of IT in asthma control? |
(GINA) 2024 |
• Allergen immunotherapy may be considered as add-on-therapy for asthmatic children who have clinically significant sensitization to aeroallergens including those with allergic rhinitis. • When considering SCIT for children with asthma the potenial benefits compared with pharmacological treatment and allergn avoidance must be weighed against the risk of adverse effects and the inconvience and the cost of prolonged coarse of therapy (3-5 years)
|
Very low |
Weak |
|
Q18 |
What is the role of biological therapy in asthma treatment? |
GINA 2024 |
•If available and affordable, consider an add-on Type 2 targeted biologic for patients with severe asthma who have allergic or eosinophilic biomarkers or need maintenance OCS. • Where relevant, test for parasitic infection, and treat if present, before commencing treatment. • Consider whether to start first with anti-IgE, anti-IL5/5Rα, anti-IL4Rα or anti-TSLP |
|
GPS |
|
|
Prevention |
||||
|
Q19 |
What is the best practice to prevent or reduce the severity of asthma attacks? |
||||
|
Q19.a |
Which interventions (avoidance or reduction of exposure to environmental factors) at home, school and outdoor environment can improve asthma control and prevent or reduce the severity of asthma attacks?
|
British 2019
British 2019
|
• Measures to reduce in utero or early life exposure to single aeroallergens, such as house dust mites or pets, or single food allergens, are not recommended for the primary prevention of asthma.
• For children at risk of developing asthma, complex, multifaceted interventions targeting multiple allergens may be considered in families able to meet the costs, demands and inconvenience of such a demanding program.
|
High
High
|
Strong
Strong
|
|
Q19.b |
Is food allergen avoidance for mothers is beneficial for preventing childhood asthma? |
British 2019 |
In the absence of any evidence of benefit and given the potential for adverse effects, maternal food allergen avoidance during pregnancy and lactation is not recommended as a strategy for preventing childhood asthma. |
Intermediate |
Strong |
|
Q19.c |
What is the effect of encouraging breast feeding in infants for asthma prevention? |
British 2019 |
Breastfeeding should be encouraged for its many benefits, including a potential protective effect in relation to early asthma
|
Low |
Weak (conditional) |
|
Q19.d |
Is Avoidance of tobacco smoke and other air pollutants decrease the risk of wheezing in infancy and the risk of persistent asthma. |
British 2019 |
Patients with asthma and parents/carers of children with asthma should be advised about the dangers of smoking and second-hand tobacco smoke exposure on their children including increased wheezing in infancy and increased risk of persistent asthma., and should be offered appropriate support to stop smoking.
|
Intermediate |
Strong |
|
Q19.e.1 |
Is Immunizations have any considerations related to asthma in infants and children |
British 2019 |
Immunizations should be administered independent of any considerations related to asthma. |
Low |
Weak (conditional) |
|
Q19.e.2 |
Is pneumococcal vaccine indicated for asthma? |
GINA 2024 |
Pneumococcal vaccine protects against invasive pneumococcal infection, but asthma alone is not a specific indication for pneumococcal vaccination.
|
|
GPS |
|
Q19.e.3 |
Is influenza vaccine indicated for asthma |
GINA 2024 |
Advise patients with moderate to severe asthma to receive an influenza vaccination every year, or at least when vaccination of the general population is advised |
|
GPS |
➡️Evidence to recommendations: Considerations
The GDG was guided by the results of the AGREE II appraisals of the eligible CPGs and thoroughly reviewed the recommendations of the original sources of appraised Guidelines CPGs in consideration of local contextual factors related to the national Egyptian health system like burden of the disease, equity, acceptability, feasibility, and other relevant factors. The GDG decided through an informal consensus process to adopt most recommendations however, there was a need to change the strength of 2 recommendations (B2 and B3) as they lack feasibility. Also, GDG develops group of good practice statements to improve acceptability and feasibility.
➡️Implementation considerations
To improve Asthma care and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing bronchial asthma diagnosis, treatment, and prevention strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of asthma care delivery, care gaps and current needs.
3. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
4. Identify barriers to, and facilitators of implementation.
5. Select an implementation framework and its component strategies.
6. Develop a step-by-step implementation plan:
▪️ Select the target populations and evaluate the outcome.
▪️ Identify the local resources to support the implementation.
▪️ Set timelines.
▪️ Distribute the tasks to the members.
▪️Evaluate the outcomes.
7. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
▪️ Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
▪️ Educational materials: printed or electronic information (software).
▪️ Web-based education: computer-based educational activities.
▪️ A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
▪️ Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
▪️ Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
▪️ Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
▪️ Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
▪️Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behaviors.
▪️ Mass media campaigns.
3. For Nurses
▪️Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
▪️ Educational materials: printed.
