Neonatal Resuscitation Guide
| Site: | EHC | Egyptian Health Council |
| Course: | دلائل الاجراءات التمريضية لقسم حديث الولاده |
| Book: | Neonatal Resuscitation Guide |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 9:14 AM |
Description
"last update: 22 January 2025" تحميل الدليل
- Prepared by
NICU guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Professor of Obstetrics and Gynecology Nursing |
Dr. Nagat Salah Shalabi Salama |
12 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Shaima Abdel Basset Ibrahim Salim |
13 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Hoda Al-Sayd Muhammad |
14 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Walaa Ahmed Ali |
15 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Omnia Abdel Qader Muhammad |
16 |
|
member of the Nursing administration at EHA- South Sinai branch |
Mrs. Yasser Abdel Karim Omar Abdel Jawad |
17 |
- Apgar Score
- The Apgar score should not be used as the sole basis for deciding whether to start or continue resuscitation. Decisions about the course of resuscitation are not based on Apgar alone; the timing in resuscitation is measured in seconds, not minutes, although the score is used for overall assessment of the resuscitation process.
- The Apgar score is calculated for every newborn at 1, 5, and 10 minutes after birth.
- The 1-minute Apgar indicates the newborn’s need for further resuscitation steps and the degree of asphyxia around the time of birth.
- The score is expressed as a whole number only (no fractions) and ranges from 0 to 10.
Components of the Apgar Score:
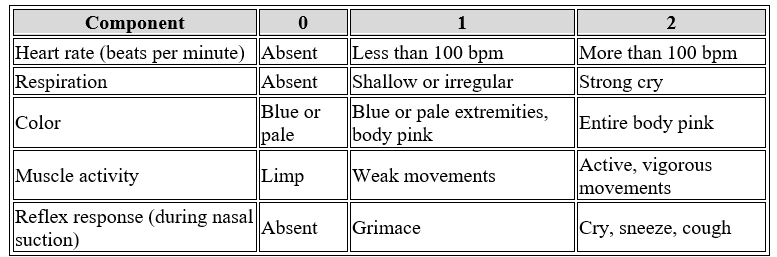
Interpretation of Apgar Score Results:
- If the Apgar score is 7–10, this indicates no neonatal distress.
- If the Apgar score is 4–6, this indicates moderate distress.
- If the Apgar score is 0–3, this indicates severe distress.
- A high Apgar score at the fifth minute indicates the success of the resuscitation process, while a low score at the fifth minute emphasizes the need to continue resuscitation steps.
- If the score is less than 7, reassessment should be done every 5 minutes until the score reaches 7 or higher, continuing up to 20 minutes.
- Neonatal Resuscitation
Introduction:
The first moments of a newborn’s life are considered the “golden moment” and are
among the most critical and dangerous for the infant’s survival. Therefore, the
neonatal nurse must anticipate potential problems the newborn may face due to
the inability to initiate effective ventilation, ensuring successful
resuscitation without complications.
The role of the neonatal unit nurse can be divided into five stages:
First: Before Birth (Preparation):
- Respond immediately upon receiving the birth notification and ensure the resuscitation kit is complete.
- Ensure the resuscitation area is prepared and contains:
- A clean, functioning warming device, securely mounted vertically on the wall and turned on 10–20 minutes before birth.
- A manual or electric suction device, clean and functioning, specifically for neonates; check suction power to ensure it is between 80–100 mmHg.
- An oxygen source connected to a flowmeter and oxygen tubing.
- A neonatal resuscitation kit or mobile emergency trolley, checked and signed off at the start of each shift, containing:
- Neonatal Ambu bag (200–750 mL) with face masks (sizes 0, 1, 2).
- Laryngoscope with straight blade: size 0 for preterm, sizes 00 or 1 for full-term, with functional light check.
- Endotracheal tubes (sizes 2, 2.5, 3, 3.5, 4).
- Cannulas (sizes 24, 26), suction catheters (size 6), umbilical catheters (sizes 3.5, 5).
- Sterile scalpel and umbilical clamp.
- Sterile gloves and mucus suction device.
- Adhesive tape, airway devices.
- Feeding tube (size 6).
- Syringes (1 mL, 3 mL, 5 mL, 10 mL).
- Ampoules: Adrenaline, Vitamin K, Solu-Cortef, Atropine.
