Newborn Feeding Guide
| Site: | EHC | Egyptian Health Council |
| Course: | دلائل الاجراءات التمريضية لقسم حديث الولاده |
| Book: | Newborn Feeding Guide |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 9:20 AM |
Description
"last update: 10 February 2025" تحميل الدليل
- Prepared by
NICU guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Professor of Obstetrics and Gynecology Nursing |
Dr. Nagat Salah Shalabi Salama |
12 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Shaima Abdel Basset Ibrahim Salim |
13 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Hoda Al-Sayd Muhammad |
14 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Walaa Ahmed Ali |
15 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Omnia Abdel Qader Muhammad |
16 |
|
member of the Nursing administration at EHA- South Sinai branch |
Mrs. Yasser Abdel Karim Omar Abdel Jawad |
17 |
- Introduction
Newborn Nutrition
Newborns can be fed through two main methods: either via the digestive system or intravenously.
First: Feeding through the Digestive System
Breastfeeding
Newborns receive breast milk through various methods, including:
- Directly breastfeeding from the mother's breast.
- Indirect feeding using expressed breast milk through a syringe, cup, dropper, feeding tube, or continuous drip.
Formula Feeding
Newborns are given formula milk when breastfeeding is not possible. This can be done through:
- A baby bottle.
- A feeding tube.
- Continuous drip feeding.
Second: Intravenous Nutrition
This method involves providing the newborn with essential nutrients in the form of intravenous solutions, either partially or fully, in cases where feeding through the digestive system is not possible.
- Breastfeeding
During the first months of life, an infant relies on the mother’s breast for nourishment. Breastfeeding is considered a natural extension of the mother’s responsibility, which began during pregnancy when the baby was fed through the umbilical cord. Therefore, mothers should be encouraged to practice exclusive breastfeeding (without any external supplements) until the end of the sixth month, and to continue breastfeeding with additional foods until the child reaches two years of age.
Structure of the Breast
The breast consists of milk glands, each made up of clusters of small sacs (alveoli). Surrounding these milk-producing glands are muscular tissue and fat, which give the breast its external shape.
Each alveolus connects to thin ducts, which merge into larger milk ducts. These ducts lead to the nipple and open through 15–20 tiny openings. Before reaching the nipple, these ducts expand into milk reservoirs (lactiferous sinuses), located behind the dark-colored area around the nipple, known as the areola.
On the areola, Montgomery glands secrete a substance that naturally moisturizes the breast.
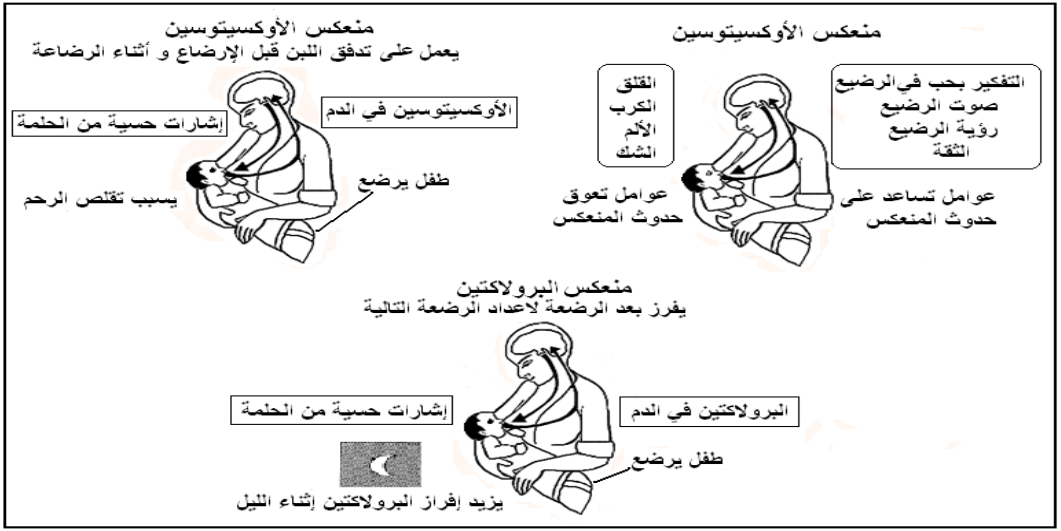
Physiology of Breastfeeding
The act of sucking by the newborn is the primary and strongest stimulus for milk production and secretion. This process triggers a neurohormonal reflex that affects the pituitary gland, leading to the release of two key hormones: prolactin and oxytocin.
Prolactin Reflex
The prolactin hormone, secreted by the anterior pituitary gland, stimulates the mammary glands to produce milk. Its secretion increases, especially at night.
Let-Down Reflex
The oxytocin hormone, secreted by the posterior pituitary gland, causes contraction of the muscle cells surrounding the alveoli, which helps push milk toward the baby’s mouth. The release of oxytocin is influenced by the mother’s physical and emotional state.
Local Regulation: Feedback Inhibitors of Lactation
If milk accumulates in the breast, the breast secretes inhibitors that stop the milk-producing cells from producing more milk. This mechanism helps prevent excessive breast engorgement.
Stages of Breast Milk
Colostrum
Colostrum is the first milk secreted by the breast in the first few days after birth. It is a thick, yellowish liquid that contains a higher concentration of proteins and antibodies that help protect the newborn from infections. It also has a mild laxative effect, helping prevent neonatal jaundice. Colostrum provides everything the newborn needs before mature milk is produced. It continues to be secreted for about three days, with the quantity gradually increasing to 40–60 mL per day.
