Newborn Assessment Guide
| Site: | EHC | Egyptian Health Council |
| Course: | دلائل الاجراءات التمريضية لقسم حديث الولاده |
| Book: | Newborn Assessment Guide |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:55 AM |
Description
"last update: 26 January 2025" تحميل الدليل
- Prepared by
NICU guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Professor of Obstetrics and Gynecology Nursing |
Dr. Nagat Salah Shalabi Salama |
12 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Shaima Abdel Basset Ibrahim Salim |
13 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Hoda Al-Sayd Muhammad |
14 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Walaa Ahmed Ali |
15 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Omnia Abdel Qader Muhammad |
16 |
|
member of the Nursing administration at EHA- South Sinai branch |
Mrs. Yasser Abdel Karim Omar Abdel Jawad |
17 |
- Initial Nursing Assessment of Newborns
Purpose:
- Identify the nursing needs of each sick child to develop an appropriate nursing plan based on those needs.
Procedures:
A. Patient Admission by the Nursing Staff:
- The responsible nurse introduces herself to the child's guardians and greets them.
- The nurse verifies the patient's information (full name, mother's full name, age, gender, nationality, and medical record number).
- The nurse prepares an identification bracelet for the newborn, including:
- Full name if a birth certificate is available.
- Mother's full name and medical record number if a birth certificate is not available.
- The bracelet should indicate "Son/Daughter of [Mother’s Name]."
