Procedural Manual For Delivery Cases
| Site: | EHC | Egyptian Health Council |
| Course: | Evidence of nursing procedures for internal sections |
| Book: | Procedural Manual For Delivery Cases |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:55 AM |
Description
"last update: 20 April 2025" تحميل الدليل
- اعداد
دليل الأقسام الداخلية
تحت اشراف
- أ.د/ محمد لطيف الرئيس التنفيذي للمجلس الصحي المصري - د/ كوثر محمود نقيب عام التمريض المصري – عضو مجلس الشيوخ
اعداد
|
م |
الاسم |
الوظيفة |
|
1 |
أ. د /امل احمد خليل مرسي |
نائب رئيس الجامعة لشئون التعليم والطلاب – جامعة بورسعيد |
|
2 |
أ.د / عفاف عبد العزيز عبد العزيز بصل |
عميد كلية التمريض –استاذ تمريض باطنه وجراحي جامعة طنطا |
|
3 |
أ.د/ زينب حسين على محمد سعد |
وكيل الكلية لشئون البيئة وخدمة المجتمع – كلية التمريض – جامعه حلوان |
|
4 |
أ.د /امل سعيد طه رفاعي |
أستاذ ورئيس قسم التمريض الباطني الجراحي – جامعة بنها |
|
5 |
أ.د /حنان احمد السباعي على |
استاذ التمريض التمريض الباطني الجراحي- كلية التمريض – جامعة القاهرة |
|
6 |
د /نيفين عبدربه النبي محمد عبد النبي |
رئيس الإدارة المركزية ندباَ –وزاره الصحة |
|
7 |
د /مايسه حسني احمد تمام |
مدير عام للإدارة ندباَ – وزاره الصحة |
|
8 |
د نانسي علاء الدين عبد الباسط على |
المشرف على التعليم الفني- الهيئة العامة للرعاية الصحية |
|
9 |
د شيرين محمد محمد سعدالدين |
المشرف على تطوير الخدمات التمريضية –الهيئة العامة للرعاية الصحية |
|
10 |
د/ مى محمود العسال |
مدير عام الإدارة العامة لشئون المعاهد الفنية الصحية |
|
11 |
أ.م.د/ هبة محمود محمد |
أستاذ مساعد تمريض صحة الام وحديثي الولادة –كلية التمريض - جامعة عين شمس |
|
المشاركين |
||
|
12 |
/أنهلة كامل مصطفي |
مسئول التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
|
13 |
/أمها سعد محمد النادي |
عضو إدارة التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
|
14 |
/أثروت عبد العال محمد |
عضو إدارة التمريض بالهيئة العامة للرعاية الصحية فرع الإسماعيلية |
|
15 |
أ /منى على عبد الرحمن الكتامى |
أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
|
16 |
أ / شيرين عبد الحكيم عبد الحكيم خطاب |
أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
|
17 |
أ/بهاء فؤاد برسوم |
أخصائي تمريض بالإدارة العامة للتمريض- وزارة الصحة |
- Profession Oath
"I swear by Almighty God
That I will be sincere in my work, fear God in my profession, respect its laws
and regulations, and perform my duties with competence and dedication.
That I will rely in my work on the knowledge derived from the science of
nursing,
And I will exert my utmost effort in caring for those entrusted to my care,
preserve their dignity, maintain their confidentiality, defend their rights,
and protect them from any harm.
That I will not fear the blame of anyone when speaking the truth, and I will
provide a safe environment for the patient, family, and community.
That I will continue to develop myself, honor and respect those who have taught
me,
And collaborate with my colleagues in the profession for the sake of
righteousness and piety.
And I bear witness to what I say before God."
- Nursing Care Vision and Mission
Vision of Nursing Care in the Internal Patient Care Unit
The nursing staff members in the internal patient care unit aim to elevate the nursing profession and provide effective, safe, and high-quality nursing care to patients in the unit according to Egyptian, national, and global standards.
Mission of Nursing Care in the Internal Patient Care Unit
The nursing staff in the internal patient care unit is committed to enhancing the health level of patients and providing the best nursing care in alignment with the hospital’s goals, procedures, and nursing management. They also aim to enhance the scientific and practical levels of all nursing staff members in the unit and change their attitudes toward modern trends in nursing and medical sciences.
- Normal Delivery
- Normal Delivery: This is the birth of a healthy, fully developed baby after 37 weeks of pregnancy, in a head-down position, with the baby being delivered smoothly and easily through the vagina without interventions (except for an episiotomy) and without complications for the mother or the newborn within the first 24 hours from the onset of true uterine contractions.