Mature Milk
Colostrum gradually transitions into mature milk within two weeks. Its quantity increases, and its appearance and composition change, becoming more fluid with a slight bluish tint. Mature milk consists of:
- Water (87%): Provides sufficient hydration for the infant.
- Fats: Essential for brain development. Hindmilk (the milk at the end of a feeding session) contains higher fat content than foremilk (the milk at the beginning of the session). Therefore, the baby should feed until the breast is emptied to receive the rich, calorie-dense hindmilk.
- Proteins: Easily digestible and include immune-boosting proteins. The balance of amino acids in breast milk is ideal for infant growth.
- Carbohydrates: Lactose is the primary carbohydrate, playing a crucial role in energy and growth.
- Vitamins and Minerals:
- Breast milk is a rich and essential source of vitamins.
- Although the iron content in breast milk is low, it is absorbed at an efficiency of 50%, ensuring the baby receives sufficient iron and remains protected from iron-deficiency anemia until six months of age.
- Calcium absorption (70%) from breast milk is also high, providing the necessary amount for infant growth.
- Enzymes: Facilitate digestion, making breast milk easy for the infant to process.
Fundamentals of Breastfeeding
Encouraging Skin-to-Skin Contact and Early Breastfeeding
In most cases, newborns do not need resuscitation after birth. The natural position for a newborn is on the mother’s chest (skin-to-skin contact). Immediately after birth, the baby is placed on the mother's chest, with its head between her breasts, supported by her arms. The umbilical cord is cut in this position, and the newborn is quickly dried (head first, followed by the body), and wet towels are removed.
The baby instinctively moves toward the breast and starts sucking—this is called "self-attachment."
Skin-to-skin contact and self-attachment are key indicators of successful breastfeeding. Therefore, all mothers should be encouraged to initiate early skin-to-skin contact and begin breastfeeding within the first 30 minutes after birth.
Benefits of Early Breastfeeding:
- Ensures successful and sustained breastfeeding while reducing common breastfeeding challenges.
- Strengthens the bond between mother and baby.
- Newborns are highly alert and responsive in the first 30 minutes after birth, making it easier for them to latch onto the breast. After about two hours, they fall into deep sleep, making latching more difficult.
- Prevents low blood sugar, dehydration, and neonatal jaundice.
- Ensures the newborn receives colostrum, which is rich in nutrients and immune-boosting properties.
- Stimulates oxytocin secretion, which helps expel the placenta and prevents postpartum bleeding.
Avoiding Glucose and Herbal Drinks in the Early Hours After Birth
Giving a newborn glucose water or herbal drinks immediately after birth disrupts early breastfeeding and may cause breastfeeding refusal later on.
Rooming-In (Mother-Baby Co-Sleeping in the Same Room)
Rooming-in means keeping the baby in the same room as the mother 24 hours a day instead of being placed in a separate nursery.
Benefits of Rooming-In:
- Allows the mother to respond to her baby’s feeding cues immediately, promoting on-demand breastfeeding and strengthening the mother-baby bond.
- Increases mothers’ desire to breastfeed.
- Encourages longer breastfeeding duration, even after leaving the hospital.
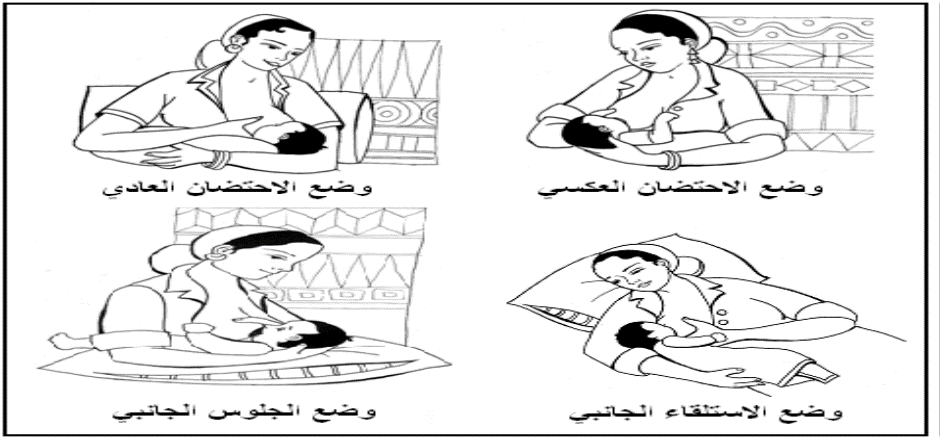
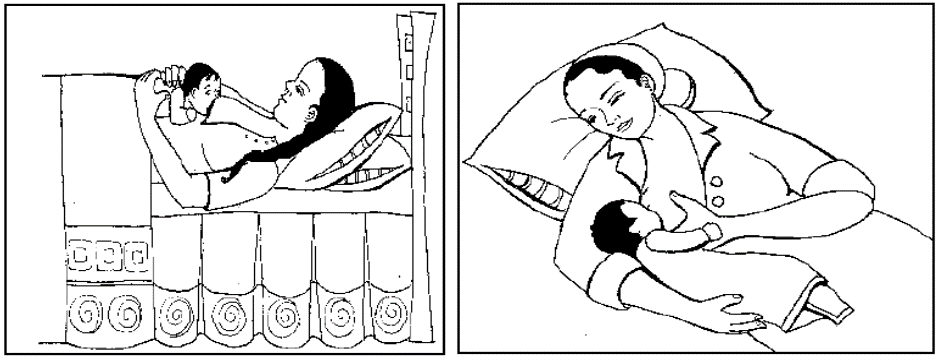
Correct Breastfeeding Positions
- The mother should be in a comfortable position. She can use pillows to support her arms or the baby, ensuring the baby is raised to breast level.
