العمل الإجرائي لرسم القلب
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | دلائل الاجراءات التمريضية لأقسام الداخلي |
| كتاب: | العمل الإجرائي لرسم القلب |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:55 AM |
الوصف
"last update: 22 April 2025" تحميل الدليل
- اعداد
دليل الأقسام الداخلية
تحت اشراف
- أ.د/ محمد لطيف الرئيس التنفيذي للمجلس الصحي المصري - د/ كوثر محمود نقيب عام التمريض المصري – عضو مجلس الشيوخ
اعداد
|
م |
الاسم |
الوظيفة |
|
1 |
أ. د /امل احمد خليل مرسي |
نائب رئيس الجامعة لشئون التعليم والطلاب – جامعة بورسعيد |
|
2 |
أ.د / عفاف عبد العزيز عبد العزيز بصل |
عميد كلية التمريض –استاذ تمريض باطنه وجراحي جامعة طنطا |
|
3 |
أ.د/ زينب حسين على محمد سعد |
وكيل الكلية لشئون البيئة وخدمة المجتمع – كلية التمريض – جامعه حلوان |
|
4 |
أ.د /امل سعيد طه رفاعي |
أستاذ ورئيس قسم التمريض الباطني الجراحي – جامعة بنها |
|
5 |
أ.د /حنان احمد السباعي على |
استاذ التمريض التمريض الباطني الجراحي- كلية التمريض – جامعة القاهرة |
|
6 |
د /نيفين عبدربه النبي محمد عبد النبي |
رئيس الإدارة المركزية ندباَ –وزاره الصحة |
|
7 |
د /مايسه حسني احمد تمام |
مدير عام للإدارة ندباَ – وزاره الصحة |
|
8 |
د نانسي علاء الدين عبد الباسط على |
المشرف على التعليم الفني- الهيئة العامة للرعاية الصحية |
|
9 |
د شيرين محمد محمد سعدالدين |
المشرف على تطوير الخدمات التمريضية –الهيئة العامة للرعاية الصحية |
|
10 |
د/ مى محمود العسال |
مدير عام الإدارة العامة لشئون المعاهد الفنية الصحية |
|
11 |
أ.م.د/ هبة محمود محمد |
أستاذ مساعد تمريض صحة الام وحديثي الولادة –كلية التمريض - جامعة عين شمس |
|
المشاركين |
||
|
12 |
/أنهلة كامل مصطفي |
مسئول التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
|
13 |
/أمها سعد محمد النادي |
عضو إدارة التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
|
14 |
/أثروت عبد العال محمد |
عضو إدارة التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
|
15 |
أ /منى على عبد الرحمن الكتامى |
أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
|
16 |
أ / شيرين عبد الحكيم عبد الحكيم خطاب |
أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
|
17 |
أ/بهاء فؤاد برسوم |
أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
- التعريف
رسم القلب أو (ECG) هو يعني رسم القلب الكهربائي ((electrocardiogram أو مخطط القلب الكهربائي electrocardiograph)).
رسم القلب يكون مهم جدا في تشخيص حالات عديدة منها :
· تغييرات في ضربات القلب الايقاعية المنتظمة.
· يساعد في تشخيص سبب الام الصدر.
· أستخدام مذيبات الجلطة في حالات الاحتشاء القلبي (myocardialinfarction) يعتمد علي رسم القلب.
. يساعد ايضا في تشخيص سبب ضيق التنفس (breathlessness).
- كهربية القلب
تعريف كهربية القلب :
أنقباض اي عضلة يكون مصاحب بتيارات كهربائية تسمي (depolarization) أي مزيل الاستقطاب و هذه التيارات يمكن ان تُسجل بواسطة أقطاب كهربائية (electrodes) وتكون هذه الأقطاب موصلة بسطح الجسم ، ولهذا فيمكن ان نسجل الانقباض لعضلات الجسم كله
و بالتالي اذا اردنا تسجيل انقباض عضلات القلب فقط بوضوح فلابد ان يكون الشخص مستريح و جميع عضلات جسمه الاخري منبسطة.
