Guide to using devices in surgical operating rooms
| Site: | EHC | Egyptian Health Council |
| Course: | دلائل الاجراءات التمريضية لقسم العمليات |
| Book: | Guide to using devices in surgical operating rooms |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:34 AM |
Description
"last update: 9 Feb. 2025" تحميل الدليل
- Prepared by
Operation Room guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Head of nursing administration at EHA |
Mr. Adham Abdel Nasser Okasha |
12 |
|
member of the Nursing administration at EHA, luxor branch |
Mr. Gehad Akram Hussein |
13 |
- The Monitor
Definition:
A medical monitor is an electronic medical device used for continuous medical observation, displaying physiological data in real-time on its screen.
Types of Medical Monitors
1. Analog Monitoring Devices:
- Previously used only to display electrocardiograms (ECG).
- Later modified to measure blood pressure and pulse rate separately.
- These devices were widely used and helped save many lives but had several drawbacks, such as:
- Electrical interference.
- Lack of alarm systems.
- High cost.
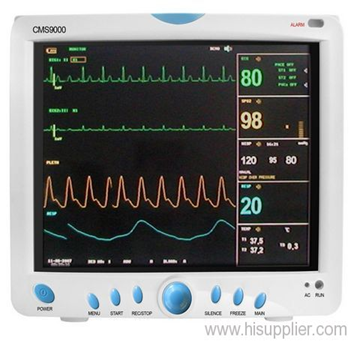
2. Digital Monitoring Devices:
- With the advancement of digital signal processing technology, medical monitors have improved significantly.
- All modern monitors are fully digital, offering compact designs and easy portability.
- Standard monitoring parameters now include:
- Pulse oximeter (measuring oxygen saturation).
- Blood oxygen level.
- Blood pressure.
- Body temperature.
- Electrocardiogram (ECG).
3. Monitoring Devices Attached to Pacemakers:
- Commonly used in emergency and reception units.
- Designed to save time and effort by eliminating the need to transfer patients between multiple devices.
Users & Applications:
1. Vital signs measurement.
2. Electrocardiogram (ECG) monitoring.
3. Blood pressure measurement using a pressure cuff wrapped around the patient’s arm.
o Normal blood pressure: 120/80 ± 20/15 mmHg.
4. Body temperature measurement using temperature transducers.
o Normal temperature: 36.5°C – 37.5°C.
5. Blood oxygen level measurement (SpO₂ monitoring).
Most used individuals :
1Critical care unit patients.
2 Patients in dialysis units.
3 Operating room patients.
4 Patients in recovery rooms.
5 Patients in reception units until they are classified.
6 Pediatric patients in the neonatal critical care unit.

