Anemia in Chronic Kidney Disease (CKD)
- Recommendations
Chapter 1: diagnostic evaluation of anemia in chronic kidney disease(CKD) patients:
Guideline 1: Evaluation of anemia in CKD
1: Hemoglobin (Hb) levels should be routinely measured to screen for anemia on initial evaluation for all CKD patients (regardless age and stage of CKD). And when anemia is suspected based on symptoms:
• At least annually in patients with CKD stage 3.
• At least twice a year in patients with CKD stage 4.
• At least every 3 months in patients with (CKD-ND) and (PD).
• At least monthly in patients with (CKD-HD) and (PD)
Good Practice Statement
Rationale
Anemia in adults is typically defined according to the thresholds from the World Health Organization (WHO): hemoglobin (Hb) <12 g/dl (120 g/l) for women, and <13 g/dl (130 g/l) for men (1) The prevalence of anemia in CKD increases at lower levels of estimated glomerular filtration rate (eGFR), reaching a prevalence of >50% at the advanced CKD (CKD G4-G5). The prevalence is disproportionately higher in women compared to men. (1)
Multiple studies showed that 21%–62% of people with CKD not receiving dialysis have anemia, defined as Hb <12 g/dl in females and <13.5 g/dl in males, with increasing prevalence in more advanced CKD (2) ( 3) (4),(5) For people with CKD receiving hemodialysis (CKD- HD), data from the United States Renal Data System (USRDS)(6) showed that 64.5%, 14.4%, and 6.6% have Hb levels between 10–12 g/dl, 9–10 g/dl, or <9 g/dl, respectively. For those treated with an ESA, they recommend measuring Hb concentration when clinically indicated and at least monthly in patients with (CKD- HD).
Good Practice Statement
Rationale
The age of the person, degree of anemia (i.e., Hb concentration), RBC volume (i.e., mean corpuscular volume [MCV]), attributable symptoms, severity of CKD, use of dialysis, comorbid diseases, and RBC transfusion risk may all influence the need for and frequency of testing for anemia and its underlying causes. This drive for screening must be counterbalanced by attempts to minimize unnecessary blood draws. (16) Anemia in CKD is frequently multifactorial. Common causes include relative erythropoietin (EPO) deficiency, shortened RBC survival, iron and other nutritional deficiencies (folate and vitamin B12), blood loss during hemodialysis, uremic toxin- induce inhibition of bone marrow response to EPO, systemic inflammation, of these factors, EPO and iron are the most important factors. (7)
Hepcidin, a liver-derived 25-amino acid hormone, is a critical regulator of iron homeostasis, or how one’s body regulates iron levels and metabolism. It is responsible for regulating the absorption of dietary iron and macrophage recycling of iron for delivery to RBC precursors Increased hepcidin levels in CKD contribute to dysregulated iron homeostasis. (16)
Many observational studies show that iron deficiency is associated with an increased risk of mortality and cardiovascular hospitalization in people with CKD. (8 ,9) In particular, iron deficiency, as captured by low TSAT, is associated with higher risk of all-cause mortality and major adverse cardiovascular events (MACE) in people with CKD not receiving dialysis, regardless of ferritin levels or the presence of anemia. (10, 11,12) Additionally, low TSAT levels (≤15%), irrespective of ferritin levels, are associated with worse physical health- related quality of life (HRQoL) compared to higher TSAT levels in people with CKD not receiving (CK-ND)dialysis.( 9) In people with( CKD- HD), normal iron status (i.e., TSAT>20% and ferritin ≤800 µg/l) was associated with better survival as compared to (systemic iron deficiency)which is previously known as absolute iron deficiency anemia defined as TSAT ≤20% and serum ferritin ≤200 ng/ml or (restricted-iron deficiency)which was previously known as functional iron deficiency defined as TSAT ≤20% and serum ferritin 200–800 ng/ml) or high iron status (i.e., ferritin>800 µg/l). (13)
1.3: Patients with CKD and anemia, in whom the initial test do not reveal the cause, consider this expanded panel to identify potential underlying causes:
· Blood smear
· C reactive protein (CRP)
· Test for hemolysis, (lactate dehydrogenase, haptoglobin)
· Serum vitamin B12 and folic acid levels
· Thyroid stimulating hormone (TSH)
· liver function tests, (ALT, AST)
· Serum protein electrophoresis (SPEP) with immunofixation, serum free light chains, urinary Bence-Jones protein,
· Occult blood in stool.
Good Practice Statement
Rationale
Although relative erythropoietin deficiency is common among patients with anemia and CKD, other potential causes should be identified or excluded. A clinical and laboratory evaluation of the cause of anemia should precede initiation of ESA therapy. (14)
The recommended laboratory evaluation aims for assessing:
o The degree and cause of anemia
o Bone marrow responsiveness, and anemia due to causes other than erythropoietin deficiency should be suspected when:
o The severity of the anemia is disproportionate to the deficit in renal function,
o There is evidence of hemolysis, or There is evidence of bone marrow disorder as manifest by leucopoenia and/or thrombocytopenia (.15)
In addition to iron deficiency, anemia may be the consequence of inflammation, hemolysis, liver insufficiency, vitamin B12 or folate deficiencies, endocrine disorders (e.g., hypothyroidism), malignancy (plasma cell disorders such as multiple myeloma), or other causes for which no diagnostic testing is available (e.g., medications). In people with persistent or progressive anemia with associated symptoms, if the initial diagnosis and management of the anemia does not yield resolution of anemia, consider intermittently repeating assessment of alternative causes for anemia (16)
In CKD patients not yet requiring dialysis and in those on peritoneal dialysis (PD), the timing of the blood sample draw is not critical because plasma volume in these patients remains relatively constant. In hemodialysis patients one issue remain to be clarified. Hemoglobin concentrations are routinely measured in dialysis patients before dialysis This potentially leads to lower hematocrit values as a result of dilution from fluid overload prior to ultrafiltration and an underestimate to actual hemoglobin value. Interdialytic weight gain contributes to a decrease in Hb level, whereas intradialytic ultrafiltration leads to an increase in Hb level. (17)
▪️ 1.4: CKD should be considered as a possible cause of anemia when the glomerular filtration rate (eGFR) is <60 ml/min/1.73m2 It is more likely to be the cause if the eGFR is <30ml/min/1.73m2. (<45/min/1.73m2 in patients with diabetes) and no other cause, e.g., blood loss, folic acid or vitamin B12 deficiency, is identified.
Conditional Recommendation
low-quality evidence:
Rationale
The prevalence of anemia in patients with CKD increases as the GFR progressively falls NHANES III data demonstrate a prevalence of anemia of 1%, 9% and 33% in CKD patients with an eGFR of 60, 30 and 15ml/min/1.73m2 respectively. (18) Anemia is more prevalent among patients with diabetes. In addition, anemia of CKD develops earlier in patients with diabetes compared with non-diabetic patients at all level of GFR. (19, 20) In a cross-sectional study involving over 800 patients with diabetes, anemia has been found to be two to three times more common in diabetic compared with general population at all stages of GFR. (21)
1.5: Consider referral of patients with CKD and anemia, when serum ferritin <45 µg/l, to gastroenterologists/urologists /gynecologists to identify the cause of blood loss.
