Infertility in she camel
- A. Repeat Breeding Syndrome
It is generally defined as any camel that failed to conceive after at least three regular spaced services, with no clinical abnormalities. It may be caused by different affections
I. Ovarian Affections
It includes ovarian cysts (follicular, luteal cysts, hemorrhagic), ovarian agenesis, ovarian hypoplasia, and Ovarian hydrobursitis.
1.1- Ovarian cysts
Cystic ovarian disease (COD) is a significant ovarian dysfunction resulting from disruptions in the hypothalamic-pituitary-gonadal axis due to either endogenous or exogenous factors. a study by (Hegazy et al., 2001) indicates that the incidence of cystic and inactive ovaries in female camels increases during summer. When a dominant follicle is present without mating, it can lead to one of two outcomes: either regression of the follicle or cystic degeneration, resembling an ovulatory follicle. According to (Dawod and Hamed, 2018), the types of ovarian cysts are categorized as follows:-
1.2- Follicular cysts
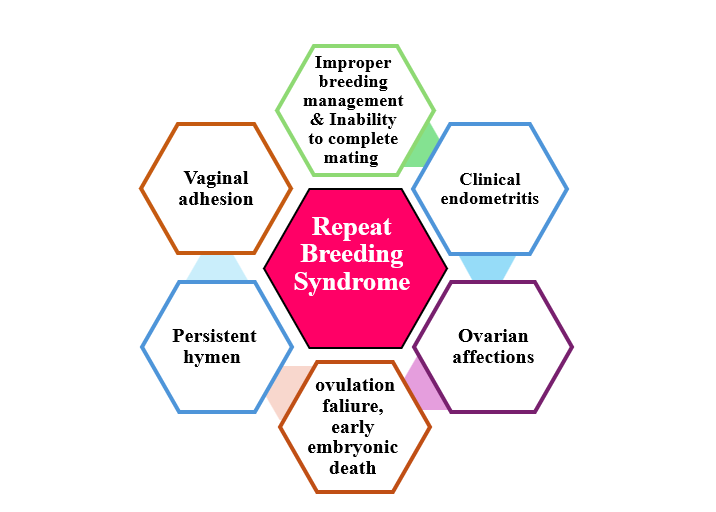
It may be unilateral or bilateral either single or multiple cysts, but mostly in a single manner. It is thin-walled, well-vascularized, or slightly opaque and filled with a straw-colored serous fluid. The diameter ranged from 17-40 mm (Fig. 2).
1.3- Luteal cysts
It is thick-walled and becomes partially or totally opaque, tense in consistency, with a grayish-yellow color. The follicular fluids reach 22 ml. The diameter reaches up to 50 mm.
1.4 Hemorrhagic cysts
It is a single, thick wall, unilateral or bilateral, and contains bloody follicular fluid that reaches about 8 ml. The diameter ranged from 10-25 mm.
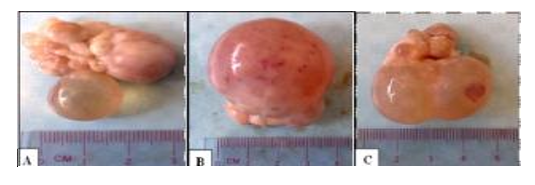
Figure 2. Ovary containing Follicular cyst characterized by a large, thin wall containing serous, clear follicular fluid (A) single small cyst (B) large cyst 40 mm in diameter (C) double cyst (Dawod and Hamed, 2018).
2- Ovarian agenesis
It is the complete absence of ovaries. It may be unilateral or bilateral (Fig. 3). The unilateral ovarian agenesis is characterized by the presence of a large bulging follicle on the right ovary and a small fatty mass on the left one. The bilateral ovarian agenesis is characterized by ending of the fallopian tube in a well-developed bursa that contains a small fatty tissue mass like the pea size while the rest of the genital tract is normal (Dawod and Hamed, 2018).
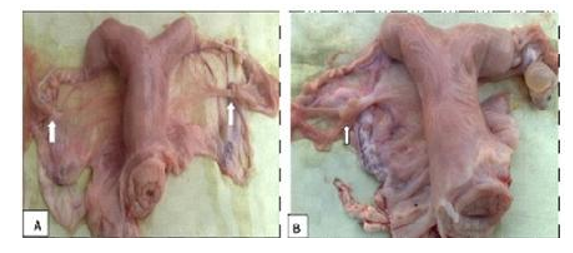
Figure 3. Ovarian agenesis (A) bilateral, (B) left unilateral agenesis with a normal right ovary, and has a large follicle (Dawod and Hamed, 2018).