- Conduct a comprehensive physical assessment.
B. Nursing Assessment:
- The responsible nurse or an accredited assistant nurse conducts the initial nursing assessment for newborns upon admission.
- The newborn assessment includes:
- Vital signs measurement
- Length, weight, head circumference, and abdominal circumference
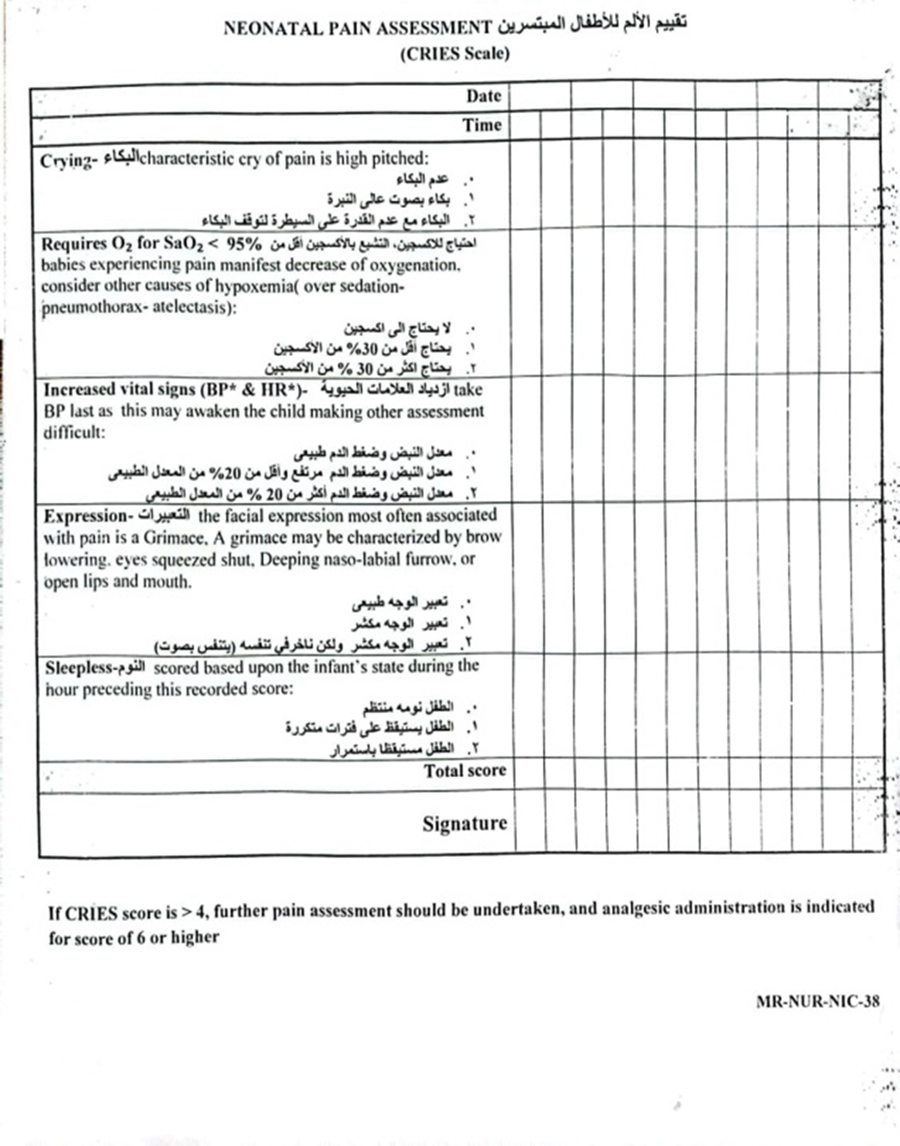
- Pain assessment using the CRIES scale
- Vaccination status
- Neurological condition
- Nutritional assessment
- Skin condition screening
- Examination for congenital anomalies
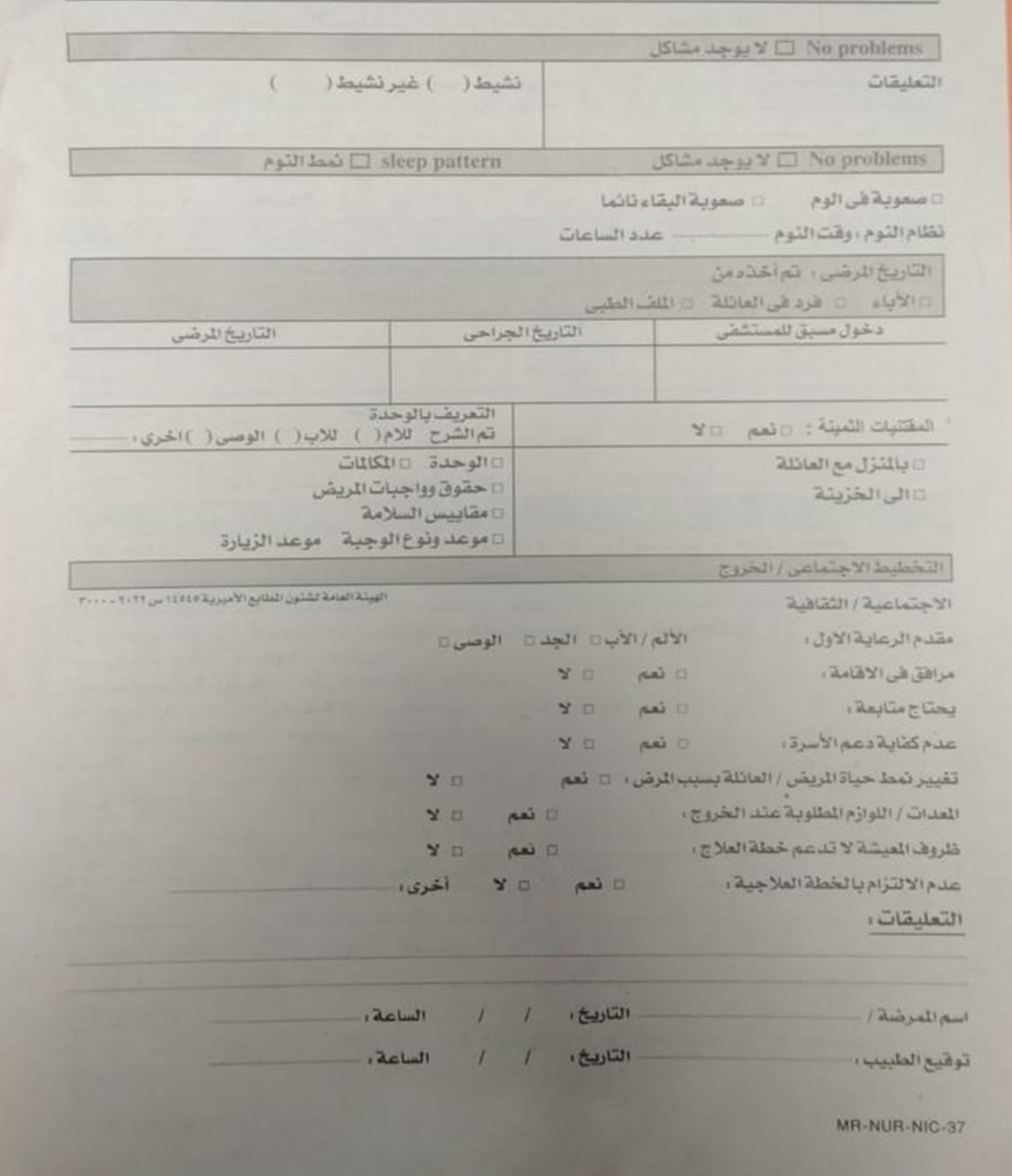
- Sleep pattern
- Medical history (obtained from the guardians)
- Discharge planning
C. Reassessment:
- The responsible nurse re-evaluates the child's condition whenever there is a change in treatment, care stage, or diagnosis, documenting it in the nursing notes.
- The nurse conducts reassessments as follows:
- Vital Signs Reassessment:
- Every 3 hours for preterm infants in incubators or as per the doctor's instructions.
- Every hour for post-open-heart surgery cases and isolation unit patients.
- Documented in the vital signs chart.
- Skin Condition Reassessment (Bedsores):
- Every 24 hours, documented in the Newborn Skin Risk Assessment (NSRA) form.
- Pain Reassessment:
- Every 12 hours.
- In case of pain occurrence.
- Before and after surgeries.
- One hour after pain relief treatment.
- As per doctor's orders.
- Documented in the pain assessment form.
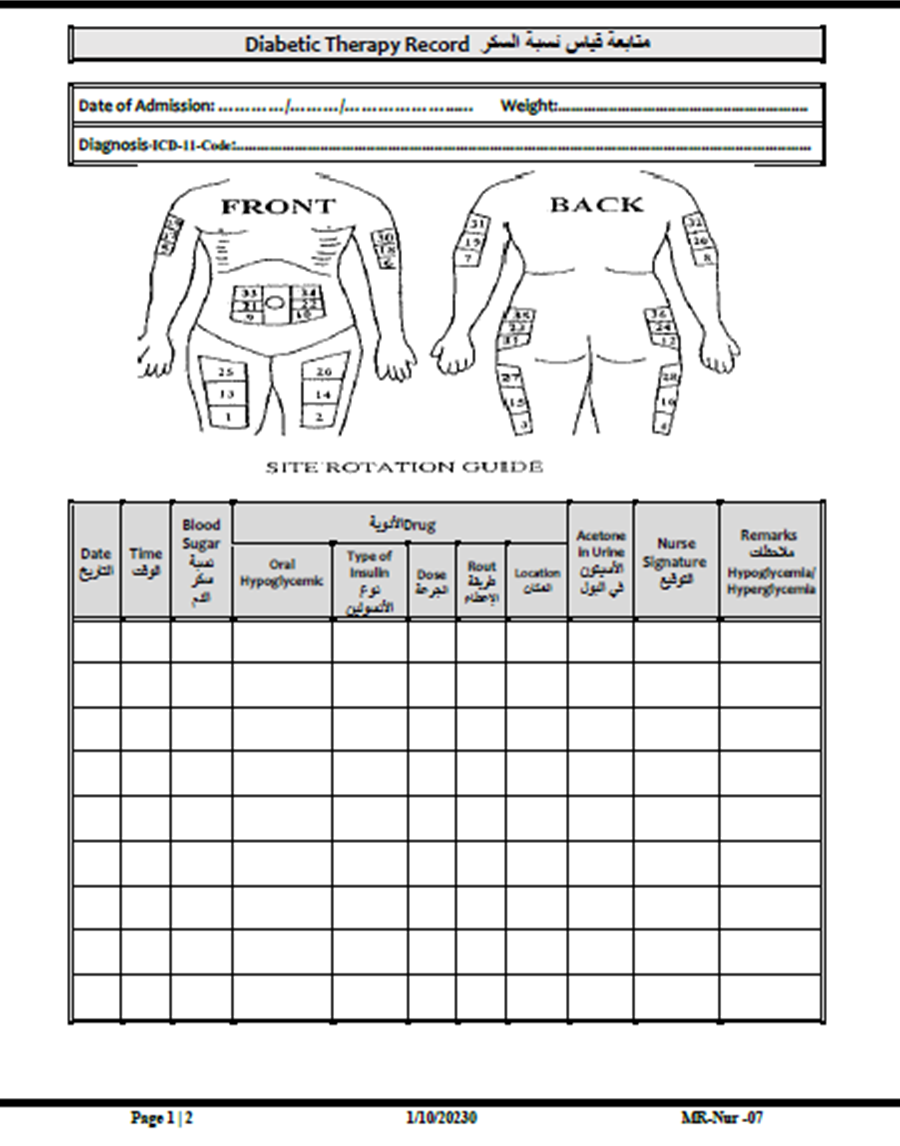
- Blood Sugar Reassessment:
- Every 6 hours (or as per the doctor's orders), documented in the blood sugar monitoring form.