Symptoms and Signs of Labor
- Initial Symptoms of Imminent Labor:
- Descent of the Fundus: By week 36, the fundus of the uterus reaches the rib cage, then it drops before labor to a level of 32-34 weeks, due to the head of the baby being engaged in the true pelvis. The mother will feel easier breathing and less pressure in the stomach, but she will experience symptoms of pressure on the lower part of the body, such as difficulty moving and pain in the back, abdomen, and thighs.
- Frequent Urination: This occurs because the baby's head presses on the bladder, reducing its capacity and requiring frequent emptying.
- False Labor Pains: These are irregular contractions that the mother feels in the lower abdomen but do not affect the dilation of the cervix.
- Shortened Cervix: This occurs due to uterine contractions (true labor pains)
|
Symptoms |
True Labor Pains |
False Labor Pain |
|
Pain |
Intense |
Mild |
|
Regularity |
Regular (occurs every 20-30 minutes, then every 10 minutes, reaching 3 contractions in 10 minutes) |
Irregular |
|
Increase in Pain and Intensity |
Increases (becomes more intense over time) |
Does not increase |
|
Response to Pain Relief |
Does not respond to pain relief |
Responds to pain relief |
Stages of Labor:
- First Stage: Begins with true uterine contractions and ends with full dilation of the cervix.
- Second Stage: Begins with full dilation of the cervix and ends with the birth of the baby.
- Third Stage: Begins after the baby is born and ends with the delivery of the placenta.
- Fourth Stage: Lasts for about two hours after the delivery of the placenta, involving post-birth monitoring.
|
Subsequent Pregnancies |
First Pregnancy |
Stages of Labor |
|
6 – 8 hours |
12 – 16 hours |
First Stage |
|
30 – 60 minutes |
1 – 2 hours |
Second Stage |
|
15 – 30 minutes |
15 – 30 minutes |
Third Stage |
|
2 hours |
2 hours |
Fourth Stage |
First Stage of Labor:
The first stage of labor begins with the onset of real labor pains and lasts until the cervix is fully dilated (10 cm).
- Real labor pains: These are uterine contractions that cause the cervix to dilate and help push the baby through the birth canal.
- Initially, contractions occur at long intervals (every 30 minutes), but the time between each contraction shortens as labor progresses. Contractions last around 45 seconds, starting mildly and increasing in intensity towards the end.
Nursing Care During the First Stage:
- Preparation of the delivery room.
- Assessment of the mother's condition:
- Taking a history of the pregnancy and previous births.
- Ask the mother about the onset and frequency of labor pains (regular, felt in the lower abdomen and back).
- Check for signs of early labor, such as the passage of mucus with blood (bloody show).
- Ask if the water has broken (amniotic sac rupture).
- Inquire about the mother's sleep, rest, and food intake in the last 6 hours.
- Assess for any pregnancy complications like preeclampsia, anemia, diabetes, etc.
- Physical examination:
- General assessment: Check vital signs, edema, blood pressure, and perform a urine test.
- Abdominal examination: Assess the shape, size, and any past surgeries or infections.
- Fetal heartbeat: Normal fetal heart rate is 120-160 beats per minute.
- Preparation for delivery:
- Ensure the mother is clean, bladder is empty, and she is resting.
- If the mother is in the early stages, she may have light drinks or glucose IV for hydration.
Second Stage of Labor:
The second stage begins when the cervix is fully dilated and ends with the birth of the baby.
- Signs of the second stage:
- Involuntary pushing or bearing down.
- Increase in the amount of bloody show.
- Rupture of the amniotic sac.
- Increased breathlessness.
- Appearance of the perineum and anus.
- Sweating on the neck, forehead, and face.
- The mother's urge to urinate or defecate.
- The baby’s head begins to show (crowning).
- Mechanics of labor: This involves the baby adjusting to the shape of the pelvis and birth canal. The steps include:
- The baby descending into the pelvis.
- Flexion and rotation of the baby’s head.
- Delivery of the head, followed by the rest of the body.
- Nursing care during the second stage:
- Help the mother into the delivery room, change into a gown.
- Prepare the delivery room and help the mother get into a comfortable position, usually on her back with legs in stirrups.
- Evaluation: Monitor the baby’s heart rate every 5 minutes between contractions, check the mother’s pulse, observe the amniotic fluid color, empty the bladder, and assist with breathing exercises.
- Preventing perineal tears:
- Support the perineum during contractions to prevent tearing.
- Guide the mother to breathe and not push too hard during crowning.
- Check for umbilical cord entanglement around the baby’s neck.
Third Stage of Labor:
This stage begins after the baby’s birth and ends with the delivery of the placenta.
- Signs of placenta detachment:
- Uterus becomes firm and easily movable.
