Management of Kawasaki Disease and its Cardiac Sequelae
- Recommendations
|
Table A. Diagnosis of Kawasaki disease |
|||||
|
N |
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
A.1: |
When to suspect Kawasaki disease? |
SHARE 2019 CPG
|
The diagnosis of KD should be considered in any child with a febrile exanthematous illness and evidence of inflammation, particularly if it persists longer than 4 days. |
Low |
Weak |
|
A.2: |
What clinical criteria should be used to diagnose Kawasaki disease? |
AHA 2024
|
COMPLETE KD DIAGNOSTIC CRITERIA • Fever for at least 4 d + at least 4/5 principal clinical features at any point during the illness (does not need to be concurrent): • Polymorphous rash • Bulbar conjunctival injection without exudate; bilateral • Oral changes: Erythema and cracking of lips, strawberry tongue, or erythema of oral and pharyngeal mucosa, or all of these o Palmar and plantar erythema : usually accompanied by swelling; resolves with subsequent periungual desquamation in the subacute phase • Cervical adenopathy: usually unilateral, cluster of nodes ≥ 1 .5 cm in diameter • Illness is not explained by known alternative disease process |
Moderate |
Strong |
|
A.3: |
What is the definition of different types of KD (Classic/ Incomplete/ Atypical )? |
SIP 2018 CPG |
Typical or classic KD is diagnosed if a fever is ≥5 days, associated with ≥4 diagnostic criteria, with or without CAA, or if fever lasts at least for 4 days with ≥4 diagnostic criteria and eventual demonstration of CAA on echocardiography. Please refer to A.2
|
Moderate |
Strong |
|
AHA 2024 |
SUSPECTED INCOMPLETE KD DIAGNOSTIC CRITERIA • Prolonged unexplained fever and 2- 3/5 clinical criteria OR infants with unexplained fevers 7 d (day 1 = day of the onset of fever) AND compatible laboratory or echocardiographic findings: o CRP ≥ 3 m g/dL or ESR >40 m m/ h, or both. +3 or more of the following: - Anemia for age - Platelets ≥,450,000 - Album in ≤ 3 g/dL - Elevated ALT - Elevated WBCs ≥15 ,000/mm3 - Urine WBCs ≥10/hpf o Z score of LAD CA or RCA ≥,2.5 Or ≥3 other suggestive features exist, including decreased left ventricular function, mitral regurgitation, pericardial effusion or Z scores in LAD or RCA 2- 2.5 |
Moderate |
Strong |
||
|
SIP 2018 CPG |
Atypical KD is diagnosed if fever, not otherwise explained, lasting for ≥5 days is associated with classic diagnostic criteria and non-classic manifestations, with or without CAA. |
Moderate |
Strong |
||
|
A.4: |
What clinical criteria could increase suspicion of Kawasaki disease in incomplete Cases? |
SHARE 2019 CPG
|
In a patient in whom KD is suspected, but all criteria have not yet been fulfilled, the following clinical signs strengthen the suspicion of KD: Irritability New erythema and/or induration at the site of previous BCG immunization. * * It is now considered a principal criterion in Japanese Society of Cardiology Guidelines. |
Low |
Weak |
|
A.5: |
What are the main differences between KD and MISC-C? |
ARC/VF 2022 CPG |
MIS-C and KD may share overlapping clinical features, including conjunctival infection, oropharyngeal findings (red and/or cracked lips, strawberry tongue), rash, swollen and/or erythematous hands and feet, and cervical lymphadenopathy. |
High |
Strong |
|
Several epidemiologic, clinical, and laboratory features of MIS-C may differ from KD in the following ways: · There is an increased incidence of MIS-C in patients of African, Afro-Caribbean, and Hispanic descent, but a lower incidence in those of East Asian descent. · Patients with MIS-C encompass a broader age range, have more prominent GI and neurologic symptoms, present more frequently in a state of shock, and are more likely to display cardiac dysfunction (ventricular dysfunction and arrhythmias) than children with KD. · At presentation, patients with MIS-C tend to have lower platelet counts, lower absolute lymphocyte counts, and higher CRP levels than patients with KD. · Ventricular dysfunction is more frequently associated with MIS-C whereas KD more frequently manifests with coronary artery aneurysms; however, MIS-C patients without KD features can develop CAA. |