Second: During Birth:
- Connect the oxygen tubing to the flowmeter and adjust flow to 5–8 L/min.
- Attach an appropriately sized suction catheter to the suction device, keeping it in its pouch.
- Ensure the Ambu bag mask fits properly, and check for leaks by placing it on the palm.
- Connect the appropriately sized laryngoscope blade and confirm the light works; use only when needed.
- Apply infection control measures throughout all steps.
- Assess readiness for neonatal resuscitation:
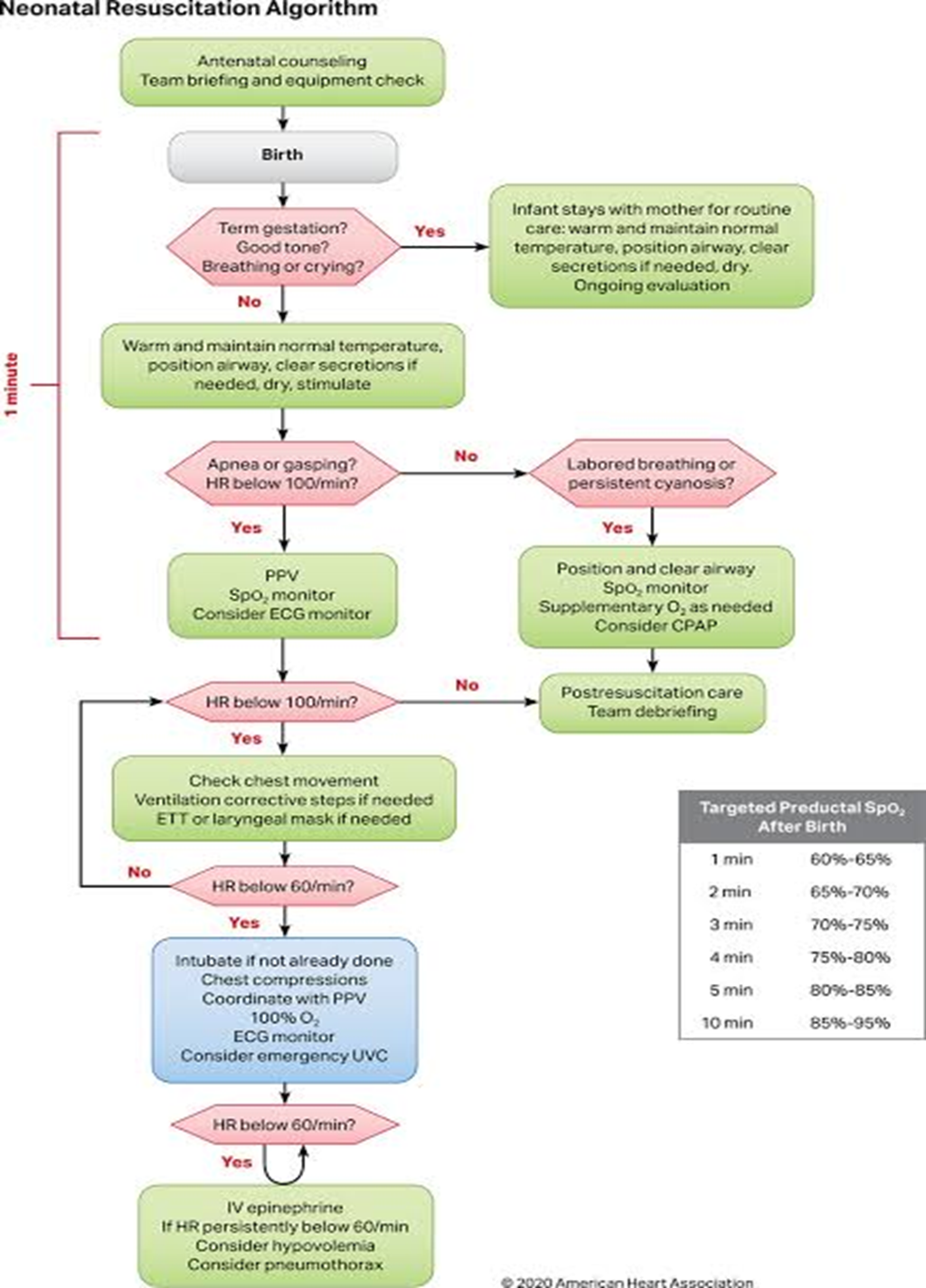
Rapid Initial Assessment (answer three questions):
- Was the gestation full-term?