- The top of the uterus rises and bulges due to the placenta.
- A sudden gush of blood when the placenta detaches.
- The umbilical cord lengthens.
- Nursing care during the third stage:
- Administer oxytocin or methylergonovine as per the doctor’s instructions.
- Monitor for signs of placenta separation.
- Gently pull the umbilical cord while massaging the uterus to help deliver the placenta.
- Inspect the placenta to ensure complete delivery.
- Monitor uterine tone, check for any vaginal tears, and apply antiseptic to the genital area.
Fourth Stage of Labor:
This stage lasts for two hours after the placenta is delivered and is critical for monitoring postpartum bleeding.
- Nursing care during the fourth stage:
- Monitor vital signs every 15 minutes during the first hour and every 30 minutes during the second hour.
- Perform uterine massage to prevent hemorrhage.
- Monitor for vaginal bleeding every 10 minutes.
- Encourage the mother to void regularly (full bladder can hinder uterine contractions).
- Ensure the mother rests, maintains hygiene, and begins breastfeeding to encourage uterine contractions.
- Monitoring complications:
- For the mother: Excessive bleeding (more than 500 mL), difficulty urinating, seizures, or pain in the genital area.
- For the baby: Difficulty breathing, weak pulse, or low birth weight.
- Neonatal Resuscitation
- Introduction: Most newborns transition smoothly from the womb to life outside, but some may need resuscitation within the first minute, known as the "golden minute."
- Initial assessment: The need for resuscitation depends on:
- Full-term pregnancy or not.
- Presence of good muscle tone.
- Breathing or crying.
- If the answer is yes to all questions, provide routine care: drying, skin-to-skin contact with the mother, and continuous monitoring of the baby's color, breathing, and activity.
- If no to any question, follow these steps in order:
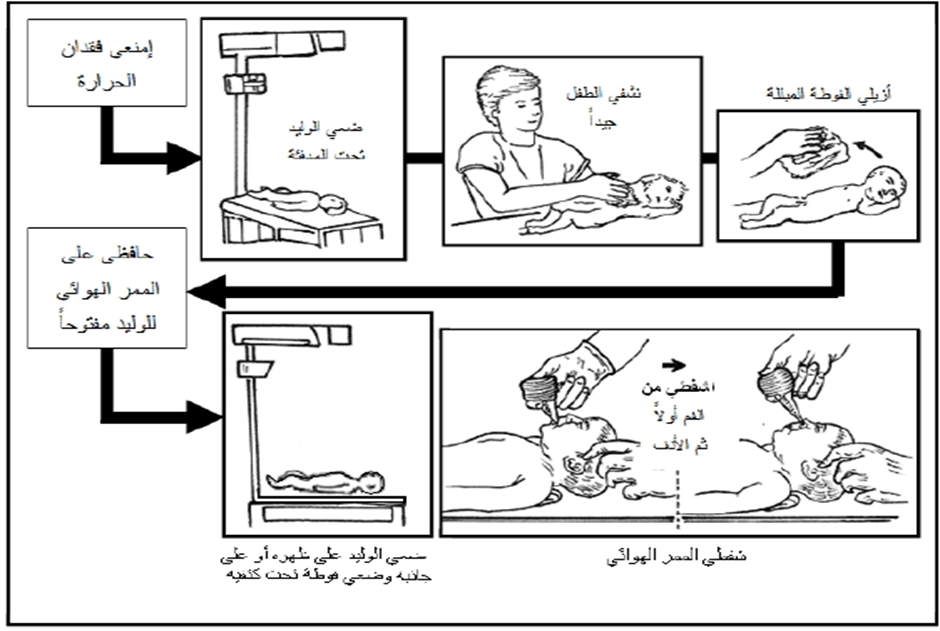
- Stabilization: Provide warmth, clear airways, dry, and stimulate the baby.
- Oxygen administration.
- Chest compressions if heart rate is below 60 bpm.
- Administer medications like adrenaline if necessary.
- Cord clamping: Delayed cord clamping is recommended for at least 30 seconds for full-term or preterm babies not requiring resuscitation.
Assessment
- The newborn's condition is assessed based on three parameters: heart rate, effort in breathing, and color.
- An elevated heart rate during recovery is considered the most important indicator of successful recovery. Continuous monitoring of heart rate is crucial during the recovery process as it is also used to assess the respiratory system and determine the need for further interventions. The assessment is done by attaching three electrodes connected to a heart monitor to track the pulse, as this method is more accurate than manually counting the pulse. Breathing effort is assessed by checking if there is any apnea (cessation of breathing). The newborn’s color is checked for signs of cyanosis (blueness).