3- Ovarian hypoplasia
It is characterized by the absence of ovarian follicular activity due to genital and chromosomal abnormalities (73XO, 75XXX, 74XX/74XY, minute chromosome) (Tibary et al., 2011). The ovaries are small, thin, and firm structures without any small follicles, while the rest of the genital tract is normal (Fig. 4) (Dawod and Hamed, 2018).
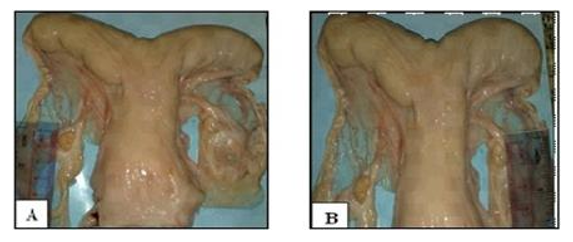
Figure 4. Ovarian hypoplasia (A) left ovary 10 mm (B) right ovary 8 mm in length (Dawod and Hamed, 2018).
Diagnosis:
· The history of multiple matings/continuous receptivity, or persistent rejection of the male.
· Transrectal ultrasonography demonstrates a small uterus and either small follicles that do not progress to a dominant size or an inability to visualize the ovaries entirely.
· Laparoscopic examination to confirm the case.
4- Ovarian hydrobursitis
The camelid's ovary is completely covered with a thin fold of the mesosalpinx, the ovarian bursa. The apex of this bursa forms a large circular orifice within which lie the fimbriae of the oviduct (Fig. 5a–c). In most cases (85%), the ovary was freely movable and could be easily uncovered from the bursa. In about 15% of cases, the bursa appeared as a large sack filled with different amounts of fluid of different physical characters (Fig. 5d–f). The mean diameters of these bursae were 35.18 ± 5.2 × 15.12 cm. On transrectal palpation, the ovarian hydrobursitis (21.8%) was suspected when the genital tract was difficult to retract, and the encapsulated ovary was not palpable (Fig. 5g). on ultrasonographic examination, a large well-demarcated, hypoechogenic sac was found lateral to or beneath the corresponding uterine horn (Fig. 5h, i). In many cases (68.4%) the ovary appeared as a floating structure and was easily identified when it was functionally active. In the other cases (30.6%), the ovary adhered to the bursal wall (Fig. 5j).
Ovarian hydrobursitis is a peculiar disease of the ovarian bursa, characterized by adhesion of the ovarian bursa, fluid accumulation, and encapsulation of the ovary (Fig. 6). It is initially an inflammatory process, and the accumulated bursal fluid is partially originates from the follicular fluid. It is associated with peri-uterine adhesion (vagina/cervix), pyometra, and Paraovarian cysts (Tibary and Anouassi, 2001, Ali et al., 2011). The affected female shows long-standing infertility, refuses to mate, repeats breeding with long heat intervals, early embryonic death, and abortion.The incidence of ovarian hydrobursitis was 6.5% in slaughtered camels and 33.8% in infertile females.
Diagnosis
- Rectal examination reveals a cord-like structure was palpated between the ovarian end of the uterus and the corresponding ovaries.
- Ultrasonography presented variable appearances of the ovarian bursa. The bursal fluid appears as clear anechoic fluid with different sizes, and in a few cases, there are echogenic particles in the bursal fluid. In addition, the ovaries carrying different structures appear as floating masses in the bursal fluid (Fig. 7) (Mansour and Karen, 2021).