D. Nursing Care Plan:
- The nurse develops a nursing care plan based on the newborn’s needs and updates it in case of any medical interventions or complications.
E. Documentation:
- The nurse completes the initial newborn assessment within 12 hours of admission to the neonatal unit or as per hospital policy.
5. Responsible Personnel:
- The responsible nurse overseeing the case.
6. Attachments:
- Newborn Initial Assessment Form
- CRIES Pain Assessment Form
- Newborn Skin Risk Assessment (NSRA) Form
- Blood Sugar Monitoring Form

- Nursing Care Plan
Purpose:
- Develop a care plan for each patient in the hospital across different specialties under the supervision of the responsible physician, ensuring comprehensive, evidence-based, and standardized care.
- Documenting the care plan ensures that medical staff, nursing staff, and other healthcare professionals achieve integrated and consistent patient outcomes.
- Promote collaborative teamwork based on a shared understanding of the best approach to managing the patient’s condition.
Steps:
The nursing team shall:
- Conduct a nursing assessment upon the child's admission to identify the patient’s problems.
- Record the child's nursing issues in the nursing care plan according to NANDA (North American Nursing Diagnosis Association).
- Document the necessary interventions to help resolve the identified nursing problems.
- Set a specific timeframe for reassessment based on each issue.
- Reassess the patient to determine their response to nursing interventions.
- Engage the child’s guardians in their care plan to ensure effective participation in the recovery process.
Responsible Personnel:
- Nursing staff in the department.
Attachments:
- Nursing Care Plan Template.
- Abuse and Neglect Assessment
Purpose:
- Establish guidelines and procedures for caring for at-risk patients by preventing unintentional or thoughtless actions that could cause injury or harm.
- Provide support and guidance to all medical team members in managing patients who may be at risk.
- Ensure respect for the rights, privacy, and dignity of vulnerable patients, particularly those with special needs.
Patients with Special Needs Who Are at Risk of Abuse and Neglect
Types of Abuse:
1. Mental Abuse (Psychological or Emotional Harm):
- Physical or verbal threats
- Intimidation
- Isolation
- Insults
- Humiliation
- Deprivation
2. Physical Abuse:
- Infliction of harm on the child’s body through (hitting, slapping, kicking)
Signs of Physical Abuse:
- Child falling or unexplained injuries
- Bedsores
- Untreated wounds
- Unexplained bruises or cuts
- Pain when touched
- Bite marks, scratches, abrasions, or bruises
- Signs of dehydration, malnutrition, sunken eyes, or eye injuries
3. Financial Abuse:
- Theft
- Misuse of money or property
- Extortion of the child’s guardians
- Fraudulent activities
- Unusual transactions in the child’s guardians’ bank accounts
- Reckless or irresponsible financial management
4. Neglect:
- Failure to provide necessary care without a valid medical reason by a responsible person during the child’s hospital stay.
Definition of a Vulnerable Patient:
- A person requiring assistance due to (intellectual disability, young age, brain atrophy, or functional impairment) that hinders their ability to protect themselves or provide self-care.
Potential Types of Neglect:
- Failure to provide adequate medical or nursing care
- Neglect in administering prescribed treatments
- Failure to meet social and psychological needs
- Lack of sufficient food and water
- Placing the patient in an unsafe environment without supervision
Procedures:
- The physician and nursing staff assess the child’s condition and determine their treatment needs.
- The physician and nursing staff inform the child’s guardians about the treatment plan and how it will be implemented.
- The ward supervisor conducts daily rounds to detect any signs of neglect or abuse, reporting them to hospital administration for appropriate action.
- If a case of abuse or neglect is identified:
- The attending physician evaluates the child’s condition, documents any signs of abuse or neglect, and ensures appropriate medical and psychological treatment.
- The physician encourages the guardians to submit a formal complaint if they choose, with or without their signature.
- The head of the medical team assigns the Patient Satisfaction Department to investigate the complaint and submit the findings for appropriate action.