▪️ A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
▪️ Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
▪️ Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
▪️ Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
▪️ Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
▪️ Administrative policies and procedures.
▪️ Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
▪️ International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
▪️ Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
➡️Implementation Tools
Educational materials based on this Adapted CPG for treatment of asthma in children have been made available in several forms including:
1. Manual for physician for diagnosis and algorithm for management of bronchial asthma
2. Arabic Educational materials for nurses and mothers

https://www.magonlinelibrary.com/doi/abs/10.12968/bjsn.2016
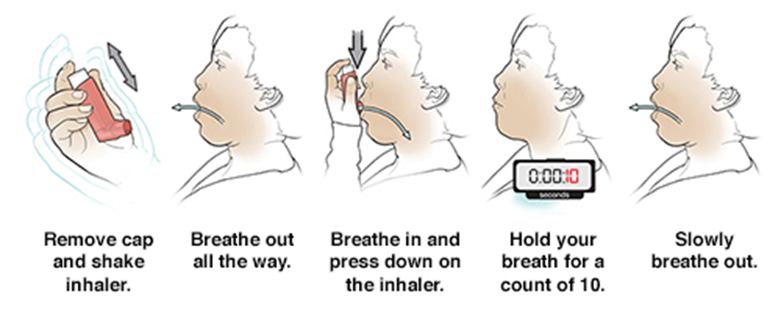
1- MDI without spacer
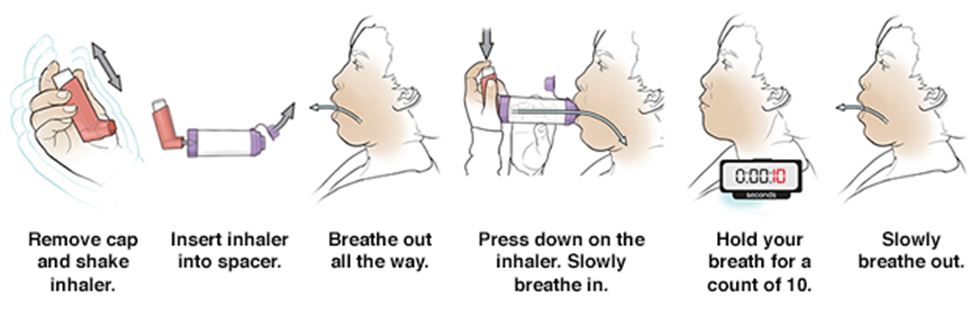
2- MDI with spacer
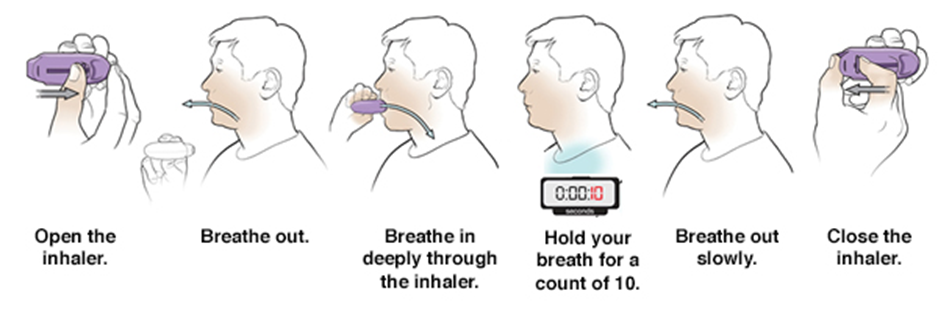
3- How to use a DPI ?
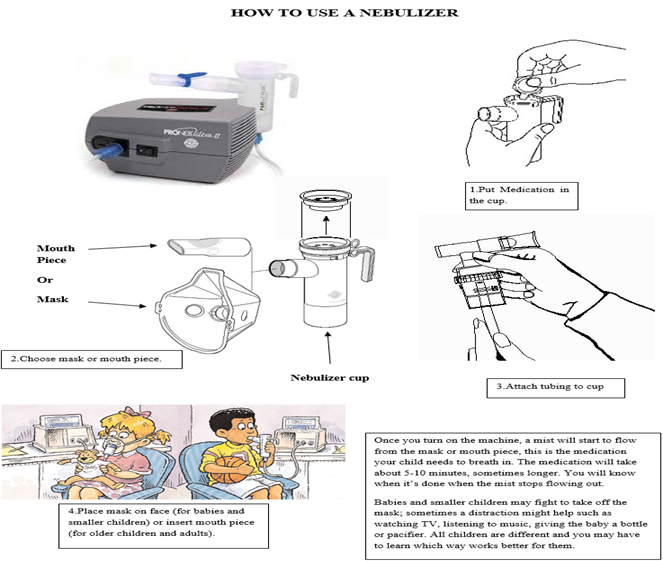
4-Nebulizer