العمل الإجرائي للعلامات الحيوية
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | دلائل الاجراءات التمريضية لأقسام الداخلي |
| كتاب: | العمل الإجرائي للعلامات الحيوية |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:55 AM |
الوصف
"last update: 22 April 2025" تحميل الدليل
- اعداد
دليل الأقسام الداخلية
تحت اشراف
- أ.د/ محمد لطيف الرئيس التنفيذي للمجلس الصحي المصري - د/ كوثر محمود نقيب عام التمريض المصري – عضو مجلس الشيوخ
اعداد
م | الاسم | الوظيفة |
1 | أ. د /امل احمد خليل مرسي | نائب رئيس الجامعة لشئون التعليم والطلاب – جامعة بورسعيد |
2 | أ.د / عفاف عبد العزيز عبد العزيز بصل | عميد كلية التمريض –استاذ تمريض باطنه وجراحي جامعة طنطا |
3 | أ.د/ زينب حسين على محمد سعد | وكيل الكلية لشئون البيئة وخدمة المجتمع – كلية التمريض – جامعه حلوان |
4 | أ.د /امل سعيد طه رفاعي | أستاذ ورئيس قسم التمريض الباطني الجراحي – جامعة بنها |
5 | أ.د /حنان احمد السباعي على | استاذ التمريض التمريض الباطني الجراحي- كلية التمريض – جامعة القاهرة |
6 | د /نيفين عبدربه النبي محمد عبد النبي | رئيس الإدارة المركزية ندباَ –وزاره الصحة |
7 | د /مايسه حسني احمد تمام | مدير عام للإدارة ندباَ – وزاره الصحة |
8 | د نانسي علاء الدين عبد الباسط على | المشرف على التعليم الفني- الهيئة العامة للرعاية الصحية |
9 | د شيرين محمد محمد سعدالدين | المشرف على تطوير الخدمات التمريضية –الهيئة العامة للرعاية الصحية |
10 | د/ مى محمود العسال | مدير عام الإدارة العامة لشئون المعاهد الفنية الصحية |
11 | أ.م.د/ هبة محمود محمد | أستاذ مساعد تمريض صحة الام وحديثي الولادة –كلية التمريض - جامعة عين شمس |
المشاركين | ||
12 | /أنهلة كامل مصطفي | مسئول التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
13 | /أمها سعد محمد النادي | عضو إدارة التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
14 | /أثروت عبد العال محمد | عضو إدارة التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
15 | أ /منى على عبد الرحمن الكتامى | أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
16 | أ / شيرين عبد الحكيم عبد الحكيم خطاب | أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
17 | أ/بهاء فؤاد برسوم | أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
- قسم المهنة
"اقسم بالله العظيم
أن أخلص فى عملى و أتقى الله فى مهنتى و أحترم قوانينها و أنظمتها و أؤدى مهامى بكل كفاءة و إخلاص
و أن أستند فى أدائى على المعرفة المستمدة من علوم التمريض
و أبذل قصارى جهدى لرعاية كل من وكل إلى رعايتهم و أحفظ كرامتهم و أكتم سرهم و أدافع عن حقوقهم و حمايتهم من أى أذى
و ألا أخشى فى قول الحق لومة لائم و أوفر بيئة أمنة للمريض و الأسرة و المجتمع
و أن أستمر فى تطوير نفسى و أوقر من علمنى و أحترمه
و أتعاون مع زملائى فى المهنة على البر و التقوى
والله على ما أقول شهيد"
- رؤية ورسالة الرعاية التمريضية
رؤية الرعاية التمريضية بوحدة رعاية مرضى الداخلى
يتطلع أفراد هيئة التمريض بوحدة رعاية مرضى الداخلى للإرتقاء بمهنة التمريض وتقديم الرعاية التمريضية لمرضى الوحدة بفاعلية وأمان وجودة طبقاً للمعايير المصرية والقومية والعالمية.
رسالة الرعاية التمريضية بوحدة رعاية مرضى الداخلى
يلتزم أفراد هيئة التمريض بوحدة رعاية مرضى الداخلى برفع المستوى الصحي للمرضى وتقديم أفضل رعاية تمريضية لهم بما يتماشى مع أهداف وإجراءات المستشفى وإدارة التمريض وكذلك تعمل على الإرتقاء بالمستوى العلمي والعملي لجميع أفراد هيئة التمريض بالوحدة وتغيير إتجاهاتهم نحو الإتجاهات الحديثة فى العلوم التمريضية والطبية .
