Nursing Guidelines for Burn Treatment
| Site: | EHC | Egyptian Health Council |
| Course: | Evidence of nursing procedures for the burn department |
| Book: | Nursing Guidelines for Burn Treatment |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:35 AM |
Description
"last update: 27 April 2025" تحميل الدليل
- Prepared by
Burn guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
nursing specialist at the General Administration of Nursing - Ministry of Health |
Ms. Mona Ali Abdul Rahman Al-Katami |
12 |
|
nursing specialist at the General Administration of Nursing - Ministry of Health |
Ms. Samar Magdy Al-Hassanin
|
13 |
- Treatment of Burn
First: Minor Burns
- Treatment is conducted on an outpatient basis.
- Topical treatment: Sulfadiazine dressings (for children aged 2 months and older and adults) or sterile fatty tulle (except for superficial first-degree burns).
- Pain management: Paracetamol ± Tramadol is usually effective.
Second: Severe Burns
- First Aid:
Upon hospital admission: - Ensure the airway is unobstructed and provide high-flow oxygen, even if blood oxygen saturation is normal.
- Establish an intravenous line through unburned skin if possible (use intraosseous access if intravenous access is unavailable).
- Administer Lactated Ringer's solution: 20 mL/kg in the first hour, even if the patient is stable.
- Administer subcutaneous morphine: 0.2 mg/kg (level 1 and 2 analgesics are ineffective).
- For chemical burns: Wash thoroughly with copious amounts of water for 15–30 minutes, avoiding contamination of intact skin. Do not attempt to neutralize the chemical agent.
Once the patient is stabilized:
- Remove clothing if it is not adhered to the burns.
- Take a burn history: mechanism, causative agent, time of occurrence, etc.
- Assess the burn: extent, depth, charred areas; check for burns to the eyes, functionally significant areas, circumferential burns of the limbs, chest, or neck. Wear a sterile face mask and gloves during the examination.
- Evaluate associated injuries (fractures, etc.).
- Protect the patient and keep them warm using a clean/sterile sheet or a thermal blanket.
- Insert a urinary catheter if burn surface area exceeds 15% of total body surface area (TBSA), in cases of electrical burns, or burns to the perineum/genital area.
- Insert a nasogastric tube if burn surface area exceeds 20% TBSA (done in the operating room during dressing procedures).
- Calculate fluid requirements for the first 24 hours and initiate administration.
- Closely monitor the following: level of consciousness, heart rate, blood pressure, oxygen saturation, respiratory rate (hourly); temperature and urine output (every 4 hours).
- Perform laboratory tests: hemoglobin, blood typing, and urinalysis.
- Prepare the patient for the first dressing procedure in the operating room.
Notes:
- Burns do not bleed initially. Investigate any bleeding if hemoglobin levels are normal or low.
- Burns do not alter consciousness on their own. Changes in consciousness suggest head injury, poisoning, or a preexisting condition like epilepsy.
- Clinical signs of electrical burns vary widely with the type of electrical current. Look for complications (e.g., arrhythmias, neurological disorders).
- General Measures During the First 48 Hours Resuscitation Measures:
Administer intravenous fluids to correct hypovolemia:
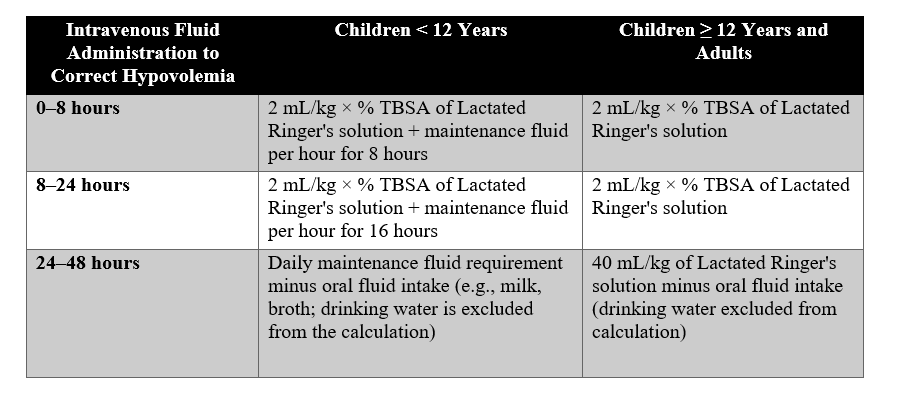
Fluid Requirements During the First 48 Hours by Age
- (A) Maintenance fluid: Alternate between Lactated Ringer's and 5% Dextrose solutions:
- 4 mL/kg/hour for the first 10 kg of body weight.
- +2 mL/kg/hour for the next 10 kg of body weight.
- +1 mL/kg/hour for each additional kg (above 20 kg, up to 30 kg).