- The baby's stomach should face the mother’s stomach, ensuring proper alignment.
- The baby should be well-supported, straight, and parallel to the mother’s body.
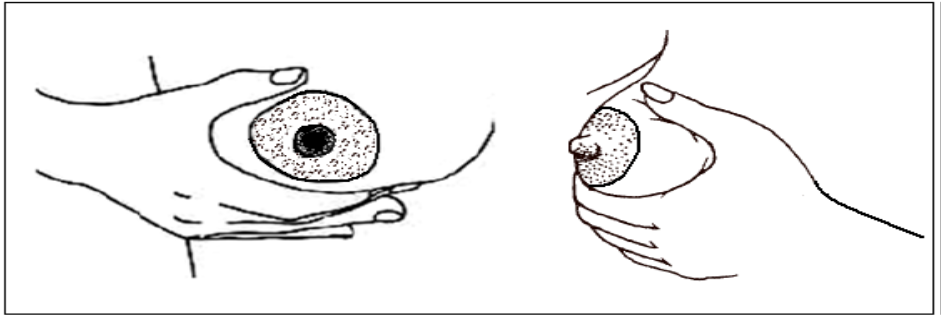
The Correct Way to Hold the Breast While Breastfeeding
When the baby's cheek or upper lip touches the nipple, the baby will naturally turn their head and open their mouth. The mother should quickly lift the baby to her breast.
To hold the breast correctly, the mother should:
- Place her thumb on top of the breast.
- Position the rest of her fingers underneath the breast, forming a "C" shape with her hand.
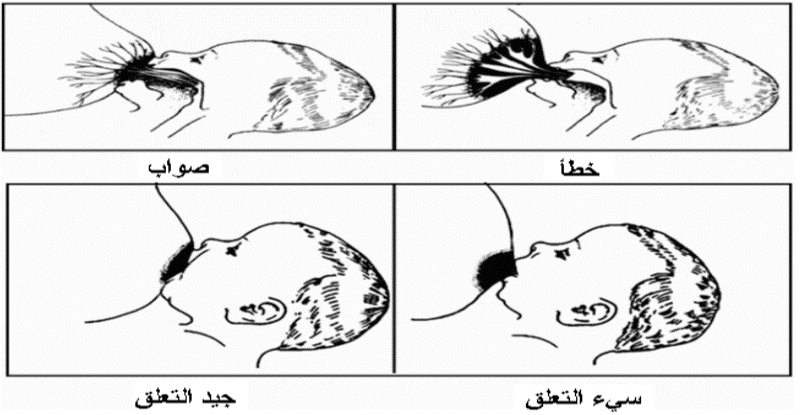
Signs of a Good Latch While Breastfeeding:
✅ The baby opens their mouth wide.
✅ The baby’s chin is pressed against the
breast.
✅ The baby’s lower lip is turned outward.
✅ More of the areola (dark area around the
nipple) is visible above the baby’s mouth than below.
✅ The baby’s cheeks appear rounded
while sucking.
Effective Breastfeeding Signs & Techniques
Signs of Effective Breastfeeding:
✔ Slow, deep sucking followed by audible swallowing.
✔ Monitoring breast milk adequacy through:
- Urine output: More than six wet diapers per day after the fourth day.
- Bowel movements: At least two stools per day after the fourth
day.
✔ Weight changes: Newborns lose 5-7% of their birth weight in the first week, then gain 25-35g daily.
Proper Breastfeeding Technique:
- Latching:
- Touch the baby's cheek with the nipple to stimulate rooting.
- Insert the nipple and most of the areola into the baby's mouth.
- If the breast is large, press it gently for easier breathing.
- Duration & Switching Breasts:
- 90% of milk is consumed in the first 5 minutes, but let the baby nurse until they stop naturally.
- Do not pull the breast away—insert a clean finger gently into the baby's mouth to release suction.
- Ensure the baby empties at least one breast per feeding to get the fat-rich hindmilk and stimulate milk production.
- Burping (Winding the Baby):
- Hold the baby upright over the shoulder and gently pat their back.
- After burping, place the baby on their right side or back.
- Hygiene:
- Wipe the baby's mouth with sterile gauze soaked in saline to prevent fungal infections.
- Starting the Next Feed:
- Begin the next session with the breast last used if it wasn’t fully emptied.
Feeding on Demand:
- Breastfeed whenever the baby shows hunger cues or when the mother feels full.
- Hunger Cues:
- Moving head from side to side.
- Opening the mouth or sticking out the tongue.
- Sucking on fingers or fists.
- Making quiet sounds.
- Smacking lips.
- Nuzzling mother’s chest.
- Turning head towards anything that touches their cheek.
- Crying is a late hunger sign—feed before reaching this stage!
Benefits of Feeding on Demand:
- Faster milk production and weight gain.
- Prevents breast engorgement.
- Ensures continuous milk supply.