- العلامات الحيوية
التعريف :
العلامات الحيوية هي مؤشرات أساسية لصحة الإنسان، وتوفر معلومات حيوية حول وظائف الجسم الأساسية. تشمل العلامات الحيوية الرئيسية: معدل النبض، ضغط الدم، معدل التنفس، ودرجة الحرارة.
قياس درجة الحرارة
أ ) قياس درجة الحرارة عن طريق الفم
التعريف :
درجة الحرارة هي مؤشر على حرارة الجسم الداخلي. يتم قياسها باستخدام ميزان حرارة.
الأسباب :
متابعة الوظائف الحيوية للمريض.
طرق القياس
هناك عدة طرق لقياس حرارة الجسم، وكل طريقة لها مزاياها وقيودها. في ما يلي نظرة على الطرق الأكثر شيوعاً:
1. الميزان الحراري الفموي (Oral Thermometer):
أ. الطريقة:
- يوضع الميزان تحت اللسان، ويغلق الفم بإحكام.
- يُترك الميزان في مكانه لمدة 3 دقائق.
ب. المزايا:
- سهل الاستخدام ومتوفر بشكل واسع.
- يوفر قياسات دقيقة للبالغين.
ج. القيود:
- قد تكون غير دقيقة إذا كان الشخص قد تناول طعاماً أو شراباً ساخناً أو بارداً حديثاً.
- لا ينصح باستخدامه للأطفال الصغار أو المرضى الذين لا يستطيعون الحفاظ على الفم مغلقاً.
2. الميزان الحراري الإبطي (Axillary Thermometer):
أ. الطريقة:
- يوضع الميزان في الإبط ويتم الضغط برفق على الذراع لتثبيته في مكانه.
- يُترك الميزان في مكانه حتى ي5 دقائق.
ب. المزايا:
- مناسب للرضع والأطفال الصغار.
- سهل الاستخدام ولا يتطلب الكثير من التعاون من المريض.
ج. القيود:
- قد يكون أقل دقة مقارنة بالطرق الأخرى.
- تأثرات مثل كثافة الشعر أو الرطوبة يمكن أن تؤثر على القياس.
3. الميزان الحراري الشرجي (Rectal Thermometer):
أ. الطريقة:
- يُدخل الميزان بلطف في المستقيم بمقدار حوالي 2.5 سم (1 بوصة).
- يُترك في مكانه حتى 1 دقيقة
ب. المزايا:
- يعتبر الأكثر دقة في قياس درجة حرارة الجسم الداخلية.
- مفيد في الحالات التي تحتاج إلى قياسات دقيقة، مثل الرضع أو الأشخاص في الحالات الطبية الخاصة.
ج. القيود:
- قد يكون غير مريح لبعض الأشخاص.
- يتطلب الحذر عند استخدامه لتجنب الإصابة.
4. الميزان الحراري الأذني (Tympanic Thermometer):
أ. الطريقة:
- يوضع ميزان الحرارة في قناة الأذن.
- يتم قياس درجة الحرارة عن طريق استشعار الحرارة المنبعثة من طبلة الأذن.
ب. المزايا:
- سريع وسهل الاستخدام.
- مناسب للأطفال والبالغين.
ج. القيود:
- قد يتأثر بالأوساخ أو الشمع في الأذن.
- قد يكون أقل دقة إذا لم يتم وضعه بشكل صحيح في الأذن.
5. الميزان الحراري الجبهي (Forehead Thermometer):
أ. الطريقة:
- يستخدم عادةً ميزان حرارة بالأشعة تحت الحمراء، يُمرر عبر الجبهة لقياس درجة الحرارة.
ب. المزايا:
- غير ملامس، مما يجعله مناسباً للأطفال الصغار والمصابين بالحالات الصحية التي تجعل القياس المباشر صعباً.
- سريع وسهل الاستخدام.
ج. القيود:
- قد يتأثر بالعوامل البيئية مثل الطقس الحار أو البارد.
- يحتاج إلى معايرة دقيقة لضمان النتائج الصحيحة.
المعدلات الطبيعية :
36.4 – 37.4 درجة مئوية.
ما تعنيه النتائج:
- ارتفاع درجة الحرارة: قد يشير إلى عدوى أو التهاب.
- انخفاض درجة الحرارة: قد يكون نتيجة لاضطراب في التنظيم الحراري أو حالة طبية طارئة.