Continuing Recovery Steps
· If there is no apnea, and the heart rate is over 100 beats per minute, but the newborn has difficulty breathing or exhibits central cyanosis, the following steps are taken:
- Adjusting the position, clearing the airway, and monitoring the oxygen saturation (SpO2).
- Administering supplemental oxygen as per the doctor's orders and possibly using CPAP if necessary.
- If there is improvement, post-recovery care is initiated. If there is no improvement or if the heart rate falls below 100 beats per minute, ventilation using an ambu-bag is carried out.
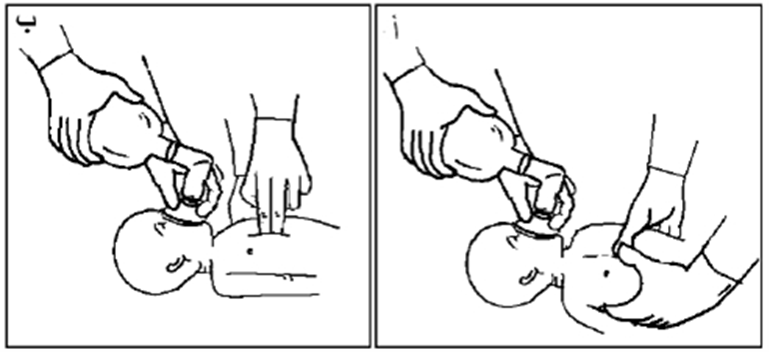
· If apnea is present and the heart rate is below 100 beats per minute, ventilation is performed using an ambu-bag and mask, while monitoring the pulse and oxygen saturation (SpO2), as follows:
- Ensure the newborn’s head is in the proper sniffing position, placing a towel under their shoulders if needed, and confirming that the airways are clear of secretions.
- A properly-sized mask is placed on the newborn's face, covering the chin, mouth, and nose but not the eyes. Ventilation is done using the (breath – 2 – 3) system, ensuring the appropriate pressure is applied.
- The rise of the chest during ventilation should be monitored, adjusting the pressure based on the chest rise. Endotracheal intubation may be performed if necessary.
· The heart rate is assessed, and if improvement occurs, post-recovery care is initiated. If no improvement is observed despite effective ventilation, and the heart rate remains below 100 beats per minute, ventilation with the ambu-bag and mask continues. If the heart rate drops below 60 beats per minute, intubation is performed (if not done already), and chest compressions are immediately started, along with continued ventilation, as follows:
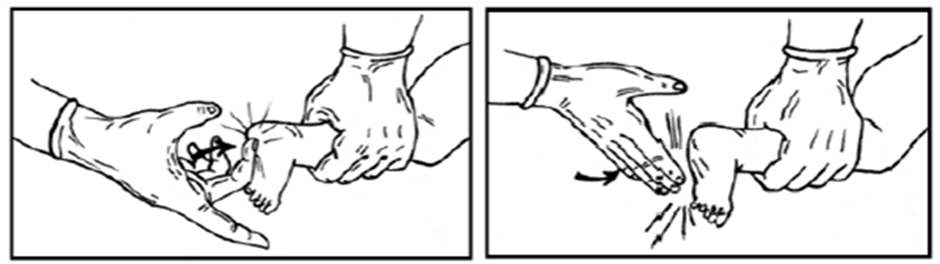
- Place the thumbs on the lower third of the sternum, with the hands wrapped around the newborn's chest, and the fingers meeting behind the newborn’s back. Alternatively, place the middle and index fingers of one hand on the lower third of the sternum, with the other hand supporting the newborn’s back. Apply pressure to the chest, compressing about one-third of the distance to the spine.
- Chest compressions are coordinated with ventilation using the (compress – 2 – 3 – breath) system, which lasts about two seconds per cycle, totaling 120 cycles per minute (90 compressions and 30 breaths per minute).
- This system is used if respiratory compromise is the main issue. If cardiac issues are the primary cause, the higher-pressure system (15 compressions: 2 breaths) is used.
· If the heart rate remains below 60 beats per minute, an umbilical catheter is inserted, adrenaline is administered intravenously, and fluid deficits are corrected, while also preventing the risk of pneumothorax (air in the chest cavity).
These guidelines focus on providing proper care for newborns during the recovery phase, ensuring their heart rate and breathing are closely monitored and supported as needed, with appropriate interventions like ventilation and chest compressions.
Fifth: Administering Medications
- If the heart rate remains below 60 beats per minute, an umbilical catheter is inserted by the pediatrician, and diluted adrenaline is administered intravenously (dosage as per the doctor's instructions). Fluid deficits are corrected by giving volume expanders as per the doctor's instructions (such as 0.9% saline solution or Ringer's lactate solution).