Exclusive Breastfeeding (Until 6 Months):
- No extra liquids or foods (e.g., water, herbal drinks, formula).
- Avoid bottles, pacifiers, or artificial nipples, as they:
- Increase infection risk.
- Confuse the baby’s latch, leading to sore nipples, engorgement, and refusal of the breast.
Breast Care:
- Wash once daily—no soap or alcohol on the nipple, as it removes natural protective oils.
- After nursing, express a few drops of milk onto the nipple and let it air dry.
Breastfeeding Twins:
- Mothers can successfully breastfeed twins, as milk production depends on how much the babies nurse and empty the breasts.
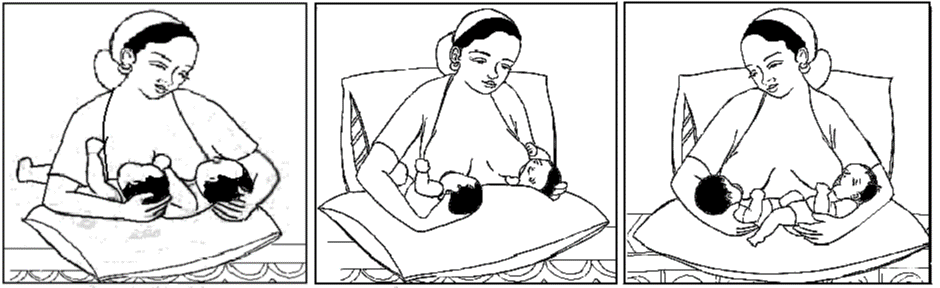
Cesarean delivery: The mother can breastfeed her baby after waking up from general anesthesia in a comfortable position, such as lying down.
Breast Milk Expression:
Indications:
- Collecting milk for a baby who cannot nurse directly, such as a baby in the neonatal unit, to ensure continued milk production.
- Collecting milk to feed the baby in the mother's absence due to work or illness.
- Relieving breast engorgement.
- Increasing milk supply, as infant sucking or breast emptying is the primary factor in maintaining and boosting milk production.
Important Considerations When Expressing Breast Milk:
- Milk should be collected using hygienic methods and stored in a sterile container.
- Hands should be washed with disinfectant, and milk should be stored in sterilized containers.
- If using a breast pump, all pump parts that come into contact with milk must be washed with hot soapy water after each use and sterilized daily.
Choosing Storage Containers:
- Glass containers are preferred over plastic bottles or bags.
- Containers should be washed with soap, rinsed thoroughly with hot water, and sterilized, especially for preterm babies.
Different Methods of Milk Expression:
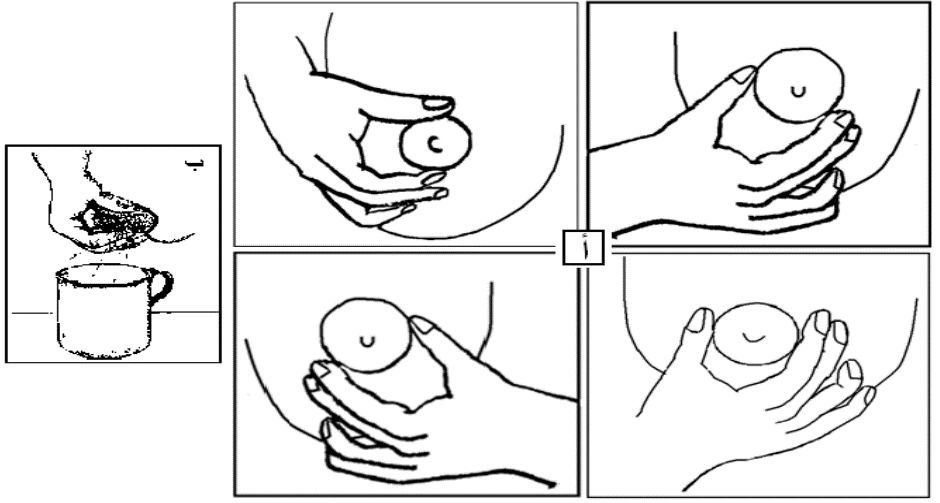
Manual Expression:
Advantages: A natural, comfortable, and cost-free method.
Steps:
- Wait at least one hour after breastfeeding. Sit in a quiet place and think about the baby, look at their picture, or nurse them on the other breast if present.
- Wash hands thoroughly with soap and water.
- Apply warm compresses or take a warm shower.
- Massage the breast in circular motions with both hands placed opposite each other from the top and bottom, as well as from the sides.
- Place the thumb and other fingers 3-4 cm behind the nipple at the edge of the areola. Imagine the areola as a clock, with the thumb at 12 o’clock and the index finger at 6 o’clock.
- Gently press the thumb and index finger inward toward the chest wall, avoiding excessive pressure to prevent blocking the milk ducts.
- Move the fingers lightly inwards toward the nipple without rubbing the skin of the areola.
- Repeat the motion several times, then change the finger positions in different directions after massaging the breast.
- Milk may not come out initially but will start dripping after repeated pressure and may flow in streams if the oxytocin reflex is active.
- Switch to the other breast when milk flow decreases.
- The amount of expressed milk varies each time.
- Express milk from one breast for 3-5 minutes. A full session takes about 20-30 minutes (or until the milk flow slows down), then switch to the other breast.
- Manual expression should not be painful. If there is pain, the technique is incorrect.
- At the end of the session, express a drop of milk and rub it on the nipple.
