Equine fluid therapy
| Site: | EHC | Egyptian Health Council |
| Course: | Equine Medicine Guidelines |
| Book: | Equine fluid therapy |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:55 AM |
Description
"last update: 5 Feb. 2025" Download Guideline
Table of contents
- - Scope
- - The Target audience
- - Introduction
- - Basics of Body Fluid
- - The roles of fluid therapy
- - Indications
- - Dehydration
- - Degree of dehydration
- -Acid-base disturbances
- - Hypovolemic and cardiogenic shock and Vasodilatory shock
- - Types of fluid
- - Principles of Rehydration
- - Signs of fluid overload
- - Administration routes
- - Fluid’s calculation
- - References
- Scope
This guideline outlines the frequent inoculation of fluid therapy in the treatment of many conditions in horses with diagnoses of equine dehydration and the physiological principles that underly the use of fluids types, volumes and routes of administration for rehydration to become an effective treatment , it is important that the proposed strategies are incorporated into routine protocols and staff training.
- The Target audience
The guideline is intended for all veterinarians who are responsible for dealing with equine population as well as who’s responsible for veterinary clinics and equine farms owners.
- Introduction
Fluid therapy is a key component in treatment and supportive care of horses with a variety of conditions, especially those with critical illness. fluids are drugs and, as such, have the potential for both life-saving benefits and serious, possibly life –threating, adverse effects in order to better align their utilization with their characterization as drugs. Water balance in the horse physiologic response to feeding and water loss or deprivation, and methods used to correct dehydration. Under normal environmental conditions horses tend to consume around 50 ml/kg/day of free water. This represents around 25 liters a day for a 500 kg animal. This value varies with environmental temperature and humidity, physical exercise, and diet. Water is an important component of the fermentation process in the large intestine and horses on hay diets will consume more water than those on meal-based diets. The intestinal tract receives fluid in the form of saliva, and gastric, pancreatic and biliary secretions. This may be around 125 - 150 liters daily in a 500 kg animal. This includes 30 - 50litres of pancreatic fluid, 12 - 25 liters per day of biliary fluid, around 50 liters per day of saliva, and a variable amount of gastric secretions.The process of hind gut digestion is dependent on large water and electrolyte fluxes in the caecum and large colon. Hind gut digestion in equids is superior to rumen digestion for dealing with high fiber plant material, provided that food intake and the rate of digesta passage are not limited through feed availability.These large intestinal fluid fluxes are maximized by meal feeding. Episodic feeding promotes movement of fluid and sodium into the intestinal tract causing a transient reduction (10-13%) in plasma volume leading to renin and angiotensin II release. Aldosterone release follows to promote post-prandial retention of sodium at renal, colonic, and other target epithelia, in exchange for potassium or hydrogen ions. Aldosterone causes a reduction in urine volume and decrease in plasma protein.
- Basics of Body Fluid
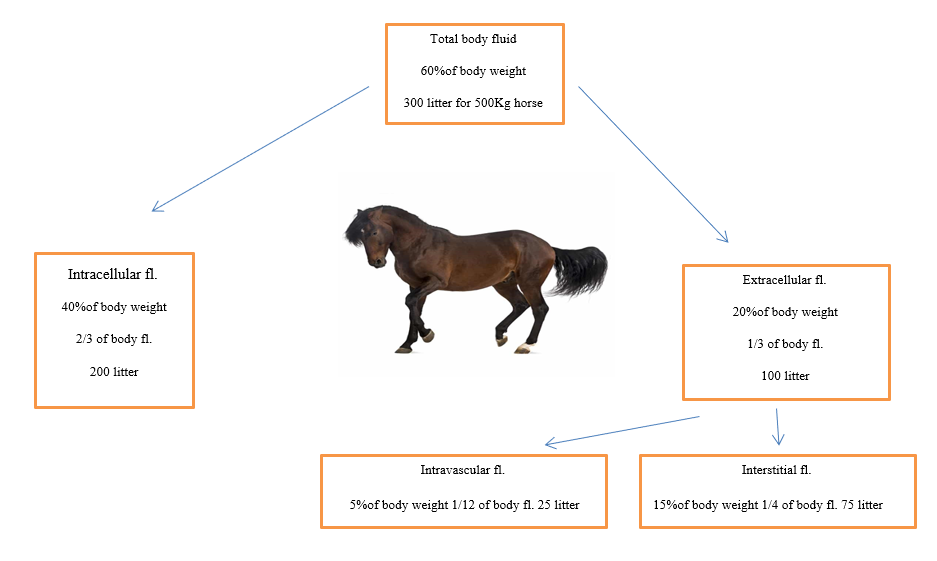
- An adult horse contains about 60% fluid of its body weight.