و بالرغم من ان القلب يحتوي علي 4 حجرات ، فسنراه في التصوير الكهربائي حجرتان فقط لأن الاذينين ينقبضان معا و البطينين ايضا.
النبض الطبيعي :
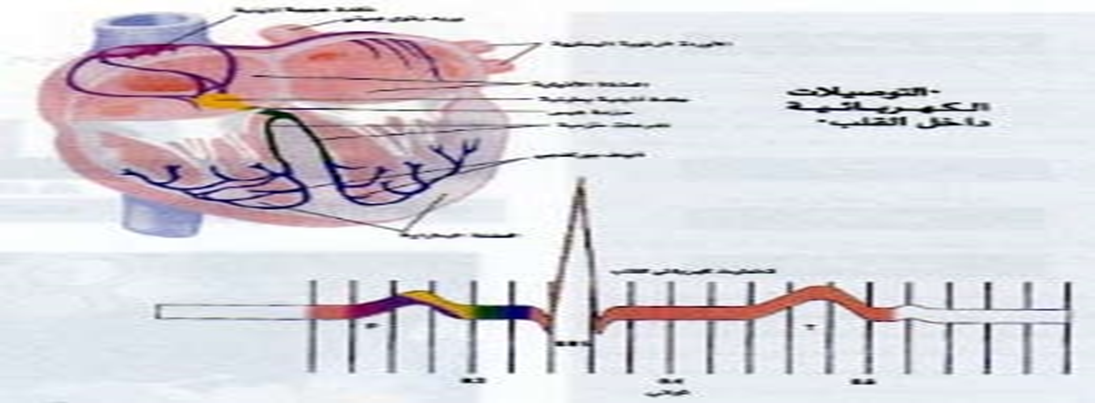
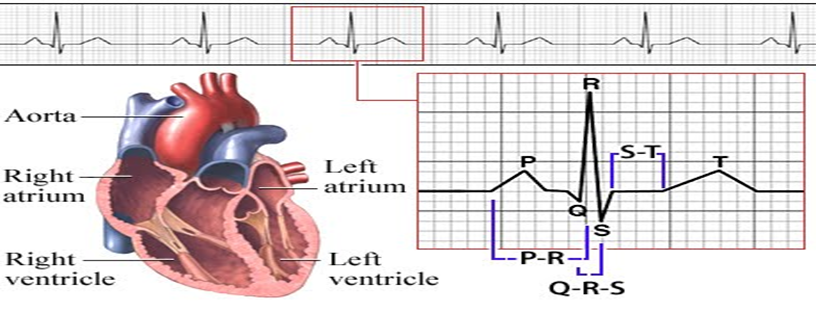
تنبع ضربات القلب الايقاعية المنتظمة من داخل نسيج عضلة القلب نفسها فهي ذاتية الحركة حيث يبدأ النبض الطبيعي بإشارة كهربائية تُصدر من مولد ومنظم كهربائي عصبي عضلي متخصص ، صغير الحجم جداً يقع في جدار الأذين الأيمن يسمى (العقدة الجيبية الأذينية) أوsinoatrial node، بمعدل 60-100 نبضة / إشارة كهربائية في الدقيقة . وتنتشر هذه الإشارة الكهربائية بسرعة كبيرة للأذينين مما يجعلهما ينقبضان لدفع الدم من الأذينين للبطينين ثم تنتقل تلك الإشارة الكهربائية إلى مستقبل وفي نفس الحال يعتبر مولداً احتياطياً صغير الحجم ويسمى (العقدة الأذينية البطينية) أو atrioventricular node جداً يقع بين البطينين والأذينين والتي تسمح بمرور الإشارة الكهربائية عن طريق توصيلات كهربائية تتفرع من العقدة البطينية الأذينية إلى البطينين في جزء من الثانية مما يجعلهما ينقبضان لدفع الدم من البطينين لخارج القلب والبطين الأيمن يدفع بالدم غير المؤكسد للرئتين ليتم أكسدته والبطين الأيسر يدفع بالدم المؤكسد لجميع أجزاء الجسم لتستفيد من الدم المؤكسد الذي يعود بعد أنتزاع الأوكسجين منه للجزء الأيمن من القلب وهكذا تكتمل دورة واحدة للدم.
