Neonatal Service Levels
| Site: | EHC | Egyptian Health Council |
| Course: | دلائل الاجراءات التمريضية لقسم حديث الولاده |
| Book: | Neonatal Service Levels |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 9:14 AM |
Description
"last update: 9 February 2025" تحميل الدليل
- Prepared by
NICU guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Professor of Obstetrics and Gynecology Nursing |
Dr. Nagat Salah Shalabi Salama |
12 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Shaima Abdel Basset Ibrahim Salim |
13 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Hoda Al-Sayd Muhammad |
14 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Walaa Ahmed Ali |
15 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Omnia Abdel Qader Muhammad |
16 |
|
member of the Nursing administration at EHA- South Sinai branch |
Mrs. Yasser Abdel Karim Omar Abdel Jawad |
17 |
- Neonatal Care Unit Service Levels
Neonatal care units in hospitals affiliated with the Ministry of Health and Population provide various services for newborns, whether full-term or preterm.
The type of services these units offer depends on several factors, including:
- Available space
- The types and number of devices and equipment in these units
- The number and skill level of healthcare providers
- The number of admissions and types of medical conditions treated in these units
Perinatal Care Based on Geographic Distribution:
- This system involves collaboration among all healthcare team members and hospitals to provide high-quality medical services for mothers and newborns during the perinatal period. This is achieved by implementing a referral system within a defined geographical area based on the required level of care.
- Level 1
Provides care for full-term and normal-weight newborns (gestational age of 37 weeks or more, birth weight of 2500g or more, and no complications). However, urgent medical and nursing care should be available in case of unexpected complications, especially neonatal resuscitation.
Appropriate Location:
- The newborn should remain with the mother in the postnatal observation room, ensuring that the number of newborn beds matches the number of maternal beds. The mother and baby should not be separated.
- The room temperature should be maintained between 24-26°C to ensure newborn comfort.
Required Equipment and Supplies:
- Infant warmer
- Fully equipped neonatal resuscitation kit with medications
- Neonatal stethoscope
- Suction device
- Infant scale
- Thermometer for newborns
- Antiseptic eye drops (antibiotic)
- 70% ethanol alcohol for umbilical cord care
Staffing:
- One nurse for every four newborns, trained in neonatal resuscitation.
- Level 2
Provides care for:
- Preterm newborns (32–37 weeks gestational age)
- Low birth weight infants (1500g – <2500g)
- Infants born to diabetic mothers
- Newborns from high-risk pregnancies or complicated deliveries
- Mild to moderate respiratory distress that does not require mechanical ventilation but may need oxygen therapy or NCPAP (Nasal Continuous Positive Airway Pressure)
- Neonatal jaundice requiring phototherapy
- Neonatal sepsis
- Hypothermic newborns
Appropriate Location:
Refer to the standard guidelines for neonatal care unit
requirements.
Required Equipment and Supplies:
Refer to the standard guidelines for neonatal care unit
requirements.
Staffing:
- One nurse for every 1–3 newborns in Level 2. (These staffing levels are not yet included in the FTE workforce planning guidelines of the Healthcare Authority.)
- Resident physician trained in neonatal care available 24/7.
- Pediatric specialist trained in neonatal care available 24/7.
- Level 3 (Neonatal Intensive Care Unit - NICU)
Provides care for:
- Preterm newborns (<32 weeks gestational age)
- Very low birth weight infants (<1500g)
- Newborns in shock
- Severe respiratory distress requiring mechanical ventilation
- Neonatal seizures
- Severe jaundice requiring exchange transfusion
- Newborns requiring total parenteral nutrition (TPN)
Appropriate Location:
Refer to the standard guidelines for neonatal care unit
requirements.
Required Equipment and Supplies:
Refer to the standard guidelines for neonatal care unit
requirements.
Staffing:
- One nurse for every 1–2 critically ill newborns per shift, trained in providing specialized neonatal intensive care.
- Resident physician available 24/7, trained in managing critically ill newborns.
- Neonatal consultant available 24/7.
- Regulating Newborn Temperature
The body temperature remains stable when heat loss and heat gain are balanced. If heat loss exceeds heat production, hypothermia occurs, and vice versa. Therefore, maintaining an optimal thermal environment is a key goal for neonatal caregivers to preserve normal body temperature and reduce energy loss.
Neutral Thermal Environment (NTE):
- The ideal environmental conditions that help maintain the newborn’s core body temperature between 36.5°C and 37.5°C with minimal energy loss and oxygen consumption.
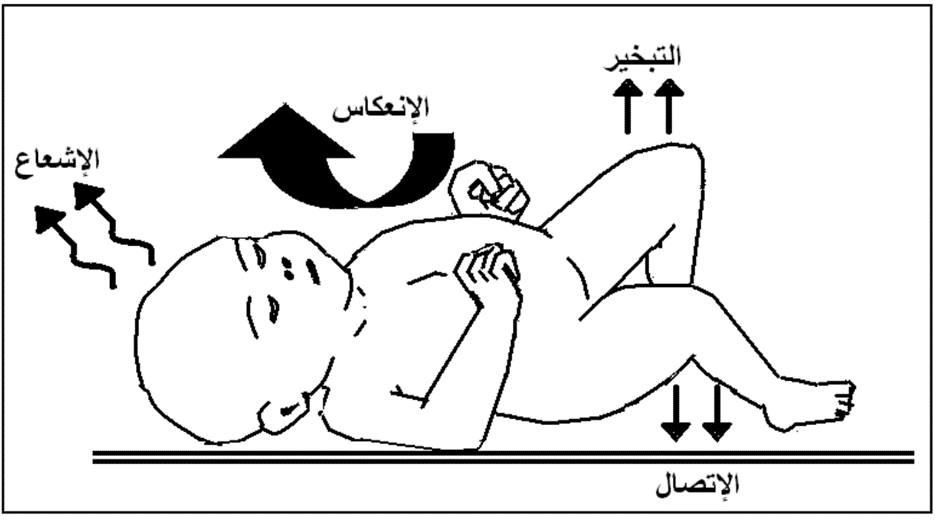
Ways Newborns Lose Heat:
1. Evaporation:
- Occurs when moisture (e.g., amniotic fluid or bath water) evaporates from the newborn's skin.