Good Practice Statement
Rationale
chapter 2. use of iron to treat iron deficiency anemia in CKD
2.1: We suggest initiation of iron therapy in patients with CKD/HD if serum ferritin ≤500 ng/ml (≤500 µg/l) and TSAT <30%.
Conditional Recommendation
Low-quality evidence:
Rationale
A definition of adequate iron status is
a serum ferritin between200-500 microgram/L in HD patients,
100-500 microgram/L in non-HD patients and
Either <6% hypochromic red cells (HRC), or reticulocyte Hb content >29 pg.
TSAT>20%
The aim of iron treatment targets is to optimize anemia therapy while minimizing potential toxicity. Therapy target aim at, (1) Minimizing the ESA dose required to maintain target Hb levels in patients on ESA therapy (2) Maximining the Hb level and minimizing the need to initiate ESA therapy to achieve target Hb levels in patients not on ESA therapy.(22)
Several studies have reported that the dose of ESA required to achieve and maintain a given Hb level is inversely related to iron stores. (24 ,14) Iron deficiency (“systemic iron deficiency) or (iron-restricted erythropoiesis) was the main cause of ESA resistance.
In a randomized controlled study involving 57 hemodialysis patients comparing iron management based on serum ferritin and transferrin saturation versus reticulocyte Hb content (CHr) CHr was a markedly more stable than serum ferritin or transferrin saturation. (23)
NICE evaluation of iron therapy in CKD patients suggests that for hemodialysis patients, percentage of hypochromic red blood cells %HRC > 6 dominated all other iron evaluation strategies. For other patients, TSAT less than 20% alone or serum ferritin less than 100 micrograms/L alone were the least cost-effective strategy, but %HRC was the most cost-effective. (24)
Use of percentage of hypochromic red blood cells (% HRC; > 6%), only if processing of blood sample is possible within 6 hours. Since a fresh blood sample is needed, this test may be difficult to use. If the percentage of hypochromic red blood cells is not available, use reticulocyte Hb content (CHr; 29 pg). If neither test is available, we recommend testing both serum ferritin and transferrin saturation rather than relying on either test separately. (24,25)
· ferritin <100 ng/ml (<100 µg/l) and transferrin saturation (TSAT) <40%, or
· ferritin ≥100 ng/ml (≥100 µg/l) and <300 ng/ml (<300 µg/l), and TSAT <25%.
Conditional Recommendation
Very low quality evidence
Rationale
.
Systematic review of the evidence indicated that compared with placebo, iron increased Hb concentrations on average by about 0.65–1 g/dl (6.5–10 g/l). Iron supplementation is likely to reduce the requirement for ESA therapy. Given the high cost of ESAs, appropriate use of oral iron in people with anemia and CKD would be expected to reduce overall costs by lowering ESA use. For people not treated with dialysis, administration of i.v. iron requires additional facilities and personnel, the relative costs of which are uncertain as compared to ESA treatment. (16)
2.3: In people with (CKD-HD) in whom iron therapy is being initiated, administer intravenous iron using a proactive approach to maintain stable iron status.
Rationale
(PIVOTAL) study, (29) compared a high-dose proactive IV iron sucrose regimen to a low-dose, reactive IV iron sucrose, regimen in 2141 adult patients in their first year of hemodialysis (HD) receiving an erythropoiesis stimulating agent (ESA). Patients in the high-dose group received 400mg IV iron sucrose proactively every month unless serum ferritin was>700μg/L or transferrin saturation (TSAT) ≥40%. The low-dose group received 0 to 400mg monthly, with a serum ferritin of <200μg/L or a TSAT of <20% being a trigger for iron administration. The authors concluded that a high-dose IV iron regimen administered proactively was superior to a low-dose regimen administered reactively; resulting in a lower risk of death or major adverse cardiovascular events, and requiring lower doses of ESA and likely helps prevent periods of iron restriction, leading to more consistent and optimal management of anemia also a lower incidence of blood transfusions.
. Repeated doses of i.v. iron may be required, depending on the specific i.v. iron preparation used. The maximum single dose varies by formulation, with some preparations allowing higher doses in one session than others. This is typically determined by the degree of labile iron release into the circulation, which limits the maximal dose. (26,30)
Conditional Recommendation
Very low quality
Intravenous iron seemed to increase ferritin concentrations and TSAT to a greater extent than oral iron, regardless of the total dose of iron given, most people with (CKD- HD) would prefer i.v. iron over oral iron as it can be administered during dialysis. Those at risk of or particularly worried about hypersensitivity reactions may prefer oral treatment (table3). (16) Evidence on the risks and benefits of IV iron, therapy in these patients is not well established. The effect of iron therapy in this group of patients was assessed in The Dialysis patients’ Response to IV Iron with Elevated ferritin (DRIVE) trial. (28)
The DRIVE studies found that in people with CKD HD, i.v. iron resulted in higher Hb concentrations and lower ESA usage even when the iron initiation threshold included serum ferritin concentrations >800 ng/ml (>800 µg/l). (28) However, whether this improved health outcomes or even provided incremental QoL benefits is unknown. Some retrospective observational data suggests that more intensive i.v. iron administration may be associated with increased risk of mortality and infections. (31)
There is a theoretical concern that iron could be deposited in tissues or that non-transferrin-bound iron could have direct toxic effects, although this has not been well-studied in people with CKD.
Ferric pyrophosphate citrate is a water-soluble iron salt administered intravenously or via dialysate. In contrast to other i.v. iron preparations that are taken up by reticuloendothelial macrophages to liberalize iron, ferric pyrophosphate citrate delivers iron directly to circulating transferrin.
Table 3 | Factors to consider when choosing between oral and intravenous iron
|
Oral Iron |
Intravenous Iron |
|
Slower increase in Hb, ferritin, TSAT |
More rapid increase in Hb, ferritin, TSAT Delayed and reduced ESA use Possibly faster increase in QoL |
|
Side effects • More frequent • Less severe Constipation and other gastrointestinal symptoms are frequent. If the patient suffers from these symptoms at baseline, then i.v. iron may be preferred |
Side effects • Less frequent • More severe Hypotension and immediate hypersensitivity reactions are uncommon but can occur with any i.v. iron agent, especially in people with a history of drug allergies |
|
Less expensive More convenient |
More expensive Requires trained healthcare providers |
|
Accessibility • Appealing to people who want to limit hospital visits. • Addresses mobility inequality for people with CKD |
|
|
Preserve veins for hemodialysis vascular access |
Consider possible effect on preserving veins for hemodialysis vascular access |
|
Inconsistent adherence |
Assured administration |
|
Avoid if intestinal absorption impaired |
|
2.5: In people with CKD treated with iron, it is reasonable to withhold iron if ferritin ≥700 ng/ml (≥700 µg/l) or TSAT ≥40%
Good Practice Statement
Intravenous iron therapy in particular has potential risks as well as benefits. Toxicity associated with high ferritin outcomes was originally reported in the context of multiple transfusions in the pre-ESA era. The risk persists that intravenous iron may reproduce similar toxicity and thus regular monitoring during therapy is required. (32,33)
The PIVOTAL Trial, found that cardiovascular outcomes were improved with a proactive iron treatment strategy to higher iron targets (treatment until serum ferritin ≥700 ng/ml [≥700 µg/l] or (TSAT ≥40%) (29). These results do not necessarily indicate that these higher iron test levels should be targeted in clinical treatment (34). An alternative interpretation of the study results was that this intensive iron strategy yielded improved cardiovascular outcomes, but specifically in comparison to a very conservative iron strategy that may have resulted in impaired health due to iron deficiency.