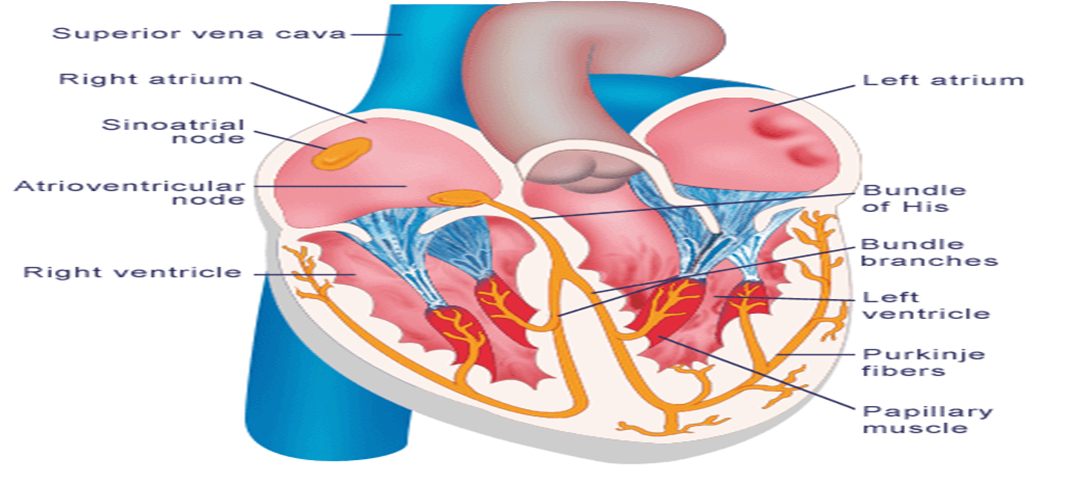
وبالتالي في الانسان الطبيعي تنشأ الاشارات الكهربية من ( العقدة الجيب أذينية) وفي هذا الحين يسمي النظام ب(النظم القلبي) أو (sinus rhythm) ، اما في بعض الحالات المرضية يمكن ان تنشأ التيارات من مصدر اخر مثل ( العقدة الاذينية البطينية) و يسمي النظام في هذا الحين ب( النظم العقدي) أو nodal rhythm أو ممكن ينبع من اي مصدر اخر مثل عضلات البطين نفسه و هذا قد يكون بسبب فشل العقدة الجيب اذينية في اصدار نبضات أو وجود مصدر خارجي - في اي مكان اخر في القلب - ينبض بمعدل اعلي من منظم ضربات القلب الاساسي فيأخذ مكانه وبالتالي في الانسان الطبيعي تنشأ الاشارات الكهربية من ( العقدة الجيب أذينية) وفي هذا الحين يسمي النظام ب(النظم القلبي) أو (sinus rhythm ) ، اما في بعض الحالات المرضية يمكن ان تنشأ التيارات من مصدر اخر مثل ( العقدة الاذينية البطينية) و يسمي النظام في هذا الحين ب( النظم العقدي) أو ( nodal rhythm ) أو ممكن ينبع من اي مصدر اخر مثل عضلات البطين نفسه و هذا قد يكون بسبب فشل العقدة الجيب اذينية في اصدار نبضات أو وجود مصدر خارجي - في اي مكان اخر في القلب - ينبض بمعدل اعلي من منظم ضربات القلب الاساسي فيأخذ مكانه.