- Does the newborn have good muscle tone?
- Is the newborn breathing or crying?
- If all answers are “yes,” the newborn stays with the mother for routine care:
- Dry the infant with a sterile towel to maintain temperature.
- Observe breathing, activity, and color continuously.
- Skin-to-skin contact with the mother.
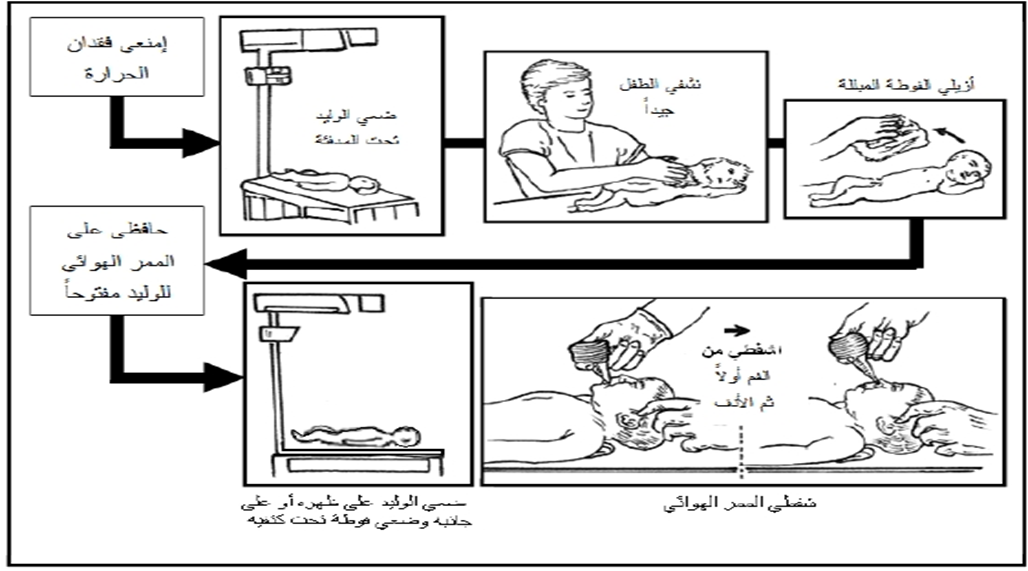
- If any answer is “no,” transfer the newborn to the warming device and follow these steps:
- Stabilize the infant (maintain normal temperature, proper positioning, clear airway if secretions are present, dry, and stimulate).
- Provide oxygen and adequate ventilation.
- Begin chest compressions if needed.
- Administer medications (e.g., adrenaline).
- Delay umbilical cord clamping for 1–3 minutes after birth, unless immediate intervention is required due to asphyxia, to reduce neonatal anemia, improve tissue oxygenation, and stabilize circulation and blood pressure.
Third: Initiating Neonatal Resuscitation Steps:
- Receive the newborn in a warm, sterile towel from the obstetrician, avoiding holding the baby by feet or head downward.
- Place the newborn on their back under the warming device, with the head toward the resuscitation nurse.
- Dry the newborn thoroughly, especially the head, and discard wet towels.
- Maintain airway patency by placing a towel under the shoulders (sniffing position).
- Gently suction the mouth first, then the nose, for no more than 5 seconds.
- Stimulate the newborn by gently rubbing the back or tapping the soles of the feet if spontaneous breathing does not start.
- If the amniotic fluid is meconium-stained and the baby is limp, perform full resuscitation on the servo device. Begin ventilation using the Ambu bag and mask if the newborn is not breathing and heart rate is below 100 bpm.
- Endotracheal intubation for meconium suction is no longer routinely recommended.
Fourth: Assessment
- Evaluate the newborn’s condition based on heart rate, respiratory effort, and color.
- An increase in heart rate during resuscitation is the most important indicator of successful resuscitation. Continuous monitoring of heart rate is essential during resuscitation, as it also reflects respiratory status and the need for further interventions. Assessment is done using three electrodes connected to a monitor for accurate heart rate measurement, which is more precise than manual pulse counting. Respiratory effort is evaluated by checking for apnea (pauses in breathing), and color is assessed for cyanosis.
