Acute Gastroenteritis in Infants and Young Children
- Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing gastroenteritis diagnosis, treatment, and prevention strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of nutritional care delivery, care gaps and current needs.
3. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
4. Identify barriers to, and facilitators of implementation.
5. Select an implementation framework and its component strategies.
6. Develop a step-by-step implementation plan:
· Select the target populations and evaluate the outcome.
· Identify the local resources to support the implementation.
· Set timelines.
· Distribute the tasks to the members.
· Evaluate the outcomes.
7. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
· Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
· Educational materials: printed or electronic information (software).
· Web-based education: computer-based educational activities.
· A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
· Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
· Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
· Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
· Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
· Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behaviors.
· Mass media campaigns.
3. For Nurses
· Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
· Educational materials: printed.
· A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
· Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
· Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
· Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
· Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
· Administrative policies and procedures.
· Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
· International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
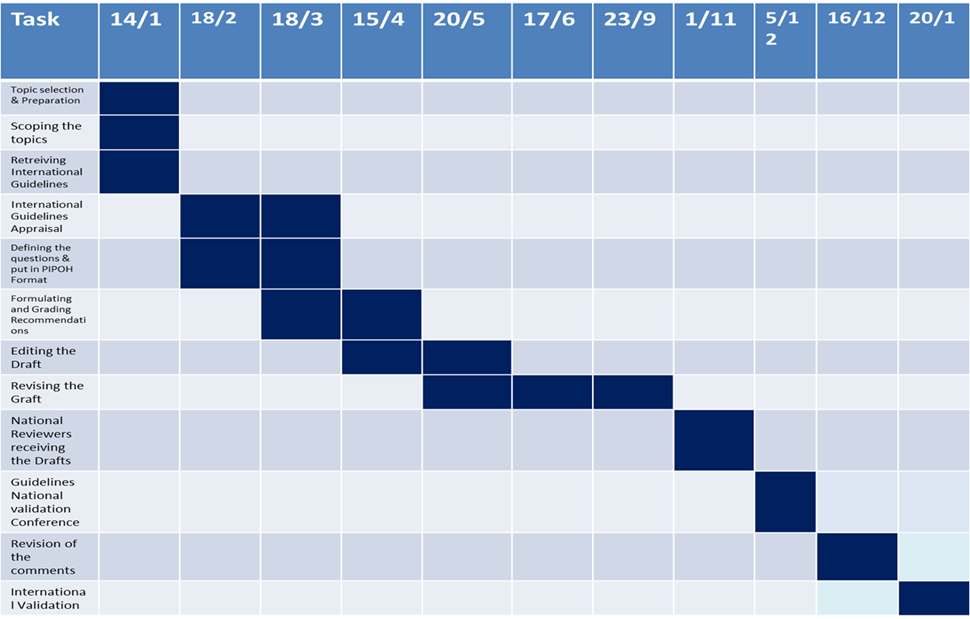
· Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
Guideline Implementation Tools
Educational materials based on this Adapted CPG for treatment of CAP in children have been made available in several forms including:
1. Manual for physician for diagnosis and algorithm for management of acute malnutrition
3. Arabic Educational materials for nurses and mothers
Implementation
To improve acute gastroenteritis care and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels, and integrated into clinical practice.
Dissemination involves educating health care providers to improve their awareness, knowledge, and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders, and should take into account local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps in implementing AGE diagnosis, management and prevention strategy into a health system:
1- Develop a multidisciplinary working group.
2- Assess the current status of acute gastroenteritis care delivery, care gaps and current needs.
3- Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
4- Identify barriers to, and facilitators of implementation.
5- Select an implementation framework and its component strategies.
6- Develop a step-by step implementation plan:
• Select the target populations and evaluate the outcome.
• Identify the local resources to support the implementation.
• Set timelines.
• Distribute the tasks to the members.
• Evaluate the outcomes.
7- Continuously review the progress and results to determine if the strategy requires modification.
Clinical Practical Guidelines Implementation strategies will focus on:
1. Practitioners
Dissemination and implementation of CPG through the following strategies:
· Educational meetings: conferences, lectures, workshops, grand rounds, seminars and symposia.
· Educational materials: printed or electronic information (software).
· Web-based education: computer-based educational activities.
· A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
· Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
· Optimize professional–patient interactions, through mass media campaigns, reminders, and education materials.
· Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. Patients
· Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
· Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behavior.
· Mass media campaigns.
3. Nurses
· Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
· Educational materials: printed.
· A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
· Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
· Practice tools: tools designed to facilitate behavioral/practice changes.