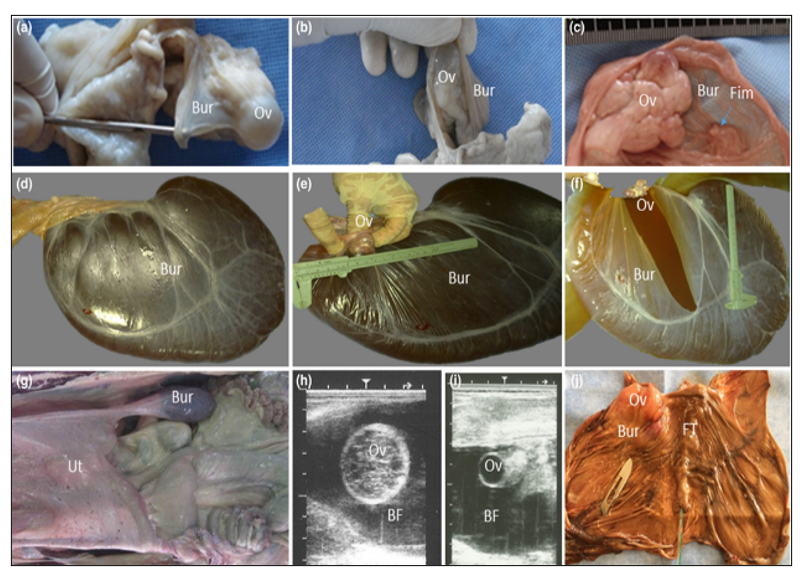
Figure 5. Ovarian bursa in camels: (a, b, c) the ovary is completely covered with a thin fold of the mesosalpinx, and the apex of bursa forms a large circular orifice within which lies the fimbriae of the oviduct (c, arrow). (d–f) A case with ovarian hydrobursitis, the bursa, appeared as a large sack filled with fluid, while the ovary was found floating within the completely closed bursa. (g) On transrectal palpation, the genital tract was hard to withdraw, and the encapsulated ovary was problematic to palpate. (h, i) On ultrasonographic examination, a large, well-demarcated, hypoechogenic sac was found lateral to or beneath the corresponding uterine horn, and the ovary appeared as a floating structure. (j) In some cases, the ovary adhered to the bursal wall. Ov: ovary; Bur: bursa; Fim: fimbria of the oviduct; Ut: uterus; FT: fallopian tube; BF: bursal fluid (Ali and Derar, 2020).
Hormonal and biochemical evaluation of the bursal fluid and its comparison with blood and follicular fluid biochemistry may be useful in clarifying the origin of the bursal fluid.
- Neutrophilia, monocytosis and eosinophilia.
- Bursal fluid had a tendency for high estradiol-17β concentration compared to blood serum. Progesterone and cholesterol concentrations were similar in bursal fluid, follicular fluid and serum.
- Total protein, phosphorus, and magnesium concentrations were greater in the bursal fluid than in serum.
- Histopathology: degeneration and hyperplasia of the lining epithelium, mononuclear cells infiltration, focal aggregation of inflammatory cells, cystic dilatation of multi-acinal structures, tiny hemorrhages, and presence of hemosiderin-laden macrophages.
- Bacterial and protozoal examination may be helpful in explaining the etiopathogenesis of the syndrome.
- Treatment: Surgical ablation in unilaterally affected animals presents potential treatment.
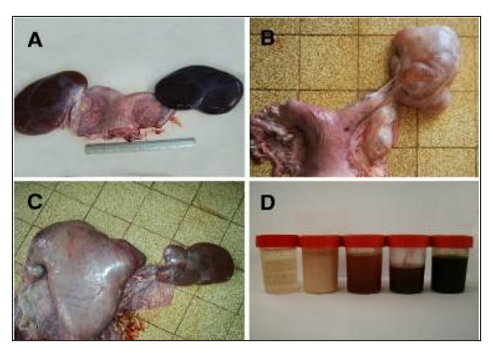
Figure 6. Ovarian hydrobursitis in slaughtered female camels. A, bilateral ovarian hydrobursitis; B, unilateral ovarian hydrobursitis; C, ovarian hydrobursitis in pregnant female; D, different fluids in the bursa (Ali et al., 2011, Benaissa et al., 2014).
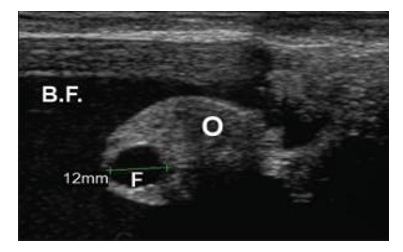
Figure 7. Ultrasound image shows a case of ovarian hydrobursitis. O: ovary; B.F: bursitis fluid; F: Graafian follicle (Mansour and Karen, 2021).