The DRIVE studies found that in people with (CKD- HD), i.v. iron resulted in higher Hb concentrations and lower ESA usage even when the iron initiation threshold included serum ferritin concentrations >800 ng/ml). (28) However, whether this improved health outcomes or even provided incremental quality of life (QoL) benefits is unknown. Some retrospective observational data suggests that more intensive i.v. iron administration may be associated with increased risk of mortality and infections. (31)
The safety of persistently very high ferritin levels remains unknown. The KDIGO 2012, (14) guideline highlighted the difficulty of trying to specify treatment initiation thresholds. PIVOTAL may have indicated that in people with CKD HD treated with ESA, higher iron dosing leads to improved outcomes, but it is not entirely clear what is driving these outcomes. Possibilities include the lower ESA doses required to maintain Hb within the target range, the correction of iron deficiency per se, a combination of these mechanisms, or other mechanisms yet unknown. (16).
Good Practice Statement
RATIONALE
At present oral iron should remain first line treatment among CKD patients not on hemodialysis and IV iron used if patients who are intolerant to oral iron or remain absolutely or functionally iron deficient despite oral iron. Two studies compared i.v. versus oral iron in 231 adults with( CKD -HD),( PD), testing different i.v. compounds for a maximum of 4 months, with doses per month of iron ranging from 500–1000 mg for i.v. iron and 5400–6000 mg for elemental oral iron. (35, 36) None reported critical outcomes, but more people reached higher Hb values with i.v. iron. This seems consistent with the analyses of i.v. or oral iron versus placebo where i.v. iron use led to higher Hb concentrations versus placebo than oral iron did.
Two randomized controlled studies of oral versus IV iron supplementation in pre- dialysis patients receiving concomitant ESAs are in agreement. In the first study of 45 patients with Hb <110g/L given either ferrous sulphate 200mg TDS versus 300mg iron sucrose IV monthly, there was no difference in Hb or ESA dose between the oral and IV group receiving ESA over a mean 5.2 months follow-up Iron stores were greater in the IV than oral group (.37)
in another study of 96 (ND-CKD) patients comparing 5 weeks of IV iron sucrose (200mg every 7 days for a total of 5 doses) versus 29 days of thrice daily oral iron (ferrous sulphate325mg TDS). There was no difference in Hb or ESA dose but greater increase in ferritin in the IV group. (38)
When offering intravenous iron therapy to people not receiving hemodialysis, consider high dose, (500mg) low- frequency in (two infusion) IV iron as the treatment of choice for adults and young people. (32)
When compared with oral iron therapy, i.v. iron provided a small additional increase in Hb of about 0.3–0.5 g/dl (30–50 g/l), and increased ferritin and TSAT. However, i.v. iron may cause serious hypersensitivity reactions, and although rare, these may be life-threatening, dependent on the compound. Oral iron, on the other hand, causes more gastrointestinal side effects. (16)
▪️ 2.7: In CKD patients not on dialysis switch from oral to intravenous iron if there is an insufficient effect of an optimal oral regimen after 1 to 3 months.
Good Practice Statement
Rationale
Oral iron is typically prescribed to provide approximately 200 mg of elemental iron daily, with most studies showing its effect on Hb concentration within 1 to 3 months. However, the desired effect may not be achieved for several reasons, justifying a switch in administration route. In people with CKD, gastrointestinal absorption of oral iron can be impaired by factors such as inflammation, reduced gastric acid production, or interactions with other medications. Intravenous iron bypasses the gastrointestinal tract, ensuring better and more consistent iron delivery to the body. (16) Additionally, oral iron may cause gastrointestinal side effects like constipation, nausea, and abdominal discomfort, leading to poor adherence, while i.v. iron avoids these issues and improves patient compliance.
▪️ 2.8: In people with CKD treated with iron, it is reasonable to test hemoglobin, ferritin, and TSAT every 3 months for those with (CKD-ND) or (CKD- PD) and every month for those with (CKD- HD).
Good Practice Statement
Rationale
No clinical trials specifically determine the optimal frequency for testing iron status during iron treatment. in line with previous guidelines, KDIGO,2025 agrees that it is reasonable to test iron status at least every three months for people with CKD not receiving HD, and every month for those with (CKD- HD). (16)
No clinical trials specifically determine the optimal frequency for testing iron status during iron treatment. Falling ferritin and/or TSAT levels are likely to reflect ongoing blood loss and can be used as an indication for additional iron supplementation. In people on oral iron, iron status testing can also be used to assess adherence with iron treatment. Conversely, increasing ferritin and/or TSAT levels may indicate that iron treatment is excessive and can be stopped or reduced. (16)
2.9: Consider treatment with oral or intravenous iron in people with CKD and profound iron deficiency (ferritin <30 µg/l and TSAT<20%) but with no anemia,
Good Practice Statement
Rationale
In fact, iron fulfills many more functions besides being the fuel for erythropoiesis, including deoxyribonucleic acid (DNA) synthesis, electron transport, and cellular proliferation and differentiation. Iron deficiency impairs myoblast proliferation (39) and impairs cardiomyocyte function. (40) Anemia is the end-phase of depleted iron stores.
Iron deficiency, independent of anemia, is associated with higher risk of all-cause mortality, MACE, and worse patient-reported outcomes in (CKD- HD) and in transplanted patients, (32, 41, 42). In addition, ample evidence from the field of chronic heart failure, including the subset of people with CKD, suggest benefit of iron therapy independent of anemia to improve functional status and hospitalizations. (43, 44, 45).
2.10: In people with CKD treated with IV iron resuscitative medication and trained personnel to evaluate and resuscitate anaphylaxis should be present at each administration of intravenous iron.
Conditional Recommendation
Low quality evidence
Rationale
Intravenous iron is rarely associated with acute hypersensitivity, hypotensive, and even anaphylactoid-type reactions. People may present with a variety of symptoms ranging from flushing, itching, shortness of breath, and hypotension. In older studies, such reactions were found to occur in 0.6%–0.7% of treated people. The frequency of reactions is probably significantly lower with newer iron preparations. Anaphylactoid reactions appear to occur more frequently with high molecular weight iron dextran (46). Labile or free iron reactions occur more frequently with non-dextran forms of iron. (47)
The MHRA has issued a guidance on the use of parenteral iron. This was in response to concerns raised as a result of serious and rarely fatal hypersensitivity reaction, particularly in pregnant women. These reactions can occur even when a previous administration has been tolerated (including a negative test dose). The risk of hypersensitivity is increased in patients with: known allergies (including drug allergies), immune or inflammatory conditions (e.g., systemic lupus erythematous, rheumatoid arthritis), or those with a history of severe asthma eczema, or another atopic allergy. (48)
Intravenous iron products should only be administered when staff trained to evaluate and manage anaphylactic or anaphylactoid reactions—as well as resuscitation facilities—are immediately available. Intravenous iron should only be administered if there is capability to manage acute hypersensitivity and hypotensive reactions, Intravenous doses of iron should not exceed the maximum dose/administration for the compound. Pretreatment with corticosteroids or antihistamines is not routinely necessary (type1 histamine [H1]-channel blockers), and the tests dose of intravenous iron are not usually required, because lack of response does not predict the risk of hypersensitivity. (49)
Chapter 3. use of ESAs, to treat anemia in CKD
3.1: Treatment of Anemia with ESA Therapy.
