First Nursing Guideline for Burn Patient Care
| Site: | EHC | Egyptian Health Council |
| Course: | Evidence of nursing procedures for the burn department |
| Book: | First Nursing Guideline for Burn Patient Care |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:35 AM |
Description
"last update: 27 April 2025" تحميل الدليل
- Prepared by
Burn guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the
Egyptian Nursing Syndicate - Member of the Senate
Prepared by
Title
Name
NO.
Dean Of Faculty Nursing, Professor of Medical and
Surgical Nursing, Tanta University
Dr Afaf Abdel Aziz Abdel Aziz Basal
1
Professor Of Critical Care Nursing
Prof.Dr/Zeinab Hussain Ali
2
Professor And Head of the Department of Medical
Surgical Nursing. Faculty-. Benha University
Amal Said Taha Refaie
3
Supervisor Of the Education Sector at Port Said
University
Amal Ahmed Khalil Morsy
4
Professor Of Medical Surgical Nursing- Faculty of
Nursing- Cairo University
Dr. Hanan Ahmed Al Sebaee
5
Head of central administration on secondment at MOHP
Dr Neveen ab drab al0nabi Mohamed
6
Director Of Primary Health Care Nursing Department at
MOHP.
Maysa Hosny Ahmed Tammam
7
Supervisor Of Technical Education- EHA
Nancy Alaa Eldeen Abd-Elbaset Ali
8
Supervisor Of Nursing Services Development- EHA
Sherien Mohamed Saad
9
Assistant Professor of Maternity and Neonatal Health
Nursing - Faculty of Nursing- Ain Shams University
Assist.Perof. Dr./Heba Mahmoud Mohammed
10
General manager of general administration of health
institutes affairs
Dr Mai Galal Ibrahim Al-Assal
11
Participants
nursing specialist at the
General Administration of Nursing - Ministry of Health
Ms. Mona Ali Abdul Rahman
Al-Katami
12
nursing specialist at the
General Administration of Nursing - Ministry of Health
Ms. Samar Magdy Al-Hassanin
13
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
nursing specialist at the General Administration of Nursing - Ministry of Health |
Ms. Mona Ali Abdul Rahman Al-Katami |
12 |
|
nursing specialist at the General Administration of Nursing - Ministry of Health |
Ms. Samar Magdy Al-Hassanin
|
13 |
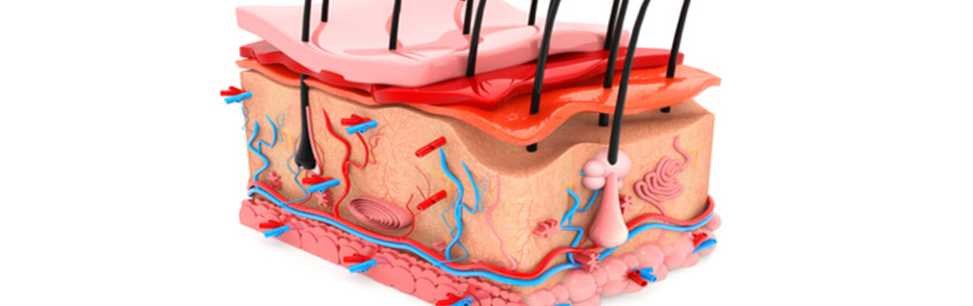
- Skin Anatomy and Functions
The skin is the largest organ in the human body, covering the outer surface of the body. There are few areas where its covering differs, such as the eyes and lips. The skin functions as a protective layer around the body, safeguarding the delicate tissues underneath from damage. Naturally, the skin is always exposed to wear and tear, unlike other parts of the body that are protected. The skin is highly flexible and bends easily to adapt to the movements of various body parts. After bending with the movement of a joint, it returns easily to its original position when the joint returns to its natural state.
The surface of the skin contains many tiny openings, known as pores. These pores are the ends of sweat gland ducts from deeper skin layers. Sweat produced in the glands exits through the pores to the surface, although we usually don’t feel it as it evaporates as soon as it appears. However, when we engage in physical activity or when the weather is hot, large droplets of sweat form, wetting the skin. The evaporation of this moisture reduces the skin temperature, and consequently, the body's overall temperature remains within the normal range.
Skin Layers:
The skin is composed of three main layers, each differing in anatomy and function as follows:
- Epidermis: The epidermis is the thin outer layer of the skin that acts as a water barrier and is responsible for skin color. It is made up of three types of cells:
- Melanocytes: Cells that produce melanin, responsible for skin pigmentation, found in the basal cell layer.
- Langerhans cells: The skin's first line of defense, located in the spinous layer.
- Merkel cells and sensory nerves: Found in the basal layer, serving as mechanoreceptors for light touch.