Responsible Personnel:
- Physician
- Nursing staff
- Patient Satisfaction Department
Attachments:
- Abuse and Neglect Assessment Form
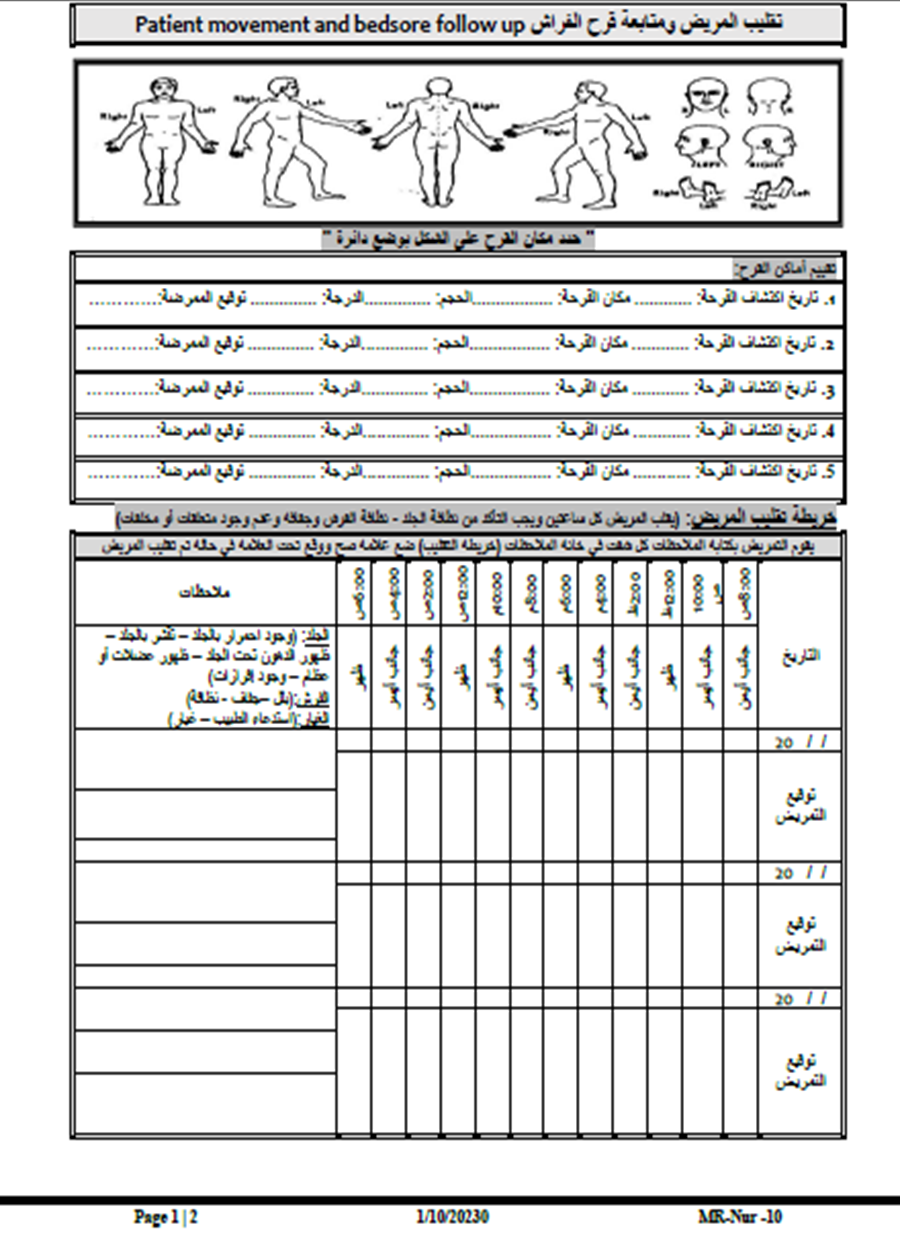
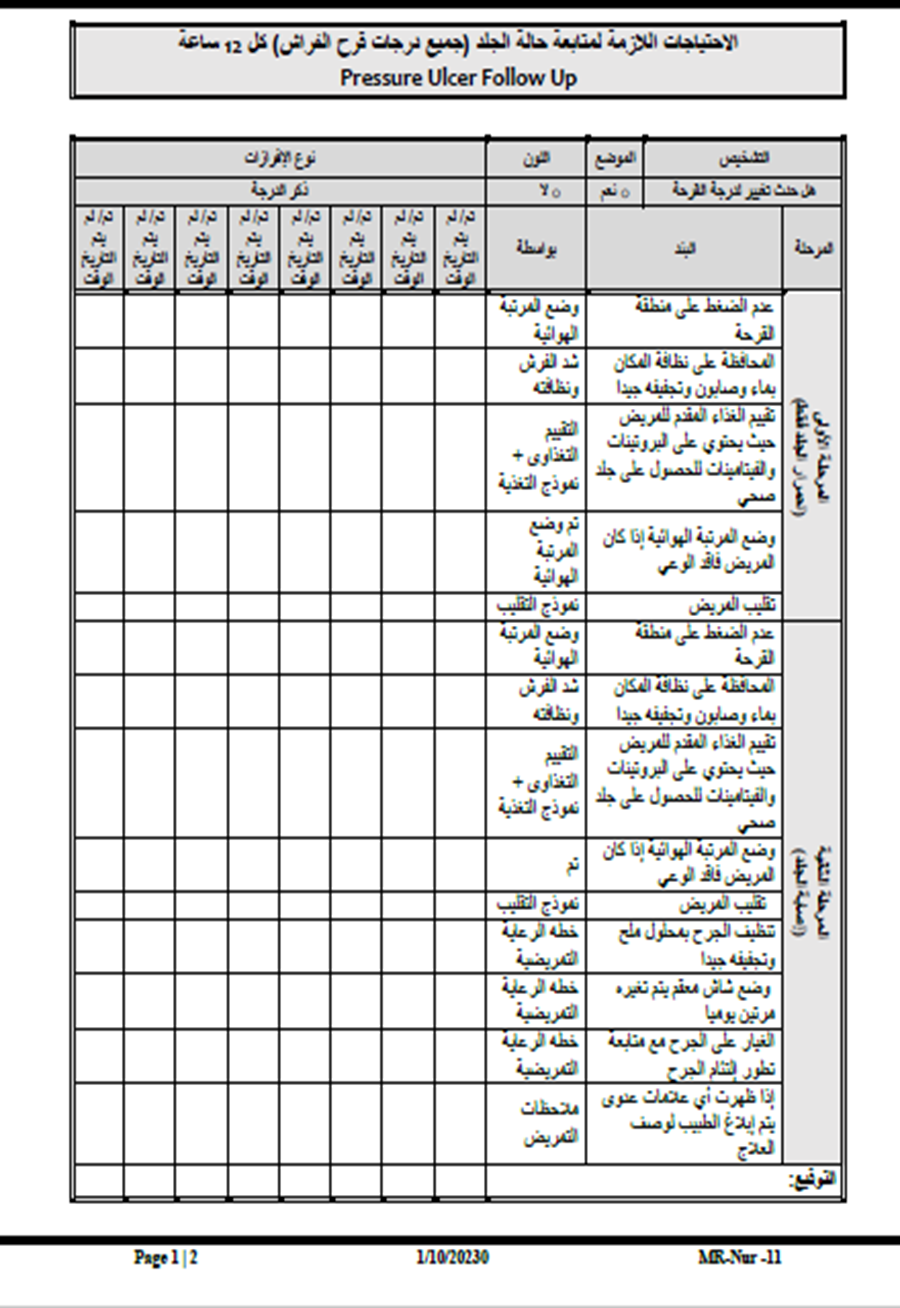
- Prevention of Pressure Ulcers in Neonates
Purpose:
- To establish a system for assessing the skin condition and safety of neonates upon hospital admission to determine their risk level for developing pressure ulcers.
