UPPER AND LOWER EYELIDS AFFECTION
- V- Ectropion of the eyelid
Ectropion is an eversion or turning out of the eyelid margin.

Fig.22:
Bilateral ectropion in a young Labrador retriever (David et al, 2008).
Causes
Ectropion is classified according to the cause into:
1- Congenital ectropion
2- Acquired ectropion
a) Senile ectropion
b) Cicatrical ectropion
c) Intermittent ectropion
d) ectropion may result in severe secondary corneoconjunctival lesions if severe
enough and left untreated.
Treatment
A- Surgical correction when it causes conjunctivitis, keratitis, or exfoliative blepharitis due to epiphora or when it exacerbates keratoconjunctivitis sicca.
B- Correction is required much less frequently than for entropion.
Techniques used to correct different types of ectropion
1- Wedge Resection
A- The lower eyelid can be shortened by resection of a full-thickness wedge from the lateral end of the lower eyelid.
B- A standard two-layer closure is then used to perfectly appose the sides of the eyelid margin.
C- For ectropion due to either focal cicatricial contraction or a “notch” deformity in the lower eyelid, the wedge should be repositioned to remove the deformed or scarred tissue, the medial canthal area and nasolacrimal apparatus must be avoided.
2- “V-to-Y” Blepharoplasty
A- For cicatricial ectropion and in cases in which a small wedge resection is insufficient The V-to-Y (Wharton-Jones) blepharoplasty procedure is used.
B- It is particularly well suited to correction of ectropion due to a broad, contracted scar.
C- The V-to-Y blepharoplasty is begun with outlining of a triangular piece of skin with the base parallel and equal in length to the affected eyelid margin.
D- A skin incision is made along the two lower sides of the triangle, and the skin between them is undermined to elevate a V-shaped flap.
E- Scar tissue beneath the flap is excised.
F- The ventral ends of the incisions then are sutured together with simple interrupted sutures of 3/0 to 5/0 braided nylon or silk to form a vertical line perpendicular to the eyelid margin.
G- This vertical portion forces the triangle and eyelid margin superiorly.
H- The length of the vertical portion depends on how much elevation/inversion of the eyelid margin is required to return it to its normal position.
I- To allow for subsequent wound contraction, it should be about 2 to 3 mm longer than required.
J- The remaining parts of the two incisions are sutured to the free edges of the flap so that the sutured skin forms a Y.
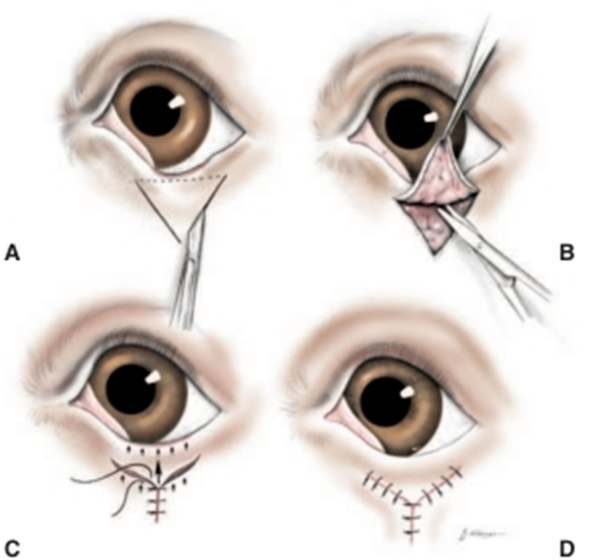
Fig.23:V-to-Y (Wharton-Jones) blepharoplasty (Moore and Constantinescu,1997).
A- A triangle of skin is outlined.
- The base is determined by the extent (width) of the lid margin affected by ectropion.
- The height of the triangle is determined by the extent of eversion to be corrected.
- A scalpel is used to incise the skin along the two sides but not the base of the triangle.
A- The skin flap created is elevated and undermined, along with any scar tissue.
B- The two sides of the triangle are sutured together to form the vertical portion of the Y.
- The length of the vertical portion of the wound is determined by the extent of eyelid eversion. Arrows show the tissue forces created.
C- The incisions are closed so as to form the two arms of the Y.