II.Ovulation Failure
It is a common problem in camelids. Anovulatory follicles can become hemorrhagic and, in some cases, luteinize and produce progesterone, resulting in rejection of the male. It occurs due to the lack of luteinizing hormone released after mating (Fig. 8, 9).
Causes:
- Bad breeding time or mating time, in contrast to follicular development.
- The abnormal ovary.
- Males with low potency could not induce the ovulation-inducing factor (OIF) due to the short time of copulation.
- The females with vagina/cervix abnormalities that may inhibit the normal mechanism of induction of ovulation.
- The ovarian follicular activity may be reduced in females that are lactating, obese, heavily parasitized, advanced in age, or have experienced severe
Diagnosis:
- level of progesterone must be kept under check.
- confirmation of ovulation through ultrasonography.
Treatment: Injection of Human chorionic gonadotropin (hCG) or gonadotropin-releasing hormone (GnRH).
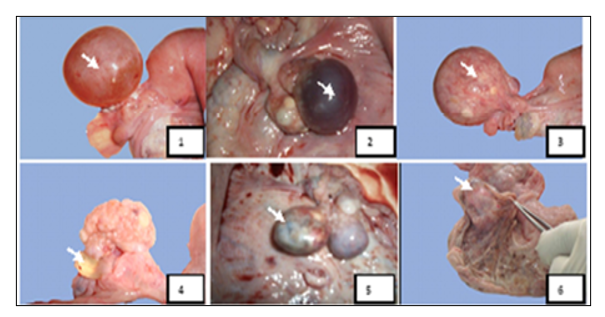
Figure 8: Macroscopic aspects of ovarian affections found in female camels studied at El-Oued slaughterhouse. Key: 1-Follicular cyst, 2-Hemorrhagic cyst, 3-Luteinized follicular cyst, 4-Para-ovarian cyst, 5- Ovarian teratoma, 6- Oophoritis (Gherissi et al., 2019).
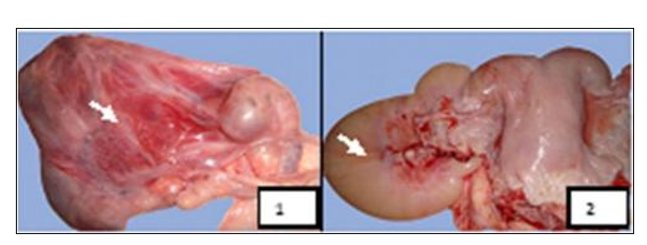
Figure 9: Macroscopic aspects of ovarian bursal affections found in female camels studied at El-Oued Slaughterhouse. Key: 1- Bursitis, 2- Hydrobursitis (Gherissi et al., 2019).
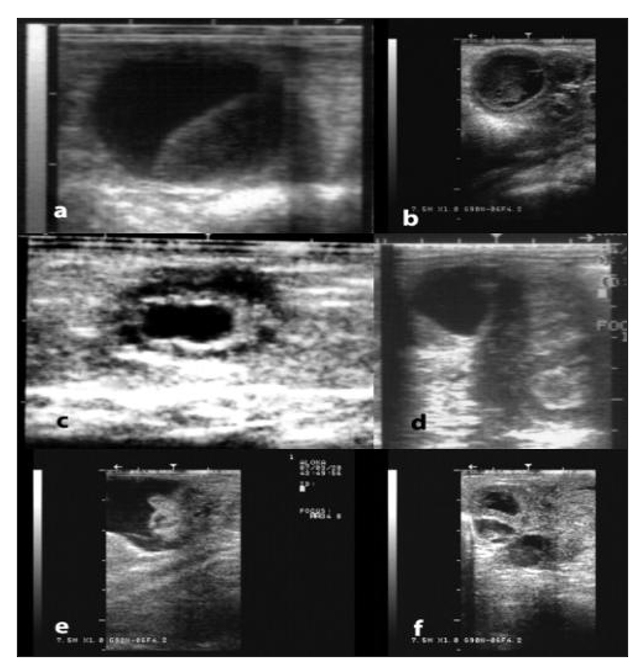
Figure 10: Ultrasonographic appearance of some ovarian and tubal disorders in camelids. a) Large anovulatory follicle, b) Luteinized/hemorrhagic anovulatory follicle, c) Cystic rete ovarii, d) Ovarian teratoma, e) Hydrobursitis, f) Hydrosalpinx (Pearson and Tibary, 2014).