4. Stakeholders
Plans have been made to contact with all the health sectors in Egypt including:
Ministry of Health, Health Insurance Organizations, University Hospitals, Ministry of Interior, Ministry of Defense, Curative Care Organizations, Non-Governmental Organizations, Private sectors and Health Care Facilities.
· Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
· Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases or observations by patients. Summary may be targeted at the individual practitioner or the organization.
· Administrative procedures/policies.
· Formularies: Drug safety programs, electronic medication administration records.
Other activities to assist the implementation of the guideline’s recommendations include:
A. International initiative: Dissemination of the presented adapted CPG internationally via sending the final draft to the Guidelines International Network (G.I.N) and the ADAPTE Working Group and contact the CPG developers.
B. Gantt Chart has been designed by the Epidemiologist supervised by Prof. Dr. Tarek Omer to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
The Implementation tools:
Examples of Dissemination and Implementation Proposed Resources
Educational materials based on this Adapted CPG for treatment of acute gastroenteritis in children have been made available in several forms including:
Table (4) Pediatric Dehydration Scale (PDS) for Children16.
|
Characteristics |
0 |
1 |
2 |
|
General appearance |
Normal |
Thirsty, restless or lethargic but irritable when touched |
Drowsy, limp, cold or sweaty ±comatose |
|
Eyes |
Normal |
Slightly sunken |
Extremely sunken |
|
Mucous membranes (tongue) |
Moist |
Sticky |
Dry |
|
Skin Turgor |
Goes back immediately |
Delayed (<2sec) |
Very delayed (>2sec) |
A score of 0 represents no dehydration; a score of 1 to 4, some dehydration; and a score of 5 to 8 moderate/severe dehydration.
Table (5) Indications for Hospitalization7.
|
Indications for Hospitalization: |
|
· Shock |
|
· Severe dehydration (>9% of body weight) |
|
· Neurological abnormalities (lethargy, seizures, etc) |
|
· Intractable or bilious vomiting |
|
· Failure of oral rehydration |
|
· Suspected surgical condition |
|
· Conditions for a safe follow-up and home management are not met · Complicated AGE ( electrolyte imbalance, DIC) |
Table (6) Indications for Discharge7.
|
Indications for Discharge: |
|
· Sufficient rehydration is achieved as indicated by weight gain and/or clinical status |
|
· IV fluids are no longer required |
|
· Oral intake equals or exceeds losses |
|
· Medical follow-up is available via telephone or office visit |
Table (7) Indications for IV Rehydration7.
|
Indications for IV Rehydration: |
|
· Shock |
|
· Dehydration with altered level of consciousness or severe acidosis |
|
· Worsening of dehydration or lack of improvement despite oral or enteral rehydration therapy |
|
· Persistent vomiting despite appropriate fluid administration orally or via an NG tube |
|
· Severe abdominal distension and ileus |
NG= Nasogastric
Table (8) Holliday–Segar Method To Calculate Maintenance Fluid17.
|
Child’s weight |
Baseline daily fluid requirement |
|
1–10 kg |
100 ml/kg |
|
10–20 kg |
1000 ml + 50 ml/kg for each kg >10 kg |
|
>20 kg |
1500 ml + 20 ml/kg for each kg >20 kg |
kg=Kilogram, ml=Milliliter
Table (9) Signs of Shock 18.