- Intracellular fluid (ICF)
which include (Ca, Mg, K, PO4 and protein) consists of about 2/3 of total body fluids.
- The extracellular fluids (ECF)
which include (Na, Cl and Hco3) consist of about 1/3 of the total body fluids. It is divided into three sub compartments interstitial, intravascular, and transcellular.
a- The interstitial contains 3/4 of all the fluid in the extracellular space.
b- The intravascular contains1/12 of body fluid, the fluid mostly plasma, that is within the blood vessels 5% of body weight .
- The fluid in the transcellular compartment is produced by specialized cells responsible for cerebrospinal fluid, gastrointestinal fluid, bile, glandular secretions, respiratory sections, and synovial fluids.
- Daily water intake is about 10% of the body weight (can vary from animal to animal with respect of their age, environment, feed intake etc.).
- Daily water loss equals daily intake and this loss occurs through the skin, lung, kidney and gastrointestinal tract.
- Body water contains solutes (substances that dissolve in solvent).
- Electrolytes are substances that split into ions when placed in water.
- Primary ions in the body are sodium, potassium, chloride, phosphate, and bicarbonate.
- Cations are positively charged ions.
- Anions are negatively charged ions.
- The roles of fluid therapy
1- Replacement therapy: Therapy in which we infuse same type of fluid which is lost from body.
2- Adjunctive Therapy: One type of fluid is given to remove other type of fluid e.g., mannitol 25% is given in case of ascites and edema.
3- Supportive Therapy: Fluid is given to animal just to support him to cure quickly i.e., amino acids, minerals, multivitamins and carbohydrates etc.
- Indications
Fluid therapy is used, firstly, to restore the circulating volume and improve cardiac output –which will, in turn, increase oxygen delivery to the tissues – and, secondly, to correct any electrolyte and acid-base disturbances. That is means:
1- To correct electrolyte imbalance, promote kidney diuresis, and maintain the tissue or organ perfusion.
2- During shock(except in cardiac shock).
3- Dehydration.
4- Diuresis (Toxicities, renal diseases).
5- After surgical procedure i.e., to prevent hypotension as hypotension may be due to vasodilation, decreased cardiovascular function etc.
6- Acid base imbalance.
7- Electrolyte imbalance.
- Dehydration
- Its meaning the loss of fluid in the form of increased fluid loss from excessive sweating, diarrhea, polyuria are the main causes of fluid reduction in equine in addition to the lack of water intake due to esophageal obstruction, toxemia and water deprivation.
- The signs include decreased skin tenting, sunken eyes, depressed mentation, and tacky/dry mucous membranes, capillary refilling time CRT 2-3 sec in mild cases and >3 sec in severe cases, Slight depression of eyes into sockets.
Diagnosis of Dehydration
• Physical exam
• Weight loss.
• PCV (HCT) increased
• Albumin or total protein increased
• BUN and creatinine are increasing (Prerenal azotemia).
- Degree of dehydration
Degree of dehydration (%) |
Clinical signs |
|
<5 |
Not clinically detectable. |
|
5<6 |
Subtle-loss of skin elasticity. |
|
6-9 |
Obvious delay in return of tented skin. Slightly ↑ CRT. Possible sunken & dry mucous membrane of eye. |
|
10<12 |
Skin remains tented. Very prolonged CRT. Sunken eyes & dry mucous membranes. Possibly signs of shock) tachycardia, cool extremities, rapid & weak pulse). |
|
12-15 |
Obvious signs of shock. Death imminent. |
-Acid-base disturbances
- The most-common acid base disturbance in the adult horse is metabolic acidosis due to poor Perfusion, resulting in anaerobic respiration and lactate production. This occurs most frequently in conjunction with hypovolemia and endotoxemia, and should be treated with fluid resuscitation using polyionic fluids. Metabolic acidosis can also occur secondary to hyponatremia – for example, in association with colitis, peritonitis or GI torsion – and should be treated with normal or hypertonic saline.
- Metabolic alkalosis occurs in association with hypochloremia – secondary to high volume gastric reflux, which should be treated with normal saline, and hypoalbuminemia, which should be treated with colloids.
