Emergency Management (Diagnosis and Treatment) of Seizures in Children beyond the Neonatal Period
- Introduction
DEFINITIONS
A seizure is a transient occurrence of signs &/or symptoms due to abnormal excessive or synchronous neuronal activity of the brain (1). Brief seizures are defined as seizures lasting less than 5 minutes, while prolonged seizures last between 5 & 30 minutes (2). A seizure that is provoked by a transient factor acting on an otherwise normal brain that temporarily lower the seizure threshold is not diagnosed as epilepsy (reactive seizure or acute symptomatic seizure) (3).
The term unprovoked seizure implies to the absence of a temporary or reversible factor lowering the threshold and producing a seizure at that point in time then. The condition of recurrent reflex seizures in response to photic stimuli represents provoked seizures that are defined as epilepsy. Even though the seizures are provoked, the tendency to respond repeatedly to such stimuli with seizures meets the conceptual definition of epilepsy (4).
Febrile seizures are seizure occurring in children between 6 months and 5 years of age in association with a fever greater than 38 C , who do not have evidence of an intracranial cause (e.g. Infection , head trauma , and epilepsy) , another definable cause of seizure (e.g. electrolyte imbalance , hypoglycemia , drug use, or drug withdrawal) or a history of an afebrile seizure (5).
Epilepsy is a disease of the brain defined by any of the following conditions:
1. At least two unprovoked (or reflex) seizures occurring > 24 hours apart.
2. One unprovoked (or reflex) seizure & a probability of further seizures similar to the general recurrence risk (at least 60%)
3. Diagnosis of an epilepsy syndrome (6,7,8&9)
Status epilepticus is defined as more than 30 minutes of either, continuous seizure activity or two or more sequential seizures without full recovery of consciousness between them (2). The 30 - Minute’s definition is based on the duration of convulsive status epilepticus that may lead to permanent neuronal injury by itself (10). Since the majority of seizures are brief, and once a seizure lasts more than 5 minutes it is likely to be prolonged (11). Continuous Generalized convulsive SE in adults and children older than 5 years was operationally defined as 5 min or more clinical and/or electrographic seizure activity or (ii) recurrent seizure activity without recovery (returning to baseline) between seizures. Status treatment protocols have used a 5 - minute definition to minimize both the risk of seizures reaching 30 minutes and the adverse outcomes associated with needlessly intervening on brief, self-limited seizures (12).
This guideline follows this convention & for purposes of treatment, uses the term status epilepticus to represent studies involving both prolonged seizures and traditionally defined status epilepticus.
Status epilepticus presents in several forms:
1. Convulsive status epilepticus consisting of repeated generalized tonic - clinic (GTC) seizures with persistent postictal depression of neurologic function between seizures.
2. Nonconvulsive status epilepticus where seizures produce a continuous or fluctuating epileptic twilight state.
3. Repeated partial seizures manifested as focal motor signs, focal sensory symptoms, or focal impairment of function (e.g. aphasia) not associated with altered awareness (epilepsies partialis continua) (13, 14&15).
DIFFERENTIAL DIAGNOSIS
The diagnosis of epileptic seizures is largely dependent on a good history and witness report, as well as good knowledge of seizure semiology, and of the symptoms of a variety of differential diagnostic conditions. Still, many episodic conditions may be confused with epileptic seizures (16). In the case of status epilepticus, many brief events can be easily excluded from the differential diagnosis. Reflex anoxic seizures and cyanotic breath breath-holding spells are the most common confusing events. They may be associated with brief extensor stiffening and a few seconds of irregular spasms or jerks because of the abrupt loss of cerebral energy supply. Occasionally, an anoxic seizure may provoke a true epileptic seizure. This combination is called an anoxic-epileptic seizure. A positive family history of epilepsy may make some children more prone to anoxic-epileptic seizures. The later may last up to 10 minutes and present as SE (17).
Differential Diagnosis of status epilepticus should include movement disorders and non-epileptic seizures (18) like psychogenic non-epileptic seizures. Sandifer syndrome can be considered a prototype of dystonic posturing that is usually evaluated as intractable seizures. It is a paroxysmal movement disorder characterized by dystonic movements of the head, neck, and trunk in association with gastroesophageal reflux disease (19&20).