The epidermis itself consists of five sub-layers working together to rebuild the skin surface:
- Basal Layer (Stratum Germinativum): The deepest layer containing small round cells called basal cells, which divide continuously, pushing older cells toward the surface.
- Squamous Cell Layer (Stratum Spinosum): Above the basal layer, this thicker layer is also known as the spinous layer. It contains basal cells that have been pushed upwards, now called squamous cells, which produce keratin, a strong protein forming the structure of the skin, hair, and nails.
- Granular Layer (Stratum Granulosum): Contains diamond-shaped cells with granules. Keratinocytes from the squamous layer are pushed into this layer, where they grow, flatten, and adhere to one another.
- Clear Layer (Stratum Lucidum): A thin transparent layer found in thick skin, such as on the palms and soles.
- Horny Layer (Stratum Corneum): The outermost layer, constantly shedding, with a full cell turnover occurring every 28 to 30 days in young people, and 45 to 50 days in the elderly.
- Dermis: The dermis lies beneath the epidermis and is thicker, consisting of two layers of connective tissue: the papillary dermis and the reticular dermis. The dermis contains:
- Blood vessels that supply the skin with nutrients and oxygen while removing waste.
- Lymphatic vessels that destroy infections or invasions by pathogens.
- Hair follicles that surround and nourish the hair.
- Sweat glands that produce sweat and regulate body temperature.
- Nerve endings containing pain and touch receptors that send sensations to the brain.
- Collagen, a strong protein that helps anchor muscles and organs in place, enhancing skin strength.
- Elastin, a substance allowing the skin to return to its shape after stretching, maintaining skin flexibility.
- Hypodermis: The hypodermis, the deepest layer, consists of a network of fat cells and collagen. It serves as insulation to retain body heat, cushions internal organs, and stores fat as an energy reserve.
Functions of the Skin Layers:
The skin acts as a protective barrier against heat, light, injury, and infection. Other functions include:
- Storing water and fat.
- Regulating body temperature.
- Preventing water loss.
- Blocking bacterial entry.
- Producing vitamin D upon sunlight exposure.
- Serving as a barrier between the organism and the environment.
- Sensory perception.
The thickness of the skin varies across the body, categorized based on the thickness of the epidermis and dermis. The thickness of the hypodermis also differs across the body and from person to person. Hairless skin on the palms and soles is the thickest due to an additional layer, the stratum lucidum. The upper back is thicker based on dermal thickness, but is considered thin in tissue terms as it lacks the stratum lucidum, making the epidermis thinner than non-hairy skin.
- Burns
Definition of Burns:
Burns refer to the destruction and damage to the skin and body tissues caused by exposure to an external factor with high heat, such as hot water, direct flames, a corrosive chemical substance, or radiation. This results in several types of damage: psychological, physical, and sensory.
Causes of Burns:
- Heat: There are two types: a. Dry heat: Fire flames. b. Moist heat: Hot water or steam.
- Radiation: (Natural radiation such as sunlight, artificial radiation such as cancer treatment radiation).
- Electricity.
- Strong chemicals (severe acidic or alkaline substances).
Types of Burns:
Burns that only affect the outer layer of the skin are called superficial burns or first-degree burns. When the damage reaches some of the layers beneath the skin, it is known as partial-thickness burns or second-degree burns. In third-degree burns, all layers of the skin are affected. Fourth-degree burns involve deeper tissues such as muscles or bones.
1) First-Degree Burns (Superficial Burns): These affect only the outer layer of the skin and are the least dangerous of the other burn types. Only the outer skin layer is burned, and healing occurs within 5-10 days without any significant physiological changes to the skin.
Symptoms:
- Redness of the skin at the burn site.
- Redness is usually accompanied by swelling.
- Presence of pain.
Causes of First-Degree Burns:
- Excessive sun exposure.
- Mild contact with a hot object or spilling hot water.
- Exposure of the skin to steam or small amounts of chemicals.

First-Aid measures for Minor Burns:
• Quickly remove the victim from the source of heat.
• Remove any jewelry or accessories.
• Immerse the burned area in cold water for 10 minutes or until the pain subsides.
• Generally, hospitalization is not needed, but if the burns are on large areas such as the hands, feet, face, thighs, buttocks, or major joints, medical attention should be sought immediately.
Patient Education on Home Care for First-Degree Burns: First-degree burns are treated at home as minor burns as follows:
- Cool the burned area by placing it under cold water, not ice-cold, like tap water, or submerge the burn area in a container with cold water, or apply cold compresses for 10-15 minutes or until the pain subsides.
- Cover the burn with a sterile gauze dressing, ensuring not to apply pressure on the burned area.
- Administer a pain reliever.
Notes: Cooling the burn site prevents swelling by halting the further spread of heat to the skin.
