The Procedural Approach For Respiratory Diseases
| Site: | EHC | Egyptian Health Council |
| Course: | Evidence of nursing procedures for internal sections |
| Book: | The Procedural Approach For Respiratory Diseases |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:34 AM |
Description
"last update: 8 April 2025" تحميل الدليل
- Prepared by
Inpatient guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Head of nursing administration at EHA, Ismailia branch |
Ms. Nahla Kamel Mostafa |
12 |
|
member of the Nursing administration at EHA, Ismailia branch |
Ms. Maha Mohamed Saad |
13 |
|
member of the Nursing administration at EHA, Ismailia branch |
Mr. Tharwat Abdel-Al Mohamed |
14 |
|
nursing specialist at the General Administration of Nursing - MOHP |
Mr. Mona Ali Abdul Rahman Al-Katami |
15 |
|
nursing specialist at the General Administration of Nursing - MOHP |
Ms. Sherine Abdel Hakim Abdel Hakim Khattab |
16 |
|
nursing specialist at the General Administration of Nursing - MOHP |
Mr. bahaa fuoad barsom |
17 |
- Oath of the Profession
"I swear by Almighty God,
that I will be faithful in my work, fear God in my profession, respect its laws
and regulations, and perform my duties with competence and dedication.
I will rely on knowledge derived from nursing sciences in my work,
and I will do my utmost to care for those entrusted to me, preserving their
dignity, keeping their secrets, defending their rights, and protecting them
from any harm.
I will not fear speaking the truth and will provide a safe environment for the
patient, their family, and the community.
I will continue to develop myself, honor those who taught me, and respect them.
I will collaborate with my colleagues in the profession on the path of
righteousness and piety.
And God is a witness to what I say."
- Vision and Mission of Nursing Care
Vision of Nursing Care in the Inpatient Care Unit:
The nursing staff in the inpatient care unit aims to elevate the nursing profession and provide effective, safe, and high-quality nursing care to patients in the unit, in accordance with Egyptian, national, and international standards.
Mission of Nursing Care in the Inpatient Care Unit:
The nursing staff in the inpatient care unit is committed to improving the health level of patients and providing them with the best possible nursing care in line with the hospital's goals and procedures. They also strive to elevate the scientific and practical level of all nursing staff in the unit and to direct them toward modern trends in nursing and medical sciences.
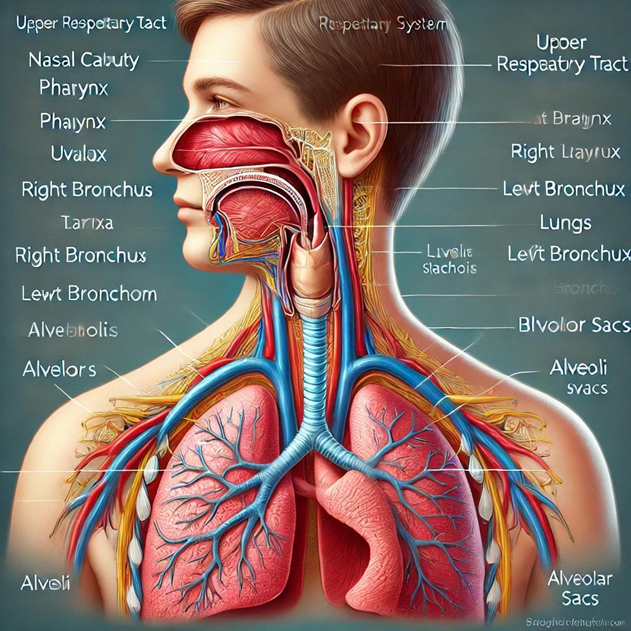
- Introduction to the Respiratory System
Anatomy of the Respiratory System:
The respiratory system is one of the most important systems in the human body, responsible for transferring oxygen from the air (ambient air) to the blood, from where it is distributed to the rest of the body. Air flows from the environment into the respiratory system, and this process occurs due to the lower pressure inside the chest compared to the atmospheric pressure, leading to inhalation. Exhalation happens when the pressure inside the chest increases, causing air to be expelled from the lungs into the environment. During this process, gas exchange occurs, transferring oxygen from the air to the alveoli, from there into the blood, and then distributed to all body cells.