However, dystonic postures can be Epileptic. A dystonic posture of a limb is a feature seen in focal seizures. It is infrequently seen in the very young but becomes more common in the school-age child. Dystonic postures of the hand are usually contralateral to the seizure focus. They may often be coupled with ipsilateral (to the seizure focus) limb automatisms. A unilateral dystonic posture suggests a focal seizure (21).
Both symmetric and asymmetric tonic postures, are seen with focal seizures. In the very young, it is possible that these tonic postures ar these tonic postures that may be generated in the deeper brainstem or subcortical structures and are not direct manifestations of the ictal discharges. In accordance with Following this, some asymmetric tonic postures can be reversed by passive turning of the head during a seizure, in a fashion similar to the tonic neck reflex elicited in the newborn (21).
Decerebrate and decorticate postures are not likely to be mistaken for a seizure, those posturing typically occur in response to noxious stimuli (22).
Other differential diagnoses of events that have duration’s compatible with status epileptics include self-stimulatory behaviors as seen in autistic children (23) and stereotyped behaviors associated with established neurologic diseases as cerebral palsy (22).
Psychogenic non-epileptic seizures (PNES) are time-limited disturbances of consciousness and motor-sensory control, not accompanied by ictal activity on electroencephalogram (EEG) and are best conceptualized as atypical neurophysiological responses to emotional distress, physiological stressors, and danger (24).
In cases where status epilepticus occurs in a newly diagnosed child or it is the first presentation of a seizure disorder, the following diagnoses should be considered; CNS vasculitis whether primary or secondary, anti NMDA encephalitis and other autoimmune illnesses (25), as well as febrile infection‐related epilepsy syndrome (FIRES) and new‐onset refractory status epilepticus (NORSE) (26). It is important to identify these disorders as early as possible to apply specific therapeutic agents.
EPIDEMIOLOGY OF ACUTE SEIZURES
Although the epidemiology of epilepsy has been well studied, less has been identified about the epidemiology of acute seizures. Studies suggest that around 4–10% of children have an experience of seizure before 16 years of age where 1/5th of total children with unprovoked seizures may develop epilepsy later. Each year, about 150,000 children and adolescents will come to medical attention for evaluation of a newly occurring seizure disorder of some type. Between 2% and 4% of all children in Europe and the United States experience at least one convulsion associated with a febrile illness before the age of 5 years (27).
EPIDEMIOLOGY OF SEIZURES IN THE EMERGENCY DEPARTMENT (ED):
Seizures are one of the common causes for hospital admissions in children with significant mortality and morbidity especially in younger children, it is estimated to be 2% of visits to children’s ED hospitals, (28) and 3.4% of admission to children’s tertiary care hospital (29). The high occurrence among small children, in comparison to older ones, is a result of the febrile seizure, accounting for 28% of all pediatric ED seizures (30).
GENDER:
Males account for a greater proportion of seizures in the ED setting, with an odds ratio of 1.4 for the association between male gender and seizure among ED visits (31). On a population level (rather than in the ED setting), acute symptomatic seizures occur in males versus females in a ratio of 1.85 to 1, with a lifetime risk of 5.0% in males and 2.7% in females (32). By contrast, epilepsy is only slightly more common in males. (33) The increased incidence of acute symptomatic seizures in males, in previously mentioned studies, is not due to trauma, as the male predominance persists across all etiologic categories. (31)
ETIOLOGY:
Most seizures managed in the ED are secondary to an underlying disease process, that is, they are either acute symptomatic seizures or pediatric febrile seizures. (28) Among children, the febrile seizure is the most common, accounting for almost a third of pediatric ED seizures. (34) Febrile seizures in children are classified as simple versus complex. Simple febrile seizures are the most common and have an excellent prognosis, while 20% of first febrile seizures are complex. The peak incidence of a first febrile convulsion occurs in the second year of life. The risk of recurrence is high, and ranges from about 12% in children whose first febrile seizure occurs in infancy to about 50% in those whose first febrile seizure occurs later. The subsequent risk of epilepsy is the same as for children who have never had a febrile seizure. Complex febrile seizures, on the other hand, do indicate an increased risk for epilepsy, and do not indicate an increased risk for future occurrence of simple febrile seizures. (36)
Between 0.5% and 1% of children and adolescents experience a seizure associated with acute metabolic causes; hyponatremia contributed to 70% of metabolic causes especially in children younger than 6 months and those in the neonatal period. (37) The contribution of “breakthrough seizures” among chronic epileptics to the burden of seizure care in the ED setting is unknown. The aforementioned study suggested that only 6.8% of seizures in the ED were due to epilepsy. (38) However, a smaller study in a different setting found that 46% of seizure visits to an urban ED were by known epileptics. (35)