Treatment initiation:
▪️ 3.1.1: In people with anemia and CKD (whether treated with dialysis or not), the decision to use erythropoietin- stimulating agents (ESAs) or hypoxia- inducible factor-prolyl hydroxylase inhibitors (HIF-PHIs) to raise the hemoglobin (Hb) should consider each individual’s symptoms, potential for harm from red blood cell transfusions, and potential risk of adverse events (e.g. stroke, cardiovascular event, cancer).
Good Practice Statement
Rationale
Treatment of anemia with ESAs or HIF-PHIs improves symptoms and reduces RBC transfusions as compared to no treatment in CKD on dialysis (CKD-HD) (50,51), and (CKD-ND) not on dialysis. ( 52, 53) However, there is no evidence that such treatment improves mortality or cardiovascular outcomes in people with CKD with or without receiving dialysis. Moreover, the use of ESAs to target higher Hb levels has been associated with harm and HIF-PHIs have not been shown to be safer than ESA. Among people with CKD not receiving dialysis, there is even more some HIF-PHIs possibly associated with a higher risk of MACE and vascular access thrombosis than ESAs. (54,55,56). Therefore, patients should be informed about the risks and benefits of such treatment, aiming to facilitate a decision that is consistent with their values and preferences.
Conditional Recommendation
very low evidence
Rationale
ESAs and HIF-PHIs are both effective for treatment of anemia in adults with (CKD- HD) or (CKD- ND) not receiving dialysis. Although the overall analyses suggest noninferiority of HIF-PHIs to ESAs for MACE and other critical outcomes, (57,58). some studies suggest that at least some HIF-PHIs may have more MACE and other vascular events than ESAs, particularly in CKD not receiving dialysis. (54,55,56) Daprodustat and vadadustat were rejected by the U.S. Food and Drug Administration (FDA) for use in CKD not receiving dialysis.
Additionally, there are limited long-term head-to-head studies demonstrating the risks and benefits of HIF-PHIs as compared with ESAs, whereas ESAs have been used for decades and their risks and benefits are well understood. Whether HIF-PHIs may have increased efficacy over ESAs in some clinical contexts (e.g., ESA hyporesponsiveness) or may reduce iron requirements compared with ESAs has not been demonstrated in RCTs. In the absence of such long-term safety data, ESAs are preferred to HIF-PHI for most patients with CKD (with or without KRT).
Conditional Recommendation
Low quality evidence
Rationale
ESAs effectively raise Hb, which reduces the risk of RBC transfusions and increases QoL for people with (CKD- HD) and (CKD-ND) when Hb concentrations <9.0 g/dl (.59,60) However, the risk of harms such as cardiovascular events and vascular access thrombosis may be increased with ESA therapy to target higher Hb concentrations >10–11 g/d1 and, thus, may outweigh the potential benefits.
In a double-blind RCT, 118 people with (CKD- HD) and Hb levels of <9.0 g/dl (<90 g/l) were randomly assigned to receive placebo, ESA for a Hb target of 9.5–11.0 g/dl, or ESA for a higher Hb target of >11.0 g/dl. After 8 weeks, a higher proportion of participants was transfused in the placebo group versus the group with the Hb target of 9.5–11.0 g/dl and a target Hb >11.0 g/dl. In addition, improvements in fatigue, physical function, and 6-minute walk tests were observed for the group with the Hb target of 9.5–11.0 g/dl as compared with placebo. (60,61)
People with cardiovascular disease or congestive heart failure may be at the lower end of the Hb range at initiation and maintenance of ESA therapy. In a study of 1233 people with (CKD-HD) and congestive heart failure or ischemic heart disease were people assigned to receive epoetin alfa to maintain a Hb of 14.0 g/dl versus 10.0 g/dl [100 g/l], people in the high Hb arm had a lower risk of RBC transfusions and higher physical functioning as compared with the low Hb arm. However, the number of deaths, nonfatal myocardial infarctions, and vascular access thromboses were higher in the high Hb arm compared to the low Hb arm. (62)
▪️ 3.1.4: In people with CKD not receiving dialysis, selection of Hb concentration at which ESA therapy is initiated should consider the presence of symptoms related to anemia, the benefits of higher Hb concentration, and the potential harms of RBC transfusion or receiving ESA therapy.
Conditional Recommendation
Very low quality evidence
Rationale
RCTs of ESA treatment among people with CKD not receiving dialysis( CKD-ND )did not reveal a survival benefit or improvement in cardiovascular outcomes for higher versus lower Hb targets.(63, 64) People with anemia and CKD not receiving dialysis experienced a greater risk of a composite of death or serious cardiovascular events when administered ESAs to target higher versus lower Hb levels (13.5 g/dl vs. 11.3 g/dl), without an incremental improvement in the QoL.( 65). The risk of stroke, prespecified as a secondary outcome, was significantly higher in people with diabetes and CKD not receiving dialysis and treated with ESA to target a Hb level of 13.0 g/dl. (65) In clinical trials comparing specific Hb targets, ESA regimens used to target higher Hb were associated with a lower risk of RBC transfusions. (66)
The Hb concentration at which ESA therapy is initiated in people with CKD not receiving dialysis should be individualized to balance the potential QoL benefits of ESA treatment among people with anemia-related symptoms against potential harms of stroke and other MACE in high-risk groups. The increased risk of RBC transfusions associated with initiating ESA at lower Hb concentrations should be considered in younger people and those being considered for kidney transplantation. (16)
3.1.5: In adult patients with anemia of CKD you should not routinely correct Hb to normal levels of 13gldl with ESAs therapy.
High quality evidence
Rationale
Besarab et al (62) reported a study of normalization of hemoglobin in 1233 prevalent CKD HD patients with high cardiovascular risk on hemodialysis. Normalization of hemoglobin showed no benefit in risk reduction but did show an improvement in quality of life. The treatment arm showed a trend towards increased risk of death, so the study was terminated early.
Two studies evaluated the effect of ESA on patients not yet on dialysis( CKD- ND) CHOIR (64) and CREATE. (63) The outcome of the CHOIR study showed no benefit of higher Hb outcome in CKD patients (eGFR 15-50ml/min) to Hb of 11.3g/dL vs 13.5g./dL. Higher outcome target Hb had an increased risk (using composite end-points of death, myocardial infarction, or hospitalization for congestive cardiac failure) and no incremental improvement in quality of life. (64)
The CREATE (63) study reported that early correction of anemia to normal Hb (130-150g/L vs. 105-115g/L) did not reduce risk of cardiovascular events. Indeed, the hazards ratio for primary endpoints of death from any cause or death from cardiovascular disease consistently (but not significantly) favored the lower hemoglobin target group.