Moderate to high |
Strong |
|||
|
Epidemiologic studies of MIS-C suggest that younger children are more likely to present with KD-like features, while older children are more likely to develop myocarditis and shock |
|||||
|
Table B. Investigations |
|||||
|
N |
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
B.1: |
What are the initial laboratory tests for Kawasaki Disease and how can it help in diagnosis? |
SHARE 2019 CPG
|
The following laboratory values should be determined: ESR, CRP, full blood count and liver function (bilirubin, AST/ALT), albumin, serum Na, renal function, and urinalysis. Ferritin and fibrinogen should be considered if there is a concern for macrophage activation syndrome. |
Moderate |
Weak |
|
SHARE 2019 CPG
|
Cerebrospinal fluid analysis may be important to rule out infectious meningitis. |
Low |
Weak |
||
|
B.2: |
Can laboratory data diagnose KD? |
SIP 2018 CPG |
Laboratory data are nonspecific in KD and can only support diagnosis in patients with suggestive clinical features. |
Very low |
Strong |
|
B.3: |
In echocardiography, What protocol an echocardiographer should follow to evaluate cardiac and coronary affection (Timing of imaging, echocardiographic features, coronary imaging)? |
SHARE 2019 CPG |
All patients with suspected KD should undergo echocardiography and ECG at baseline, as soon as the diagnosis is suspected. An intermediate echocardiogram, 2 weeks after the first IVIG, should be performed in all patients with KD whose initial echo was normal and in whom disease activity has been arrested. |
High |
Strong
|
|
SIP 2018 CPG |
Echocardiogram must be performed in all patients with a diagnosis of KD; then after 2, 4, and 8 weeks since KD onset in uncomplicated cases, as CAA can be detected in the subsequent weeks after diagnosis. |
Very low |
Strong |
||
|
SHARE 2019 CPG
|
In those with ongoing active inflammation (increasing or persistently elevated CRP and/or persisting signs and symptoms), ECG and echocardiography should be performed at least weekly to monitor the possible development of cardiac sequelae. In those with coronary abnormalities detected on initial echocardiography, echocardiography should then be performed at least weekly to monitor progression until there is clinical stabilization. |
Moderate |
Strong |
||
|
SIP 2018 CPG |
Persistently febrile non-responders KD patients with CAA, impaired left ventricular function, mild/moderate mitral regurgitation or significant pericardial effusion need a more frequent echocardiogram check-up (at least twice per week). |
Very low |
Strong |
||
|
SHARE 2019 CPG
|
In children with CAA, ECG and echocardiography should be performed 3- to 6-monthly, depending on the severity of the CAA. |
Low |
Weak |
||
|
B.4: |
How can an echocardiographer classify coronary aneurysms? |
JSC\JSCS 2020 CPG |
For coronary artery sequelae, evaluation by Z-score is the standard method, and +2.5 or higher is defined as a long-term significant CAL (sequelae) |
Moderate |
Strong |
|
For those above the age of 5 years, the definition of a giant aneurysm is ≥8mm inside diameter. |
Moderate |
Weak |
|||
|
B.5: |
What are the other non-echocardiographic imaging modalities that should be used to evaluate cardiac affection in KD? |
SIP 2018 CPG |
Cardiovascular CT scan and MR angiography, where available, are important to assess persistent CAA in children with KD and monitor the remodeling of either coronary or systemic arteries in the whole body |
|
Good practice statement |
|
Cardiovascular CT scan, ideally with a DSCT scanner, should be used in patients with KD to: • Confirm CAA (and rule out false positive cases due to coronary artery anomalies or anatomical variants) • Detect middle-distal CAA (not usually seen at routine echocardiograms) • More accurately define the caliber and morphology of CAA and identify coronary artery thrombosis or occlusions • Evaluate other aneurysms, both central and peripheral, in the entire body • Reveal myocardial ischemia or reassess the caliber and morphology of CAAs and better define their treatment. |
Very low |
Weak |
|||
|
SHARE 2019 CPG
|