SEMIOLOGY:
In the majority of studies, Generalized tonic tonic-clonic seizures were the commonest seizure type and were seen in; 63.3% in one study. (39) 82.1% by Chaudhary et al, (29) and even up to (98.0%) by Mwipopo1 et al. (40)
STATUS EPILEPTICUS:
In the ED-based series, when status epilepticus was mentioned, it represented 6% to 7% of seizures. (41) In 1995, DeLorenzo and colleagues estimated 195,000 status events in 152,000 patients per year in the United States, with 42,000 deaths. The highest rate was in infants. Fewer than half of the cases were managed by neurologists, and the majority (58%) occurred in patients with no prior history of epilepsy. In children, mortality was estimated with 3% in, while risk factors were: infection (52%), remote insult (39%), low antiepileptic drug levels (21%), stroke, metabolic, hypoxia, idiopathic, and trauma. (42)
EPIDEMIOLOGY OF EPILEPSY WITH SPECIAL REFERENCE TO EGYPT:
Epilepsy affects 50 million people worldwide, with an estimated 2–3 million living in the United States, 6 million in Europe, and at least 40 million in the developing world. Epilepsy poses a significant burden on the quality of life of affected individuals and their families. Nearly 80% of the people with epilepsy are found in developing regions. Seventy percent of people who develop epilepsy do so in the first two decades of life. Seizures and epilepsy affect infants and children more than any other age group. (43, 44)
Studies (with population size more than 1000) conducted in the Mediterranean region have shown that the prevalence of epilepsy ranges from as low as 4.04 per 1000 population to those as high as 12 or more per 1000 population. Furthermore, higher rates are reported in young age groups and in rural populations (45) In a comprehensive review of the epidemiology of epilepsy in the Arab World (22 countries), and epidemiological literature search was conducted utilizing Google and PubMed, Google provided 21 prevalence, four CAMP and nine incidence estimates while PubMed provided 10 such estimates none of which has been identified by Google. No epidemiological data about epilepsy were found in 10/22 countries. (46)
Regarding Egypt, the epidemiological profile of epilepsy in New Valley Governorate in Egypt (2013) was conducted to estimate its magnitude of treatment gap and revealed that life time prevalence of epilepsy in Al Kharga district is 6.76/1000, with the highest peak during early childhood. The annual incidence rate is 43.14/100, 00047. Another study was conducted to estimate the prevalence of different types of epilepsy in the region of the Assiut Governorate/Egypt (2013). The study revealed that the prevalence rate of active epilepsy was 9.3/1000 and the incidence rate was 1.5/1000. (75%) of them had idiopathic epilepsy. (CPR 9.5/1000) that high prevalence rate of epilepsy in Egypt is comparable with that in other Arabic and European countries (48).
Another study was conducted to evaluate the prevalence of epilepsy in primary school children in El-Minia City, Egypt (2009). Lifetime prevalence was 7.2/1000 in conventional schools and 133.3/1000 in schools for subnormal children. Male: Female ratio was 2:1. Prevalence was significantly higher among the lower socioeconomic class. In a door to door survey, a study conducted to determine prevalence and clinical patterns of epilepsy among children and adolescents in Upper Egypt. It revealed that lifetime prevalence was 9.7/1000 with a higher prevalence among children < 12 years than adolescents. The age-specific prevalence was highest among early childhood (12.01/1000) and lowest in adolescence. More than half of the target population have has idiopathic epilepsy. The most frequent causes of symptomatic/structural epilepsy were perinatal complications particularly in infancy, followed by CNS infection in early childhood and post-traumatic epilepsy in adolescence. Partial seizures were more frequent in infancy while generalized seizures were commoner in childhood and adolescence (49).
Another study for epilepsy prevalence in Al-Maniel Island using a door to door survey revealed a lifetime point prevalence of 6.9/1000 inhabitants and active epilepsy prevalence of 5.1/1000 inhabitants. The age distribution showed bimodal peaks one in adolescents and another in the elderly with equal sex ratio. Focal seizures were the most frequent (58.3%) and the treatment gap was (66.7%) (50). Studying stigma about epilepsy, a review was published in 2016 stated that people with epilepsy devalued and stigmatized. There are many factors that Many factors affect these stigmas including: false false-negative historical background of epilepsy, psychological aspects, knowledge, and attitudes towards people with epilepsy, uncontrolled epilepsy, and the effect of anticonvulsant drugs. (51) Studying the health-related quality of life in epilepsy revealed that patients with epilepsy are at a high risk of developing the impaired quality of life with lower mean scores in all domains especially those with generalized, frequent fits, those on polytherapy and those with younger age of onset of seizures and a longer duration of illness (52).