In TRATE study, 4038 patients with diabetes, chronic kidney disease not on dialysis, and anemia, were randomly assigned in a 1:1 ratio to darbepoetin α, to achieve Hb level of approximately 13gd/L or to placebo, with rescue darbepoetin α when the hemoglobin level was less than 9 g/dL. were the composite outcomes of death or a cardiovascular event (nonfatal myocardial infarction, congestive heart failure, stroke, or hospitalization for myocardial ischemia) and of death or end-stage renal disease. After a median follow up of 29 months, there was no difference between the two arms in the primary outcome of death, cardiovascular event or end stage renal disease. Fatal or nonfatal stroke occurred in 101 patients assigned to darbepoetin α and 53 patients assigned to placebo (.65)
3.2 ESA maintenance therapy
3.2.1: We recommend a hemoglobulin target between 10-11.5 g/dl when treating adult CKD patients with ESAs.
Strong Recommendation
High quality evidence:
Rationale
Maintaining a Hb higher than 11.5 g/dl (115 g/l) with ESA therapy does not improve survival in people with anemia in (CKD- HD) or (CKD- ND) not receiving dialysis and may result in adverse cardiovascular outcomes such as stroke. The potential for further improvement in QoL when Hb levels are maintained above 11.5 g/dl (115 g/l) is uncertain and, in some trials, was not considered clinically significant. This recommendation attempts to balance the benefits of ESA treatment to maintain a higher Hb target against its harms (.63, 65)
Current targets that aim for partial correction of Hb are based on clinical trials conducted several years ago. (63, 64,65) These trials compared higher versus lower Hb targets achieved using ESAs, revealing that major adverse cardiovascular events (MACE), mortality, and thrombotic events were more common among patients assigned to the higher Hb targets. In addition, one trial comparing a high Hb target with placebo (and a conservative rescue strategy) in CKD patients with diabetes not on dialysis found an increased rate of stroke. (64)
In large RCT of 1233 participants with (CKD- HD) and congestive heart failure or ischemic heart disease did reveal that the incidence of deaths, non-fatal myocardial infarctions, and vascular access thromboses were higher in people in the high Hb arm (14.0 g/dl [140 g/l]) versus the low Hb arm (10.0 g/dl [100 g/l]). (62)
In determining target Hb it is important to assess potential benefits (in terms of possible improved survival improvement in health-related quality of life (HRQoL) and avoidance of transfusion requirement and hospitalization) vs. potential harms (increased mortality, increased risk of vascular events). ( 68)
3.2.2: In all adult patients, we recommend against using ESAs to intentionally increase the Hb above 13g/dl.
Strong Recommendation
High Quality Evidence:
Rationale
The Medicines and Healthcare products Regulatory Agency (MHRA) guidance (2007) notes that using ESAs to achieve Hb levels greater than 12 g/dL is associated with an increased risk of death and serious cardiovascular events in people with CKD. The MHRA advises that patients should be monitored closely to ensure that the lowest approved dose of ESA is used to provide adequate control of the symptoms of anemia. (68)
In a meta-analysis comparing possible adverse events related to ESA therapy, The higher Hb concentrations in ESA treated CKD patients increased risk for stroke (RR 1.51, 95% CI 1.03–2.21), hypertension (RR 1.67, 95% CI1.31–2.12), and vascular access thrombosis (RR 1.33; 95% CI 1.16–1.53), and possibly the risk of death (RR1.09; 95% CI 0.99–1.20), serious cardiovascular events (RR 1.15, 95% CI 0.98–1.33) or ESRD (RR 1.08; 95% CI0.97–1.20).( 69)
In the TRATE study, there was an increased risk of stroke in the high ESA group (HR 1.92; 95% CI 1.38–2.68), 5.0% of the high Hb group had a stroke compared to 2.6% in the placebo group(P<0.001). Venous thrombo-embolic events occurred significantly more frequently in the high Hb arm (2.0%) compared to the placebo arm (1.1%, P=0.02). (65)
Conditional Recommendation
Low quality evidence
Rationale
ESA dose adjustment may be higher during initiation (or titration after switch between different ESAs) than maintenance phases of ESA therapy. In HD patients, withholding ESA doses for Hb levels greater than the target is associated with subsequent downward Hb excursions often to levels less than target range. The time between withholding ESA doses and return of Hb to target range is variable and unpredictable. In HD patients with Hb values greater than14 g/dL, the median time for Hb to return to 12 g/dL or less after withholding of a SC-administered ESA is 7-9 week. (78)
3.3: ESA dosing, frequency, route of administration, and monitoring
3.3.1: Choice of ESA: In adults with anemia and CKD G5HD the decision of the choice of ESA is based on local availability of ESAs, the target Hb response achieved, route of administration and cost
Rationale
Many studies have been published comparing different ESA products against each other when used at different dosing intervals, by different routes of different administration and in different groups. All the available products are efficacious when administered according to the manufacturer’s recommendations. (73) Higher doses of epoetin are required when administered via i.v. as compared with s.c.,by 30% which in turn will increase costs. However, people with (CKD- HD) may prefer an i.v. route to reduce injection pain.
The objective of initial ESA therapy is a rate of increase in Hb concentrations of 1 to 2 g/dl per month This is consistent with the findings in ESA trials of CKD- associated anemia where the mean initial rates of Hb concentration increase were of 0.7 to 2.5 g/dl (7 to 25 g/l) in the first 4 weeks However, a rise in Hb of greater than2.0 g/dl (20 g/l) over a 4-week period should be avoided. (74) In adults and with anemia and (CKD-ND), (CKD -PD), or kidney transplant recipients receiving ESA therapy, administer ESA by the subcutaneous route.
3.3.2: Hb concentration should be monitored every 2–4 weeks in the correction phase and every 1–3 months for stable patients in the maintenance phase, for (CKD- HD) measure Hb concentration every month.
Conditional Recommendation
Moderate quality evidence:
Rationale
It is important to closely monitor Hb response to treatment to detect rapid rises in Hb to prevent overshooting of Hb targets. RCT data indicate an increased risk of adverse events such as hypertension and cardiovascular events with high Hb levels (.65, 64) In the Correction of Hemoglobin and Outcomes in Renal Insufficiency (CHOIR) study, people with CKD randomized to a Hb target of 13.5 g/dl had a higher risk of a composite of death and cardiovascular events as compared with a Hb targets of 11.3 g/dl, (64). In the TRATE study, the risk of stroke was higher in people with CKD randomized to darbepoetin to maintain a Hb level at approximately 13.0 g/dl vs to placebo group. 65 More frequent Hb monitoring may be needed for patients with unstable Hb out of target Hb level, anticipated Hb drop due to blood loss/hemolysis, infection or suboptimal dialysis. (73)
A minimum frequency of 1–3 months is suggested, with more frequent monitoring among people with CKD HD where trial data shows dose adjustments were required in 40%–50% of people during the maintenance phase of ESA therapy (76) to avoid overshooting the Hb beyond target, as well as being able to identify ESA hyporesponsiveness.