Note: Increase fluid volume by 50% (3 mL/kg × % TBSA for the first 8 hours) in cases of inhalation injury or electrical burns. For burns > 50% TBSA, limit calculations to 50% TBSA. Adjust fluid administration based on systolic blood pressure and urine output to avoid fluid overload.
Vascular Resuscitation Targets:
|
Type of Burn |
Systolic BP |
Urine Output |
|
Non-electrical burns |
≥ 60 mmHg (children < 1 year) |
1–2 mL/kg/hour |
|
70–90 mmHg + (2 × age) (children 1–12 years) |
0.5–1 mL/kg/hour (adults) |
|
|
Electrical burns |
Age-appropriate systolic BP |
1–2 mL/kg/hour |
For patients with oliguria despite adequate fluids:
- IV dopamine: 5–15 mcg/kg/min via an infusion pump.
- Or IV epinephrine: 0.1–0.5 mcg/kg/min via an infusion pump.
Discontinue IV fluids after 48 hours if oral fluid intake can meet hydration needs.
Types of Fluids Used in the Burn Unit:
- Crystalloids:
- Lactated Ringer's Solution: The first choice for fluid resuscitation.
- Normal Saline: Used in specific cases, but monitor for metabolic acidosis.
- Colloids:
- Albumin or plasma expanders: Used later to replenish proteins and osmotic pressure.
- Respiratory Care – Pain Relief – Nutrition
▶️ Respiratory Care
- In all cases: continuous inhalation of humidified oxygen and chest physiotherapy.
- Emergency surgical intervention if necessary: pneumothorax or the presence of fluid or blood collection in the chest.
- Corticosteroids should not be given (do not affect edema; susceptibility to infection). There is no specific treatment for direct bronchopulmonary lesions.
▶️ Pain Relief
- Pain management by administering over-the-counter pain relievers such as ibuprofen (Advil, Motrin), acetaminophen (Tylenol), naproxen (Aleve). Aspirin should not be given to children under the age of 16.
▶️ Nutrition
- Early initiation of nutrition is recommended.
- Nutritional status should be assessed regularly (measure weight twice a week).
- Daily requirements for adults:
- Calories: 25 kcal/kg + 40 kcal/% of the body surface area affected.
- Proteins: 1.5-2 g/kg.
- Provide energy-dense foods.
- Nutritional needs are applied with the following distribution: carbohydrates 50%, fats 30%, proteins 20%.
- Provide 5-10 times the recommended daily intake of vitamins and trace elements.
- Enteral nutrition is preferred: oral or nasogastric tube (necessary if burn area > 20% of body surface area).
- Begin with small amounts on the first day, then gradually increase to meet the recommended energy needs within 3 days.
- Reduce energy loss: occlusive dressing (elastic), warm environment (28-33°C), early skin grafting; management of pain, insomnia, and depression.
- Infection Control
- Infection control measures are of utmost importance until complete healing. Infection is one of the most common and serious complications of burns:
- Standard infection control precautions (e.g., wearing sterile gloves when handling patients).
- Strict wound management (changing dressings, early debridement).
- Isolate “new” patients (<7 days from burn) from those in the recovery phase (≥7 days from burn).
- Antibiotics should not be administered unless there is systemic infection.
Infection is defined by at least two of the following four signs:
- Temperature > 38.5°C or < 36°C
- Tachycardia
- Tachypnea
- Increase in white blood cell count by more than 100% (or significant decrease in white blood cell count).
For systemic infections, initiate empirical antibiotic treatment:
- Intravenous Cefazolin:
- Children >1 month: 25 mg/kg every 8 hours
- Adults: 2 g every 8 hours
- Oral Ciprofloxacin:
- Children >1 month: 15 mg/kg twice a day
- Adults: 500 mg three times a day
- For local infections, in the absence of systemic infection signs, treat with topical silver sulfadiazine. Do not apply in children under 2 months of age.
Other Treatments
- Intravenous Omeprazole starting on day 1:
- Children: 1 mg/kg once daily
- Adults: 40 mg once daily
- Tetanus vaccination
- Prevention of thrombosis: low-molecular-weight heparin subcutaneously after 48-72 hours of injury.
- Physical therapy from day 1 (prevention of contractures) and pain relief are essential.
- Intentional burns (suicide attempt, assault): appropriate psychological follow-up.
- Local Treatment- Basic Principles
- Regular dressing changes to prevent infection, reduce heat and fluid loss, limit energy loss, and improve patient comfort. Dressings should be occlusive (elastic), help relieve pain, allow movement, and prevent contractures.
Basic Principles
- Strict adherence to sterilization principles.
- Dressing changes require morphine administration for the patient who is not sedated.
- The first dressing change is performed in the operating room under general anesthesia; subsequent dressing changes can be done in the operating room under general anesthesia or at the bedside with morphine administration.
Method
- For the first dressing, shave any areas with hair (armpit, groin, pubic area) if the burns involved adjacent tissues; scalp (front for facial burns, or entirely for scalp burns). Trim nails.