- Use cold water to cool the burn, not ice, as ice can worsen the burn and cause more damage to the skin.
- Cover the burn with sterile gauze and avoid using cotton or any fabric that could stick to the burn.
- Do not apply egg whites, butter, or toothpaste to the burn.
- Monitor the burn, as it often heals on its own. However, if any signs of infection such as increased pain, redness, swelling, or fever are noticed, seek medical advice.
2) Second-Degree Burns: These affect both the outer and inner layers of the skin, characterized by blisters, swelling, and the leakage of plasma beneath the skin. Healing occurs within 2-3 weeks.
Symptoms: Blisters, noticeable swelling, severe pain, and leakage of plasma through damaged skin layers.
First-Aid for Second-Degree Burns: • Move the victim away from the heat source. • Remove any clothing over the burn area. • Immerse the burned area in cold water to reduce pain (cooling the tissue this way reduces the heat from adjacent tissues). • Do not use ice or frozen water, as this can damage the tissue. • Dry the area and cover with sterile dressings or a cold cloth.
• Cover the burn with sterile gauze and a dry bandage, avoiding the removal of burned tissue or attempting to pop the blisters. • Change the dressing every 1-2 days or if the dressing becomes soaked with plasma. • Watch for signs of infection, such as fever, unexplained pain, or pus. • Second-degree burns on the face, neck, or larger than 3 cm require medical intervention.
3) Third-Degree Burns: These burns affect all layers of the skin and can also involve deeper tissues like muscles and bones. The victim may lose sensation in the burned area due to nerve damage, and the skin may char.
Symptoms: The burn area may appear waxy white or blackened. No pain is felt after the burn due to nerve damage.
• Do not remove clothing from the burned area as it may tear the skin. • Do not apply cold water or medication to the burn. • Place a clean, moist gauze over the area. • Rush the victim to the hospital. • If the burn is on a hand or foot, elevate it above heart level to reduce blood flow. • If the burn is on the face, monitor for breathing difficulties.
4) Fourth-Degree Burns: Fourth-degree burns involve damage to deeper tissues, including muscles and bones, and are caused by fires, explosions, or high-voltage electrical burns. These burns may require amputation of limbs or major reconstructive surgery for other body parts.
Causes of Burns:
Burns are skin injuries caused by exposure to heat, electricity, chemicals, or radiation, leading to severe pain and potentially life-threatening conditions that hinder functionality.
Main Causes of Burns:
- Exposure to heat: This can be from flames, hot materials, or heated surfaces.
- Electric current.
- Exposure to chemicals.
- Friction.
- Sunlight exposure.
- Radiation.
Classification of Burns:
- Minor Burns: Affect less than 10% of the body surface area in children and 15% in adults, without additional risk factors.
- Severe Burns: One or more of the following criteria: • More than 10% of the body surface area affected in children and more than 15% in adults. • Inhalation injury (smoke, hot air, particles, toxic gases, etc.). • Significant trauma (fractures, head injuries, etc.). • Location: face, hands, neck, genitals, or major joints (risk of functional disability). • Electrical, chemical, or explosion-related burns. • Age <3 years or >60 years or severe underlying conditions (e.g., epilepsy, malnutrition).
Diagnosis of Burns:
Burns are diagnosed by a specialist through:
- A clinical examination by the doctor.
- Blood tests to check for inflammation, electrolyte levels, and liver/kidney function to ensure no fluid loss in the bloodstream.
- An X-ray to assess the extent of the burn.
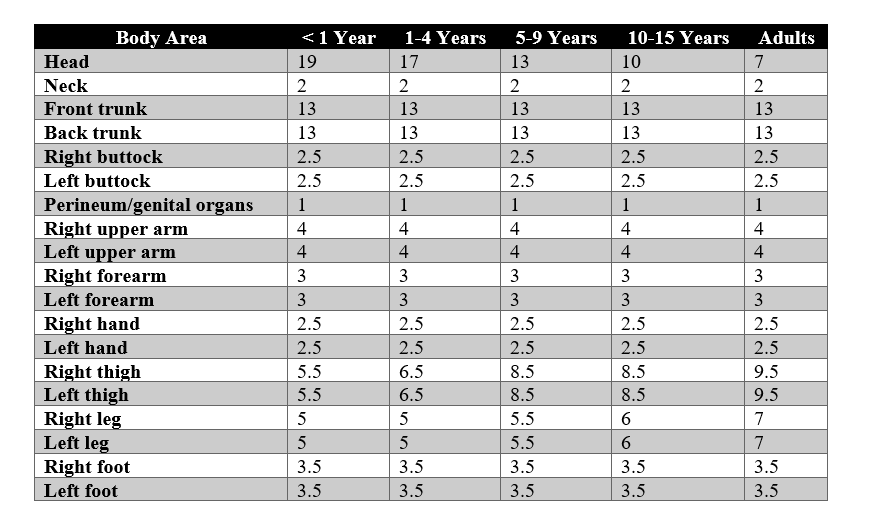
Burn Assessment
Extent of Burns
The Lund and Browder chart shows the percentage of body surface area based on
age. This chart helps in accurately calculating the percentage of the body
surface area affected based on the patient’s age.