- To identify neonates most at risk of pressure ulcers and take necessary preventive measures.
- To help heal existing pressure ulcers in affected neonates.
Definitions:
- Pressure Ulcer: A skin injury caused by impaired blood circulation and continuous friction against a bony area of the body, occurring when the skin is under prolonged pressure from a firm surface, such as a bed.
Procedures:
A. Risk Assessment at Admission, Including Skin Evaluation:
- The nurse conducts a pressure ulcer risk assessment and records it in the neonatal nursing assessment form.
- The nurse examines the skin over bony prominences such as the heels, ankle joints, pelvis bones, coccyx, ears, shoulders, and elbows.
- The nurse checks for areas of redness that persist for more than 30 minutes. For dark-skinned neonates, skin warmth in affected areas should be assessed.
- The nurse classifies the neonate's skin condition as:
- Low risk
- Moderate risk
- High risk
- Severe risk
B. Timeframe for Pressure Ulcer Screening Completion:
- The nurse must complete the screening within two hours of the neonate’s admission to the neonatal intensive care unit (NICU) and record the findings in the neonatal nursing assessment form.
C. Frequency of Pressure Ulcer Risk Reassessment:
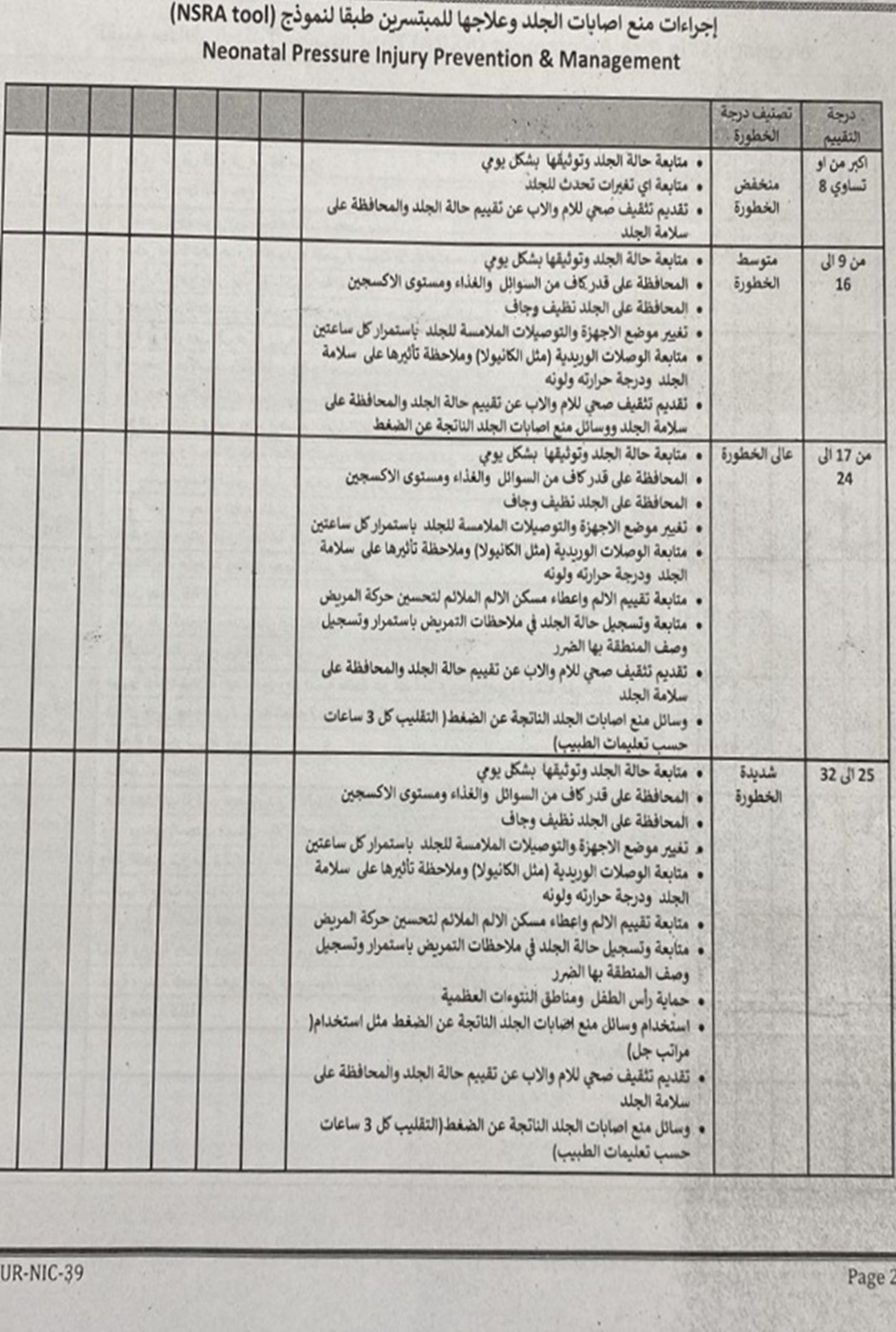
- If no pressure ulcers are present at admission, the nurse reassesses the neonate within 24 hours using the Neonatal Skin Risk Assessment (NSRA) Scale:
- Score ≥ 8: Low risk
- Score 9-16: Moderate risk
- Score 17-24: High risk
- Score 25-32: Severe risk
- The nurse performs a daily reassessment every 24 hours using the NSRA scale.