- Clean the burn using povidone-iodine foam solution (1 part 7.5% povidone-iodine + 4 parts 0.9% saline or sterile water). Gently scrub using a gauze pad, being careful not to cause bleeding.
- Rinse with 0.9% saline solution or sterile water.
- Dry the skin by patting with sterile gauze.
- Apply silver sulfadiazine directly with clean hands (wear sterile gloves) in a uniform layer of 3-5 mm thickness over all burn areas (except eyelids and lips) for children over 2 months old and adults.
- Apply a greasy dressing (or sterile gauze) in a back-and-forth motion (do not use a circular motion).
- Cover with sterile gauze, in a single layer without folding any ends.
- Apply a compressive bandage, leaving it loose without tightening.
- Elevate limbs to prevent edema; stabilize in an extended position.
Frequency
- Routine: every 48 hours.
- Daily in case of additional infection or in certain areas (e.g., perineum).
Monitoring
- Dehydration (ischemia) of the burned limb is the main complication in the first 48 hours. Evaluate signs of dehydration (ischemia): cyanosis or pallor of the limb, decreased sensation, hyperalgesia, poor capillary refill.
- Daily monitoring: pain, bleeding, wound healing, and infection development.
- Medications Used in the Burn Unit
- Antimicrobials:
- Topical Ointments: Such as silver sulfadiazine to prevent bacterial infections.
- Intravenous Antibiotics: Used in cases of systemic infections.
- Pain Relievers:
- Morphine and Fentanyl: Strong pain relievers for managing severe pain.
- Paracetamol or Ibuprofen: For moderate pain.
- Anti-inflammatory Drugs:
- Steroids may be used cautiously to reduce inflammation caused by burns.
- Immunotherapy:
- Immunoglobulins: To enhance the body's response in severe burn cases.
- Anticoagulants: To prevent blood clotting in cases of large burns.
- Intravenous Nutrition:
- IV nutrition provides the body with the energy needed for recovery.
- Electrolyte levels (potassium, sodium, magnesium) should be monitored and replaced as needed.
- Management of Special Cases:
- Chemical Burns: Managed using special washing solutions.
- Electrical Burns: Special attention to heart monitoring, fluid stability, and appropriate treatment.
- Infection Prevention and Wound Care:
- Emphasis on sterilization and care for exposed wounds.
- Use of infection-resistant dressings, keeping the wound environment moist.
- Pain Management and Psychological Rehabilitation:
- The importance of psychological support alongside medication therapy.
- Long-term rehabilitation strategies to reduce pain and improve mobility.
- التعامل مع الحالات الخاصة
- الحروق الكيميائية: التعامل بإستخدام محاليل غسل خاصة.
- الحروق الكهربائية: مراقبة القلب وإستقرار السوائل بشكل خاص وإعطاء العلاج المناسب للحالة.
7. الوقاية من العدوى والعناية بالجرح
- إعطاء أهمية قصوى للتعقيم والعناية بالجروح المكشوفة.
- إستخدام الضمادات المانعة للعدوى، والمحافظة على بيئة الجرح رطبة.
- ادارة الألم والتأهيل النفسي
- يراعى أهمية الدعم النفسي بجانب العلاج الدوائي.
- يتم تنفيذ إستراتيجيات التأهيل طويلة الأمد لتقليل الألم وتحسين الحركة.
- References
- AskMayoExpert. Burn rehabilitation. Rochester, Minn.: Mayo Foundation for Medical Education and Research; 2018.
- Burns. American College of Emergency Physicians. http://www.emergencycareforyou.org/emergency-101/burns/#sm.00001vmpo9txgzeszpr9msb2lf8tm.
- Burns. Centers for Disease Control and Prevention. https://www.cdc.gov/masstrauma/factsheets/public/burns.pdf.
- Burns. Merck Manual Professional Version. https://www.merckmanuals.com/professional/injuries-poisoning/burns/burns.
- Cooking safety for older adults. American Burn Center. http://ameriburn.org/prevention/prevention-resources/#1493037731300-e4bd5ba9-3769.
- Kermott CA, et al., eds. Emergencies and urgent care. In: Mayo Clinic Guide to Self-Care. 7th ed. Rochester, Minn.: Mayo Foundation for Medical Education and Research; 2017.
- Murphy F, et al. Treatment for burn blisters: Debride or leave intact? Emergency Nurse. 2014;22:24.
- Stone CK, et al., eds. Burns and smoke inhalation. In: Current Diagnosis & Treatment: Emergency Medicine. 8th ed. New York, N.Y.: McGraw-Hill Education; 2017. https://accessmedicine.mhmedical.com.
- Wiktor A, et al. Treatment of minor thermal burns. https://www.uptodate.com/contents/search.
- York, N.Y.: McGraw-Hill Education; 2015.