القائم بالعمل :
الفريق التمريضي.
الأدوات :
ترمومتر زئبقي- كحول - قطعه شاش - مؤقت زمني.
الخطوات :
- التعرف على المريض. ( اسم المريض و اسورة التعريف )
- اشرح الإجراء للمريض.
- غسل الأيدي.
- تحضير الأدوات.
- الحفاظ على خصوصية المريض.
- ضبط الترمومتر و تحريكه بقوة ليصل خط الزئبق إلى 35 درجه ( نقطة البداية ).
- تنظيف الترمومتر من الجزء الزئبقي من اعلي إلى أسفل بالكحول.
- وضع الترمومتر عند مستوى النظر للتأكد من وصوله الي نقطة البداية.
- وضع الجزء الزئبقي بالترمومتر تحت اللسان لمدة (ثلاث دقائق) بفم المريض.
- استخراج الترمومتر من فم المريض.
- تنظف الترمومتر من الاسفل الي الاعلي بقطعة شاش جافة.
- قراءة القياس تسجيل قراءة الترمومتر بالنموذج الخاص بتسجيل درجة الحرارة.
- تحريك الترمومتر بقوة لينخفض مستوي الزئبق.
- تنظيف الترمومتر الجزء الزئبقي من اعلى إلى اسفل بالماء والصابون وتجفيفه وتطهيره بالكحول.
- وضع الترمومتر بالوعاء المخصص له.
- غسيل الايدي.
- طمأنة المريض.
- تسجيل اية علامات طارئة.
ب) قياس درجة الحرارة عن طريق الإبط
المعدلات الطبيعية :
36.4 – 37.4 درجة مئوية.مع زيادة نص درجة مئوية علي المعدل الموجود
القائم بالعمل :
الفريق التمريضي.
الأدوات :
ترمومتر زئبقي- كحول - قطعه شاش - مؤقت زمني.
الخطوات :
1. التعرف على المريض. ( اسم المريض و اسورة التعريف )
2. اشرح الإجراء للمريض.
3. غسل الأيدي.
4. تحضير الأدوات.
5. الحفاظ على خصوصية المريض.
6. ضبط الترمومتر و تحريكه بقوة ليصل خط الزئبق إلى 35 درجه (نقطة البداية).
7. تنظيف الترمومتر من الجزء الزئبقي من اعلي إلى أسفل بالكحول.
8. وضع الترمومتر عند مستوى النظر للتأكد من وصوله إلي نقطة البداية.
9. وضع الجزء الزئبقي بالترمومتر تحت الإبط مع مراعاة أن يكون هذا المكان جاف.لمدة (خمسة دقائق).
10. استخراج الترمومتر من فم المريض.
11. تنظف الترمومتر من الأسفل إلي الاعلي بقطعة شاش جافة.
12. قراءة القياس تسجيل قراءة الترمومتر بالنموذج الخاص بتسجيل درجة الحرارة. مع مراعاة ( زيادة نصف درجه عند قراءه الترمومتر) وموقع عليه.
13. تحريك الترمومتر بقوة لينخفض مستوي الزئبق.
14. تنظيف الترمومتر الجزء الزئبقي من اعلي إلى أسفل بالماء والصابون وتجفيفه وتطهيره بالكحول.
15. وضع الترمومتر بالوعاء المخصص له..
16. غسيل الأيدي.
17. طمأنة المريض.
18. تسجيل أية علامات طارئة.
ج) قياس درجة الحرارة عن طريق فتحة الشرج
التعريف :
درجه الحرارة هي عدد يدل علي حاله الجسم من حيث السخونة و البرودة.
الأسباب :
متابعة الوظائف الحيوية للمريض.
المعدلات الطبيعية :
36.4 – 37.4 درجة مئوية مع طرح نصف درجة.
القائم بالعمل :
الفريق التمريضي.
الأدوات :
ترمومتر زئبقي- كحول - قطعه شاش - مؤقت زمني.
الخطوات :
1. التعرف على المريض. ( اسم المريض و أسورة التعريف )
2. اشرح الإجراء للمريض.
3. غسيل الأيدي.
4. تحضير الأدوات.
5. الحفاظ على خصوصية المريض.
6. ضبط الترمومتر وتحريكه بقوة ليصل خط الزئبق إلى 35 درجه ( نقطة البداية ).
7. تنظيف الترمومتر من الجزء الزئبقي من اعلي إلى أسفل بالكحول.