- If a pressure ulcer is present at admission, the nurse documents:
- The number, location, and severity of the ulcers
- The presence of any discharge
Stages of Pressure Ulcers:
- Stage 1: Red or pink area that does not disappear within 30 minutes, similar to a mild sunburn. Skin may feel painful or itchy.
- Stage 2: Red, swollen, and painful skin. Blisters may be present, and the upper skin layers begin to deteriorate.
- Stage 3: The ulcer extends deeper into the skin layers, forming a crater-like wound.
- Stage 4: The ulcer extends into the fat, muscle, or even bones.
D. Actions in Case of Existing Pressure Ulcers:
- The nurse informs the neonate's family about the ulcer's location, severity, and presence of discharge, obtaining written acknowledgment.
- The attending physician is notified to create a treatment plan, which may include consultation with a dermatologist or surgeon.
- For high-risk neonates, the nurse reassesses the skin every two hours to check for redness or dryness and records it in the patient repositioning log.
E. Preventive Measures:
- Regular Repositioning:
- The nurse repositions the neonate every two hours and documents it in the repositioning log.
- The neonate's head should be elevated at a 30-degree angle, except during feeding, per physician instructions.
- Skin Protection:
- Use prescribed emollients to reduce friction injuries.
- Avoid massaging over bony prominences.
- Keep the skin clean and dry.
F. Individualized Care Plans Based on Risk Assessment:
- Following the skin assessment, the nurse:
- Reports findings to the physician.
- Develops a care plan to minimize pressure on bony areas, reduce friction, and prevent moisture-related skin damage.
- Establishes a patient repositioning schedule (every two hours or as prescribed by the physician).
- Educates the family on pressure ulcer prevention, documenting it in the health education form and nursing care plan.
Responsibility:
- Attending physician
- Ward nurses
- Nutrition specialist
Attachments:
- Patient Repositioning Log
- Neonatal Skin Risk Assessment (NSRA) Form
- Pressure Ulcer Staging Guide
- Incident Reporting Form
Incident/Error/Unexpected Event Report Form
1. Injured Party Information:
- Name: ................................................
- File/Card Number: ..................
- Age: ...........
- Gender: ..................
- Department: ...............................................
- Admission Date (for patients): ............................
- Category:
- □ Patient
- □ Employee
- □ Visitor
- □ Other (Specify): ........................
2. Type of Incident:
- □ Error
- □ Accident
- □ Significant Unexpected Event
- (Specify) ..................................................
3. Incident Details:
- Date: ....../....../20......
- Time: .......... (AM / PM)
- Exact Location: ..................................................
4. Incident Description and Contributing Factors:
..................................................
5. Corrective Actions Taken:
..................................................
6. Reporter’s Information:
- Name: ..................................................
- Department: ...............................................
- Physician Notified: ...............................................
- Time Report Initiated: ........................
- Witness (if any): ..................................................
- Contact Number: ............................
7. Supervisor’s Information:
- Name: .........................................
- Position: ............................
- Date: ....../....../20......
- Time: .......... (AM / PM)
- Signature: ..........................
8. Medical Supervision (If Injury Occurred):
(Include patient examination, required tests, results, and
diagnosis)
..................................................
- Name: .........................................
- Date: ....../....../20......
- Signature: ..........................
9. Medical Follow-up Information:
..................................................
- Name: .........................................
- Date: ....../....../20......
- Signature: ..........................
10. Department Head’s Instructions (Verification of Report Details):
..................................................
- Name: .........................................
- Date: ....../....../20......
- Signature: ..........................
11. Hospital Director’s Instructions:
..................................................
The report is submitted to the Hospital Quality Improvement Committee Coordinator for recommendations, implementation, and filing.
- Hospital Director’s Signature: ..................................................
- Date: ....../....../20......
- Physical Examination of the Newborn
A comprehensive evaluation of the newborn's condition is conducted upon admission to the neonatal care unit. Additionally, an assessment is performed at the beginning of each shift, with findings documented in the newborn's medical record. The evaluation includes:
- General Examination
- Vital Signs Measurement (respiration, pulse, temperature, blood pressure) every 3 hours or as per physician’s instructions
- Growth Measurements Monitoring
- Comprehensive Assessment of Various Body Systems
First: General Examination
This includes observing the following:
1. Body Position
- The newborn is observed while lying on their back, with the head slightly flexed forward (chin touching the upper chest) and full flexion of both arms and legs.
2. Skin Condition
- Assessment of skin color (any discoloration—pale or dark), elasticity, presence of scratches, wounds, or birthmarks.
3. Head and Face
- Fontanelles:
- The anterior fontanelle should be open in a diamond (◊) shape.
- The posterior fontanelle is usually closed at birth, but if open, it appears triangular (Δ).
- Birth Trauma Signs:
- Caput succedaneum: Swelling of the scalp due to fluid accumulation, which resolves within a few days without complications.
- Cephalhematoma: Blood accumulation under the scalp, which disappears within weeks.
- Eyes: Checked for discharge, redness, or swelling.
- Nose: Examined for discharge, nasal septum deviation, or blockage during suction catheter insertion.
- Ears: Checked for visible congenital anomalies.
- Mouth: Assessed for cyanosis, discharge, oral thrush, or congenital defects such as cleft lip or palate.
4. Chest (Breast Tissue)
- Temporary breast swelling in newborns is normal due to maternal hormones transferred through the placenta. Breast tissue should not be squeezed to avoid infection.
5. Umbilical Cord
- Checked for signs of infection, including redness, discharge, foul odor, or bleeding.
6. Other Observations
- Any visible congenital abnormalities should be documented during the initial newborn assessment.
Second: Vital Signs Measurement
Vital signs are measured every 3 hours if the newborn is stable. If unstable, they are checked hourly. The vital signs include:
1. Respiratory Rate
- Measured before touching the newborn.