- Preventive measures:
- Dry the newborn thoroughly with a dry cotton towel immediately after birth and after bathing, especially the head.
2. Conduction:
- Occurs when the newborn's skin comes into direct contact with a cold surface (e.g., metal objects).
- Examples:
- Placing the newborn on a cold mattress or examination table.
- Using a cold weighing scale or X-ray plate without insulation.
- Placing a cold stethoscope on the newborn's skin.
- Preventive measures:
- Ensure insulation (e.g., cloth layers) between the newborn’s skin and any cold surfaces.
3. Convection:
- Occurs when air currents replace the warm air around the newborn with cooler air, leading to heat loss.
- Examples:
- Exposure to cold oxygen from a humidifier.
- Exposure to air currents from air conditioners or fans.
- Preventive measures:
- Keep newborns away from air drafts.
- Use warm water in oxygen humidifiers and change it regularly.
4. Radiation:
- Occurs when the newborn loses heat to a colder solid object nearby without direct contact.
- Example:
- Placing an incubator near a cold wall without maintaining the required 1-meter clearance on all sides.
- Preventive measures:
- Maintain room temperature at 24–26°C in delivery and neonatal units.
- Place incubators centrally in the room and ensure the 1-meter clearance from walls.
Body Temperature Regulation Disorders in Neonates
These disorders manifest either as hypothermia or hyperthermia.
I. Hypothermia
Definition:
A decrease in the infant’s core body temperature below 36.5 °C.
Causes:
- Exposure to a cold external environment due to failure to maintain the delivery room temperature at the appropriate range (24–26 °C).
- Failure to maintain the neonate’s temperature immediately after birth, especially in preterm infants, where body temperature may drop by 1 °C right after birth. Examples include:
- Not placing the neonate under a pre-warmed radiant warmer during immediate postnatal care.
- Delayed drying of the neonate, or leaving wet towels underneath.
- Separation from the mother.
- Giving the neonate a bath immediately after birth, even with warm water.
- Dressing the neonate inadequately or in light clothing.
Infants at higher risk of hypothermia:
- Low birth weight or growth-restricted infants.
- Infants with hypoglycemia.
- Infants with birth asphyxia.
- Infants with neonatal sepsis.
- Infants with congenital heart or gastrointestinal anomalies (e.g., omphalocele, gastroschisis).
- Infants with hemolytic disease due to Rh incompatibility.
- Infants with respiratory distress.
Clinical manifestations of hypothermia:
Early signs:
- Cool skin to touch, especially extremities, with peripheral cyanosis.
- Weak suck or poor feeding ability.
- Signs of respiratory distress (increased respiratory rate) and tachycardia.
- Lethargy and weak crying.
- Skin color changes from pallor and cyanosis to mottling.
Late signs:
- Apneic episodes.
- Bradycardia.
- Hypoglycemia.
- Metabolic acidosis.
- Intracranial or pulmonary hemorrhage.
- Sclerema neonatorum (hardening of subcutaneous fat tissue).
II. Hyperthermia
Definition:
An increase in the infant’s core body temperature above 37.5 °C.
Causes:
- Exposure to excessive environmental heat.
- Overheating due to high incubator temperature.
- Exposure to phototherapy without adjusting incubator settings.
- Severe dehydration.
- Neonatal sepsis.
- Intracranial hemorrhage.
Clinical manifestations of hyperthermia:
- Warm skin to touch, initially flushed then later pale.
- Tachycardia.
- Tachypnea.
- Irritability.
Role of the Nurse in Maintaining Neonatal Temperature
1. In the Delivery Room:
- Prepare a warm environment, free from air drafts, with room temperature maintained at 24–26 °C.
- Preheat the radiant warmer (servo-controlled) 10–20 minutes before delivery.
- Dry the neonate immediately after birth, ensuring no wet towels remain underneath.
- Encourage skin-to-skin contact with the mother whenever possible.
2. In the Neonatal Intensive Care Unit (NICU):
- Upon admission, undress the neonate except for the diaper, and place under the radiant warmer.
- Attach the temperature probe to the right upper abdominal wall.
- Adjust the radiant warmer to 36.5 °C.
- Measure the neonate’s temperature every 30–60 minutes or as prescribed until it stabilizes.
- Monitor temperature every 3–4 hours, and adjust incubator settings according to age and weight (Table 8-1).
- Place incubators away from sunlight or drafts.
- Minimize incubator door openings.
- Monitor temperature closely during phototherapy to prevent overheating.
Table 8-1. Neutral Thermal Environment (Incubator Temperature Settings)
|
Age & Weight |
Incubator Temperature (°C) |
|
|
Initial Temperature (°C) |
Range (°C) |
|
|
0–6 hours <1200 g |
35.0 |
34.4 – 35.0 |
|
1200–1500 g |
34.1 |
33.9 – 34.4 |
|
1501–2500 g |
33.4 |
32.8 – 33.8 |
|
>2500 g |
32.9 |
32.0 – 33.8 |