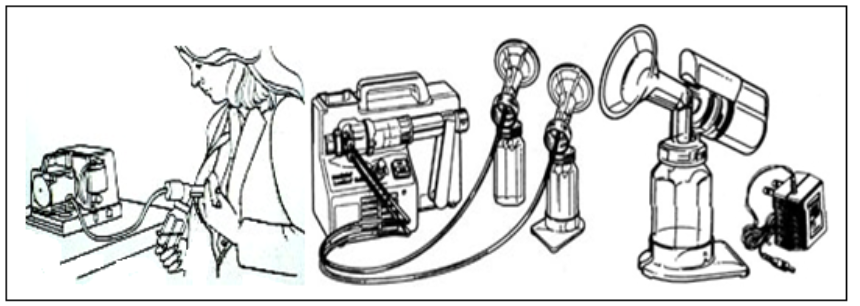
Breast Pump:
- Breast milk can be expressed using either manual or electric breast pumps.
- When using a breast pump, the following points should be considered:
- Read the cleaning and operating instructions carefully.
- Wash hands thoroughly before use.
- Follow techniques to enhance milk flow, such as warmth and massage.
- Wipe the breast with a damp cotton pad before pumping.
- Center the nipple inside the pump flange to ensure proper suction.
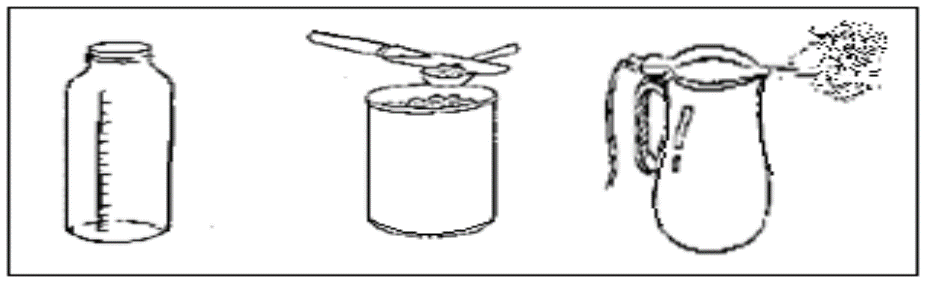
Manual Breast Pumps:
- Affordable and easy to use.
- However, they can be painful and are not reliable for long-term milk expression due to:
- Difficulty controlling suction strength.
- Challenges in proper sterilization.
Note: It is advised not to use the type of pump shown in the image.
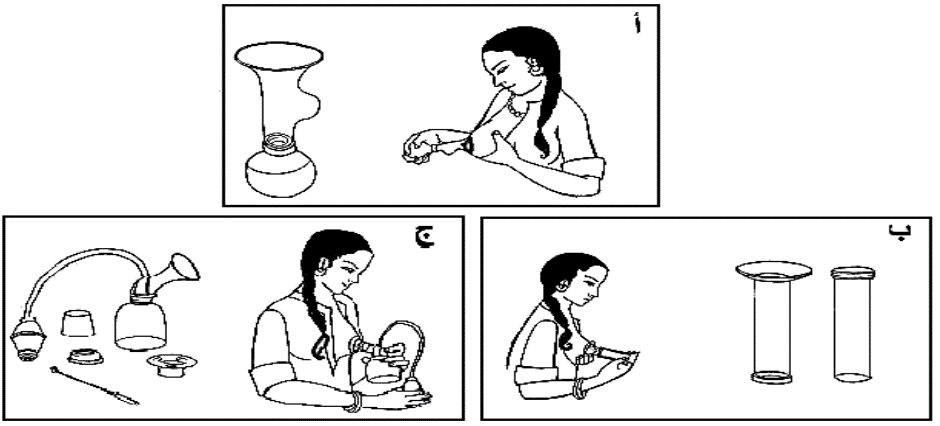
Electric Breast Pumps:
- Effective in stimulating and expressing milk.
- However, they are expensive compared to manual pumps.
Expressed Milk Storage and Transportation
- Transport expressed milk in a clean container surrounded by ice.
- Store in clean, covered cups, labeled with the date and time of expression.
- Refrigerate immediately after expressing.
- Storage guidelines:
- 4°C: Up to 48 hours in the refrigerator.
- Freezer (-20°C): 3 to 6 months storage.
- Divide milk into small portions (50-100ml) to reduce waste.
- Leave space in containers for expansion when freezing.
Using Frozen Expressed Milk
- Thaw in the refrigerator for one day before use.
- Warm by placing the cup in warm water, stirring gently.
- Do not boil or microwave to prevent nutrient loss.
- Do not reuse leftover milk after feeding.
- Once thawed, use within 24 hours—do not refreeze.
- Use the oldest milk first.
- Milk may separate into layers during storage—this is normal.
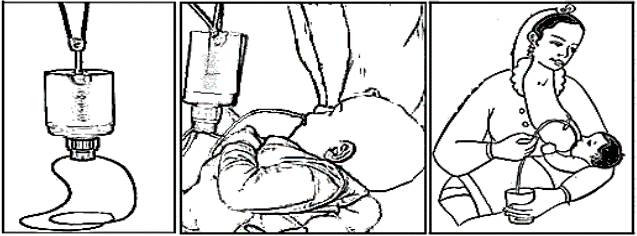
Feeding Expressed Milk to the Infant
Feeding Tube
- Administer milk quickly to prevent fat from sticking to the tube.