8. وضع الترمومتر عند مستوى النظر للتأكد من وصوله إلي نقطة البداية.
9. وضع جيل على حافة الجزء الزئبقي ووضع الترمومتر لمده دقيقه مع مراعاة أن يكون المريض على جانبه.
10. إزالة الترمومتر وينظف من أسفل إلى الجزء الزئبقي بقطعة شاش جافة.
11. قراءة القياس وتسجيل قراءة الترمومتر بالنموذج الخاص بتسجيل درجة الحرارة. مع مراعاة ( نقص نصف درجه عند قراءه الترمومتر).
12. تحريك الترمومتر بقوة لينخفض مستوي الزئبق.
13. تنظيف الترمومتر الجزء الزئبقي من اعلي إلى أسفل بالماء والصابون وتجفيفه وتطهيره بالكحول.
14. وضع الترمومتر بالوعاء المخصص له.
15. غسيل الأيدي.
16. طمأنة المريض.
17. تسجيل أية علامات طارئة.
ملحوظة : تستعمل طريقة القياس عن طريق فتحة الشرج فى حالات الأطفال وحالات الحروق. |
قياس النبض
التعريف :
النبض هو الموجه المتولدة في الشرايين نتيجة لانقباض القلب ويمكن إحساس النبض عبر تحسس الشرايين الكبيرة في جسم الإنسان مثل العنق والمعصم .
الأسباب :
متابعة الوظائف الحيوية للمريض.
كيفية القياس:
- الموقع: يمكن قياس معدل النبض عند معصم اليد أو العنق.
- الطريقة: استخدم أصابعك لإيجاد النبض واضغط برفق. قم بعد عدد النبضات خلال 60 ثانية، أو خلال 30 ثانية واضرب النتيجة في 2.

المعدلات الطبيعية :
- البالغون: 60-100 نبضة في الدقيقة.
- الأطفال: 70-120 نبضة في الدقيقة.
- الرضع: 100-160 نبضة في الدقيقة.
ما تعنيه النتائج:
معدل نبض مرتفع: قد يدل على الإجهاد، القلق، أو مشاكل في القلب.
معدل نبض منخفض: قد يشير إلى انخفاض نشاط الغدة الدرقية أو مشاكل قلبية.
القائم بالعمل :
الفريق التمريضي.
الأدوات :
مؤقت زمني.
الخطوات :
1. التعرف على المريض. ( اسم المريض و أسورة التعريف )
2. اشرح الإجراء للمريض.
3. غسل الأيدي.
4. تحضير الأدوات.
5. اختيار وضع مريح للمريض.
6. وضع طرف اثنين أصابع من اليد (السبابة والوسطى ) على الشريان (الكعبري – السباتي -الفخذى)
7. استخدام الساعة باليد الأخرى.
8. عد النبض لمدة دقيقه واحدة كاملة
9. تسجيل النبض بنموذج الملاحظات الحيوية وتقوم بالإبلاغ إذا كان النبض ( سريع – بطئ – قوي - ضعيف- غير منتظم ).
10. طمأنة المريض.
11. غسيل الأيدي.
قياس التنفس
التعريف :
تقييم معدل التنفس وانتظامه (وهو عمليه حصول الجسم علي الأكسجين من خلال التنفس وهو ضروري للقيام بأنشطته والتخلص من ثاني أكسيد الكربون ).
الأسباب :
متابعة الوظائف الحيوية للمريض.
كيفية القياس:
- الطريقة: راقب حركة الصدر أو البطن خلال دقيقة كاملة، واحتسب عدد مرات التنفس.
المعدلات الطبيعية :
البالغون: 12-20 نفساً في الدقيقة.
الأطفال: 20-30 نفساً في الدقيقة.
الرضع: 30-60 نفساً في الدقيقة.
ما تعنيه النتائج:
- معدل تنفس مرتفع: قد يشير إلى مشاكل في الجهاز التنفسي أو القلق.
- معدل تنفس منخفض: قد يدل على مشاكل في الرئة أو مشاكل عصبية
القائم بالعمل :
الفريق التمريضي.
الأدوات :
مؤقت زمني.
الخطوات :
1. التعرف على المريض. ( اسم المريض و أسورة التعريف )
2. اشرح الإجراء للمريض.
3. تحضير الأدوات.
4. مراعاة عدم قياس التنفس بعد مجهود عضلي.
5. وضع المريض في وضع مريح يفضل نصف جالس.