Continuation of Resuscitation Steps
- If there is no apnea and the heart rate is above 100 bpm, but the newborn has respiratory distress or central cyanosis:
- Adjust position, suction the airway, monitor oxygen saturation (SpO₂), provide free-flow oxygen per physician orders, and apply CPAP if needed.
- Reassess the infant: if improved, proceed with post-resuscitation care; if not, or if heart rate drops below 100 bpm, begin ventilation using Ambu bag.
- If there is apnea and the heart rate is below 100 bpm:
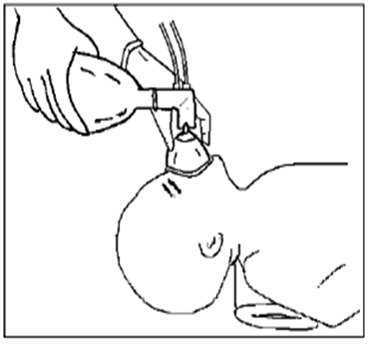
- Perform ventilation using Ambu bag and mask while monitoring heart rate and SpO₂ as follows:
- Ensure the head is in the sniffing position; place a towel under the shoulders if necessary; confirm airways are clear.
- Place appropriately sized mask over the chin, mouth, and nose without touching the eyes. Ventilate following a “1–2–3” system, adjusting squeeze strength according to the newborn’s chest rise.
- Observe chest rise during ventilation and adjust squeeze strength; intubate if required.
- Reassess heart rate:
- If improved, proceed with post-resuscitation care.
- If not improved, continue ventilation; if heart rate drops below 100 bpm, continue Ambu ventilation.
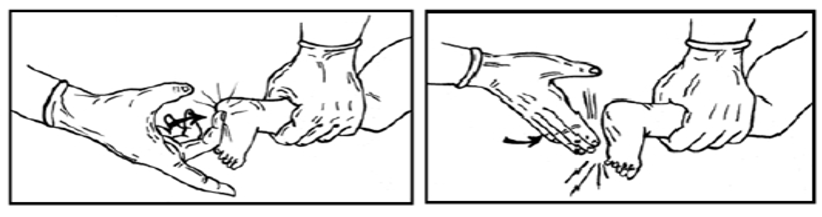
- If heart rate drops below 60 bpm, intubate if not already done and begin chest compressions while continuing ventilation:
- Place thumbs on the lower third of the sternum, wrap hands around the chest with fingers meeting behind the back, or place index and middle fingers of one hand on the lower third of the sternum and the other hand supporting the back. Compress the chest about one-third of its lateral diameter.
- Coordinate compressions with ventilation using the “three compressions” system, taking ~2 seconds per cycle, totaling 120 actions per minute (90 compressions to 30 breaths per minute).
Important Note:
- The “1–2–3” system is used when respiratory compromise is the primary cause.
- If cardiac problem is the main cause, use the higher rate system: 15 compressions : 2 breaths.
- If heart rate remains below 60 bpm:
- Insert an umbilical catheter, administer IV adrenaline, correct fluid deficits, and take measures to prevent pneumothorax.
Fifth: Medication Administration
- If heart rate remains below 60 bpm:
- An umbilical catheter is inserted by the pediatrician.
- Diluted IV adrenaline is administered (dose per physician’s instructions).
- Fluid deficits are corrected using volume expanders as directed (e.g., 0.9% saline or Ringer’s lactate).
Note:
- If prolonged ventilation with an Ambu bag is required, a feeding tube (Ryle tube) should be inserted to decompress the stomach, preventing diaphragmatic pressure and allowing full lung expansion.
Termination of Resuscitation
- If the newborn does not breathe or the heart does not beat after 15 minutes of full resuscitation efforts, resuscitation is stopped, and emotional support is provided to the mother and family.
- If the newborn responds to resuscitation, they should remain under a warming device with close monitoring until stable.
- The newborn may be transferred to the neonatal care unit for ongoing care if needed, with continuous monitoring of vital signs and observation for abnormal signs such as apnea, increased respiratory effort, or central cyanosis, and the physician should be notified immediately.
Ethical Considerations in Resuscitation
- Written consent should be obtained from parents if resuscitation is not to be continued.
- According to physician judgment, resuscitation may not be attempted in the following cases:
- Gestational age less than 22 weeks.