- When using a syringe pump, tilt it upwards to ensure the fat reaches the baby first.
Cup Feeding (Suitable even for premature infants)
- Keep the baby in an upright position.
- Fill the cup at least halfway with milk.
- Place the cup on the baby’s lower lip so milk touches the inner part.
- Let the baby lick the milk with their tongue.
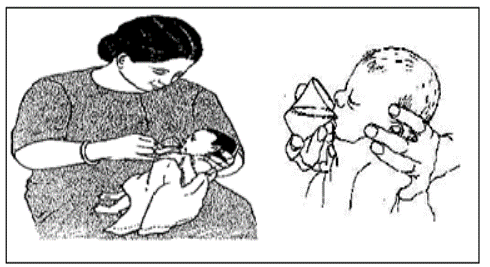
Other Feeding Methods
- Use a spoon, dropper, or syringe, directing milk to the side of the mouth to prevent choking.
Supplementary Feeding Device
- A small bottle with a thin tube attached to the mother’s breast. The baby sucks from both the breast and the device, stimulating milk production.
- A syringe or cup with a feeding tube can be a cheaper alternative.
- Benefits:
- Ensures adequate milk intake while maintaining breastfeeding stimulation.
- Can be placed on the mother’s finger to feed the baby in her absence.
Baby Bottles
🚫 Strictly prohibited. 🚫
Maternal Nutrition and Comfort During Breastfeeding
- A well-balanced diet with essential nutrients is important.
- Drink fluids as needed (when feeling thirsty).
- Get enough rest and sleep.
- Fenugreek and fennel may help increase milk supply.
- Avoid medications unless prescribed by a doctor.
Common Breastfeeding Issues
Postpartum Depression
- Many mothers experience mood swings or mild depression starting around day 2-3 postpartum, lasting 3-4 weeks.
- Usually mild and does not require treatment, but support from nurses and family is crucial for successful breastfeeding.
Breast Fullness (Engorgement)
- Between days 3-6 postpartum, milk production increases, causing fullness.
- This subsides within 2-3 weeks. If milk is not removed frequently, it can lead to painful engorgement.
Breast Engorgement & Hardness
- Symptoms: Extreme fullness, pain, redness, warmth, possible fever.
- Causes:
- Tight areola, making it difficult for the baby to latch.
- Painful milk flow due to swelling.
- Infection risk if untreated, leading to reduced milk supply.
Prevention:
✔ Correct baby’s latch during breastfeeding.
✔ Frequent feeding day and night.
✔ Avoid artificial nipples or formula supplementation.
Treatment:
✔ Apply warm compresses before feeding.
✔ Try different breastfeeding positions.
✔ Express some milk before feeding to ease latching.
✔ Massage the breast to improve milk flow.
✔ Apply cold compresses between feeds to reduce
swelling.
✔ Continue breastfeeding even if inflammation occurs.
Painful or Cracked Nipples
- Breastfeeding should not be painful, but mild discomfort in the first few days is normal.
Causes:
✔ Poor latch or flat/inverted nipples.
✔ Breast engorgement or baby tongue-tie.
✔ Artificial nipples or incorrect breast pump use.
✔ Reaction to nipple creams or fungal infections.
✔ Baby teething.
Prevention:
✔ Teach proper latching and positioning.
✔ Avoid artificial nipples.
✔ After feeding, apply breast milk on the nipple and
let it dry.
Treatment:
✔ Start feeding with the less painful breast.
✔ Try different positions to relieve pressure on sore
areas.
✔ Keep nipples clean and dry to promote healing.
✔ Apply pure lanolin or breast milk to soothe the
nipples.
✔ Air-dry nipples between feeds.
✔ For fungal infections, use antifungal creams
like Nystatin or Miconazole (as prescribed).
✔ Frequent feeding prevents engorgement and pain.
✔ If feeding is too painful, express milk manually or with
a pump and feed the baby.
Note: If nipple bleeding occurs, swallowing small amounts of blood is not harmful to the baby, and breastfeeding should continue.
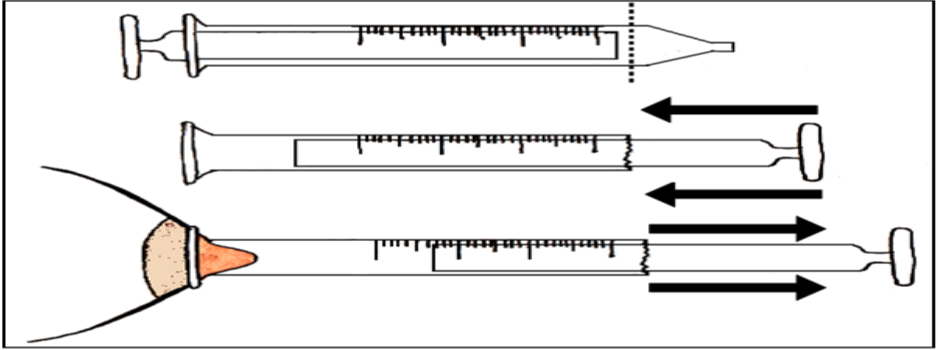
Flat or Inverted Nipples
Babies breastfeed from the breast, not just the nipple.
Treatment After Birth:
✔ Massage the nipple using thumbs to gently pull it
outward.
✔ Reverse syringe method:
- Cut a syringe near the tip to create a smooth opening.