Note: If the newborn requires prolonged ventilation using an ambu-bag, a nasogastric tube (Ryle's tube) should be placed to remove stomach distension, preventing pressure on the diaphragm, which could hinder the full expansion of the lungs.
Ending the Recovery Process
- Recovery efforts are stopped if the newborn does not breathe or has no pulse 15 minutes after full recovery efforts. In such cases, psychological support is provided to the mother and family.
- If the newborn responds to recovery efforts, they must remain under a heating device for monitoring until their condition stabilizes.
- The newborn may be transferred to the neonatal care unit for further required care if necessary, with continuous monitoring of vital signs and any abnormal signs such as (apnea, increased respiratory effort, central cyanosis). The doctor should be informed immediately.
Routine Care for the Newborn After Stabilizing Vital Signs
- Care for the umbilical cord
- Administer Vitamin K
- Apply antiseptic eye drops
- Ensure temperature stability of the newborn
- Initiate breastfeeding
- Foster mother-infant bonding immediately after birth
- Encourage skin-to-skin contact between mother and newborn
- Establish newborn identity
- Weigh the newborn
After Completing the Recovery Process
- Dispose of any tools used for the newborn in their designated place.
- Clean and disinfect the heating device.
- Disinfect the ambu-bag, masks, and laryngoscope blade.
- Record the duration of recovery and document all actions taken for resuscitation in the mother’s or newborn’s medical record, in case the newborn is admitted to the unit.
- Replace used items in the recovery kit when arriving at the neonatal care unit.
This outlines the complete procedure for neonatal resuscitation, administration of necessary medications, post-recovery care, and the hygienic processes to follow after resuscitation efforts.
- Abnormal Birth
Abnormal birth refers to various conditions that affect the natural course of labor. Among these is difficult labor (dystocia), which requires medical intervention. If left untreated, it can lead to complications such as uterine rupture or fetal death.
Difficult Labor
Difficult labor is one that cannot proceed naturally and requires external intervention. If neglected, it can lead to complications like uterine rupture or fetal death.
Symptoms and Signs of Difficult Labor:
Symptoms in the mother:
- Severe pain.
- Fever (above 38°C).
- Increased heart rate (over 120 beats per minute).
- Presence of acetone in urine.
- Signs of exhaustion (such as facial congestion, color changes, and severe dry lips).
- Swelling of the genital area and vaginal dryness.
Symptoms in the fetus:
- Increased heart rate above 160 beats per minute or decreased below 120.
- Cessation of fetal movement.
- Presence of meconium in the amniotic fluid in the case of vertex presentation.
- Slippage of the skull bones.
Causes of Difficult Labor:
- Abnormal fetal position and presentation: Such as breech or transverse presentation.
- Narrow or deformed pelvis: Can hinder the passage of the baby through the birth canal.
- Abnormal uterine contractions: Can be excessively strong or weak, hindering labor progress.
Early Rupture of Membranes
Early rupture of membranes (amniotic sac tear) can occur before labor begins. This may lead to serious complications like preterm birth or fetal injury.
Symptoms of Early Membrane Rupture:
- Unusual flow of amniotic fluid.
- Continuous leakage of fluid when walking, standing, or straining.
- Presence of meconium in the amniotic fluid.
- Fever in the mother if there is an infection.
Nursing Care:
- Monitor the mother's temperature and fetal heart rate.
- Maintain cleanliness and avoid frequent vaginal examinations.
- Administer medication as per the doctor’s instructions.
Twin Pregnancy
Twin pregnancy occurs when the mother carries more than one fetus. It can be either a monozygotic (identical) or dizygotic (fraternal) pregnancy. Twin pregnancies are associated with complications such as hypertension or preterm birth.
Nursing Care for Twin Pregnancy:
- Delivery should take place in a hospital.
- Support the mother in increasing iron and calcium intake.
- Encourage a healthy diet and continuous monitoring.
Perineal Tears
Perineal tears may occur during delivery, where the skin or muscles of the perineum are damaged as the baby's head passes through.
Types of Perineal Tears:
- First-degree tears: Involve the skin only.
- Second-degree tears: Involve the skin and muscles of the perineum.
- Third-degree tears: Involve the skin, muscles, and the anal sphincter.
- Fourth-degree tears: Involve the skin, muscles, anal sphincter, and rectal wall, creating a single cavity between the vagina and rectum.
Causes of Perineal Tears:
- Lack of perineal flexibility.
- Large fetal head.
- Allowing the head to stretch before crowning.
- Narrow pelvic arch.
- Rapid delivery during uterine contractions.
- Use of forceps during delivery.