- صور رسم القلب
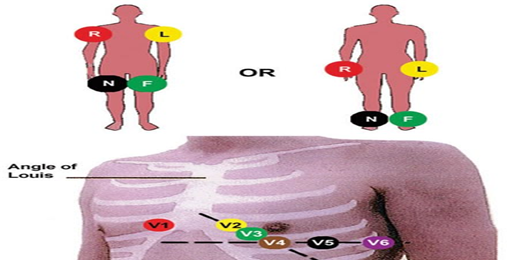
كل قطب كهربي موصل بالجسم يعتبر كاميرا و نقوم بوضع 10 اقطاب علي جسم الانسان واحد على كل
ذراع وكل ساق وعند ستّ نقاط على الصدر و بالتالي نحصل علي 10 أقطاب ( كاميرات ) من جهات مختلفة ، كل كاميرا تنتج لنا صورة مختلفة عن الكاميرا الاخري لان كل واحدة تلتقط منظر القلب من زاوية مختلفة و لكنه هو نفس المنظر ، مثل مباراة كرة القدم ، فنجد انه يوجد اكثر من كاميرا في الملعب و كل واحدة تلتقط منظرا معينا من زاوية معينة و لكن هي نفس المباراة .
و جهاز رسم القلب ينتج لنا 12 صورة :
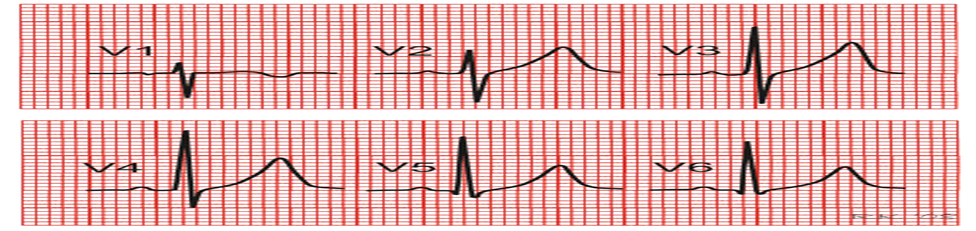
الستة أقطاب( كاميرات) التي علي الصدر تنتج لنا 6 صور مختلفة (leads) و تسمي V1,V2,V3,V4,V5,V6
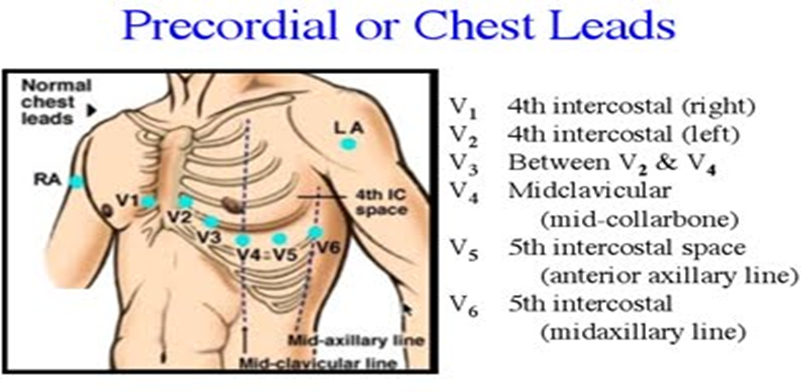
أماكن الأقطاب التي علي الصدر هي كالاتي :
{kind=link}
· V1: في المسافة رقم 4 التي بين الضلوع علي اليمين . 4th intercostal space Rt
V2: في المسافة رقم 4 التي بين الضلوع علي اليسار Lt.4 th intercostal space
· V3: في النقطة ما بين V2&V1
V4: عند قمة القلب APEX
V5: في نفس مستوي قمة القلب عند خط الابط الامامي anterioer axillary line
V6: في نفس مستوس قمة القلب عند خط الابط المنتصفmid-axillary line
أماكن الوصلات :
الأقطاب التي علي الاطراف فكل واحدة تنتج لنا صورة ماعدا التي عند الساق اليسري فهي فقط للتوصيل الارضي لا تتدخل في الرسم .
· اليد اليمني تسمي : aVR
· اليد اليسري :aVL
· القدم اليسري : aVF
أما الثلاثة صور المتبقية فهما عبارة عن اندماج كل صورتين من الصور الناتجة عن الاقطاب الموجودة عند الاطراف
اندماج الصورة :
• اليد اليمني مع اليد اليسري تنتج لنا صورة تسمي:( lead I).