- Respiratory acidosis occurs in conjunction with pneumonia and hypoventilation, while respiratory alkalosis occurs in conjunction with hyperventilation due to pain. In these situations, the underlying respiratory problem should be addressed.
- Hypovolemic and cardiogenic shock and Vasodilatory shock
Clinical signs |
Hypovolemic and cardiogenic shock |
Vasodilatory shock |
|
Heart rate |
Tachycardia and end stage bradycardia. |
Tachycardia |
|
Pulse rate |
Weak becoming absent. |
Bounding |
|
Capillary refill time CRT
|
Prolonged |
Rapid |
|
Mucous membrane
|
Pale Bright |
Red (hyperemic) |
|
Blood pressure |
May initially be normal due to sympathetic response then decline |
Low |
|
Temperature of extremities
|
Cool |
Warm |
- Types of fluid
a) Crystalloids
Crystalloids contain water, sodium or glucose, other electrolytes plus a buffer. The fluid may be hypotonic, isotonic or hypertonic relative to plasma. They distribute between the intravascular (25%) and interstitial compartments (75%) within one hour; thus, 1L of crystalloids results in a 250ml increase in plasma volume. Distribution into the interstitial compartment is beneficial if the animal is dehydrated as well as hypovolemic, but it will also promote tissue oedema formation, which may compromise perfusion.
Distribution in the intravascular compartment will result in a decrease in the total protein concentration (through dilution), which, in turn, will decrease the colloid osmotic pressure (COP), thus favoring further fluid loss into the interstitium, which again may be beneficial or detrimental depending on the individual case. These factors should all be borne in mind when considering the fluid therapy plan.
Isotonic solutions
Isotonic polyionic solutions are the most commonly used crystalloid solution in equine veterinary practice. Their electrolyte composition is similar to plasma; however, the potassium concentration is too low for maintenance requirements so 10 - 20 milliequivalent (mEq) potassium chloride (KCl)/L should be added . When choosing a fluid, it should be remembered Hartmann’s solution contains calcium, which will bind anticoagulants in blood products and that these fluids contain a buffer (lactate, acetate or gluconate) metabolized (by the liver, muscle or most cells, respectively) to bicarbonate, which will affect the acid-base balance.
Isotonic saline (0.9% NaCl) is hypernatremia and hyperchloremic relative to plasma and lacks other electrolytes. it’s used in cases of hyponatremia and hypochloraemia, rather than for resuscitation or maintenance.
Hypertonic solutions
Hypertonic saline (7% to 7.5% NaCl) is hypertonic relative to plasma and so initiates movement of water into the intravascular space from the interstitium, resulting in rapid expansion of the circulating volume. The plasma volume expansion achieved is two to four times that of the infused volume (2-4 ml/kg). However, this will result in intracellular dehydration, so it should be followed up with 10L of isotonic fluids for every 1L of hypertonic saline administered in two-and-a half hours.
Hypotonic solutions
A5% dextrose is a hypotonic solution that will replace water without electrolytes. Thus, it is only used in animals that are hypernatraemic and hyperchloraemic. It should be used with caution as it can cause hyperglycaemia with rapid administration, which will subsequently result in osmotic diuresis, and so further fluid loss.
b) Colloids
- Contain high molecular weight substances which don't readily migrate across capillary walls such as large sugar or protein molecules and are a mix of large and small molecules.
- The advantages of colloids over crystalloids are the large molecules improve oncotic pressure and provide rapid intravascular volume replacement by expanding the plasma volume by 100% of the volume infused, thus improving microvascular perfusion with less tissue oedema formation.
- The disadvantages are they are affected by alterations in capillary permeability, do not correct dehydration (interstitial losses).
Colloids available include plasma, whole blood and the synthetic colloid (gelofusine,
pentastarch and hetastarch).
plasma
Albumin is the primary component of plasma contributing 65% to 75% of plasma collected from a suitable donor or is commercially available in the form of hyperimmune plasma. immunoglobulins (in failure of passive transfer due to failure of colostrum intake ), clotting factors, anticoagulants and platelets.
Horses receiving plasma should be closely monitored for signs of hypersensitivity including tachycardia, pyrexia and urticaria. If signs occur, the infusion should be stopped and corticosteroid therapy IV may be necessary.
Whole blood
Whole blood is only indicated in cases of acute severe haemorrhage or haemolysis. No universal donor exists, but, ideally, the donor should be Aa and Qa antibody and antigen negative, although this requires a donor to have been blood typed in advance. Suitable alternatives include a young, healthy gelding that has never received a blood product, or a mare that has never had a foal.