- Uterine Rupture
Uterine rupture can occur in the later stages of pregnancy or during a difficult delivery if not addressed immediately.
Causes of Uterine Rupture:
- Use of uterine stimulants without proper monitoring.
- Pressure on the uterus or abdomen during delivery.
- Multiple previous pregnancies (more than five).
- Mismatch between fetal head size and pelvic size.
- Abnormal fetal position, such as a posterior vertex.
- Uterine tumors or fibroids blocking the baby’s descent.
- Birth defects or twin pregnancies.
Signs of Impending Uterine Rupture:
- Severe lower abdominal pain due to strong, continuous uterine contractions.
- Mild vaginal bleeding.
- Difficulty distinguishing fetal parts due to the tight contraction of the uterus.
Signs of Actual Uterine Rupture:
- Sudden and intense abdominal pain, followed by cessation of uterine contractions.
- Shock symptoms due to bleeding.
- Fetal parts may be palpable upon abdominal examination.
- Vaginal bleeding, and the cervix may be dilated with visible uterine rupture.
Nursing Care for Uterine Rupture:
- Nurses play an essential role in identifying warning signs and preventing uterine rupture.
- In case of rupture, two IV cannulas should be inserted, fluids should be administered, and blood transfusions should be prepared.
- Emergency management should be carried out, and the patient should be prepared for exploratory surgery as per medical instructions.
- Cesarean Section
A cesarean section is the delivery of the baby through an incision in the abdomen and uterus after 28 weeks of pregnancy.
Indications for Cesarean Section:
- Abnormal birth presentation.
- Inability of the fetus to pass through the birth canal (disproportionate fetal head and maternal pelvis).
- Maternal health conditions like preeclampsia or diabetes.
- Active herpes infection in the mother, which could pose a risk to the baby.
- Previous cesarean section or uterine surgery.
- Fetal complications, such as cord prolapse or abnormal position.
Risks of Cesarean Section:
- Maternal risks: Anesthesia complications, respiratory problems, bleeding, blood clots, injury to the urinary system, bowel injury, and infection.
- Fetal risks: Prematurity complications, respiratory issues, and superficial injuries.
Preoperative Nursing Care for Cesarean Section:
- Complete patient assessment on admission (e.g., maternal history, current pregnancy details).
- Electronic fetal heart monitoring for 20-30 seconds.
- Explain the surgical process to the mother and her support person.
- NPO (nothing by mouth) for 4-6 hours before surgery.
- Obtain necessary blood tests and prepare the skin for surgery.
- Establish IV access and urinary catheter insertion, if needed.
- Administer preoperative medications according to the doctor’s orders.
- Monitor fetal heart rate if active labor is occurring.
Postoperative Nursing Care for Cesarean Section:
- Ensure the airways are clear.
- Monitor vital signs frequently (every 15 minutes for the first 2 hours, then every 30 minutes for the next 2 hours, then every hour for 4 hours).
- Administer fluids and medications as ordered by the doctor.
- Assess the patient's level of consciousness, skin color, and hydration.
- Inspect the surgical site for any abnormal discharge or infection.
- Encourage early ambulation (within 6 hours after surgery).
- Provide pain management and support.
- Assist with breastfeeding, and provide guidance on newborn care.
Postpartum and Newborn Care
Nursing care for mothers after birth (postpartum) is essential to ensure recovery and support for the newborn.
Importance of Postpartum Nursing Care:
- To ensure the safety and well-being of both mother and newborn.
- To prevent complications like hemorrhage and infection.
- To provide emotional support to the mother and family in adjusting to the new baby.
Changes During Postpartum:
- Temperature: A slight increase within the first 24 hours, but it should not exceed 38°C.
- Pulse: Decreases in the first two days, then returns to normal after day three.
- Urine Output: Increases in the first five days due to excess fluid loss.
- Skin: Sweating increases, and skin changes like melasma fade.
- Bowel Movements: Constipation may occur due to relaxed intestinal muscles and fluid loss.
Psychological Needs of Postpartum Mothers:
- Emotional and physical adjustment to new responsibilities, including caring for the newborn.
- Providing guidance on self-care, infant care, and family adjustment.
Simple postpartum discomforts include abdominal pain, hemorrhoids, urinary retention, delayed uterine involution, constipation, and sore nipples.