CLASSIFICATION OF SEIZURES & EPILEPSY
Figure (1): The basic ILAE 2017 operational classification of seizure types (54)
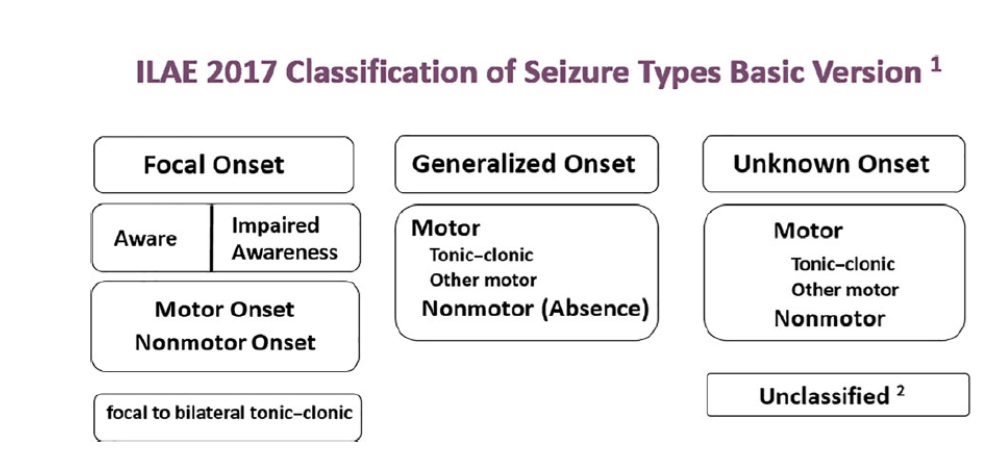
Figure (2): The expanded version of ILAE 2017 operational classification of seizure types (54)
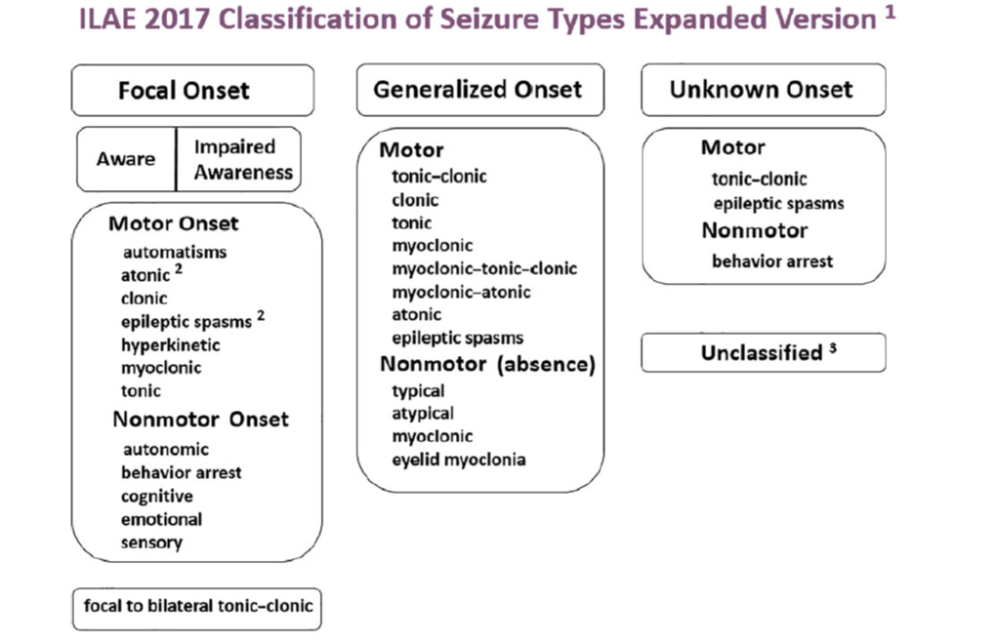
Seizure and epilepsy classification systems have been used in clinical practice and research since the 1970s(53). Over the years, multiple revisions have been implemented, the most recent of which is the 2017 International League Against Epilepsy (ILAE) operational epilepsy classification system. (54) This system aims to better define seizures and epilepsies by classifying them using key clinical features, EEG findings, imaging, and genetics. Seizure classification starts with whether the initial manifestations of the seizure are focal or generalized. Focal seizures originate within a neuronal network limited to one hemisphere that may be discretely localized or more widely distributed, whereas generalized seizures originate at some point within the brain and rapidly engage bilateral distributed networks. (55) If the onset of the seizure is missed or is unclear, the seizure is of unknown onset. Focal seizures are classified according to the patient’s level of awareness and the first most prominent motor or non-motor features of the seizure. (56) These early prominent features are important to consider when localizing the seizure onset or of the epileptogenic zone. The final feature used in the classification of focal seizures is whether the focal seizure evolves to a bilateral tonic-clonic seizure. A focal aware seizure replaces the previously termed simple partial seizure, and a focal impaired awareness seizure replaces the term complex partial seizure. Focal motor seizures can be more specifically defined. Motor-onset manifestations include automatisms, epileptic spasms, and atonic, clonic, hyperkinetic, myoclonic, or tonic seizures. Focal seizures with non-motor symptoms as the first prominent feature include autonomic, behavior arrest, cognitive, emotional, or sensory seizures. (57) Focal seizures can be further classified as to whether they evolve to a bilateral tonic-clonic seizure. This spread is typically clearly seen on EEG. (56) Generalized Seizures; similar to focal seizures, are classified according to a motor or non-motor manifestations. Broadly, motor seizures are either tonic-clonic or other motor seizures. Non-motor generalized seizures primarily refer to absence seizures. Motor onset more specifically includes tonic-clonic, clonic, tonic, myoclonic, myoclonic-tonic-clonic, myoclonic-atonic, atonic, or epileptic spasms. Non-motor or absence seizures include typical, atypical, myoclonic, or eyelid myoclonia. (58) Unknown Seizures are seizures of unknown onset and can be classified by a motor (tonic-clonic, epileptic spasms) or nonmotor (behavior arrest) presentations. If information is inadequate or if the seizure cannot be categorized, then the seizure is considered unclassified. (57)