Importance of the Respiratory System:
The importance of the respiratory system lies in its provision of the necessary amount of oxygen required for cellular respiration. If there is any dysfunction or disruption in the respiratory system, it leads to insufficient oxygen supply to the cells, a condition known as hypoxia. This condition impacts all body cells, especially brain cells, leading to their death if untreated.
Components of the Respiratory System:
- Nasal Cavity:
The first part of the respiratory system, which allows the passage of air and filters, warms, and humidifies it before it enters the lungs. This is done through the fine hairs in the nasal cavity and the blood capillaries that warm the air. - Pharynx:
A common passage for both the respiratory and digestive systems. It contains the epiglottis, which separates the air passage from the food passage. - Larynx:
The organ responsible for voice production, allowing air to pass from the pharynx into the trachea. It protects the lower respiratory system from foreign bodies and facilitates coughing. - Trachea:
A tube approximately 11 cm in length, made up of about 16 cartilage rings, lined with a membrane that warms the air as it passes through to the bronchi. The bronchi further distribute air to the lungs. The trachea is also lined with small cilia that trap bacteria and dust, expelling them via mucus. - Bronchi:
These are small branches of the trachea that distribute air into different parts of the lungs. The bronchi divide into two branches: - Right Bronchus: Shorter, wider, and more vertical than the left bronchus.
- Left Bronchus: Longer, narrower, and more horizontal than the right bronchus, making foreign bodies more likely to enter the right lung. Each bronchus further divides into smaller bronchioles.
- Alveoli:
These are air-filled sacs located at the ends of the bronchioles and are the critical site for gas exchange. There are approximately 300 million alveoli in the lungs, and they are surrounded by a fine network of capillaries that facilitate the exchange of gases. - Lungs:
The elastic organs located in the chest cavity, with the right lung having three lobes and the left lung having two lobes. Each lobe contains a large number of small air sacs called alveoli, which are crucial for gas exchange. - Pleural Membrane:
A double-layered membrane covering the lungs, with a small space between the layers filled with fluid that helps the lungs move smoothly during breathing.
The Importance of Oxygen and How It Transports to Alveoli:
Body cells require energy, which is produced through metabolism as a result of burning fats and nutrients. This process depends on the presence of oxygen, which enters the body through breathing. During oxidation, carbon dioxide is produced, and the body expels it through exhalation. As air passes through the upper respiratory system and reaches the alveoli, the alveoli fill with air, allowing gas exchange to occur between the alveoli and the surrounding capillaries. Oxygen has a higher concentration in the alveoli than in the blood of the capillaries, so oxygen moves from the alveoli (high concentration) to the capillaries (low concentration). In contrast, carbon dioxide has a higher concentration in the capillaries than in the alveoli, so it moves from the capillaries to the alveoli to be exhaled. In this way, oxygen enters the bloodstream and is distributed to all body cells, completing the gas exchange process.
Nursing Assessment for Respiratory Patients:
Various problems can affect the amount of air entering or leaving the alveoli, impacting the gas exchange process. Respiratory disorders can be either acute or chronic, and many respiratory diseases are infectious.
Symptoms and Signs Indicating Respiratory Diseases:
- Cough:
A clear sign of a disease in the airways or bronchi. Coughing helps expel foreign bodies and harmful secretions irritating the respiratory mucous membranes. The cough may be: - Dry: If the mucous membranes of the bronchi are simply inflamed.
- Productive (with mucus): Indicating excessive secretions in the bronchi, possibly due to an infection.