- The normal range for neonates is 40–60 breaths per minute.
2. Body Temperature
- The normal range is 36.5 – 37.5°C.
- Axillary temperature (underarm) is measured using a thermometer held vertically for:
- 5–7 minutes in full-term newborns.
- 7–10 minutes in preterm or low-birth-weight newborns.
- Note: Some neonatal units measure rectal temperature initially to rule out anal atresia, but using a soft catheter for this is safer. The newborn’s bowel movements are also monitored and recorded for the first 48 hours after birth.
3. Heart Rate
- The normal range is 120–160 beats per minute.
- Counted for a full minute using a stethoscope.
4. Blood Pressure
- Measured at admission from all four limbs using a Dynamap device.
- Routine measurements are then taken from the arm without an intravenous cannula.
- Blood pressure varies with crying (increases) and sleep (decreases) and depends on gestational age and postnatal age.
- Normal systolic: 67–84 mmHg, diastolic: 35–53 mmHg.
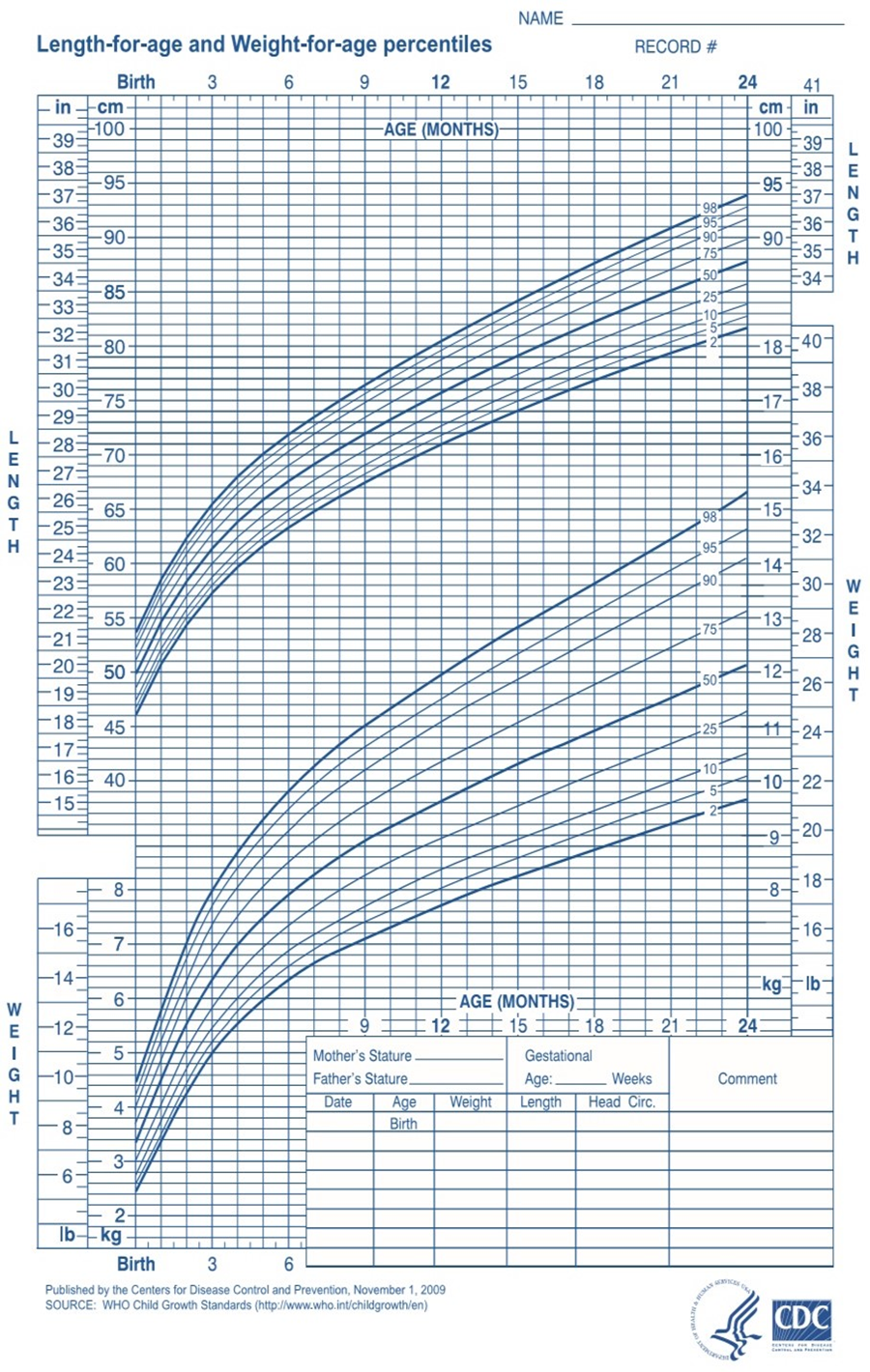
Third: Growth Measurements
1. Weight
- Normal newborn weight: 2700–3850 g.
- Measured once daily (twice daily if birth weight is <1000 g).
- Weight is recorded and tracked using a growth chart, especially for underweight newborns.
- Note: Newborns may lose about 10% of their weight within the first 3–4 days due to fluid loss, urination, and passage of meconium. They regain their birth weight within 10 days.
2. Length
- Normal newborn length: 46–56 cm.
- Measured at admission and then weekly.