The second level of classification is the epilepsy type. The epilepsy type is predominantly determined clinically; characteristic EEG findings provide supportive evidence. Similar to seizure classification, the epilepsies are classified as generalized or focal. (59) The new classification system additionally recognizes two new categories: combined generalized and focal epilepsy and unknown epilepsy. Patients with generalized epilepsy have one or more of the generalized seizure types, and their EEGs typically display generalized spike-wave activity. For individuals who have generalized seizure types and a normal EEG, other data are needed to determine whether the epilepsy is generalized. Having myoclonic jerks or a pertinent family history supports the diagnosis of a generalized epilepsy type. (60) Clinically, patients with one or more focal seizure types have focal epilepsy. These epilepsies can be either unifocal or multifocal. Although not always seen, focal EEG findings such as focal slowing or epileptiform discharges support the diagnosis of focal epilepsy. Concordant focal MRI findings are also supportive. Designation The designation of combined generalized and focal epilepsy is for patients with both focal and generalized seizures. EEG may reveal both focal and generalized electrographic findings. (56) Examples of combined generalized and focal epilepsy include Dravet syndrome and Lennox-Gastaut syndrome. When the patient has epilepsy as defined by the ILAE but it remains undetermined whether the patient has focal or generalized epilepsy, the classification of unknown epilepsy type is used. (61)
The epilepsy syndrome is a new addition to the current classification system and is defined as “a cluster of features incorporating seizure types, EEG, and imaging features that tend to occur together.” Factors that contribute to epilepsy syndrome include the age of onset, remission, triggers, diurnal variation, intellectual and psychiatric dysfunction, EEG findings, imaging studies, family history, and genetics. (56) The etiology of seizures and epilepsies is emphasized in the new classification system. Six etiologic categories (structural, genetic, infectious, metabolic, immune, unknown) have been defined. When multiple potential etiologies are present, priority should be given to the etiology with more relevant management issues. (62)
Status epilepticus (SE) is classified by four axes: (1) semiology; (2) etiology; (3) electroencephalography (EEG) correlates; and (4) age. Axis 1 (semiology) lists different forms of SE divided into those with prominent motor systems, those without prominent motor systems, and currently indeterminate conditions (such as acute confusional states with epileptiform EEG patterns). Those forms with prominent motor symptoms and impairment of consciousness may be summarized as convulsive SE as opposed to the non-convulsive forms of SE (NCSE). Axis 2 (etiology) is divided into subcategories of known and unknown causes. The etiologic classification of SE includes 1) acute symptomatic, 2) remote symptomatic, 3) remote symptomatic with an acute precipitant, 4) progressive encephalopathy, 5) febrile, and 6) cryptogenic (idiopathic). Axis 3 (EEG correlates) adopts the latest recommendations by consensus panels to use the following descriptors for the EEG: name of the pattern, morphology, location, time-related features, modulation, and effect of the intervention. Finally, axis 4 divides age groups into neonatal, infancy, childhood, adolescent and adulthood, and elderly. (63)