|
Signs of compensated shock: |
|
· Tachycardia |
|
· Cool extremities |
|
· Prolonged capillary refill (despite warm ambient temperature) · Weak peripheral pulses compared with central pulses · Normal blood pressure |
|
Signs of decompensated shock: |
|
In addition to the above, these signs include: |
|
· Depressed mental status · Decreased urine output · Metabolic acidosis · Tachypnea |
|
· Weak central pulses |
|
* Signs of decompensated shock include the signs listed above plus hypotension. In the absence of blood pressure measurement, decompensated shock is indicated by the non-detectable distal pulses with weak central pulses in an infant or child with other signs and symptoms consistent with inadequate tissue oxygen delivery. |
Figure (2) Management of a Case of AGE
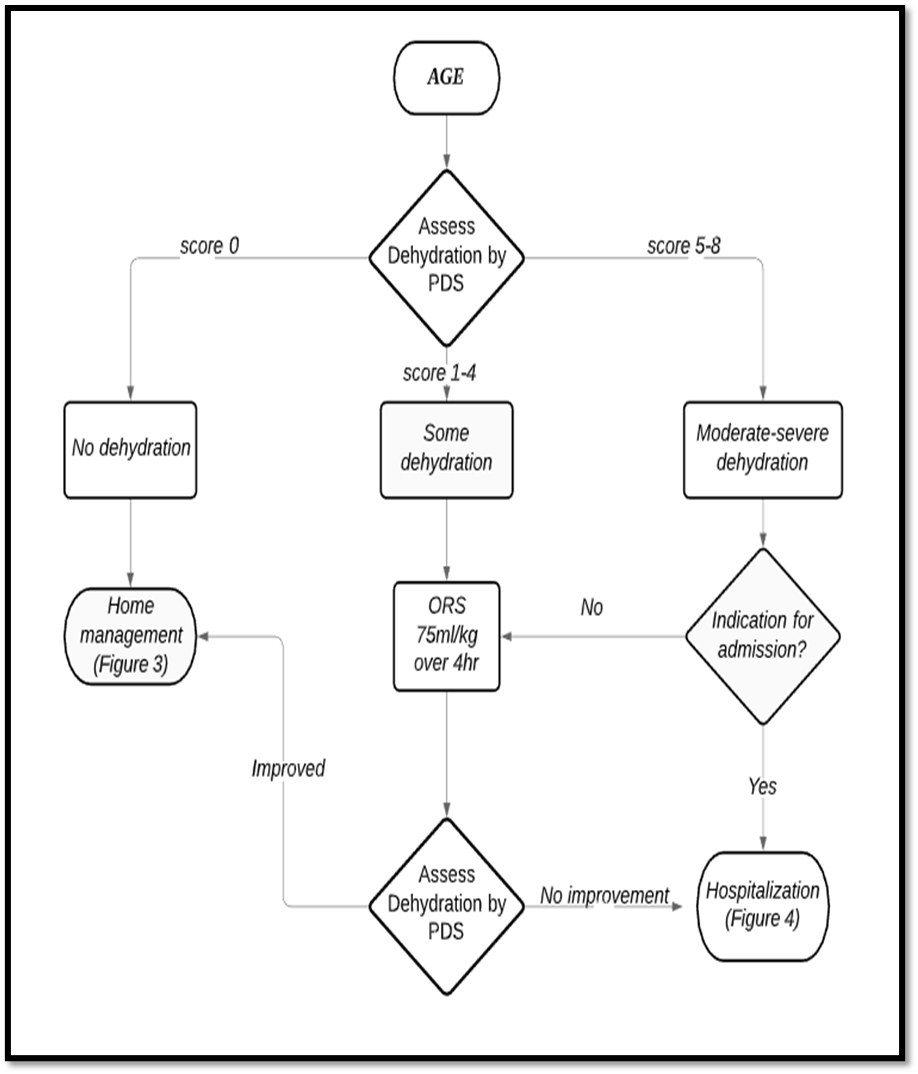
AGE= Acute gastroenteritis, PDS= Pediatric dehydration scale, ORS= Oral rehydration salts solution.
Figure (3) Home Management of a Case of AGE

AGE= Acute gastroenteritis, ORS= Oral rehydration salts solution.
Figure (4) Hospital Management of a Case of AGE
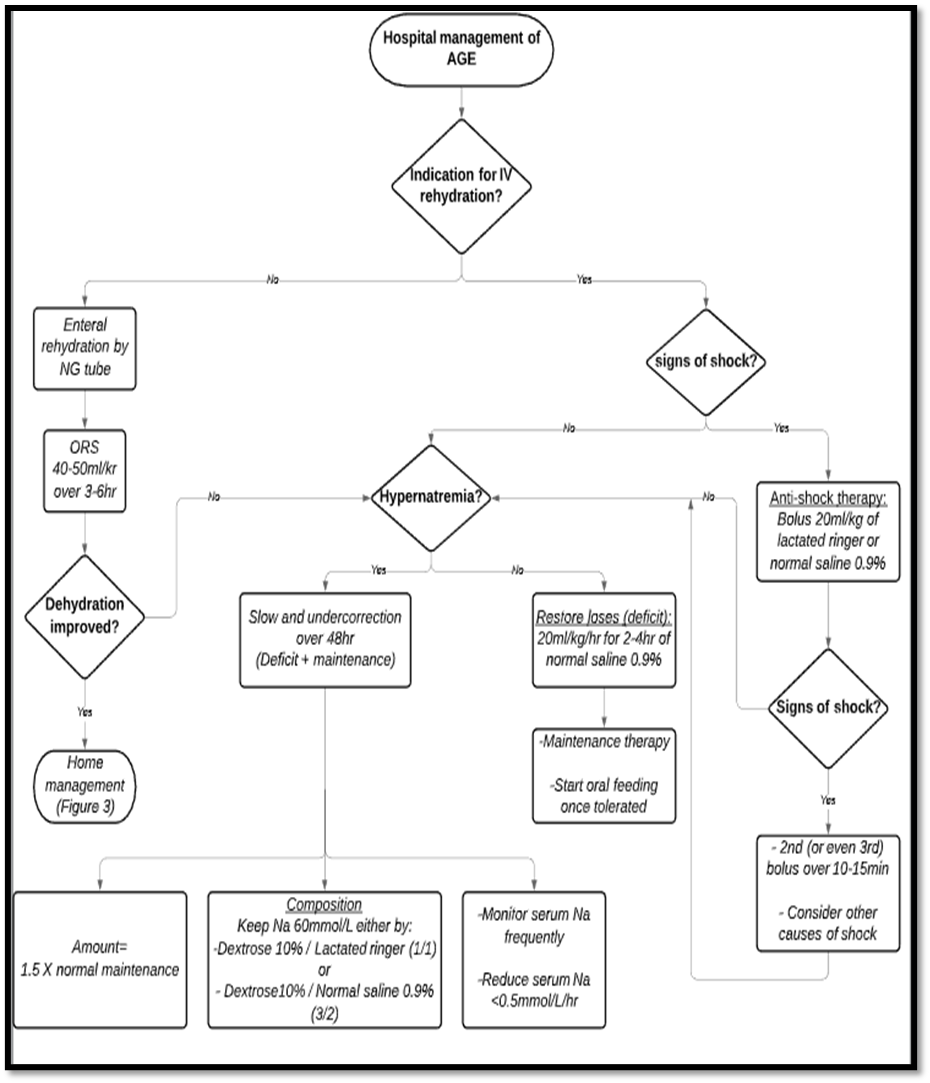
AGE= Acute gastroenteritis, IV= Intravenous, Na= Sodium, NG= Nasogastric, ORS= Oral rehydration salts solution.
علاج النزلات المعوية فى المنزل
1. محلول معالجة الجفاف:
▪️طريقة الاعداد:
يتم اضافة محتويات الكيس على 200 سم
ماء فى كوب نظيف-