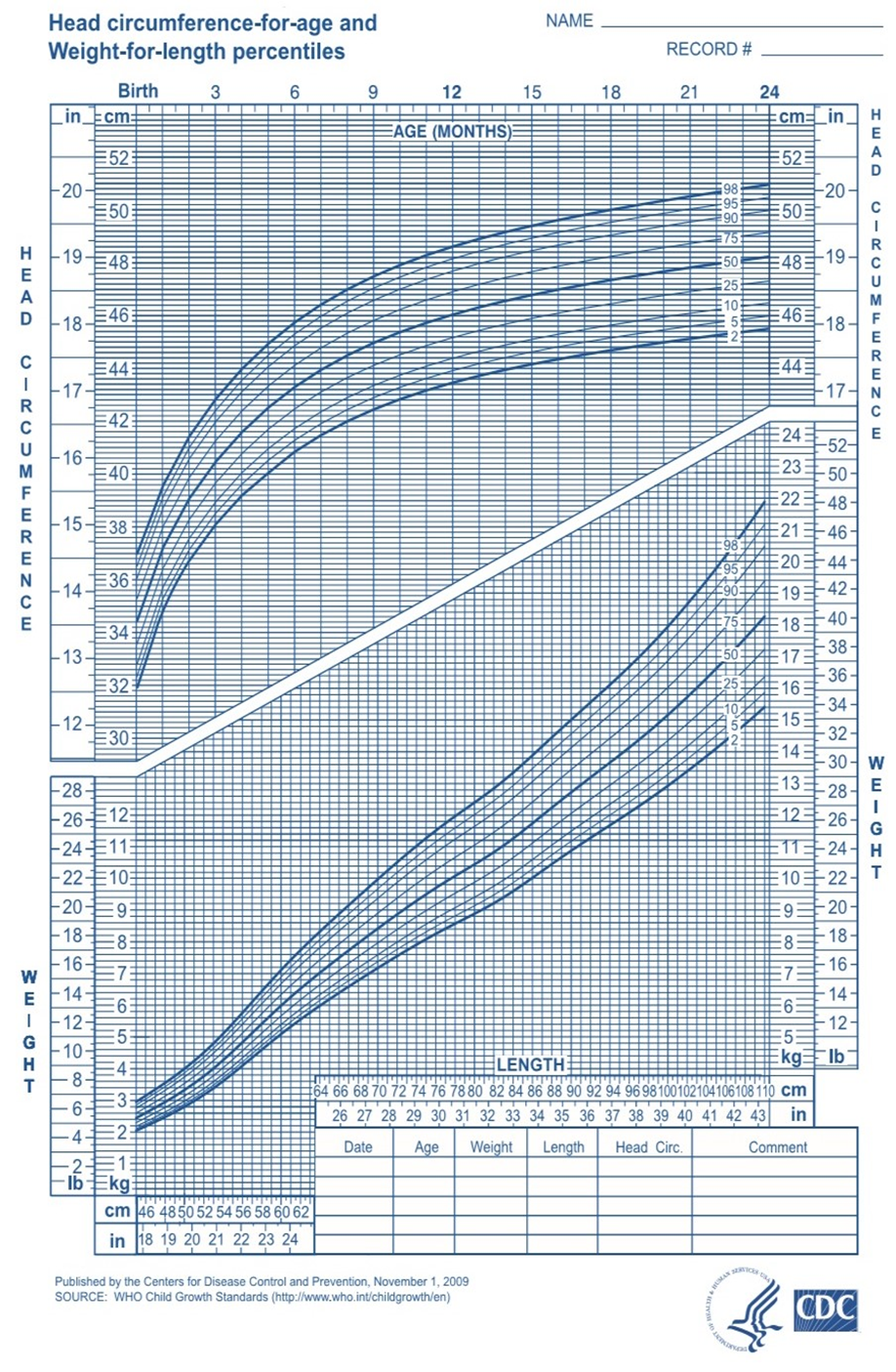
3. Head Circumference
- Normal range: 33–37 cm.
- Measured at admission and weekly.
- Daily measurements are required for newborns with neurological issues (e.g., intraventricular hemorrhage, hydrocephalus, birth asphyxia, or spinal cord infections).
4. Abdominal Circumference
- Normal range: 31–33 cm.
5. Chest Circumference
- Normal range: 30–35 cm.
Fourth: Comprehensive Assessment of Body Systems
1. Nervous and Motor System
The nervous system in newborns is characterized by reflex responses, the most notable being the Moro reflex. The neurological examination includes:
- Movement and Alertness: Whether the newborn is sleeping, awake, tense, stiff, or floppy.
- Body Position: Whether the newborn maintains a flexed posture or has muscle laxity.
- Crying: Whether the cry is strong or weak.
- Fontanelle Condition: Whether it is open or closed, bulging or sunken.
- Seizures: Any presence of convulsions, which should be described if observed.
- Muscle Tone: Whether it is rigid, normal, or weak.
- Weakness or Stiffness in Limbs: Such as Erb’s palsy (brachial plexus injury), clavicle fracture, or muscle stiffness.
- Spinal Abnormalities: Any visible congenital defects of the spine.
2. Cardiovascular System
The cardiovascular assessment includes:
- Heart Rate and Rhythm: Ensuring a regular heartbeat.
- Capillary Refill Time: Pressing on the sternum and counting the seconds until the color returns to normal (normal is <3 seconds).
3. Respiratory System
Respiratory evaluation involves:
- Skin Color: Observing if it is pink, blue (cyanotic), or pale.
- Respiratory Rate: Checking if it is within the normal range.
- Symmetry of Chest Movements: Ensuring both sides of the chest move equally with breathing.
- Chest and Abdominal Coordination: Evaluating synchronized movements.
- Signs of Respiratory Distress:
- Increased respiratory rate (>60 breaths per minute)
- Grunting sounds
- Chest retractions
- Episodes of apnea (pauses in breathing)
- Presence of secretions
- Chest Circumference Measurement.
4. Digestive System
The digestive system examination includes:
- Abdominal Shape: Checking for distension or abnormalities.
- Abdominal Circumference Measurement: At the level of the umbilicus.
- Presence of Vomiting: Recording the content and color, if present.
- Passage of Meconium: Ensuring that the first stool (meconium) is passed within 24–48 hours after birth.
5. Genitourinary System
For Female Newborns:
- Mild swelling of the external genitalia (normal).
- Ensuring the labia majora covers the labia minora.
- Possible vaginal discharge or slight bleeding due to maternal hormone transfer.
For Male Newborns:
- Checking that the urinary meatus is at the tip of the penis.
- Ensuring both testes have descended into the scrotum.
- Observing the scrotum for swelling, fullness, dark coloration, and prominent folds.
- Ensuring urination occurs within 24 hours of birth and assessing the color (light yellow) and quantity (1–3 mL/kg/hr).