Cardiovascular MR angiography should be used in patients over 8 years with KD to: - Confirm CAA (and rule out false positive cases due to coronary artery anomalies or anatomical variants). - Identify other aneurysmal dilations, either central or peripheral, in the vascular system. - Assess biventricular global/regional systolic function. - Depict any myocardial scar with contrast enhancement and visualize gross coronary artery anatomy. |
Very low |
Weak |
||
|
Recommendation Table C. Management of Kawasaki disease |
|||||
|
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
|
C.1 |
What is the first line of treatment in the management of KD? |
ARC/VF 2021 CPG |
IVIG is the standard-of-care therapy for the initial treatment of KD. |
High |
High
|
|
SIP 2018 CPG |
IVIG must be administered at dose 2 g/kg of body weight in a single infusion, within the first 7th day of illness, anyway within the 10th day. Administration should be performed over 12 h if the patient’s cardiac function is normal, or in 16–24 h for patients displaying cardiac failure. |
High |
Strong |
||
|
SHARE 2019 CPG
|
All patients diagnosed with KD who are treated with IVIG should be treated with aspirin at a dose of 30-50 mg/kg/day until fever has settled for 48 h, clinical features are improving, and CRP levels are falling. |
Moderate |
Strong |
||
|
SHARE 2019 CPG
|
The dose of aspirin should subsequently be reduced to an antiplatelet dose of 3-5 mg/kg once daily when fever and inflammation have subsided. |
Moderate |
|
||
|
ARC/VF 2021 CPG |
For patients with acute KD, using aspirin is strongly recommended over no aspirin. |
Very low |
Very low |
||
|
C.2 |
When should physicians start treatment? |
SIP 2021 CPG |
IVIG is preferably given within the 10th day, better if within the 7th day of illness, but as soon as possible after diagnosis. |
|
Conditional |
|
SIP 2018 CPG |
IVIG should also be administered to children presenting after the 10th day of illness in case of: – persistent fever – no more fever but aneurysms and ongoing systemic inflammation, as shown by elevation of CRP |
Very low |
Strong |
||
|
SIP 2021 CPG |
IVIG should not be administered if fever spontaneously disappears and no CAA are shown, and if inflammatory markers (ESR and CRP) are within normal limits. |
|
Conditional |
||
|
C.3 |
How long should low dose aspirin be used in patients with acute KD? |
SIP 2018 CPG |
In patients without CAA low-dose ASA is to be discontinued 8 weeks after KD onset. In children who develop CAA low-dose ASA may be continued until the resolution of vascular lesions or indefinitely in case of its persistence. |
Very low |
Strong |
|
C.4 |
How should physicians modify initial treatment in high-risk patients |
SIP 2018 CPG |
High-risk KD patients should receive initial therapy with IVIG + ASA + corticosteroid. |
High |
Strong |
|
C.5 |
What risk factors are suggestive of IVIG resistance? (Laboratory risk assessment of IVIG resistance) |
SHARE 2019 CPG
|
The following laboratory values can be important in assessing risk stratification for IVIG resistance: · Low sodium · Raised bilirubin · Raised Alanine Transferase. · Low platelet count · High CRP · Low albumin. |
Moderate |
Weak |
|
JSC\JSCS 2020 CPG |
Resistant KD is defined by failure in the response to IVIG and is revealed by recrudescent fever reoccurring or persisting 36–48 h after IVIG infusion. The following features are elements of the risk scores for predicting IVIG resistance. (1) Leukocytosis with left shift (2) Thrombocytopenia (3) Hypoalbuminemia (4) Hyponatremia (5) Hyperbilirubinemia (jaundice) (6) Elevation of CRP. (7) Age <1 year |
High |
Strong |
||
|
C.6 |
How should physicians modify treatment in the presence of IVIG resistance? |
SIP 2021 CPG
|
In non-responders, treatment requires additional anti-inflammatory therapy including: second infusion of IVIG, Corticosteroids, anti-TNF alpha, or interleuin-1 antagonist |
|
Conditional |
|
C.7 |
When should corticosteroids be used in pediatric patients with Kawasaki? And what are the proposed regimens? |
SHARE 2019 CPG
|