COMPLICATIONS OF ACUTE CONVULSIONS
Complication A complication is was defined as an event that requires additional attention, time, and effort by the treating physician and nursing staff. The majority of the generalized tonic tonic-clonic seizures (GTCS) are benign but some lead to complications such as cardiac arrhythmias, fractures/falls, rhabdomyolysis, and increase creatinin phosphokinase enzyme (CPK), aspiration pneumonia, acute kidney injury and disturbed level of consciousness or acute confusional state. While briefer, focal, and myoclonic seizures have less few complications. (64) The first stage of convulsive status epilepticus (CSE) is characterized by a high level of catecholamines in the blood, which leads to hyper -adrenergic stimulation and extreme stress on the body systems. It is triggered by intense and prolonged brain electrical activity and ending by blood vessels damage of many organs. (65)
All complications encountered could be summarized in the following table:
|
Classification |
Complications |
|
Systemic: |
|
|
Cardiac: |
Hypertension, tachycardia (reversing after 30 minutes), arrhythmias, and cardiac arrest. |
|
Pulmonary: |
Apnea, respiratory failure, hypoxia, neurogenic pulmonary edema, and aspiration pneumonia. |
|
Autonomic: |
Fever and hyperpyrexia, sweating, hypersecretion (including tracheobronchial), and vomiting. |
|
Metabolic: |
Hyperkalemia, hyperglycemia then hypoglycemia, volume depletion, metabolic acidosis, venous stasis, and possible thrombosis/ hemorrhage. |
|
Endocrine: |
Increased prolactin and cortisol |
|
Gastrointestinal complications: |
Stress ulcer, gastrointestinal hemorrhage, diarrhea, and paralytic ileus. |
|
Others: |
Leukocytosis, cerebrospinal fluid pleocytosis, vertebral and other fractures, physical injury, rhabdomyolysis, renal failure and disseminated intravascular coagulation |
|
Cerebral: |
Neuronal damage ، cerebral edema, raised intracranial pressure،, cortical vein thrombosis, and cerebral hemorrhage. |
|
Neurologic sequelae: |
Increased seizure frequency, recurrent status epilepticus, and decreased cognitive function. |
Adapted from: Drislane FW. Status epilepticus. In: Schachter SC, Schomer DL. Eds. The comprehensive evaluation and treatment of epilepsy. San Diego, CA: Academic Press: 1997. P. 149-172. With permission from Elsevier (www.elsevier.com)(3). (66)
Another source of complications is the medications used to control seizures as Benzodiazepines, which may cause respiratory and cardiovascular depression as well as immunologic dysfunction. Other drugs used in the treatment of SE include anesthetic and non-anesthetic drugs are also accompanied by various complications such as hypersensitivity, breathing difficulty, hemodynamic alterations, and renal injury. The distributive shock caused by these drugs can cause further deterioration of the neurological status by inducing or enhancing neuronal necrosis.