- Sputum:
When the body produces large amounts of mucus, it can cause irritation in the airways, changing the color and consistency of the sputum, especially in respiratory illnesses. - Hemoptysis (Blood in Sputum):
May occur in cases of chronic or acute bronchitis, pulmonary embolism, bronchial tumors, tuberculosis, or mitral valve stenosis. - Chest Pain:
Severe pain in the chest, particularly with inhalation, which may make the patient breathe shallowly. The pain may be sharp or stabbing, and it can occur under the armpit, breast, back, or chest. - Shortness of Breath:
Difficulty breathing that can affect the patient’s general condition, including their ability to sleep and sit up in bed. This may result from lung inflammation or constriction of the bronchi and can also be related to heart disease.
Nursing Needs for Respiratory Patients:
Continuous monitoring is required for respiratory patients, and any abnormal signs should be promptly communicated to the physician.
Nursing needs include:
- Ensure complete bed rest for the patient and monitor with a heart rate monitor.
- Administer oxygen therapy as prescribed.
- Monitor the patient's breathing rate and depth (difficulty breathing, rapid or shallow breathing).
- Observe for cyanosis (bluish discoloration of the skin or lips).
- Track any coughing or sputum production, noting color, quantity, and whether blood is present.
- Check the patient's temperature to rule out respiratory infections.
- If sputum is abnormal or has a foul odor, perform a sputum culture.
- Assist the patient in expelling secretions from the lungs by teaching breathing exercises, especially after chest or heart surgery or extended anesthesia.
- Administer medications as directed by the physician.
- Provide warm fluids and nutrition as prescribed.
- Prevent infection by placing a tissue over the patient's mouth during coughing and disposing of waste in a sealed container.
- For patients on mechanical ventilation or unconscious patients, suction the trachea and perform chest exercises regularly.
- Conduct blood gas analysis as directed by the physician.
- Notify the physician of any changes in the patient's condition.
- Ensure the patient’s physical and psychological comfort.
- Provide a quiet environment and minimize disruptions during nursing activities, including regular oral care.
- Nursing Care for Patients with Chronic Obstructive Pulmonary Disease (COPD)
Chronic Obstructive Pulmonary Disease (COPD):
COPD is a group of chronic, non-infectious
lung diseases that cause significant disruption in the airways, leading to
difficulty breathing. COPD is one of the leading causes of death globally, and
it is primarily caused by smoking. However, it is preventable and manageable if
caught early and the risk factors are controlled.
COPD typically results from one or both of the following conditions:
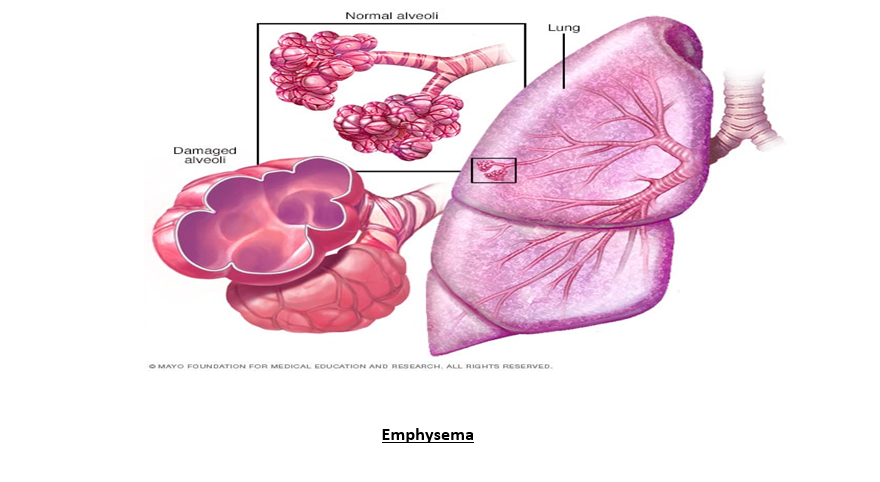
- Emphysema:
Emphysema is a condition where the alveoli are damaged, leading to difficulty in breathing due to the loss of tissue and impaired function of the lungs. It is one of the most common causes of COPD and leads to chronic airway obstruction. - Chronic Bronchitis:
Chronic bronchitis is characterized by long-term inflammation of the bronchial lining, resulting in persistent coughing with mucus production, difficulty breathing, and wheezing. The condition is considered chronic if it lasts for at least three months over two consecutive years.