3.3.3: In people with anemia and CKD treated with ESA, avoid adjusting the dose of ESA more frequently than once every 4 weeks. The exception is when Hb increases by more than 1.0 g/dl (10 g/l) in 2–4 weeks after initiation of therapy, at that time the dose should be reduced by 25%–50%
Good Practice Statement
Initial therapy with ESA aims to increase the Hb concentration by 1.0 g/dl (10 g/l) per month, which is consistent with the findings in clinical trials that used ESA to treat anemia in people with( CKD -HD) and (CKD- ND) not receiving dialysis. Initial rates of Hb concentration increase were 0.7–2.5 g/dl (7–25g/l) in the first 4 weeks. However, a rise in Hb of >2.0 g/dl (20 g/l) over a period of 4 weeks should be avoided to reduce the likelihood that concentrations will exceed11.5 g/dl (115 g/l), which may increase the risk of hypertension and/or stroke, (64.65)
(Table-4) Dosing of erythropoietin-stimulating agents (ESAs)
|
ESA Agent |
Initial Dose |
Dose Adjustment |
|
Epoetin alfa and beta |
CKD not receiving dialysis: 4,000 or 10,000 units weekly or every 2 weeks
CKD G5D: 50-100 units/kg, 3 times weekly (may round to convenient dose in units) |
CKD not receiving dialysis: Increase or decrease dose and/or dosing frequency as needed (generally not given more than once per week)
CKD G5D: Increase by 25 units/kg/dose if Hb rise is < 1.0 g/dl (<10 g/l) after 4 weeks. Reduce by 10–25 units/dose if Hb rise is >2 g/dl (20 g/l) in 4 weeks |
|
Erythropoietin biosimilars |
Product names and doses vary by region - Refer to individual product information |
|
Good Practice Statement
Rationale
Clinical trials of ESA therapy revealed an increased risk of stroke, vascular thrombosis, and nonfatal myocardial infarction. (65 ,62) One in 4 stroke survivors will have another stroke. In addition, the risk of vascular access thrombosis and future thromboembolic events is increased in people with a prior history of these events. For these reasons, holding of ESA treatment should be considered in people with a history of these events. Reinitiation of ESA therapy should be based on shared decision-making after discussion of benefits and risks. (65)
3.3.5: We recommend exerting extreme caution while prescribing ESA therapy in CKD patients with a history of stroke, or malignancy, particularly in those with active malignancy when cure is the anticipated outcome.
Strong Recommendation
High quality evidence
Rationale
The joint guideline from the American Society of Clinical oncology and American Society of Hematology recommends using ESA therapy with great caution in patients active malignancy, particularly when cure is the anticipated outcome .(69 ,70) This advice is supported in CKD patients by the post-hoc analysis in TRATE study which demonstrated a significantly higher death rate from cancer(7.4%) in the darbepoetin arm in patients with a history of a malignant condition at baseline as compared to(0.6%) in the placebo arm .(65)
NICE evaluated the efficacy and safety of ESAs in treating anemia in cancer patients receiving chemotherapy. In total 16 studies were included in the analysis of the outcome related to anemia and 7 trials in the outcome related to overall survival. NICE analysis of available trials concluded that ESAs are recommended, within their marketing authorizations, as options for treating anemia in people with cancer who are having chemotherapy. ESAs were effective in increasing hemoglobin concentrations, improving hematological responses, reducing the need for transfusions and improving health-related quality of life, but that it could not assume that either prolonged or shortened survival compared with treatment without an ESA. ( 72)
3.4: ESA Hyporesponsiveness
3.4.1: In patients with anemia and (CKD-HD), or anemia of (CKD-ND) with initial or subsequent ESA hyporesponsiveness, identify and treat the underlying causes of ESA hyporesponsiveness, if possible
Good Practice Statement
Rationale
Hyporesponsiveness in CKD patients with previously stable Hb values should lead to an intensive search for potentially correctable factors which might be causally involved. Unfortunately, besides iron deficiency, there are only few other easily reversible factors that contribute to ESA hyporesponsiveness Hyporesponsiveness could be initial If no increase in Hb concentration from baseline after the first month of ESA treatment on appropriate weight-based dosing. Or acquired if after treatment with stable doses of ESA, they require increases in ESA doses up to 50% beyond the dose at which they had been stable Hb concentration. ESA hyporesponsiveness can be acute or chronic (>4 months) (79, 80)
The most common causes of ESA hyporesponsiveness are inflammation and iron deficiency. (table 5) Inflammation suppresses erythropoiesis via cytokine-mediated effects on bone marrow, EPO-responsiveness and synthesis, iron restriction (as a consequence of elevated serum hepcidin levels), and other mechanisms. (81) These mechanistic concepts are supported by clinical studies, which demonstrated that higher serum levels of inflammatory markers, such as CRP and IL-6, as well as iron-regulatory peptide hepcidin were associated with and/or predict increased ESA requirements in people receiving or not receiving dialysis. (82,83)
Recent studies have suggested that causes of ESA hyporesponsiveness cannot be identified in approximately 30% of people with anemia and CKD. (84) ESA hyporesponsiveness is also often transient and sustained. ESA hyporesponsiveness in people with CKD not receiving dialysis is rare in the absence of iron deficiency, hemoglobinopathies, myelofibrosis and other hematological diseases. (80)
table5, Causes of erythropoiesis-stimulating agents (ESA) hyporesponsiveness
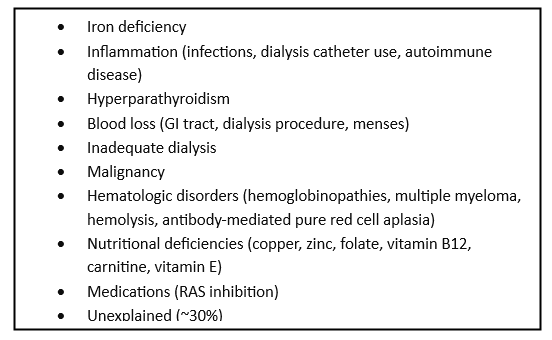
GIT, gastrointestinal tract; RAS, renin -angiotensin system
chapter 4. Novel anemia therapies: hypoxia-inducible factor prolyl hydroxylase inhibitors HIF-PHIS
4.1: Treatment initiation and maintenance
4.1.1: Do not use ESAs and HIF-PHIs in combination in people with anemia and CKD, including those with ESA hyporesponsiveness
Good Practice Statement
Rationale
No RCTs have investigated the efficacy or safety of combining ESA with HIF-PHIs.only one small study in 9 PD with ESA hyporesponsiveness, they used roxadustst 6 of them their ESA dose was reduced. However, the authors did not believe that there was a sufficiently reasonable rationale using them together. (91)
Good Practice Statement
Rationale
The safety and benefits of HIF-PHI in people with ESA-hyporesponsiveness have not been established; few, if any, data support their use. People with ESA hyporesponsiveness are at increased risk for cardiovascular events, kidney failure, and death. (85) Given the cardiovascular safety concerns raised in large global cardiovascular safety trials (86,87) HIF-PHI use in people with CKD and ESA hyporesponsiveness may further increase their pre-existing risk for serious cardiovascular events. (88)
Good Practice Statement
Rationale
In the absence of evidence that treatment improves clinically relevant outcomes and with limited data about the risks of HIF-PHI treatment in this patient population, the lowest possible dose should be used to alleviate symptoms due to anemia and/or to achieve a Hb level that might reduce the need for RBC transfusion rather than using HIF-PHI to try attaining the same Hb level that might be targeted in people with( CKD- HD) who are not ESA hyporesponsive.(89,90)