- Severe congenital malformations affecting multiple body parts.
Routine Post-Resuscitation Care
- Care of the umbilical cord.
- Administration of Vitamin K.
- Instillation of antiseptic eye drops.
- Maintain stable body temperature.
- Initiate breastfeeding.
- Promote maternal-infant bonding immediately after birth.
- Encourage skin-to-skin contact.
- Identification of the newborn.
- Record the newborn’s weight.
After Completion of Resuscitation
- Dispose of used instruments in their designated locations.
- Clean and disinfect the warming device.
- Disinfect the Ambu bag, masks, and laryngoscope blade.
- Record resuscitation duration and interventions in the mother’s or newborn’s record.
- Replenish used items in the resuscitation kit upon return to the neonatal care unit.
- Cardiopulmonary Resuscitation (CPR)
- Assessment:
- Check responsiveness and palpate the brachial pulse.
- Basic Resuscitation:
- Perform chest compressions with two fingers at a depth of 4 cm, at a rate of 100–120/min.
- If two rescuers: 15 compressions followed by 2 breaths; if alone: 30 compressions followed by 2 breaths.
- Defibrillation (if needed):
- Use infant/child pads; adult pads can be adapted if necessary.
- Airway Management:
- Use a laryngeal mask airway (LMA) or small endotracheal tube, confirming placement via CO₂ monitoring or auscultation.
- Continuous Assessment:
- Monitor the infant’s response and adjust interventions as needed.
Staff Education and Preparedness for Neonatal Emergencies:
- All hospital staff must be familiar with neonatal emergency recognition.
- All staff should know how to activate Code Blue.
- All staff trained in Basic Life Support (BLS).
- Code Blue pediatric team must have successfully completed BLS, PALS, and ACLS.
- The quality and training departments coordinate simulations to ensure rapid response.
Code Blue Activation Locations:
- Active: inpatient wards, non-medical and medical departments (e.g., sterilization, radiology)
- Silent: intensive care units, nurseries
Code Blue Pediatric Team Composition:
- Pediatrician
- Head nurse or designated substitute
- 2 NICU nurses
- Ward charge nurse
- Attending physician or nurse in charge if needed
|
Team Member |
Tasks and Responsibilities |
|
Team Leader (Pediatrician/Attending Physician) |
- Manages the entire resuscitation process to ensure effective and efficient execution. - Coordinates interventions such as administering defibrillation, inserting an endotracheal tube, and giving medications. - Assesses the patient’s condition. - Requests assistance or additional investigations if needed. - Organizes post-resuscitation care and ensures proper documentation of all procedures. |
|
Nursing Team |
- Tasks are assigned by the team leader as follows: • One nurse provides ventilation while another performs chest compressions. • One nurse records all steps and notes observations. • One nurse inserts and manages IV lines. • One nurse handles the crash cart and operates the defibrillator. • Participates in documenting the Code Blue report. |
|
Attending Physician |
- Provides detailed information about the patient’s medical condition. - Reviews the patient’s file and informs the team leader of any critical information. - Assists in performing chest compressions and advanced CPR as needed. |
|
Anesthesiologist (if required) |
- Manages the airway and performs endotracheal intubation. - Establishes IV access if standard attempts are unsuccessful. |
Other Personnel Not Included in the Core Team:
- Security Officer: Responsible for managing crowd control, clearing the area except for the Code Blue team, securing the patient’s belongings, and accompanying the deceased to the morgue while confirming the identity of the deceased.
Mechanism for Activating Staff Response (Including Emergency Code):
- The first responder calls loudly for help and activates Code Blue, stays with the patient, ensures the safety of the surroundings, and begins basic CPR.
- The assisting staff member contacts the switchboard number announced to all staff to activate the Code Blue alert and assists the first responder with basic CPR until the team arrives.
- The responsible staff announces the Code Blue, specifies the location and department, and repeats three times clearly and loudly.
Response Timeframe:
- Response must be immediate, as cardiac arrest can lead to death within minutes if resuscitation is not started promptly. The Code Blue team should reach the designated location within 3 minutes.
24/7 Unified Response:
- The Code Blue team responds around the clock, 24 hours a day, 7 days a week.
- Heads of relevant departments (e.g., ICU) prepare monthly Code Blue schedules, reviewed by the medical director.
- The nursing administration prepares monthly staff rotation schedules for the response teams.