Causes of COPD:
COPD is most commonly caused by smoking, including cigarettes, cigars, and pipes. The longer the duration of smoking, the higher the likelihood of developing COPD. Other causes include:
- Secondhand smoke exposure
- Exposure to polluted air or dust
- Inhalation of irritating chemicals
- Inhalation of fumes from burning fuel in poorly ventilated homes
- Family history of COPD
- Genetic factors, such as a deficiency in alpha-1 antitrypsin, a protein that helps protect the lungs from damage. About 5% of people with COPD have this deficiency, which can also affect the liver.
Physiology of COPD:
Air enters the lungs through the trachea and bronchi, where it passes into
smaller bronchioles and ends in the alveoli. The alveoli are lined with very
thin walls and surrounded by capillaries, where gas exchange occurs—oxygen from
the air moves into the blood, and carbon dioxide from the blood is expelled
during exhalation. COPD causes the loss of elasticity in the airways and
alveoli, leading to air trapping during exhalation, which affects breathing
efficiency.
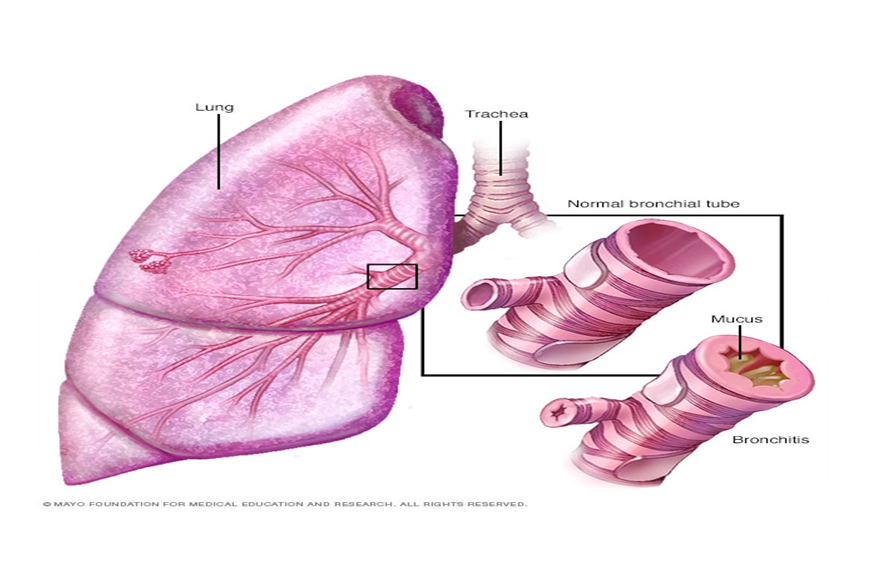
- Bronchitis
Bronchitis is the inflammation of the lining of the airways (bronchi) that carry air to and from the lungs. It can be classified as acute or chronic.
Acute bronchitis often develops from a cold or respiratory infection, and it is common. Chronic bronchitis, a more severe condition, results from continuous irritation or inflammation of the bronchial tubes, typically caused by smoking.
Symptoms of Chronic Bronchitis:
- Mucus production (sputum): This can be clear, white, gray, or yellowish/green, and rarely may be tinged with blood.