For example, a burn on the face, front torso, inner forearm, and the peripheral
burn of the left upper arm in a 2-year-old child:
8.5 + 13 + 1.5 + 4 = 27% of the body surface area.
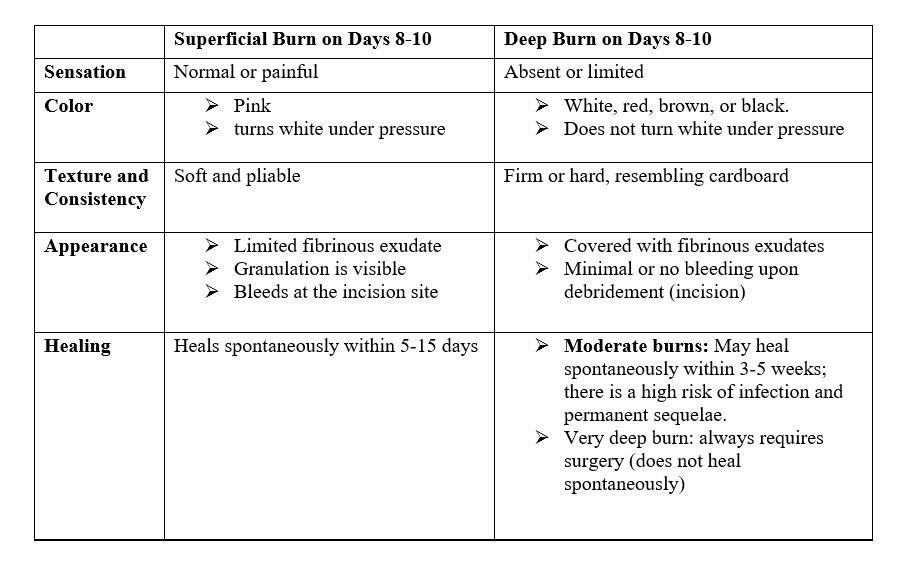
Depth of Burns
Except for first-degree burns (painful redness of the skin without blisters)
and very deep burns (third-degree burns, charring), the depth of burns cannot
be determined during the initial assessment. Differentiation is possible after
8-10 days.
Rule of Nines:
The body is divided into parts, and
each part is assigned a percentage of 9%, which helps in quickly estimating the
injury area at the site of the incident.
The body is divided as follows:
- Head = 9%
- Right arm = 9%
- Left arm = 9%
- Anterior torso = 18% (Chest = 9%, Abdomen = 9%)
- Posterior torso = 18% (Back = 9%, Buttocks = 9%)
- Anterior of each lower limb = 9%
- Posterior of each lower limb = 9%
- Genital area = 1%
Inhalation Injury Assessment :
- Dyspnea with retraction of the chest wall inward
- Bronchospasm
- Nasal or oral secretions
- Productive cough with black (sooty) sputum
- Hoarseness (raspy voice), etc.
- References
- Andersson T, ErtürkBergdahl G, Saleh K, Magnúsdóttir H, Stødkilde K, Andersen CBF, Lundqvist K, Jensen A, Brüggemann H, Lood R. Common skin bacteria protect their host from oxidative stress through secreted antioxidant RoxP. Sci Rep. 2019 Mar 05;9(1):3596.
- AskMayoExpert. Burn rehabilitation. Rochester, Minn.: Mayo Foundation for Medical Education and Research; 2018.
- Brown TM, Krishnamurthy K. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Nov 14, 2022. Histology, Dermis.
- Burns. Merck Manual Professional Version. https://www.merckmanuals.com/professional/injuries-poisoning/burns/burns.
- Kermott CA, et al., eds. Emergencies and urgent care. In: Mayo Clinic Guide to Self-Care. 7th ed. Rochester, Minn.: Mayo Foundation for Medical Education and Research; 2017.
- O'Connell RL, Rusby JE. Anatomy relevant to conservative mastectomy. Gland Surg. 2015 Dec;4(6):476-83.
- Stone CK, et al., eds. Burns and smoke inhalation. In: Current Diagnosis&Treatment: Emergency Medicine. 8th ed. New York, N.Y.: McGraw-Hill Education; 2017. https://accessmedicine.mhmedical.com.
- York, N.Y.: McGraw-Hill Education; 2015.