NICTITATING MEMBRANE (THIRD EYELID)
- Prolapse of the nictitans gland (or “cherry eye”)
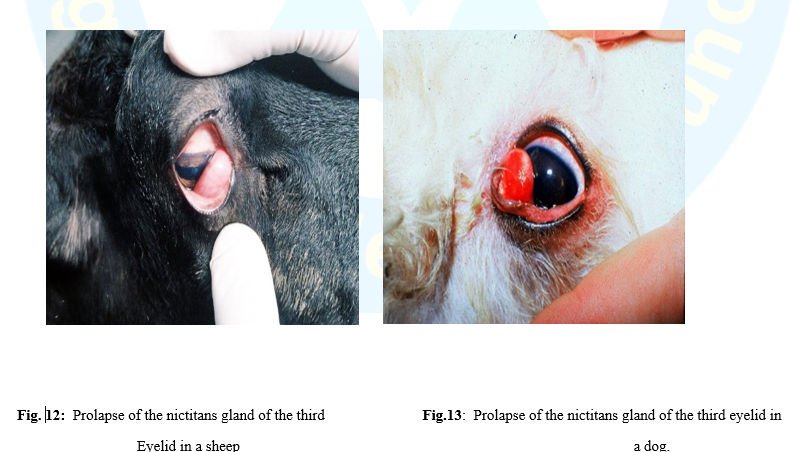
Prolapse of the nictitans gland over the free border of the third eyelid also known as hypertrophy, hyperplasia, adenoma of the nictitans gland and cherry eye. The nictitans gland protrudes from behind the nictitating membrane as a reddish mass over its free border. The normal gland has a connective tissue bands anchoring it to the periorbital tissues at the base of the membrane. When these bands are not developed properly, the gland moves towards the free edge of the membrane. The movement of the membrane causes the gland to prolapse outwards. Inflammation and hypertrophy of the gland develop as soon as the gland is prolapsed.
Causes:
1- Congenital, perhaps hereditary weakness of the connective tissue bands between the gland and periorbital tissues.
2- Trauma to the third eyelid or orbit. The condition is seen frequently in dogs and reported in cat, sheep and buffalo.
3- It likely results from lymphoid hyperplasia (in young animals exposed to environmental antigens for the first time) and laxity of the retinaculum that should attach the third eyelid to the periorbita. This combination of events allows the gland to evert while remaining attached to the cartilage of the third eyelid.
Symptoms:
1- A rounded, cherry or pea-like mass appears at the medial canthus of the eyeball. The condition is usually bilateral.
2- Secondary epiphora and conjunctivitis may occur.
Treatment:
- Prolapsed glands of the third eyelid are treated by replacement, not by excision. Since the gland accounts for a significant part of the tear production, neither the gland nor the entire nictitating membrane should be removed. The purpose of treatment is to relocate the gland in its normal position.
- In cases of recurrence, the gland may be excised but the owner should be warned in advance about the high risk of KCS. Grasp the gland by fixation forceps and apply a mosquito artery forceps at its base for a minute and then cut it by a scissors. An alternative procedure is that the bulbar conjunctiva is incised first over the gland and bluntly dissected from it then the mosquito artery forceps is applied to the base of the gland. Hemorrhage is controlled, if present, by light pressure on the surgical wound for few minutes. Antibiotic-corticosteroid ophthalmic ointment is applied twice a day for 5 days postoperatively.
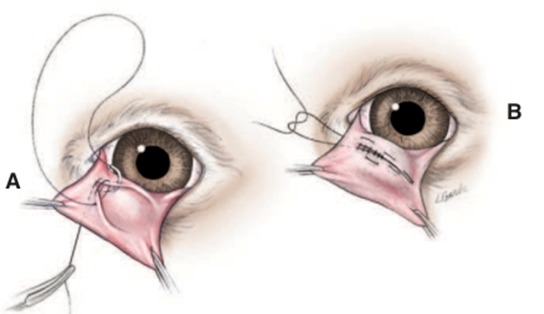
Fig.14: Surgical replacement of a prolapsed gland of the third eyelid (“cherry eye”) via a modification of the conjunctival pocket technique of Morgan. A, Two semielliptical incisions are made through the bulbar conjunctiva around the periphery of the prolapsed gland. The outer (free) edges of conjunctiva created by these incision are then apposed over the prolapsed gland using 4/0 to 6/0 absorbable suture, such as polyglactin 910 (Vicryl) in a simple continuous pattern. The initial and final anchorin knots are placed on the anterior face of the third eyelid to avoid frictional irritation of the cornea. B, The second (Cushing) layer of a continuous Connell-Cushing pattern is then placed with bites parallel to the conjunctival incisions, and, again, knots are placed on the anterior face of the third eyelid. (Stanley and Kaswan ,1994).