- Insert the plunger in reverse
and use suction for 30-60 seconds.
✔ Repeat these 5-8 times before each feed until the baby latches naturally.
✔ Express breast milk without using artificial nipples if needed.
Breastfeeding and Maternal Care:
Maternal Nutrition and Rest During Breastfeeding:
- A well-balanced diet should include various essential nutrients.
- The mother should drink fluids as needed (drink when thirsty without a fixed amount).
- Ensure sufficient rest and sleep.
- Fenugreek and fennel are recommended as they help with milk production.
- Medications should only be taken with a doctor's approval.
Common Issues During Breastfeeding:
Postpartum Depression:
Many mothers experience mood changes or postpartum depression, usually starting between the second and third day after childbirth. It may last for 3-4 weeks and is usually mild, not requiring treatment. Nurses should be well-trained in counseling methods to support mothers during this period for successful breastfeeding.
Normal Breast Fullness:
When milk begins to flow abundantly between the third and sixth day postpartum, the mother may feel intense breast fullness, which subsides within 2-3 weeks. If milk is not continuously expressed, fullness can develop into engorgement.
Breast Engorgement:
Severe breast fullness may occur, accompanied by pain, redness, and possibly fever. The areola may become tight and less flexible, making it difficult for the baby to latch and causing painful milk flow. If untreated, the breast may develop infections and abscesses, leading to reduced milk production.
Prevention:
- Ensure proper baby positioning and latch during breastfeeding.
- Frequent breastfeeding, day and night.
- Avoid giving the baby formula or artificial nipples.
Treatment:
- Apply warm compresses before feeding or expressing milk.
- Try different breastfeeding positions.
- Express accumulated milk to ease flow.
- Massage the breast.
- Use cold compresses between feedings to reduce swelling.
- Continue breastfeeding even if the breast is inflamed.
Sore or Cracked Nipples:
Proper breastfeeding should not cause pain, but mild nipple discomfort is common in the first few days postpartum.
Causes:
- Incorrect baby positioning or latch.
- Inverted nipples, breast engorgement, or baby’s tongue-tie.
- Use of artificial nipples or improper use of breast pumps.
- Sensitivity to nipple creams.
- Fungal infections.
- Baby teething.
Prevention:
- Educate mothers on proper breastfeeding positions and latching techniques.
- Avoid artificial nipples.
- Apply a few drops of breast milk on the nipple after feeding and let it dry.
Treatment:
- Start feeding with the less painful breast.
- Try different feeding positions to reduce pressure on the sore area.
- Keep nipples clean and dry after feeding to promote healing.
- Apply a gentle nipple moisturizer like pure lanolin or a drop of expressed breast milk and allow it to dry.
- Allow nipples to air dry between feeds.
- For fungal infections, use topical antifungal creams such as Nystatin or Miconazole as prescribed by a doctor.
- Frequent breastfeeding keeps the breasts as empty as possible, relieving pain. If the pain is severe, milk can be expressed with a breast pump and given to the baby.
- Note: Swallowing small amounts of blood from nipple cracks is not harmful to the baby and does not require stopping breastfeeding.
Flat or Inverted Nipples:
This is not a significant issue since the baby feeds from the breast, not just the nipple.
Treatment After Birth:
- The mother may need time to help the baby latch. The following techniques may help:
- Nipple massage: Place both thumbs on either side of the nipple, press gently, and pull them apart. Repeat in different directions.
- Reverse syringe method: Cut a syringe near the needle end, insert the plunger from the cut side, and place the smooth side on the nipple. Gently pull the plunger for 30-60 seconds.
- Expressing milk before feeding: This helps the baby latch onto the breast. Avoid artificial nipples. Repeat this process 5-8 times before each feeding until the baby can latch directly.
- Formula Feeding
Formula milk should be prepared in bottles in quantities enough for a single feeding or for up to 4 hours if using continuous feeding via gastric tube. Refrigerated formula can be stored for up to 24 hours but should be used within 4 hours after opening.
Preparing and Giving Formula Milk:
Bottle Feeding:
- Use small nipples for premature babies, soft nipples for weak feeders, and regular nipples for strong feeders.
Preparation:
- Follow the doctor’s instructions regarding the formula type, concentration, and quantity.
Required Equipment:
- Bottle sterilizer or a large pot for boiling bottles.
- Bottles with nipples and caps.
- Kettle for boiling water.
- Sterile tray.
- Bottle tongs.
- Bottle brush.
- Liquid soap for washing bottles.
- Infant formula (check expiration date).
- Formula scoop.
- Knife.
- Clean cotton pad.
Steps:
- Wash hands properly.
- Boil the necessary amount of water plus 60ml extra to compensate for evaporation. Boil for one minute to sterilize.
- Let the water cool to room temperature.
- Pour the required amount of warm water into sterilized bottles.
- Add the correct formula amount using a leveled scoop.
- Shake well to mix.
- Test the temperature by dropping a few drops on the inner wrist before feeding.
- Cool the formula if needed by placing the bottle in cold water.
Feeding Steps:
- Wash hands properly.
- Verify baby’s full name and medical number, type of formula, and amount.
- Measure abdominal circumference as instructed.
- Ensure the baby is fully awake.
- Hold the baby as if breastfeeding.
- Place a cotton pad on the baby’s chest.
- Stimulate the baby’s lips with the nipple; once the baby opens its mouth, gently insert the nipple.