Documentation and Handling of Medical Emergencies & Cardiac Arrest:
Documentation of Response:
- The nurse responsible for recording provides a summary of events to the nurse tasked with writing the Code Blue report, or records it herself.
- The team leader completes the form and performs an audit on recorded data and procedures performed.
- The form is submitted to the relevant unit supervisor.
- The unit supervisor sends it to the Quality Department for review and places a copy in the patient’s file.
- The Quality Department monitors all Code Blue events and reports them to improve performance.
Handling Medical Emergencies and Cardiac Arrest:
- If the patient is away from a medical service area (e.g., parking lot, rooftop, sterilization, laundry, kitchen), the designated Code Blue team responds with mobile resuscitation equipment (emergency bag).
- Emergency carts are strategically distributed throughout the hospital.
Emergency Bag Deployment in the Hospital:
- If the patient is in a medical service area, advanced cardiac life support (ACLS) begins immediately upon Code Blue team arrival.
- The team starts advanced CPR, connects the patient to 100% oxygen, monitor, and ECG machine.
- All team members are fully aware of the locations of emergency carts.
- Emergency carts must be accessible, fully stocked for both children and adults, and ready for immediate use.
- One team member retrieves the emergency cart from the designated location under supervision.
- Each Code Blue member knows their assigned role as delegated by the team leader.
- The team leader decides on the use of the defibrillator based on the patient’s condition.
- The team continues resuscitation until the leader decides to terminate.
- The attending physician informs the patient’s family about condition changes and outcomes.
- After CPR completion, the emergency cart is checked and restocked according to the hospital’s emergency supply policy.
- Neonatal Shock
Shock is a serious and acute condition of circulatory failure and insufficient oxygen to meet the needs of the neonate's tissues and vital organs. This deficiency may result from blood loss, weak heart muscle, or septicemia, causing cells to rely on anaerobic metabolism for energy, which leads to increased blood acidity.
Causes:
- Hemorrhage and significant blood loss, either before birth (e.g., placental abruption) or after birth (e.g., coagulation disorders, severe pulmonary hemorrhage).
- Neonatal asphyxia
- Bacterial contamination of the amniotic fluid and severe septicemia
- Congenital heart defects, such as aortic valve obstruction
Symptoms:
Symptoms and signs depend on the stage of shock:
- Early shock:
- Increased heart rate (sometimes decreased in neonates <1000 g)
- Weak peripheral perfusion; prolonged capillary refill (>3 seconds)
- Cold, cyanotic extremities
- Pale or mottled skin
- Established shock:
- Increased heart rate
- Low blood pressure
- Oliguria or anuria
- Lethargy
- Muscle hypotonia
- Advanced shock:
- Signs of vital organ failure (lungs, kidneys, brain, heart)
- Irreversible shock:
- Final stage of shock, characterized by:
- Oxygen deficiency and respiratory distress (cyanosis, tachypnea, grunting, chest retractions)
- Acidosis
- Arrhythmias
- Coma
Treatment:
- Prevention is the best strategy. If shock occurs, early recognition and a prioritized, goal-directed plan are essential to avoid serious complications.
- Administer 10–20 ml/kg of volume expanders (e.g., saline, Ringer’s, plasma) as directed by the physician.
- Monitor central venous pressure if possible to assess fluid balance.
- Treat hypoxia and hypoglycemia.
- Administer dopamine, dobutamine, or adrenaline according to physician instructions.
Nursing Care:
Maintaining Airway and Oxygenation:
- Keep airway open and ensure proper ventilation and oxygenation.
- Suction secretions if present.
- Monitor respiratory status and oxygen saturation using a monitor.
- Administer oxygen as needed according to blood gas results and physician orders.
Maintaining Circulation:
- Monitor vital signs, especially pulse, blood pressure, and temperature.
- Assess peripheral perfusion via capillary refill.
- Monitor consciousness and activity.
- Correct acidosis and ensure organ perfusion with medications such as dopamine, dobutamine, or sometimes adrenaline per physician instructions.
Controlling Bleeding and Replacing Fluids:
- Take measures to stop bleeding.
- Administer IV fluids via peripheral cannula or umbilical catheter.
- Transfuse blood products as directed.
Treatment of Septicemia:
- Administer antibiotics according to the identified pathogen and physician instructions.