Good Practice Statement
Rationale
In the absence of evidence that HIF-PHI treatment in these people confers any benefit other than a small increase in Hb in some people, and given the uncertainty as to the risks of such treatment, it seems that to use the lowest possible HIF-PHI dose and discontinue treatment after 4 months if there has not been a meaningful increase in Hb. (16, 91)
4.1.5: In people with anemia and CKD, the Hb thresholds for the initiation and maintenance of HIF-PHIs are unknown, but it is reasonable to use the same Hb thresholds as those recommended or suggested for ESA therapy
Good Practice Statement
Rationale
No RCTs have been performed to date to establish new thresholds/targets for HIF-PHI therapy. All RCTs on HIF-PHIs based on the same Hb thresholds the same as for ESA therapy. (16 )
4.1.6: In people with anemia and CKD, dose HIF-PHIs according to the recommended starting doses as shown in this table if they are available (table 6) (Good practice statement)
|
Roxadustat |
CKD not receiving dialysis and CKD G5D (ESA-naïve): [EU] 70 mg for body weight <100 kg, 100 mg for body weight >100 kg
CKD not receiving dialysis (switch from ESA): [EU] 70–200 mg, [Japan] 50 mg (ESA-naïve), 70–100 mg (switch from ESA) |
3.0 mg/kg body weight |
3 times per Week |
CYP2C8, UGT1A9, BCRP, OATP1B1, OAT1, OAT3122 inhibitor of: CYP2C8, BCRP, OATP1B1, OAT3 |
Egypt |
Good Practice Statement
Rationale
The use of ESAs to target higher Hb levels has been associated with harm and HIF-PHIs have not been shown to be safer than ESA. Among people with CKD not receiving dialysis, there is even more some possibility that HIF-PHIs are associated with a higher risk of MACE and vascular access thrombosis than ESAs. (54 ,55,58)
Good Practice Statement
Rationale
Higher HIF-PHI doses may result in adverse events as it increases risk of MACE, and vascular access thrombosis and cancer. (54, 55)
4.2. HIF-PHI monitoring
4.2.1: In people with anemia and CKD, when dosing HIF-PHIs, monitor the Hb levels 2–4 weeks after initiation or dose changes and subsequently, every 4 weeks during therapy.
Rationale
The ideal frequency of monitoring is uncertain a big effort should be done to reduce the risk of overshooting the Hb target, one study of vadadustat in (CKD-ND), for example, required dose adjustments in 12.5%–54.4% (0–8 weeks) and in 11.5%–38.5% (8–24 weeks) on biweekly monitoring, to increase or maintain Hb, respectively. (93)
Good Practice Statement
Rationale
Factors affecting hyporesponsiveness to HIF-PHIs are not clearly defined. In the majority of clinical trials of HIF-PHIs, increases and stabilization of Hb are achieved within 6–16 weeks after initiation of therapy, both in people who are ESA-naïve or after conversion from ESA to HIF-PHI. Due to insufficient clinical information on the long-term safety of HIF-PHIs, other therapeutic options, such as ESAs, may be considered in cases of insufficient erythropoietic response to HIF-PHIs. (93)
4.2.3: In people with anemia and CKD, suspend treatment with HIF-PHIs in those who experience cardiovascular events (e.g., stroke, myocardial infarction); thromboembolic events (e.g., deep vein thrombosis, pulmonary embolism); vascular access thrombosis; or newly diagnosed cancer.
Good Practice Statement
Rationale
This practice point is based on insufficient clinical information regarding the long-term safety of HIF-PHIs, which include risks of cardiovascular events, stroke, thromboembolic events and cancer progression or recurrence. (table7)(.93,95)
|
Theoretical risk or experimental evidence of risk for disease development or progression |
Concern for risk based on adverse event profiles in clinical trials |
Insufficient data for risk assessment; dedicated studies needed |
|
• Active cancer or with a history of cancer not in complete remission for at least 2–5 years (based on trial exclusion criteria)94 • Polycystic kidney disease117 • Proliferative retinal disease118 • Pulmonary arterial hypertension119 • Pregnancy* |
• Prior cardiovascular events (i.e., stroke, myocardial infarction)94 • Prior thromboembolic events (i.e., deep venous thrombosis, pulmonary embolism)94 • Prior vascular access thrombosis94 • Hepatic impairment† • • Seizures, exfoliative dermatitis, hypothyroidism, bacterial infections/sepsis (roxadustat)116 |
• Post-kidney transplant anemia94
|
*HIF-PHIs are contraindicated in pregnancy, please refer to package inserts for individual compounds.
†Caution is advised in patients with hepatic impairment. HIF-PHIs are not recommended for patients with significant hepatic impairment. Please refer to package inserts of individual compounds for specific guidance.
chapter 5. red cell transfusion in chronic anemia
Moderate quality evidence:
Rationale
The risk of sensitization after RBC transfusion has probably decreased over time, at least partly due to changes in blood transfusion practices and the use of more precise methods to measure allosensitization. However, the risk of allosensitization with RBC transfusion is not exactly known, but generally, an overall response rate ranging from 2%–21% has been reported.( 96, 97) .The annual report of the USRDS 2010 showed that the risk of allosensitization with RBC transfusion is substantial; people who received transfusions have an odds ratio (OR) of 2.38 for having panel reactive antibody (PRA) >80%.,(98) conclusions from previous studies include the following: a) washed RBC do not appear to be less immunogenic than nonwashed RBCs;( 99) b) no consistent reduction in sensitization has been demonstrated with donor-specific and HLADR matched transfusions; 100,101 c) higher numbers of RBC transfusions have been associated with an increased risk of sensitization in some studies, (112, 103), but not in others.( 99, 104)
A systematic review by Scornik et al. identified 180 eligible studies from 1984 to 2011. He reported that alloimmunization was significantly more common in people with CKD receiving a pretransplant blood transfusion compared with people with CKD not being transfused. (105). In addition, the risk of allosensitization was also determined by the number of RBC transfusions, with an increased number of RBC transfusions increasing the risk of allosensitization. Allosensitization was linked with higher rates of graft rejection and lower rates of graft survival compared to people who are non-sensitized.
Potential harms of RBC transfusions are infrequent and encompass transfusion errors, infection, transfusion-related acute lung injury [TRALI], transfusion-associated circulatory overload [TACO], hemolytic transfusion reactions, febrile nonhemolytic transfusion reactions, iron overload (with chronic transfusion dependence), volume overload, citrate toxicity (leading to metabolic alkalosis and hypocalcemia), coagulopathy, allosensitization, allergy, coagulopathy, hypothermia, hyperkalemia, and health-related errors. Most of these potential harms are uncommon. (108,109)
· ESA or HIF-PHI therapy is ineffective (e.g., hemoglobinopathies, bone marrow failure, ESA or HIF-PHI resistance)
· ESA or HIF-PHI therapy is harmful (e.g., previous or current malignancy, previous stroke).