6. التأكد أن حركه صدر المريض واضحة لها.
7. ملاحظه ارتفاع وانخفاض صدر المريض.
8. يعد كل شهيق وزفير بمرة تنفس واحدة ولمدة دقيقه كاملة.
9. ملاحظة إي علامات غير طبيعيه في التنفس.
10. ملاحظة لون المريض خاصة حول الشفتين وأظافر الأصابع.
11. تسجيل معدل التنفس في الاستمارة الخاصة بالمريض.
12. إبلاغ الطبيب عن اي علامات غير طبيعية.
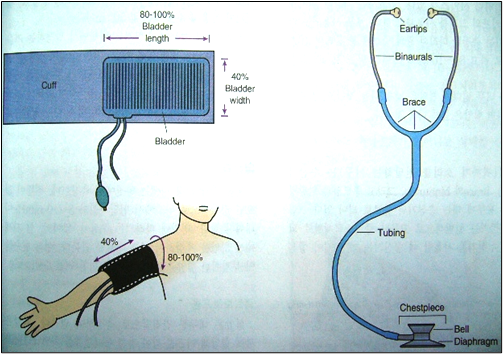
قياس ضغط الدم
التعريف :
تقييم حركه الدورة الدموية عن طريق معرفه حجم الدم ، الدم العائد للقلب مدي مقأومه الأوعية الدموية الطرفية، ومرونة الشرايين.
الأسباب :
متابعة الوظائف الحيوية للمريض.
كيفية القياس:
- الأدوات: استخدم جهاز قياس ضغط الدم (سوار أوتوماتيكي أو تقليدي) لتحديد القيم.
- الطريقة: اجلس في وضع مريح وضع السوار حول ذراعك. اتبع التعليمات الموجودة على الجهاز لقياس الضغط.
المعدلات الطبيعية :
- ضغط الدم الطبيعي: أقل من 120/80 ملم زئبق.
- ارتفاع ضغط الدم: 140/90 ملم زئبق أو أعلى.
ما تعنيه النتائج:
ضغط الدم المرتفع: قد يشير إلى زيادة مخاطر الأمراض القلبية والسكتة الدماغية.
ضغط الدم المنخفض: قد يكون نتيجة للجفاف أو مشاكل في القلب.
القائم بالعمل :
الفريق التمريضي.
الأدوات :
جهاز ضغط وسماعة طبيب.
الخطوات :
1. التعرف على المريض.
2. (اسم المريض و أسورة التعريف )
3. اشرح الإجراء للمريض.
4. تحضير الأدوات.
5. مراعاة عدم قياس الضغط بعد مجهود عضلي.
6. وضع المريض في وضع مريح.
7. الحفاظ على خصوصية المريض.
8. قياس ضغط الدم قبل و بعد إعطاء أدوية ارتفاع ضغط الدم.
9. تسجيل قياس ضغط الدم مباشرة بالنموذج المخصص لذلك.
10. تحديد نوعية الوجبات الغذائية ( قليل الملح و الدهون ).
11. ملاحظة المضاعفات التي قد تحدث للمريض ( نزيف من الأنف ).
المعدلات الطبيعية للعلامات الحيوية طبقا للفئة العمرية
ختلف معدلات العلامات الحيوية مثل ضغط الدم، معدل ضربات القلب، معدل التنفس ودرجة الحرارة حسب الفئة العمرية. فيما يلي جدول يوضح المعدلات الطبيعية لهذه العلامات وفقاً للعمر:

ملاحظات:
- معدل ضربات القلب: يمكن أن يكون أعلى عند الأطفال والرضع ويقل مع التقدم في العمر.
- معدل التنفس: يكون أعلى عند الرضع والأطفال الصغار، ويقل تدريجياً مع التقدم في العمر.
- ضغط الدم: يزداد تدريجياً مع تقدم العمر، ويختلف باختلاف الجنس والصحة العامة.
- درجة الحرارة: تكون عادةً ضمن نطاق 36.1 إلى 37.2 درجة مئوية في البالغين، وقد تختلف قليلاً بناءً على وقت اليوم والنشاط.
تذكر أن هذه القيم هي نطاقات عامة وقد تختلف بعض الشيء من فرد إلى فرد. للحصول على تقييم دقيق للحالة الصحية، من الأفضل استشارة طبيب أو مقدم رعاية صحية.
- المراجع
دليل العمل الاجرائي قسم الداخلي2017