• اليد اليمني مع القدم تسمي : ( lead II ) .
• اليد اليسري مع القدم تسمي: ( lead III ).
وبما ان هذه الصور اندماج لاكثر من صورة فهي بالتالي تكون مكبرة (augmented) ولكي تكون الصور الناتجة كلها متساوية يقوم الجهاز بتكبير الصور الاخري الصادرة من الآطراف
( aVR , aVL, aVF) .
• حيث أن الحرف(V) يعني كلمة (Vector) أي المتجه اليها الكاميرا (electrode).
• (a) هي (augmented) أي مكبرة كما أوضحنا.
• (R) هي (Right arm) .
• (L) هي (Left arm).
• (F ) هي (Foot).
الصور تكون مرتبة كالاتي ( من الشمال لليمين طبعا ):
• Lead I, lead II, lead III, aVR, aVL , aVF, V1,V2,V3,V4,V5,V6))-
شكل رسم القلب :
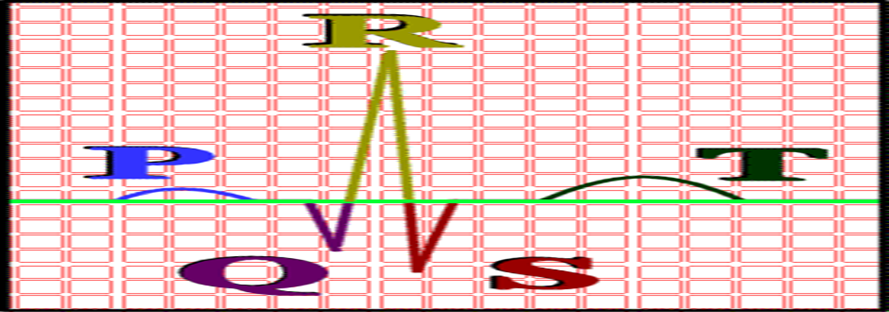
عضلات الاذينين أصغر من عضلات البطينين و لذلك فان التيار الكهربائي المصاحب لانقباض الاذينين سيكون صغيرا و يرمز له في رسم القلب برمز (الموجة ب) (P wave)،بينما انقباض البطينين يرمزله بالرمز (مجموعة كيو ار اس ) (QRS complex )، و بعدها يرمز لانبساط البطينين برمز ( الموجة ت) T wave ،حيث ان الدورة القلبية تبدأ بأنقباض الاذينين ثم انبساطهما ثم انقباض البطينين ثم انبساطهما ، و كل هذا يسجل كموجات في ورقة رسم القلب..
{kind=link}
• انقباض الاذينين (الموجة ب) (P wave) - ثم انبساطهما (-)و هنا لا يسجل انبساط الاذينين لانه يحدث في نفس وقت انقباض البطينين و بالتالي انقباض البطينين يعوق تسجيل انبساط الاذينين.
• انقباض البطينين (مجموعة كيو أر أس) (QRS complex) - ثم أنبساطهما (الموجة تT wave).
• بالنسبة الي مجموعة (كيو أر اس) فاول انحناء لاسفل الخط المستقيم يسمي (موجة كيو) (Qwave) و الانحناء الذي يليه الي اعلي يسمي (موجة أر) (R wave) وهو ممكن يكون مسبوق ب (موجة كيو) أو لا ،ثم يليه لاسفل انحناء اخر يسمي (موجة اس) (S wave) و هو أيضا ممكن يكون مسبوقا بموجة كيو أو لا ... أي انه ليس شرطا أن يمثل انقباض البطينين بـ (مجموعة كيو أر اس) كلها .
• و أي تغير في هذه الصور يكشف عن مشكلة قد تكون في معدل ضربات القلب او نتيجة أنسداد شريان او شيء اخر، و لكن الصور الاكثر استخداما و الاكثر وضوحا هي (lead II) و (avR) و يستخدم احداهما لمتابعة حالة المريض في وحدات العناية المركزة، و ان كان الأكثر أستخداما هو (lead II).
