diagnosis and treatment of functional constipation in infants and children
- Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing functional constipation diagnosis, treatment, and prevention strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of nutritional care delivery, care gaps and current needs.
1. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
2. Identify barriers to, and facilitators of implementation.
3. Select an implementation framework and its component strategies.
4. Develop a step-by-step implementation plan:
· Select the target populations and evaluate the outcome.
· Identify the local resources to support the implementation.
· Set timelines.
· Distribute the tasks to the members.
· Evaluate the outcomes.
5. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
· Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
· Educational materials: printed or electronic information (software).
·Web-based education: computer-based educational activities.
· A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
· Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
· Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
· Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
· Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
· Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behaviors.
· Mass media campaigns.
3. For Nurses
· Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
· Educational materials: printed.
· A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
· Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
· Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
· Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
· Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
· Administrative policies and procedures.
· Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
· International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
· Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
➡️Guideline Implementation Tools
Educational materials based on this Adapted CPG for treatment of CAP in children have been made available in several forms including:
1. Manual for physician for diagnosis and algorithm for management of acute malnutrition
3. Arabic Educational materials for nurses and mothers
The CPG adaptation group decided to adopt all of the CPG implementation tools proposed by member group including the following: -
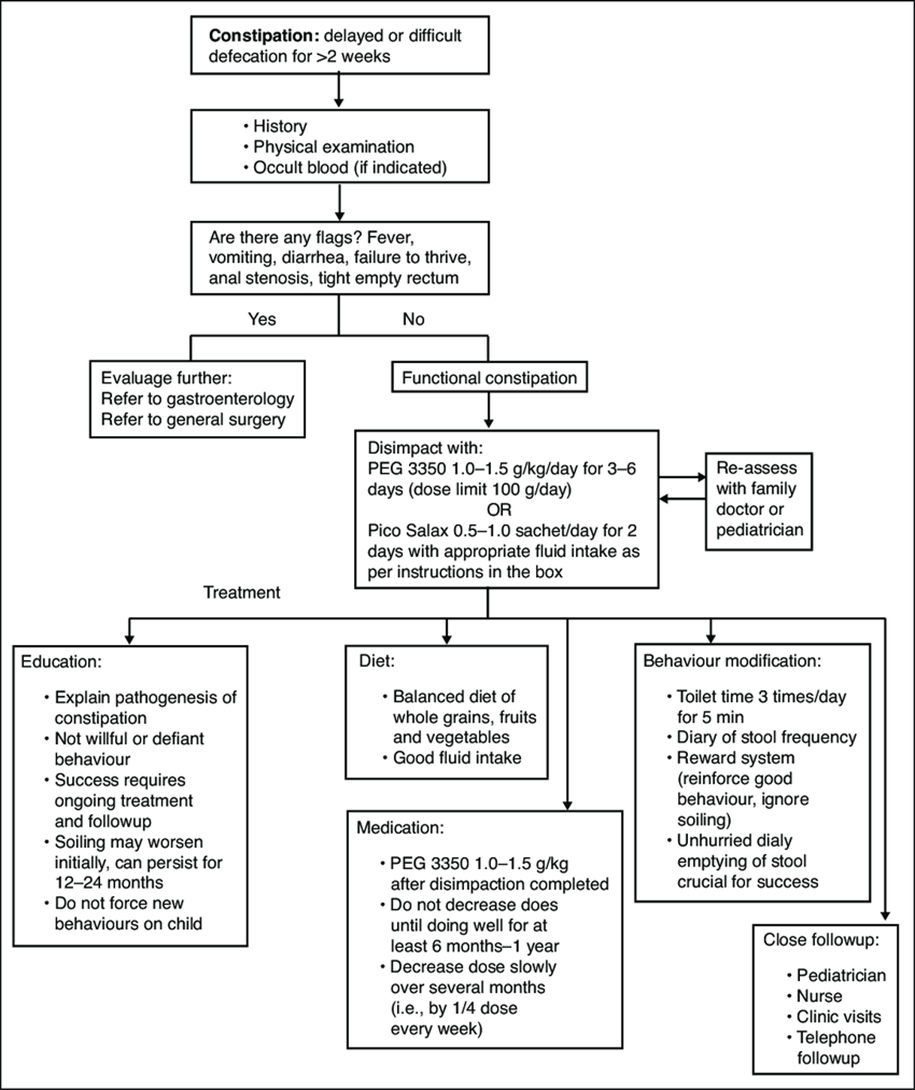
Constipation treatment algorithm. Adapted from The Hospital for Sick Children constipation fluxogram 2013.