III. Utero-tubal affections
▪️ Hydro-salpinx
The uterine tube is filled with fluids and can be rectally palpated as a tortuous, distended structure near the ovary (Fig. 11, 12). By ultrasonography, the uterus is demonstrated as many hypoechogenic, well-demarcated sacs adjacent to the ovary (Mansour and Karen, 2021).
▪️Clinical endometritis
The uterine inflammation has been described as the most commonly encountered form of infertility in dromedary camels. It can lead to irreversible damage of the salpinx, resulting in a total loss of fertility. It can be classified as acute, sub-acute, or chronic. According to the thickness of the uterine wall and the amount and consistency of the vaginal discharges, endometritis is classified into three degrees (mild degree: uterus of normal consistency with small amount of mucopurulent vaginal discharge; moderate degree: thick-walled uterus with moderate mucopurulent discharge; and severe degree: large-sized uterus with hard consistency and thick or pasty vaginal discharges) (Fig. 13) (Ali et al., 2010).
Causes
- Over-breeding
- Unaddressed postpartum complications
- Improper obstetrical manipulations
- Nutritional deficiencies, such as selenium and copper, may also be linked to an increased incidence of endometritis
Diagnosis
- Observation of vaginal discharges
- Trans-rectal palpation reveals a slight enlargement of the uterine horns
- Vaginal examination: the uterus and/or cervix are enlarged, tough, and have thick wall, with different degrees of vaginal discharges.
- Transrectal ultrasonography: areas of increased echogenicity and thickening of the uterine wall.
- Cytology and culture are necessary in cases of suspected endometritis »»»»» Endometrial biopsy should also be considered in the diagnosis of endometritis and can be a prognostic indicator of future fertility. For camelids, the use of a Turret rectal biopsy punch is recommended. Targeted biopsies can be performed in combination with hysteroscopy. Although a grading system for histological evaluation has been proposed in camelids it is not widely used in a clinical setting. These techniques should be performed when the female has the presence of a dominant follicle and the cervix is open (Table 2).
- Bacteriological culture should include sensitivity testing for the major antibiotics. The most common bacteria isolated from cases of camelid endometritis are Escherichia coli, Streptococcus equi zooepidemicus, β-hemolytic Streptococci, Enterococcus spp., coagulase negative Staphyloccocus spp., Proteus spp, Enterobacter aerogenes, Klebsiella pneumonia, Pseudomonas aeruginosa and Trueperella pyogenes. Venereal transmission should be considered in case of herd infertility or abortion outbreaks. Pseudomonas aeruginosa, Campylobacter fetus fetus, Tritrichomonas foetus, Aspergillus spp., and Mucor spp. have been isolated from infertile camels.
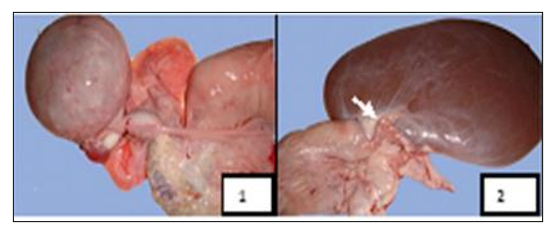
Figure 11: Macroscopic aspects of oviduct affections found in female camels studied at El-Oued slaughterhouse. 1 - Oviduct hypertrophy, 2 - Oviduct torsion (Gherissi et al., 2019).
Table 2. Classification of endometrial biopsy and the potential effect on fertility (Tibary, 2009).