يوجد 10 أقطاب (كاميرات) - electrodes)) - توضع علي الصدر و الساقين و الاذرع .... ينتج عنهما 12 صورة (leads) وهما كالاتي :
• (Lead I, lead II, lead III, aVR, aVL , aVF, V1,V2,V3,V4,V5,V6)
قاعدة مهمة
• ان كان اتجاه التيار الكهربائي في القلب في نفس اتجاه القطب ( الكاميرا) الموجهه فيكون الناتج انحناء سالب (لاسفل) علي ورقة رسم القلب ، و العكس ان كان اتجاه التيار عكس اتجاه الكاميرا فيكون الناتج انحناء موجب (لأعلي) علي ورقة رسم القلب ، وان كان اتجاه التيار ليس له علاقة باتجاه الكاميرا فتكون الاشارة ( الانحناء) له أي شكل.
و لذلك نجد ان أغلب انحناءات (lead II) موجبة (لأعلي) لان القطب ( الكاميرا ) الموجهة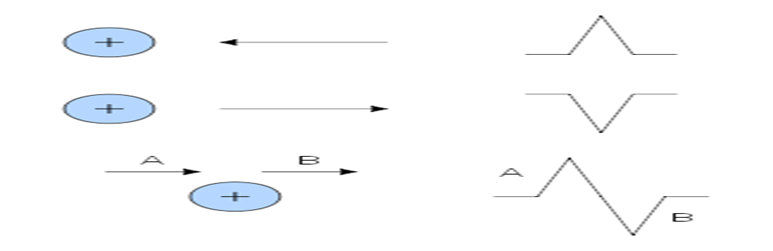
• تصور عكس اتجاه التيار ، أما أنحناءات (avR) فهي لاسفل لان الكاميرا الموجهه تصور في اتجاه التيار.
للقراءة رسم القلب يجب أتباع الأتى :
1. معدل ضربات القلب / الدقيقة.
2. ايقاع معدل ضربات القلب (منتظم أم لا).
3. أختلال محور القلب.
4. علامات وجود اقفار دموي ischemia.
5. الموجة ب (P wave ).
6. المسافة ب – أر P-R interval.
7. المجموعة كيو أر أس QRS complex.
8. الموجة ت T wave.
. الجزء أس – ت ST segment.
معدل ضربات القلب و إيقاعه :
• يلتقط جهاز رسم كهربائية القلب التيارات الكهربائية ويسجلها علي ورق رسم بياني ذات مربعات متساوية الحجم بمعدل منتظم حيث يحتوي ورق رسم القلب علي مربعات كبيرة وكل مربع كبير يحتوي علي 25 مربع صغير (5×5) و كل مربع صغير(1مم) يمثل 0.04 ثانية،وبالتالي كل مربع كبير( 5 مم) يمثل 0.2 ثانية اي أن 5 مربعات كبيرة تمثل (1ثانية) و 300 مربع كبير يمثل (1دقيقة) ومن ذلك
{kind=link}
• يمكن ان نحسب معدل نبض القلب في الدقيقة فمثلا اذا وجدنا دورة القلب كاملة تتكرر كل مربع كبير أي أن القلب ينبض بمعدل 300 دقة/الدقيقة و هكذا
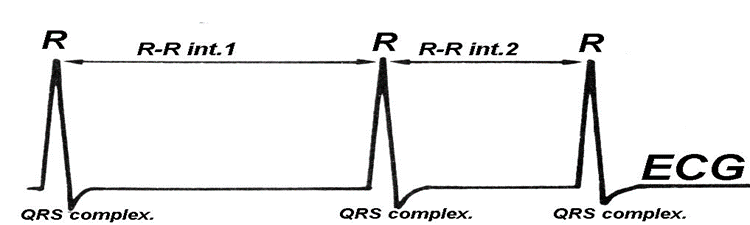
• قياس المسافة بين ( موجات أر ) ( R waves ) و بعضها _ علي أعتبار انها أعلي نقطة في الرسم _ تمثل معدل دقات القلب فالمسافة بين (أر_ أر) (intervalR- R) تمثل الوقت الذي أستغرق في توصيل التيارات الكهربائية خلال أجزاء القلب المختلفة
يمكن قياس معدل ضربات القلب كالاتي :
• معدل ضربات القلب =300 ( 300 مربع لحساب عدد دقات القلب في الدقيقة) ÷ المسافة بين ( أر- أر) ،و لكن هذا في حال ان يكون معدل ضربات القلب يسير بايقاع منتظم....