Parent and carer health educational guide (in Arabic) ازاي تعرفي أن ابنك عنده امساك ؟- لو بيعمل براز أقل من ٣ مرات في الأسبوع أو لو البراز ناشف جدا أو لو بيتالم أو يبكي أثناء التبرز
· ده معناه ايه ؟ انك لازم تتابعي عملية التبرز و خصوصا .لما يكبر شوية و يبدأ يدخل الحمام لوحده اوقات كتير تيجي الام تشتكي من طفلها عنده مغص و الام مستمرة في البطن و لما نسأل عن التفاصيل نلاقي أن الطفل عنده امساك بيعمل حمام كل ٣-٤ ايام و الام .فاكرة أن دي طبيعته عادي
· ٣ مراحل مهمة في حياة الطفل يكثر فيها حدوث - : الإمساك لازم تاخدي بالك منهم
١ -عند سن ٦ شهور مع ادخال طعام الفطام
٢ -عند سن ٥.٢-٣ سنوات مع تدريب الطفل علي استعمال الپوتي أو التواليت حيث يبدأ في رفض التدريب في البداية
٣ -عند دخول المدرسة حيث يبدأ الطفل في رفض استعمال حمام المدرسة في كل مرحلة لازم نخلي بالنا .
· عند ادخال طعام الفطام لازم اهتم بوجود عناصر غذائية ملينة زي الكوسة و . القرع و الفاكهة الملينة سواء عنب أو كونتالوب مثلا و في المرحلة التانية لابد من الصبر علي الطفل أثناء عملية التدريب و إعطاؤه الوقت الكافي للتدريب و برضه الحفاظ علي نوعية الطعام زي ما قلنا سابقا . و في المرحلة دي انواع الاطعمة بتزيد . يعني مثلا بدل ما يتعود ياكل عيش فينو طول الوقت
· لازم يتعود ياكل عيش بلدي المحتوي علي الردة و هي ألياف هامة .
· لازم يتعود ياكل خيار او طماطم او خس ... يا منفردة يا في صورة سلطة .
· برجاء عدم إدخال عصائر السوبرماركت و شيبسي و خلافه و كيك و بسكوتات....
· و هكذا في المرحلة التالثة لازم تشجعه أنه يدخل حمام المدرسة حين يشعر أنه يحتاج الي دخول الحمام و اعطيه مطهر و مناديل ورقية و قاعدة حمام بلاستيكية و اعلمه كيفية التعامل مع الحمامات العامة في البيت
· لازم اعود طفلي أنه يدخل الحمام ٣ مرات في اليوم بعد الاكل حتي لو لم يكن يرغب في الدخول لمدة ١٠ دقائق و إذا شعر في اي وقت بالرغبة في دخول الحمام يدخل فورا لان الاحساس بالرغبة في التبرز يختفي بعد قليل و إذا تكرر الأمر فيحدث ما نسميه امساك تعودي
· لازم برضه نخلي بالنا أن الأطفال لاترغب في ترك اللعب مع الاخوات و الأقارب و الاصدقاء و حاليا في اللعب بالاجهزة الإلكترونية لتضيع وقتها في دخول الحمام فلابد من ملاحظة ذلك
· و طبعا التوجه للطبيب ضروري في أي مرحلة لان هناك بعض الأمراض تبدأ بالامساك و قد يضطر لإعطاء الطفل بعض الأدوية لتسهيل عملية التبرز و برجاء عدم ايقاف الأدوية الا تحت إشراف الطبيب حيث أن الامساك قد يحتاج لفترات طويلة لعلاجه.
Rome III diagnostic criteria for functional constipation
In the absence of organic pathology, >2 of the following must occur
For a child with a developmental age <4 years*
1. <2 defecations per week
2. At least 1 episode of incontinence per week after the acquisition of toileting skills
3. History of excessive stool retention
4. History of painful or hard bowel movements
5. Presence of a large fecal mass in the rectum
6. History of large-diameter stools that may obstruct the toilet
· Accompanying symptoms may include irritability, decreased appetite, and/or early satiety, which may disappear immediately following passage of a large stool
For a child with a developmental age >4 years with insufficient criteria for irritable bowel syndrome #
1. <2 defecations in the toilet per week
2. At least 1 episode of fecal incontinence per week
3. History of retentive posturing or excessive volitional stool retention
4. History of painful or hard bowel movements
5. Presence of a large fecal mass in the rectum
6. History of large-diameter stools that may obstruct the toilet.
*Criteria fulfilled for at least 1 month. Adapted from Hyman et al (12)
#Criteria fulfilled at least once per week for at least 2 months before diagnosis. Adapted from Rasquin et al (13)