- Fatigue
- Shortness of breath
- Mild fever and chills
- Chest tightness
- Wheezing
- Continuous cough
- Sputum production
- Discomfort and constant irritation
Causes of Bronchitis:
The airway is lined with a mucus membrane that is highly sensitive to irritants. This sensitivity causes a rapid response and increased mucus production, as well as thickening of the muscle layer inside the bronchial walls.
The irritants that can cause bronchitis include:
- Tobacco smoke
- Dust (especially asbestos, coal, cotton, and silica)
- Smog and chemical vapors like sulfur dioxide or nitrogen dioxide
- Gastroesophageal reflux (GERD)
- Viral strains (such as those causing influenza) and some bacteria also play a role in causing and prolonging bronchitis.
Diagnosis of Chronic Bronchitis:
The most prominent sign of chronic bronchitis is a persistent cough accompanied by sputum. This is the primary diagnostic criterion. Other tests may include:
- Physical examination: It can reveal wheezing and prolonged exhalation time, indicative of the disease.
- Chest X-ray: This helps exclude other lung conditions that may cause cough, such as pneumonia.
- Lung function tests: These tests evaluate the breathing process, lung efficiency, and help diagnose respiratory diseases, including asthma and respiratory infections.
- CT scan: To provide detailed images of the lungs.
Complications of Chronic Bronchitis:
- Shortness of breath
- Pneumonia
- Respiratory failure
- Pneumothorax (collapsed lung)
- Polycythemia (excessive red blood cells)
Treatment of Chronic Bronchitis:
While there is no definitive cure for chronic bronchitis, the disease can be managed and controlled with medication and lifestyle changes, especially when diagnosed and treated early.
- Stop smoking: The first step in treatment is smoking cessation.
Medications:
- Bronchodilators: These medications open the airways in the lungs, making it easier to breathe. These are often administered via an inhaler (such as Albuterol and Ipratropium).
- Steroids: To reduce inflammation, often used in inhaled form, but sometimes orally, if symptoms persist.
- Antibiotics: If the infection is bacterial, antibiotics such as Levofloxacin may be prescribed.
- Cough suppressants: Such as Guaifenesin to alleviate symptoms.
Pulmonary Rehabilitation: This is a program aimed at improving breathing through specific breathing exercises taught by a specialist.
Nursing Care for Acute Bronchitis:
- Improve secretion clearance through walking, deep breathing, and controlled coughing.
- Increase fluid intake to loosen mucus and prevent dehydration, which can be common due to rapid breathing and fever.
- Provide rest and avoid bronchial irritants, while maintaining a light and healthy diet to facilitate recovery.
- Educate patients to complete the full course of antibiotics if prescribed and avoid over-the-counter antihistamines, cough suppressants, or decongestants, which may exacerbate mucus retention.
- Encourage the patient to quit smoking completely.
- Educate the patient to recognize early symptoms of acute bronchitis and report them immediately.
Nursing Interventions for Chronic Bronchitis:
- Answer patient’s questions and encourage them and their family to express concerns about the disease.
- Perform chest physiotherapy, including chest percussion, vibration, and postural drainage multiple times a day.
- Ensure the patient gets enough fluids (around 3 liters per day) to ease mucus clearance.
- Schedule respiratory therapy before meals or an hour after meals.
- Provide oral care after bronchodilator inhalation.
- Promote daily activities and offer recreational activities when appropriate.
- Encourage the patient to alternate between periods of activity and rest to avoid fatigue.
- Monitor for changes in the quality and quantity of sputum, increased respiratory rate, changes in breath sounds, and sleep disturbances.
- Check the patient’s weight regularly (three times a week).
- Assess nutritional status regularly.
- Look for signs of respiratory infections, such as increased cough, fever, and purulent sputum, and report these changes immediately.
- Advise the patient to avoid crowds and people with known respiratory infections and encourage vaccinations for pneumonia and influenza.
- Provide medications as prescribed and monitor the patient’s response.