Complications may also arise from the long duration of severe illness and immobilization following the onset of SE and prolonged stay in the intensive care unit may lead to various respiratory and infectious ones. These may include nosocomial pneumonia, ventilator-associated pneumonia, pulmonary embolism, atelectasis or collapse of the lung alveoli, adult respiratory distress syndrome, and neurogenic pulmonary edema. Clostridial colitis and other infectious complications could also be enhanced by the slowed gastrointestinal motility. (65)
Sudden Unexplained Death in Epilepsy (SUDEP)
SUDEP is defined as a death that occurred suddenly, unexpectedly and of non-traumatic and non-drawing, witnessed or unwitnessed, with or without the evidence of a seizure, excluding status epilepticus, and without a toxicological or anatomical cause of death in post-mortem examination and will be responsible for about 7.5 to 17% of all deaths in epilepsy. Risk factors possible associated with SUDEP are refractoriness of the epilepsy, the occurrence of generalized tonic-clonic seizures, antiepileptic drugs polytherapy, early age of epilepsy onset, long term seizure disorder (more than 15 years), cardiovascular and pulmonary abnormalities and genetic factors. (67)
LABORATORY INVESTIGATIONS
All patients with acute seizure presentation should be investigated with routine blood tests to exclude infection or metabolic disturbance. (68) When evaluating a first seizure occurring in children, the American Academy of Neurology has recommended that laboratory screening tests should be ordered based on individual clinical circumstances. (69)
Acute and/or severe electrolyte imbalances can manifest with rapidly progressive neurologic symptoms or seizures, which may be the sole presenting symptom. (70)
Obtaining intravenous access is the next step after establishing the airway and circulation. (71) Blood should be measured for glucose, serum electrolyte; calcium, magnesium, sodium, potassium, blood urea nitrogen. Antiepileptic drug levels, as well as a toxic drug screen and complete blood cell count, are also required. Lumbar puncture was recommended when fever occurred with SE, especially in young children, unless a contraindication to LP was present. (72)
TREATMENT OF ACUTE SEIZURE
Given the urgency of terminating seizures, the initial diagnostic assessment and medical treatment should occur simultaneously. Though treatment options and diagnostics may be dictated by available medications and capacity, it is possible for virtually any healthcare setting to develop a relevant and feasible local guideline for seizure management. Clear specifications on when to refer to a higher level of care should be part of the care plan. (73&74)
PREHOSPITAL SEIZURE MANAGEMENT
In the prehospital setting or in a health care facility that is not equipped to administer intravenous medications, the WHO Guidelines Approved by the Guidelines Review Committee 2016 recommended that 0.5 mg/kg (maximum dose of 10 mg) of liquid diazepam can be given rectally. (74)
ACUTE MANAGEMENT
The urgent priority is terminating seizures, the WHO Review Committee 2016(75) recommended that the initial diagnostic assessment and emergency medical treatment should occur simultaneously. A brief history and rapid clinical examination should be done to find underlying etiology (e.g., neuro-infection, poisoning, established epilepsy) and to confirm that the event is a seizure. (73)
World Health Organization (WHO) updated their its emergency triage assessment and treatment (ETAT) guidelines. The guidelines are used to identify children with the life-threatening conditions seen most frequently in developing countries. Thus, children presenting with the following signs should be treated as emergencies: obstructed or absent breathing, severe respiratory distress, central cyanosis, signs of shock (cold extremities with capillary refill time > 3 s and weak and fast pulse), coma (or seriously reduced level of consciousness), seizures or, in a child with diarrhea, any two signs of severe dehydration signs: lethargy or unconsciousness, sunken eyes, very slow return of skin after pinching. Immediate treatment is begun when any emergency sign is identified (by assessment of Airway, Breathing and Circulation, ABC) until the end of the algorithm. Children who require prompt, full assessment, and rapid treatment are then checked for priority signs. Children without emergency or priority signs are deemed “non-urgent” on completion of triage. (74&76)
ABC with high concentration oxygen. Check glucose and establish an IV line. First First-line with IV is lorazepam. If lorazepam not available then diazepam. If no IV, then buccal midazolam. Second Second-line includes phenobarbital or phenytoin. Refractory status with midazolam or thiopental. (77)
The guideline, which reviewed all available adult and pediatric evidence, provides a treatment algorithm that comprises three phases of treatment. It also offers evidence-based answers to the effectiveness, safety, and tolerability questions regarding the treatment of convulsive status epilepticus.
• Stabilization phase (0-5 minutes of seizure activity), includes standard initial first aid for seizures and initial assessments and monitoring.