Corticosteroid treatment should be given to patients with severe KD: (a) Who are IVIG resistant, that is, with ongoing fever and/or persistent inflammation or clinical signs ≥48 h after receiving IVIG as a single dose of 2 g/kg. A second dose of IVIG is at the discretion of the treating physician. (b) Kobayashi score ≥5 (c) With features of MAS. (d) With features of shock (e) Who are under the age of 1 year (f) Who present with coronary and/or peripheral aneurysms |
High
High
Moderate
Low Low Low
|
Strong
Strong
Weak
Weak Weak Weak |
|
SHARE 2019 CPG
|
Proposed regimen: If corticosteroids are indicated, the following regimens would be reasonable: Regimen 1: prednisolone 2mg/kg/D for 5-7 days or until CRP normalizes; wean off over next 2-3 weeks. Regimen 2: methylprednisolone 10-30 mg/kg (up to maximum of 1g/day) once daily for 3 days followed by oral prednisone/prednisolone 2 mg/kg per day until day 7 or until CRP normalizes; then wean over next 2-3 weeks. |
Moderate
|
Strong |
||
|
SHARE 2019 CPG
|
TNF-alpha blockade (e.g. infliximab) should be considered in KD patients with persistent inflammation despite IVIG, aspirin and corticosteroid treatment, after consultation with a specialist unit |
Moderate |
Strong |
||
|
SHARE 2019 CPG
|
The use of Disease Modifying Antirheumatic Drugs (DMARDs) such as ciclosporin, cyclophosphamide and methotrexate, along with anakinra and plasma exchange, cannot be recommended, except on an individual basis after consultation with a specialist unit. |
Moderate |
Weak |
||
|
C.7 |
How can physicians modify treatment in KD patients complicated by Macrophage Activation Syndrome? |
ARC/VF 2021 CPG |
For patients with acute KD and suspected or diagnosed MAS, treatment with IVIG for KD and additional agents to treat MAS is strongly recommended. |
Very low |
|
|
For children with unexplained MAS, obtaining an echocardiogram with coronary artery measurements is strongly recommended. |
|
Strong |
|||
|
Recommendations table D: Management of coronary involvement in children with KD |
|||||
|
D.1 |
How can physicians treat medium sized or multiple aneurysms in KD? |
SIP 2021 CPG
|
KD patients with medium-sized coronary artery aneurysms or those with multiple and complex aneurysms require dual anti-platelet prophylaxis, based on low-dose ASA (at a single dose of 3–5 mg/kg/day) and clopidogrel (at a single dose of 0.2 mg/kg/day in children aged < 24 months and up to 1 mg/kg/day in children aged ≥ 24 months). |
Moderate
|
Strong
|
|
D2 |
How can physicians treat complex or severe CAA (Z score > 10, diameter >8) aneurysms in KD? |
SIP 2021 CPG
|
• It is reasonable to treat KD patients having complex or severe CAA (Z score > 10, diameter >8) with low-dose ASA associated with warfarin (keeping INR targeted at 2.0–3.0) or LMWH (if regular INR checking is difficult). Triple therapy with ASA, warfarin or LMWH and clopidogrel should be considered in KD patients with a relevant risk of thrombosis. • Warfarin is used in combination with low-dose aspirin for patients with large CAA, history of MI, and thrombosis in the CAA. The dose is adjusted for the international normalized ratio of prothrombin time (PT-INR) target range of 2.0–2.5 |
Moderate |
Strong
|
|
D.3 |
How can physicians treat patients with thrombosed coronary aneurysms? |
SIP 2021 CPG
|
Recombinant tissue plasminogen activator (rtPA) is the first-choice thrombolytic drug in children with KD complicated by coronary artery thrombosis; the glycoprotein IIb/IIIa inhibitor abciximab may be used in case of thrombosis with high risk of occlusion. Both therapies require a concomitant association with low-dose ASA and intravenous heparin. |
Moderate |
Strong |
|
Recommendations table (E) Long term management of KD patients |
|||||
|
E1 |
How can physicians manage vaccination in children younger than 5 years of age with KD? |
SIP 2021 CPG
|
All inactivated vaccines can be safely administered at any time after IVIG in KD patients. Attenuated live virus vaccines (MMR, V, and MMRV vaccines) should be administered 10–12 months after the administration of IVIG to avoid a reduced specific immune response in KD patients. influenza vaccination is recommended in KD patients receiving ASA.