- Assist with adjustments to respiratory function as needed.
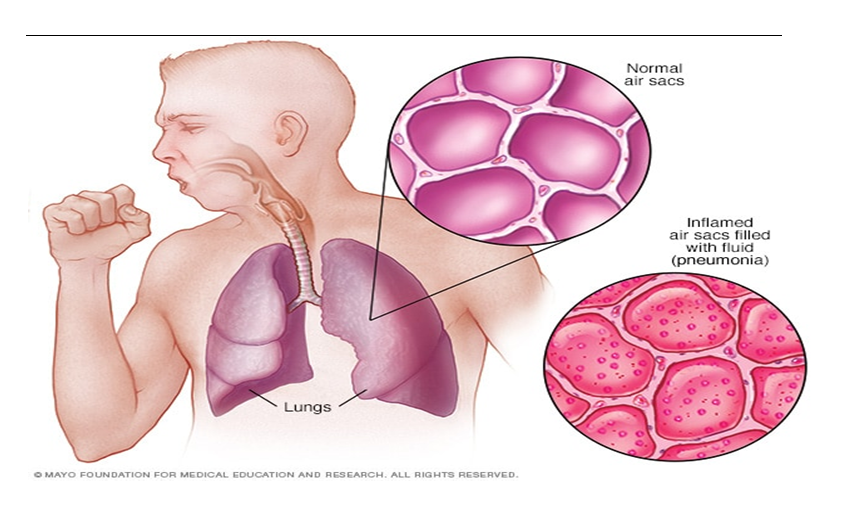
- Nursing Care for Pneumonia
Pneumonia
is a microbial infection that affects all or part of the lung, and it can be
caused by lung microbes or the inhalation of vomit or chemical gases, or due to
chronic inflammation of the respiratory system and reduced immunity.
Symptoms:
- Fever
- Shivering
- Bluish discoloration of the lips, nails, and skin
- Increased heart rate and rapid breathing
- Cough with chest pain
Complications of Pneumonia: Common complications include:
- Low oxygen levels in the blood
- Drop in blood pressure to levels that threaten the patient’s life
- Lung abscess or empyema
- Severe lung injury
- Acute Respiratory Distress Syndrome (ARDS)
Treatment of Pneumonia:
- Antibiotics and sometimes antiviral or antifungal medications.
- Breathing support treatments.
Nursing Care:
- Continuously monitor vital signs (pulse, respiration, temperature).
- Observe the color of the patient (lips, nails).
- Monitor sputum (color, quantity, odor).
- Monitor the patient's symptoms and report immediately to the doctor if they occur, such as:
- Sudden drop in temperature with persistent pulse and respiration, indicating spread of the disease and shock.
- Persistent high fever, chest pain, and shortness of breath, which could suggest pus in the pleural membrane.
- Provide emotional and physical comfort to the patient.
- Ensure the patient is in a comfortable position in bed.
- Encourage the patient to cough to expel secretions and practice breathing exercises.
- Administer oxygen as per doctor's orders.
- Administer medication as prescribed by the doctor.
- Provide nutrition as instructed by the doctor.
- Maintain oral care, skin care, and general hygiene.
- Ensure laboratory blood tests and sample analysis are completed.
- Administer antibiotics as required.
- Keep the patient warm and comfortable.
- Perform suctioning as needed.
- Manage pain and cough.
- Provide overall comfort.
- Teach the patient proper hand hygiene.
- References
- National Institutes of Health (NIH): https://www.nih.gov/
- Centers for Disease Control and Prevention (CDC): https://www.cdc.gov/
- World Health Organization (WHO): https://www.who.int/about
- Chronic Obstructive Pulmonary Disease (COPD): https://www.copdfoundation.org/What-is-COPD/Understanding-COPD/What-is-COPD.aspx
- American Journal of Respiratory and Critical Care Medicine: https://www.atsjournals.org/journal/ajrccm