• وقياس الايقاع يتم عن طريق مطابقة المسافة بين (أر- أر) تكون متساوية في كل الصور،
في حالة ان الايقاع غير منتظم فسنحسب معدل ضربات القلب كالاتي :
• معدل ضربات القلب = عدد (موجات ار _R waves) .
• في خلال6 ثواني × 10 .
هذه العملية الحسابية تتم علي طول صور رسم القلب لمدة 6 ثواني.
الموجة بى ((P wave:
• الفترة : هي تمثل فترة انقباض الاذينين .
• المدة : تساوي 0.08_0.12 ثانية أي من (2-3 ) مربع صغير و في بعض الاوقات يقال عنها انها (2.5× 2.5 ) مربع صغير طول في عرض.
الحالات التي يمكن تشخيصها من الأختلافات التي تحدث في (P wave ):
1- كبر حجم الاذين الايمن : أسبابه أرتفاع الضغط الرئوي (Pulmonary hypertension)
و يتم تشخصيه من زيادة ارتفاع (طول) الموجة (ب) اكثر من 3 مم نتيجة زيادة فترة انقباض الاذين الايمن لكبر حجمه و لان من اشهر اسبابه ارتفاع الضغط الرئوي(Pulmonary hypertension) فسميت (P wave) بإسم (P-Palmonale).
2- كبر حجم الاذين الايسر : أسبابه ضيق الصمام المترالي (Mitral stenosis)
و يتم تشخصيه من زيادة عرض الموجة (ب) اكثر من (0.11 ثانية) نتيجة زيادة فترة انقباض الاذين الايسر لكبر حجمه و لان من اشهر أسبابه ضيق الصمام المترالي (Mitral stenosis) فسميت (P wave) بإسم (P-Mitral).
المسافة ب - أر (P-R interval) :
{kind=link}
• و هي تبدأ من بداية (الموجة ب) الي بداية (مجموعة كيو أر اس) أي من بداية لبداية و هي تمثل الوقت المستغرق لانتقال التيار الكهربائي من العقدة الجيب اذينية الي الاذينين و منه الي البطينين.
و هي تساوي = 0.12_ 0.20 ثانية أي من (3-5) مربعات صغيرة.
المجموعة كيو أر اس (QRS complex) :
• الفترة: تمثل الوقت المستغرق لانتقال التيار خلال البطينين.
• المدة: تساوي = 0.12 ثانية ( 3 مربعات صغيرة).
• التشخيص: كما ذكرنا فهي تساعد في تشخيص حالات الرجفان الاذيني و البطيني و الرفرفة الاذينية و انواع اضطرابات نظم القلب.
كما انها تساعد ايضا في تشخيص امراض الذبحة الصدرية و الجلطة كما سنوضح و امراض اخري للقلب.
• خط وهمي يرسم علي القلب يمثل محصلة التيار الكهربائي حيث ان اتجاه التيار الكهربائي في القلب يأتي من العقدة الجيب اذينية- كما اشارنا من قبل – الي أسفل وحيث ان البطين الايسر اكبر من البطين الايمن – لانه يغذي الجسم كله بالدم – فلذلك لو تخيلنا مسار التيار الكهربائي في القلب سيكون من اعلي الي أسفل و متجه ناحية اليسار قليلا....هذا ما يسمي بمحور القلب.
• أي تغييرات في هذا المحور تسمي اختلال محور القلب ناحية اليمين أو اليسار (Rt or Lt axial deviation)