Nursing care should address both physical and emotional needs, ensure proper wound healing, and prevent complications during the postpartum period.
|
Mother Warning Signs |
Newborn Warning Signs |
|
Abnormal vaginal bleeding |
Convulsions or persistent sleepiness |
|
Severe headache, blurred vision, severe abdominal pain, or seizures |
Refusal to breastfeed or weak sucking |
|
Fever or lochia with a foul odor |
Failure to pass stool within 48 hours after birth |
|
Pain in the calf muscle |
Severe diarrhea or vomiting |
|
Delayed or slow descent of the uterine fundus |
High or low body temperature |
|
Severe pain upon palpation of the uterus |
Yellowing of the eyes (jaundice) |
|
Chest pain or difficulty breathing |
Bleeding or purulent discharge with a foul odor from the umbilical cord |
|
Breast inflammation or abscess |
Rapid or difficult breathing |
|
Fainting |
Central cyanosis (bluish color of the body) or muscle flaccidity |
|
|
Continuous, severe crying |
|
|
Eye inflammation or swelling |
|
|
Failure to urinate within 24 hours after birth |
Role of the Nurse in Postpartum Care
The nurse's role in caring for the postpartum woman (nifas) involves following the nursing process to assess the health of both the mother and the newborn in order to identify their needs and problems. The following steps should be taken:
- Collecting a Comprehensive Health History:
- Take a thorough health history of the mother, especially regarding her recent birth history.
- General Physical Examination: The nurse should conduct a comprehensive examination that includes the following:
- Skin: Inspect the skin for color and condition (paleness, jaundice, dryness, excessive sweating).
- Observation for Fatigue: Look for signs of fatigue, loss of appetite, or dehydration.
- Vital Signs: Measure vital signs such as temperature, pulse, respiration, and blood pressure.
- Eyes and Tongue: Check for signs of anemia.
- Extremities: Examine for signs of thrombophlebitis (inflammation of veins and blood clot formation).
- Breast Examination: Assess the size, abnormal changes, nipple type, discharge, and any signs of infection.
- Abdominal Examination: Check the level of the uterine fundus, its firmness, shape, and position.
- Perineal Examination: Observe the perineum every 15 minutes after delivery to detect any signs of bleeding or hematoma formation.
- Lochia Examination: Assess the amount, color, odor, and composition of the lochia (postpartum discharge). It is normal for lochia to be blood-tinged for the first 4 days, then the color lightens and the amount decreases, turning into yellowish mucus after about 10 days. This should continue for 3-4 weeks.
This assessment is crucial to identify any complications early and ensure proper care for both the mother and her newborn.
|
Importance |
Abnormal Changes in Lochia |
|
||
|
Retained parts of the placenta |
Heavy |
Quantity |
||
|
Puerperal fever |
Low with high fever |
|
||
|
Risk of hemorrhage |
Persistent bright red |
Color |
||
|
Delay in the uterus returning to pre-pregnancy size |
Brown and heavy (Enlarged uterus) |
|
||
|
Retained parts of the membranes and placenta |
Foul |
Smell |
||
|
Puerperal fever |
Foul with high fever. |
|
Immediate Nursing Care After Delivery (First Two Hours Post-Delivery)
• Follow infection control procedures for all nursing interventions. • Position the patient in a comfortable position with warmth (Avoid placing her in the supine position to prevent posterior tilting of the uterus. It is preferable to place her in a semi-sitting position as it helps with the drainage of lochia). • Observation and documentation of:
- Vital signs
- Amount of blood lost
- Uterine tone (firm or relaxed)
- Condition of the perineum (tears, swelling, redness, bleeding)
- Height of the uterine fundus (gentle uterine massage every 15 minutes)
- Bladder condition
- Proper nutrition and increased fluids
- Encouraging breastfeeding
- Encouraging early movement • Administer vitamin A capsules immediately after delivery and iron tablets.
- Shock
Types of shock include:
- Hypovolemic shock due to blood or fluid loss.
- Septic shock from infection.
- Neurogenic shock (e.g., from trauma or anesthesia).
- Cardiogenic shock.
- Anaphylactic shock due to medication reactions.
Symptoms of Shock:
- Pale skin, low blood pressure, rapid pulse, sweating, cold extremities, and possibly loss of consciousness.
Nursing Care for Shock:
- Immediate physician notification and initial resuscitation measures, such as airway management, IV access, and blood transfusions.
- Continuous monitoring of vital signs and fluid balance.
Puerperal Fever: Puerperal fever is a fever above 38.5°C that persists for more than two consecutive days following delivery, often caused by infections in the reproductive tract.
Symptoms and Causes of Puerperal Fever:
- Fever above 38.5°C, chills, fatigue, and tachycardia.
- Possible uterine infection, pelvic infection, or sepsis.
Prevention of Puerperal Fever:
- Early detection and treatment of infections during pregnancy.
- Ensuring proper hygiene during labor and postpartum care.
- Monitoring the patient for signs of infection, and isolating affected individuals to prevent transmission.