|
Moderate |
strong |
|
E2 |
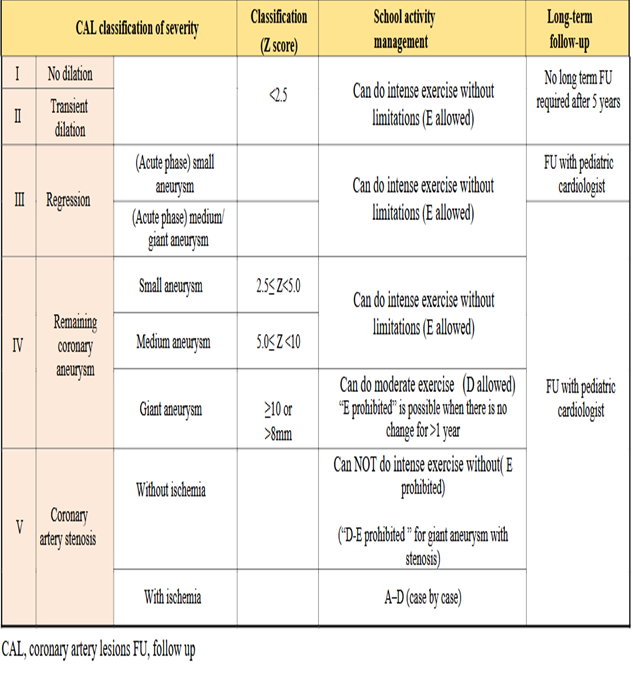
How can school activities be modified in patients post convalescence? |
JSC\JSCS 2020 CPG |
Level of management: A - Requires treatment at home or in hospital, B - Goes to school but must avoid exercise, C - Can do mild exercise, D - Can do moderate exercise, E - Can do intense exercise. Exercise intensity: Mild exercise: Physical activities that do not increase respiratory rate in average children at the same age, Intermediate exercise: Physical activities that increase respiratory rate without causing shortness of breath. Players may talk with others during exercise, and Intense exercise: Physical activities that increase respiratory rate and cause shortness of breath. Express the allowed exercise intensity from “A” to “E”. Only “E” will be noted as “Allowed” or “Prohibited” for school sport club activities and will be referred to as “E-allowed” or “E-prohibited”. |
|
Conditional |
|
E3
|
What is the long-term management of KD patients post convalescence? |
JSC\JSCS 2020 CPG |
Low-Dose Aspirin is orally administered to patients with persistent CAA |
High |
Weak |
|
JSC\JSCS 2020 CPG |
Statins should be used to prevent cardiovascular events in patients with CAL. |
Moderate |
Weak |
||
|
JSC\JSCS 2020 CPG |
ACEI or ARB may be used to prevent coronary artery stenosis in patients with CAL. |
Moderate |
Strong |
||
|
JSC\JSCS 2020 CPG |
Beta-blockers, Calcium antagonists, or nitrates can be used to prevent Acute coronary syndrome (ACS) in patients with CAL |
Moderate |
Strong |
||
|
E4 |
How can patients be safely transferred to adult care? |
JSC\JSCS 2020 CPG |
Preventing the loss of follow-up (the so-called dropouts) is the most important issue in the management of the adolescent and young adult (AYA) generation. |
Moderate |
Low |