يتم اعطاء المحلول للاطفال باستخدام
ملعقة صغيرة نظيفة (للاطفال اقل من عامين) او عن- طريق اخذ رشفات مباشرة من الكوب.
الاطفال اقل من 6 اشهر يمكن اعطائهم
المحلول عن طريق حقنة منزوعة السن ويتم تقطير المحلول فى فم الطفل (لا يتم اعطاء
المحلول فى زجاجات الرضاعة).
▪️الجرعة المناسبة:
- يتم اعطاء الطفل 5-10 مل (1-2 ملعقة صغيرة) لكل كيلوجرام من وزن الطفل بعد كل حركة اسهال.
· طريقة اعطاء محلول معالجة الجفاف:
- يتم اعطاء ملعقة صغيرة او رشفة من الكوب للطفل كل 1-2 دقيقة.
- اذا حدث قئ يتم الانتظار لمدة 10 دقائق ثم نعيد اعطاء المحلول للطفل ببطء أكثر (ملعقة صغيرة او رشفة من الكوب للطفل كل 2-3 دقيقة).
2. تغذية الطفل:
· لا يجب ايقاف التغذية للطفل سواء كانت رضاعة طبيعية او صناعية او غذاء اعتيادى.
· يجب الإكثار من إعطاء السوائل للطفل قدر المستطاع إلى حين توقف الإسهال.
· السوائل التى لا يجب إعطائها للطفل هى:
- المشروبات الغازية
- العصائر التجارية المعلبة
- المشروبات المحلاه بالسكر
- المشروبات التى تحتوى على مادة الكافيين
3. الزنك:
يتم اعطاء شراب الزنك للأطفال الذين يعانون من النزلات المعوية لمدة 14 يوما وتكون الجرعة:
- 10 مجم يوميا للأطفال أقل من 6 أشهر.
- 20 مجم يوميا للأطفال أكبر من 6 أشهر.
4. البروبيوتيك.
▪️ يجب زيارة الطبيب فى الحالات الآتية:
- القئ المستمر
- قيام الطفل بتمرير العديد من البراز المائي
- ارتفاع درجة الحرارة
- الأكل أو الشرب القليل
- العطش الشديد
- وجود دم بالبراز
- عدم تحسن الطفل خلال 3 أيام.
Gantt Chart for the Second Wave: Appendix