Nursing Care for Puerperal Fever:
- Monitor vital signs, especially temperature and heart rate.
- Ensure proper hygiene and provide comfort measures.
- Administer antibiotics as prescribed and monitor their effectiveness.
Deep Vein Thrombosis (DVT) and Pulmonary Embolism: Thrombosis in the lower limbs can occur during the postpartum period, leading to potential complications like pulmonary embolism.
Nursing Care for DVT:
- Encourage early movement after delivery and monitor for signs of deep vein thrombosis (pain, swelling, redness).
- Administer prescribed medications and provide support for mobility.
- Monitor for complications like embolism.
Breast Engorgement and Mastitis: Mastitis is an infection of the breast, often associated with breastfeeding, causing pain, swelling, and fever.
Nursing Care for Mastitis:
- Encourage continued breastfeeding, even from the affected breast.
- Use warm compresses for relief, administer prescribed antibiotics, and support the mother through any necessary procedures for abscess drainage.
- Postpartum Complications
Types of Postpartum Bleeding: There are two main types of postpartum bleeding:
- Early Bleeding: Occurs within the first 24 hours after delivery.
- Late Bleeding: Occurs after 24 hours and up to 6 weeks post-delivery. Early bleeding is more common than late bleeding and is more often associated with hemorrhagic conditions.
Symptoms of Postpartum Hemorrhage: Some common signs of postpartum bleeding include:
- Severe, uncontrollable bleeding
- Low blood pressure
- Increased heart rate
- Swelling and pain in the vagina
Causes and Risk Factors of Postpartum Hemorrhage:
- Causes of Early Bleeding:
- Failure of uterine contraction, which may be a secondary issue from an overly enlarged uterus.
- Following multiple pregnancies, large baby, excessive amniotic fluid, prolonged labor, use of uterine relaxants, or infection of amniotic fluid.
- Tears in the birth canal, often caused by vacuum or forceps-assisted delivery, large baby size, or rapid labor.
- Retained placenta may hinder uterine contraction, leading to bleeding.
- Causes of Late Bleeding:
- Infection of the uterus.
- Uterine atony.
- Retained placenta.
- Blood clotting disorders.
Risk Factors:
- Placental separation, retained placenta, placenta previa, rapid labor, multiple gestations, vaginal trauma, obesity, and large baby size (greater than 4 kg).
Complications of Postpartum Bleeding:
- Infertility
- Uterine perforation
- Urinary tract injury
- Pelvic hematoma
- Sepsis
- Maternal death
Diagnosis of Postpartum Bleeding: Bleeding can be difficult to diagnose due to reliance on subjective assessment of blood loss. Additional methods, such as:
- Hemoglobin and hematocrit tests
- Blood transfusion needs May be used to determine the extent of blood loss.
Treatment of Postpartum Bleeding: Successful treatment involves identifying the underlying cause and preventing further complications:
- Manual uterine massage
- Use of uterotonic medications like Oxytocin immediately post-delivery.
- Surgical intervention may be required for uterine rupture or retained placenta.
Nursing Care for Postpartum Bleeding:
- Initial Resuscitation:
- Insert large-bore IV catheters and perform necessary blood tests.
- Administer IV fluids as directed by the physician.
- Monitor vital signs and keep track of fluid input and output.
- Monitor uterine tone and massage the uterus as needed.
- Observation:
- Assess vital signs every 30 minutes.
- Monitor lochia for volume and consistency.
- Watch for signs of shock and bleeding.
- Laboratory Tests:
- Blood type and Rh factor
- Complete blood count (CBC)
- Coagulation studies
- Nursing Interventions:
- For uterine atony: Manual uterine massage, use of uterotonic drugs, and breastfeeding to stimulate uterine contractions.
- For retained placenta: Manual removal or surgical intervention as per doctor’s orders.
- For vaginal or cervical tears: Assess and prepare for repair as needed.
- If infection is suspected: Administer antibiotics and follow infection control procedures.
- References
· WHO Recommendations for Augmentation of Labour: https://www.ncbi.nlm.nih.gov/books/NBK258884/
· Normal Labor and Delivery: Practice Essentials, Definition, Stages of Labor and Epidemiology: https://www.medscape.com/article/260036-overview
· Management of Normal Labor: https://www.msdmanuals.com/professional/gynecology-and-obstetrics/labor-and-delivery/management-of-
· Normal labor and delivery: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3611131/
· National Institutes of Health (NIH): Labor and Delivery: https://www.nichd.nih.gov/health/topics/labor-delivery
· Mayo Clinic: Labor and Delivery
· Healthline: Labor and Delivery: https://www.healthline.com/health/pregnancy/labor-and-delivery