· In life threatening conditions.
Good Practice Statement
Rationale:
For people with CKD and chronic anemia, RBC transfusion can be considered in states of ESA or HIF-PHI hyporesponsiveness, such as in bone marrow failure, hemoglobinopathies, and ESA or HIF-PHI resistance settings, or if the potential risks of ESA or HIF-PHIs outweigh the benefits, such as people with current or previous malignancy.
According to the 2023 Annual Report of the USRDS, (109) the mean Hb among people with incident kidney failure was 9.4 g/dl (94 g/l), and the percentage of patients with Hb <9g/dl (90 g/l) at onset of kidney failure was >30%. Fewer than 1 of 6 people with incident kidney failure had received ESAs prior to initiating dialysis, despite the large percentage of people with CKD having a low Hb level. Those with Hb <9 g/dl (90 g/l) were 4 times more likely to have received an RBC transfusion than those with Hb 9–<10 g/dl (90–<100 g/l). RBC transfusions were more common than ESA use in with CKD G 4 and were almost as common as ESA use in people with CKD G5. This finding underscore that anemia is undertreated prior to the onset of kidney failure, and undertreatment may lead to high rates of RBC transfusion, which in turn has negative consequences, especially for people who are eligible for kidney transplantation. (109).
The magnitude of the potential harms of transfusion (e.g., from infection) and some of the benefits from ESAs and HIF-PHIs (e.g., transfusion avoidance) are dependent on the threshold for transfusion. If that threshold is high (i.e., transfusion is reserved until symptoms become severe or the Hb reaches a very low level) the risks related to transfusion will be low and the benefit of ESA or HIF-PHI therapy in avoiding transfusions will be small. (16)
When rapid correction of anemia is required to stabilize the patient’s condition (e.g.
acute hemorrhage, unstable coronary artery disease), and when rapid preoperative Hb correction is required
Good Practice Statement
Rationale
In certain urgent clinical situations, RBC transfusion may be needed for the immediate correction of anemia. The Hb threshold for transfusion in this situation is uncertain especially as there is a paucity of randomized studies evaluating thresholds for RBC transfusions specifically in people with CKD
A Cochrane review involving 48 RCTs with 21,433 people across different clinical settings showed that a restrictive transfusion strategy (using a Hb threshold of most commonly7.0–8.0 g/dl decreased proportion of people exposed to RBC transfusion to 41% compared to the liberal transfusion strategy (using generally a Hb threshold of 9–10 g/dl) Importantly, the restrictive RBC transfusion strategy did not impact 30-day. mortality, or morbidity (i.e., cardiac events, myocardial infraction, stroke, pneumonia, thromboembolism, infection) compared with a liberal transfusion strategy. (110). The results of this Cochrane library review are also applicable for people with CKD as none of the individual studies excluded people with CKD.
Restrictive transfusion strategy can be used when hemoglobin level is less than 7.5 g/dL for patients undergoing cardiac surgery, less than 8 g/dl for those undergoing orthopedic surgery or those with preexisting cardiovascular disease. (111) These thresholds reasonable guides to consider RBC transfusion, but symptoms and signs caused by anemia should also be considered when transfusing CKD patients.
RBC transfusion should be considered in acute clinical situations where delaying anemia correction may lead to serious outcomes, including the imminent risk of death. These acute clinical situations include, but are not limited to, severe acute hemorrhage from gastrointestinal, genitourinary disorders, or other causes, unstable coronary artery disease, and preoperative situations necessitating rapid Hb correction.
The K-DOQI anemia guideline recommends that no single Hb concentration justifies or requires transfusion and the target Hb recommended for chronic anemia management should not serve as a transfusion trigger. (113)
. NICE guideline agrees that there are clinical reasons to minimize blood transfusion in anemia of CKD and if blood transfusion is essential the relevant hematology guidelines should be followed (e.g. the British Committee for Standards in Hematology (BCSH) guidelines www.bcshguidelines.com.120 In hospitalized patients who are hemodynamically stable, the need for transfusion is directed by symptoms and the Hb values. A value in CKD patients of <70g/L or <80g/L in post-operative surgical patients or pre-existing cardiac disease should prompt transfusion. (114)
5.4: In people with anemia and CKD, the decision to transfuse should be based on symptoms and signs caused by anemia rather than an arbitrary Hb threshold.
Good Practice Statement
Rationale
There is a paucity of RCT data evaluating transfusion thresholds in people with CKD and chronic anemia. The current daily practice is that RBC transfusion in CKD is performed as a target Hb-driven approach or during acute illnesses.,(109) The latter was shown in a Canadian study involving people receiving outpatient dialysis in which a low Hb value was the reason for RBC transfusion (92%), whereas only 4.5% of patients had symptoms of severe anemia necessitating RBC transfusion.,(115) In a choice-based survey in the Veteran Administration System on the decision to transfuse people with anemia receiving dialysis, absolute Hb level was the most important consideration (29%), followed by patient functional status (16%).(112)
Anemia related symptoms such as dyspnea and fatigue are nonspecific and may occur at different Hb levels in different people. So, anemia-related signs and symptoms be the primary trigger for deciding when to give RBC transfusions rather than an arbitrary Hb threshold. (16)
5.5 Consider implementing strategies at the individual, organizational, and public health policy levels to reduce RBC transfusions in people with CKD
Good Practice Statement
Rationale:
Consider implementing strategies at the individual, organizational, and public health policy levels to reduce RBC transfusions in people with CKD. There are different strategies to reduce blood transfusion such as, 16,108
• Option for less invasive procedures in hospitalized patients whenever possible.
• Limit blood sampling when medically appropriate.
• Continue ESA/HIF-PHI/iron therapy in hospitalized patients unless clinically contraindicated.
• Consider Hb trend over time rather than absolute Hb values, in people using ESA/HIFPHI/iron therapy.
• Avoid RBC transfusion in patients with chronic anemia who are asymptomatic.
• Individualize transfusion need based on the clinical situation.
• In every person with CKD patient, triage the decision for RBC transfusion on whether the person is a potential future transplant
• Brenner N, Kommalapati A, Ahsan M, et al. red cell transfusion in chronic kidney disease in the United States in the current era of erythropoiesis stimulating agents. J Nephrol 2020; 33: 267-275.
Research recommendations
· Studies are needed to evaluate the prevalence of iron overload in people with CKD on iron therapy, how it should be detected, and what thresholds are associated with toxicity.
· Studies are needed on iron treatment in people with CKD with iron deficiency in the absence of anemia.
· Investigate the long-term risks and benefits of treatment with HIF-PHI versus ESA in adults with CKD5D and CKD not receiving dialysis.
Clinical monitoring and evaluating the impact of the guideline
· There are potential indicators that can be used to monitor and evaluate management of anemia in CKD patients
v Indicators that should be used at the initiation and follow-up of the treatment
· CBC, CRP, serum iron, transferrin saturation (TSAT), serum ferritin.
v Circumstances warranting more frequent iron testing
• Initiation of or increase in dose of ESAs or HIF-PHIs
• Episodes of known blood loss
• Recent hospitalization
• Important increase in ferritin or TSAT or overshooting target limit