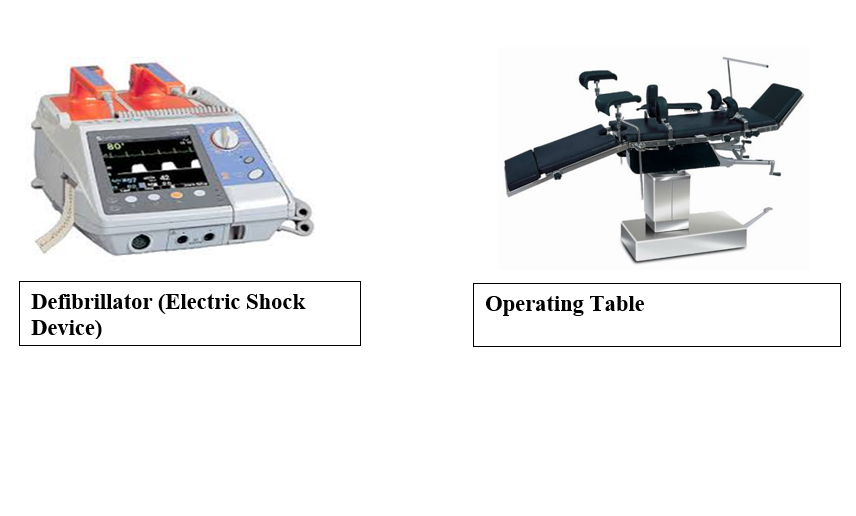
- electric shock device DC Shock
Definition:
Defibrillation is the process of delivering an electric shock to the surface of the heart to suppress an irritated focus in either the atrium or ventricle. It is most effective when administered within 15–20 seconds of the onset of arrhythmia (irregular heartbeat).
This procedure stabilizes the irritated focus, allowing the sinoatrial (SA) node to restore the heart’s natural rhythm.
The energy of the shock is measured in joules (J) and is typically administered as follows:
- First dose: 200 J
- Second dose: 200–300 J
- Third dose: 360 J
Device Description and Operation:
A defibrillator functions both as a monitor and a shock-delivering device.
Steps to Operate the Device:
1. Set the shock energy as per the protocol mentioned above.
2. Select the mode of defibrillation:
- Synchronized (Sync Mode): Delivers the shock in sync with the R wave on the ECG.
- Used for:
- Atrial fibrillation
- Atrial flutter
- Non-Synchronized Mode: Used only for Ventricular Fibrillation (VF), where there is no R wave.
3. Apply a sufficient amount of conductive gel on both paddles and the patient’s skin to prevent burns.
4. Correct placement of paddles:
- The sternum paddle (labeled Sternum) is placed on the right upper chest below the clavicle (collarbone).
- The apex paddle (labeled Apex) is placed at the heart's apex, below the left nipple.
Purpose of Using the Defibrillator:
- To correct irregular heartbeats (arrhythmias).
- To restart the heart in cases of sudden or complete cardiac arrest.
How the Defibrillator Works:
- The device delivers an electric shock through two paddles placed on the patient’s chest.
- This shock forces the heart muscle cells to contract momentarily.
- The electrical charge is stored in a high-voltage capacitor, which takes a few seconds to charge.
- Once charged, an alarm sounds, signaling that the device is ready to deliver the shock.
- The capacitor then releases the stored energy into the patient's body through the paddles, resetting the heart’s electrical activity.
Nursing care with defibrillator
Safety and Security Procedures
1. Device Safety Measures:
- Complete electrical isolation between the input and output circuits.
- Each paddle should have a discharge button to release residual energy.
- The device should have both audible and visual alarms to indicate when it is charged.
- The device should include automatic internal discharge to prevent accidental shocks.
2. Patient Safety Measures:
- Apply a sufficient amount of conductive gel to prevent skin burns.
- Firmly press the paddles onto the chest to prevent movement, ensuring that the gel does not create a gap between them, which could cause an ineffective discharge.
- Ensure the patient is not connected to any other electrical medical device during defibrillation.
3. User Safety Measures:
- Clean the paddles thoroughly after use to remove gel residue.
- Do not touch the patient while delivering the shock.
- Never discharge the shock into the air or on adhesive electrode pads.
Steps for Performing Defibrillation
1. Expose the patient's chest.
2. Begin CPR (Cardiopulmonary Resuscitation) immediately.
3. Apply conductive gel on both paddles and the patient’s skin to prevent burns.
4. Set the shock energy level according to the doctor’s instructions.
5. Correct paddle placement:
o Sternum Paddle: On the upper right chest, below the clavicle (sternum).
o Apex Paddle: Over the apex of the heart, below the left nipple (apex).
6. Press the charge button.
7. Lift the paddles after delivering the shock.
- Types of Electrical Shocks
1. Non-Synchronized Shock (Defibrillation)
- The shock is delivered immediately when the button is pressed (not synchronized with the heart rhythm).
- Energy levels:
- First shock: 200 J
- Second shock: 300 J
- Third shock: 360 J
- If unsuccessful, perform CPR for 1 minute and then reattempt defibrillation.
Indications for Non-Synchronized Shock:
1. Pulseless Ventricular Tachycardia (VT)
2. Ventricular Fibrillation (VF)
2. Synchronized Shock (Cardioversion)
- The shock is synchronized with the R wave of the ECG.
- The device automatically selects the right timing for shock delivery.
- Lower energy levels (typically 50–100 J).
- A sedative should be given before delivering the shock.
- Only one shock is delivered per cycle.
Indications for Synchronized Shock:
Unstable Tachycardia (irregular heart rate with low blood pressure), including:
1. Atrial Fibrillation (AF)
2. Ventricular Tachycardia (VT) with a pulse
3. Supraventricular Tachycardia (SVT)
If blood pressure is normal:
- Start with medications such as:
- Digoxin
- Adenosine
- Verapamil (Isoptin)
- Amiodarone (Cordarone)
- If blood pressure drops, then proceed with synchronized cardioversion.
Critical Mistake in Defibrillation
- Fatal error: Misdiagnosing Ventricular Tachycardia (VT) with a pulse as Pulseless Ventricular Tachycardia (PVT).
- Why is this dangerous?
- Both conditions may appear identical on an ECG.
- If the patient has a pulse, but a non-synchronized shock (defibrillation) is delivered instead of a synchronized shock (cardioversion), the incorrect shock can eliminate the pulse, worsening the condition and possibly causing death.

1. Ventricular Fibrillation (VF)

2. Immediately After the Electric Shock

3. In Case of Success