• Initial therapy phase (5-20 minutes of seizure activity) when it is clear the seizure requires medical intervention, a benzodiazepine (specifically IM midazolam, IV lorazepam, or IV diazepam) is recommended as the initial therapy of choice, given its demonstrated efficacy, safety, and tolerability. A benzodiazepine is the initial therapy of choice (Level A):
Choose one of the following 3 equivalent first first-line options with dosing and frequency:
1. Intramuscular midazolam (10 mg for > 40 kg, 5 mg for 13-40 kg, single dose, Level A) OR
2. Intravenous lorazepam (0.1 mg/kg/dose, max: 4 mg/dose, may repeat dose once, Level A) OR
3. Intravenous diazepam (0.15-0.2 mg/kg/dose, max: 10 mg/dose, may repeat dose once, Level A)
If none of the 3 options above are available, choose one of the following:
1. Intravenous phenobarbital (15 mg/kg/dose, single single-dose, Level A) OR
2. Rectal diazepam (0.2-0.5 mg/kg, max: 20 mg/dose, single dose, Level B) OR
3. Intranasal midazolam (Level B), buccal midazolam (Level B)
• Second therapy phase (20-40 minutes of seizure activity) when a response (or lack of response) to the initial therapy should be apparent. Reasonable options include fosphenytoin, valproic acid, and levetiracetam. There is no clear evidence that any one of these options is better than the others. Because of adverse events, IV phenobarbital is a reasonable second-therapy alternative if none of the three recommended therapies are available.
Choose one of the following second second-line options and give as a single dose:
1. Intravenous fosphenytoin (20 mg PE/kg, max: 1500 mg PE/dose, single single-dose, Level U) OR
2. Intravenous valproic acid (40 mg/kg, max: 3000 mg/dose, single dose, Level B) OR
3. Intravenous levetiracetam (60 mg/kg, max: 4500 mg/dose, single dose, Level U)
If none of the options above are available, choose one of the following (if not given already)
Intravenous phenobarbital (15 mg/kg, single dose, Level B)
• Children younger than 2 years presenting with seizures lasting more than 30 minutes, especially if myoclonic or if they are known to have pyridoxine dependent / /responsive seizures, should receive pyridoxine trial of 50-100 mg IM. It is to be noted that the IV forms are not available in Egypt, and using the IM route also avoids possible side effects previously mentioned with the IV route.
Third therapy phase (40+minutes of seizure activity). There is no clear evidence to guide therapy in this phase. The guideline found strong evidence that initial second therapy is often less effective than initial therapy, and the third therapy is substantially less effective than initial therapy. Thus, if second therapy fails to stop the seizures, treatment considerations should include repeating second-line therapy or anesthetic doses of either thiopental, midazolam, pentobarbital, or propofol (all with continuous EEG monitoring). (78)
PROGNOSIS
Seizure recurrences
- For febrile seizures, epilepsy occurs more frequently than in the general population. In a normal child with a simple febrile seizure, the risk is approximately 1 to 2 percent, only slightly above that of the general population. (79) For children with complex febrile seizures, an abnormal developmental history, or a family history of epilepsy, the risk is closer to 5 to 10 percent. (80)
- Children who have an acute symptomatic seizure (e.g., acute infection, acute head injury), have a low risk of seizure recurrence compared with other children with a first seizure and seizure recurrence is likely only if the underlying etiology recurs (Examples include seizures associated with febrile illnesses, metabolic derangements such as hyponatremia, and concussion). (81)
- The child who is a neurologically normal neurologically normal child with, has no history of a prior neurologic illness who, and has an unprovoked seizure with no evident acute cause has an approximately 25 percent risk of having another seizure in the next year and a 45 percent risk over the next three years. Clinical factors associated with an increased risk of recurrent seizures include: 1) Prior neurologic insult, 2) Significant brain MRI findings, 3) Abnormal EEG. (82-85)
Morbidity and Mortality
- The prognosis for children with febrile seizures is favorable. While early reports had suggested that febrile seizures were associated with an increased risk of sudden death, the results from a large population-based study indicate that the small excess in mortality among children with febrile seizures is restricted to those with complex febrile seizures. (86) Furthermore, the increased risk in those patients is explained by preexisting neurologic abnormalities and subsequent epilepsy. (87)
- Neurologic sequelae, including new neurologic deficits, intellectual impairment, and behavioral disorders, are rare following febrile seizures. (88)
- Children with status epilepticus (SE) have an overall mortality of approximately 0% to 3%. Considering only children admitted to pediatric intensive care units, the mortality is approximately 5% to 8%. Further, children surviving SE are at risk of lifelong sequelae, including cognitive and neurodevelopmental impairments, new-onset epilepsy, and recurrent SE. The occurrence of seizures and the recurrence of SE are influenced by the underlying etiology, with structural or metabolic lesions having the highest risk. (89)