|
Biopsy Category |
Histopathological Characteristics |
Effect on Fertility |
|
Grade 1A |
-Normal endometrium |
-Normal conception rates |
|
Grade 1B |
Few lymphocytes within the endometrium. |
Low-grade infection or remnants of previous inflammation. Mild surface irritations may indicate a reaction to breeding. May be postpartum or post-abortion |
|
Grade 2A to 2B |
Active and acute, chronic, or chronic active endometritis. Chronic inflammation tends to be more deeply located in the endometrium, compared with active and chronic active inflammation |
Interferes with conception and may cause early embryonic death. |
|
Grade 3A |
Chronic endometritis with glandular fibrosis. |
Interferes with implantation and placentation. May cause early embryonic death |
|
Grade 3B |
Uterine neoplasia |
Pregnancy loss or abortion. |
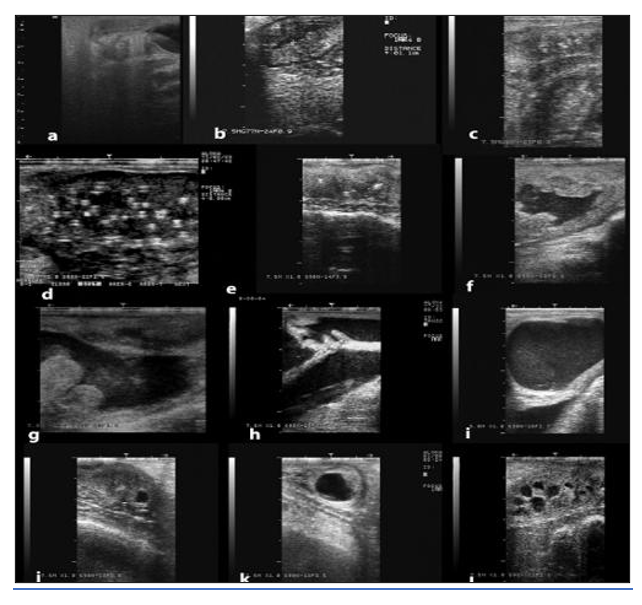
Figure 12: Ultrasonographic appearance of some disorders of the uterus. a) Infantile uterus, b) Endometritis, c) Chronic endometritis, d) Endometrial abscesses, e) Cervical adhesions, f) Pyometra; g) Post-fetotomy pyometra; g) mucometra due vaginal adhesions, note the open cervical rings, i) Mucometra due to vaginal aplasia, j-l) Uterine cysts (Pearson and Tibary, 2014).
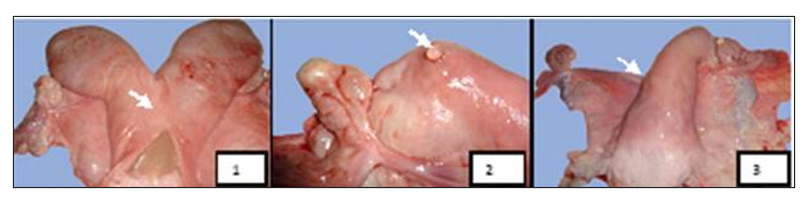
Figure 13: Macroscopic aspects of uterine affections found in female camels studied at El-Oued Slaughterhouse. 1 - Pyometra, 2 - Uterine serosal inclusion cyst, 3 - Uterine agenesis (Gherissi et al., 2019).
IV. Vaginal and cervical adhesions
Vaginal and cervical adhesions are severe long-standing reproductive disorder in dromedaries and consequently result in a high culling rate. The incidence of vaginal and cervical adhesion amounted to about 14.4% and 6.7%, respectively, of the infertility problem. The affected animals are often unable to breed due to obstruction of the genital tract. Moreover, the results of adhesion treatment trials have not been optimistic. Several risk factors are assumed for cervico-vaginal adhesion, such as chronic vaginitis, over-breeding, aggressive mating practice, and injuries during parturition.
Generally, adhesion occurs secondary to surgery, infection, trauma, or radiation. The bacterial infections of the genital tract of the female camel have been shown to be the main causes of reproductive disorders. In camelids, the invasive breeding nature and frequent mating can cause trauma to the cervix and uterus.
Diagnosis
§ Vaginal examination: access to the cranial part of the genital tract was blocked. This adhesion was found at the mid or caudal vagina or the cervix.
§ Trans-rectal ultrasonography: accumulation of hypo- or hyper-echogenic materials in the uterus.
V. Persistent hymen
o It was detected through vaginal examination of some heifers as a membrane cranial to the external opening of the urinary.
o Persistent hymen can be complete and incomplete, leading to accumulation of vaginal fluid or sometimes protruding of Hymen outside the vagina.
o In case of incomplete perforation of the hymen, the female feels pain after mating, because the hymen is very thick, and the opening is small.
o This is treated by giving an incision using a pair of scissors or a scalpel.