Usually, cross matching is not performed the first time a blood or plasma transfusion is given, but should be performed for all subsequent transfusions, regardless of the donor.
Gelofusine
The synthetic colloid gelofusine contains succinylated gelatin and sodium chloride. It has been shown to expand the blood volume by 68% one hour after infusion and by 30% after six hours.
Side effects reported include:
- proteinuria (not clinically significant),
- hyperchloraemia (which may cause metabolic acidosis) and anaphylaxis.
- 10ml/kg and 20ml/kg gelofusine resulted in haemodilution and an increase in COP in healthy.
- Ponies were not associated with clinically significant adverse effects on haemostasis or renal parameters.
- Principles of Rehydration
1- Correct dehydration, electrolyte, and acid-base abnormalities prior to surgery.
2- Do not attempt to replace chronic fluid losses all at once.Severe dilution of plasma proteins, blood cells and electrolytes may result.
3- Aim for 80% rehydration within 24 hours.
4- Monitor pulmonary, renal and cardiac function closely.
- Signs of fluid overload
1- Serous nasal discharge.
2- Increased respiratory rate (Dyspnea).
3- Crackles or muffled lung sounds on pulmonary auscultation
4- Late stage consequence = pulmonary edema (pleural effusion ).
5- Decreased PCV.
6- Increased BP.
- Administration routes
Two main administration routes should be considered: oral and IV.
- Oral fluids are contraindicated if ileus, intestinal obstruction or severe mucosal inflammation is present or if the horse is unable to stand or require rapid, large volume resuscitation. In these cases, only IV fluid therapy should be considered.
- The two routes can be used alone or in combination.
Oral fluids
- The main advantages of oral fluids are easier and the fact GI mucosa acts as a natural selective barrier – making iatrogenic imbalances less likely. Absorption from the GI tract is increased in hypovolaemia, so oral fluids have a haemodynamic effect in about 30 minutes, which is quick enough in many cases.
- The indications for oral fluids include restoration of electrolyte balance and hydration status:
- to prevent dehydration occurring in horses with ongoing losses that are not drinking.
- to increase hydration of the GI contents – for example, if a large intestinal impaction is present.
- to stimulate intestinal motility via the gastrocolic reflex.
- Oral fluids can be administered via a nasogastric or naso-oesophageal tube, and as a bolus or continuously by gravity. Most commonly, a bolus is administered via a nasogastric tube. Up to 10L every 30 minutes (40ml/kg/hr) can be given and maintenance rates are 2.5ml/kg/hr. Ideally, the fluid should be isotonic. This can be achieved by adding 4.9g NaCl and 4.9g (KCl) to each litre of water. Including glucose has no apparent beneficial effect on the rate of absorption in the horse.
Complications that should be monitored for include aspiration, nasogastric tube complications, abdominal discomfort, GI rupture and electrolyte imbalances.
IV fluid therapy
IV fluid therapy via the jugular vein is the only site suitable for high volume resuscitation.
However, it must be remembered thrombophlebitis at this site can cause significant morbidity. If the horse is severely dehydrated, fluids can be administered via both jugular veins simultaneously using a large gauge catheter combined with a wide bore delivery system, allowing a maximum administration rate of 35 L/hr.
- Fluid’s calculation
- Rehydration is based on the estimated percent of dehydration.
dehydration % x weight in kg = deficit in liters. Rate of administration 50% in 1–2 h; 50% throughout rest of day.
- Maintenance fluids can be dosed at 50 ml/kg/day in adults and 110 ml/kg/day in foal.
- References
- Dewitt SF. Proceedings 22nd Annual ACVIM Convention, 2004.
- Jones PA et al. Effect of hydroyethyl starch infusion on colloid oncotic pressure in hypoproteinemic horses. JAVMA 2001:218:1130-5.
- Jones PA et al. Oncotoic, hemodilutional, and hemostatic effects of isotonic saline and hydroxyethyl starch solution in clinically normal ponies. Am J Vet Res 1997;58:541-8.
- Marlin DJ et al. Rehydration following exercise: effects of administration of water versus an isotonice oral rehydration solution (ORS). Vet J 1998;156:41-49.
- Sosa Leon LA et al. The effects of tonicity, glucose concentration and temperature of an oral rehydration solution on its absorption and elimination. Equine Vet J 1995;Suppl(20):140-146.