- Keep the nipple filled with milk at a 45-degree angle to avoid air intake.
- Maintain eye contact and emotional bonding with the baby.
- Encourage burping mid-feed and after feeding to prevent gas.
- Lay the baby on the right side to prevent choking and reduce stomach pressure.
- Clean the baby’s mouth with sterile saline-soaked gauze to prevent fungal growth.
- Discard any remaining milk—do not reuse.
- Wash hands properly.
- Record the amount of milk consumed, any vomiting, or abnormal signs (e.g., bluish skin) and inform the doctor.
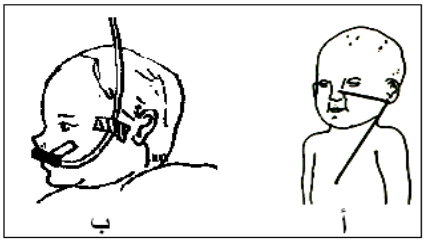
Feeding via Nasogastric Tube:
Required Equipment:
- Sterile feeding tube (size 6 for preemies <1500g, size 8 for larger babies).
- Syringe (10-20ml).
- Clean towel.
- Stethoscope.
- Warm formula per doctor’s instructions.
- Adhesive tape for fixation.
- Sterile water ampoules.
- Bottle nipple with cotton filling.
- Sterile gloves.
- Waste disposal bins (black & red bags, sharps box).
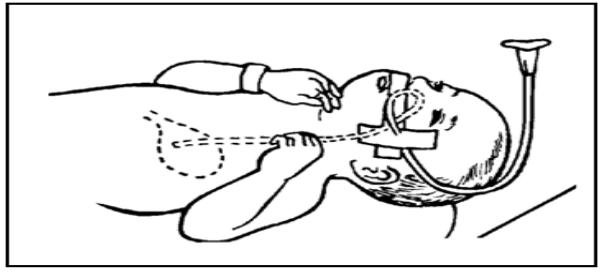
Tube Insertion Steps:
- Wash hands properly.
- Open the sterile feeding tube package.
- Wear sterile gloves.
- Measure the tube length from nose/mouth to the earlobe, then from earlobe to the bottom of the sternum, marking with tape.
- Insert the tube while positioning the baby’s head at a 30° angle.
- If resistance, choking, or blue discoloration occurs, immediately remove the tube and retry.
- Verify correct placement by injecting 0.5-1ml air and listening for gurgling sounds in the stomach with a stethoscope.
- Secure the tube with adhesive tape.
Continuous Drip Feeding and Intravenous Nutrition
1. Continuous Drip Feeding:
This method is preferred for:
- Newborns with severe gastroesophageal reflux (GERD).
- Low birth weight infants weighing less than 1000g at birth.
Preparation of Feeds:
- Follow the doctor's instructions regarding formula type, concentration, and quantity.
Feeding Procedure:
- Draw the required amount of milk into a syringe.
- Attach the syringe to a syringe pump, then connect it to the feeding tube using a syringe extension.
- Set the pump speed to the required drip rate per hour as per the doctor's instructions.
- Administer the feed using the syringe pump.
- Change milk containers (syringes) and connecting extensions every 4 hours to prevent milk exposure to room temperature for too long.
- Intravenous Nutrition
Intravenous (IV) nutrition provides newborns with essential nutrients, including:
- Glucose, amino acids, fats, vitamins, and minerals
- Given as Partial Parenteral Nutrition (PPN) or Total Parenteral Nutrition (TPN) through a peripheral or central venous catheter to meet the baby’s nutritional needs.
Indications for IV Nutrition:
- Premature infants (weighing less than 1000g at birth).
- Gastrointestinal disorders, such as intestinal paralysis, bowel obstruction, necrotizing enterocolitis, and congenital anomalies requiring prolonged feeding suspension.
- Post-surgical cases, such as corrective surgeries for congenital gastrointestinal defects.
Components of Total Parenteral Nutrition (TPN):
- Fluids: Calculated based on the infant’s weight and age.
- Calories: 90-100 kcal/kg/day.
- Glucose: Given at a concentration based on blood glucose levels.
- Proteins: Provided as amino acids, adjusted based on weight and age. Protein intake is reduced if blood urea levels are elevated.
- Fats: Administered as fatty acids, adjusted based on blood triglyceride levels. If triglycerides exceed normal levels, fat infusion is reduced or stopped.
- Electrolytes & Vitamins: Added according to the daily requirements for sodium, potassium, calcium, phosphorus, magnesium, and vitamins.
Nursing Care for IV Nutrition:
- Verify that the bottle label matches the medical chart (checked by two nurses).
- Follow infection control protocols in all steps.
- Use a pump infusion system to regulate flow and prevent stoppage (IV infusion should not be interrupted except for changing the solutions and equipment).
- Cover the IV bottle and tubing with silver adhesive tape to protect fats from light exposure.
- Monitor the infusion rate and solution clarity every 3 hours.
- Maintain a fluid balance chart at the end of each shift.
- Change the IV solution bottle and tubing every 24 hours.
- Use a separate cannula for administering medications and antibiotics.
- If the infusion stops suddenly due to blockage or dislodgement of the IV catheter, administer glucose as per the doctor’s instructions and monitor blood glucose levels.
- Monitor the infant continuously during total parenteral nutrition administration
Potential Complications of Total Parenteral Nutrition (TPN):
1. Catheter-Related Issues:
- Bloodstream infections (sepsis).
- Skin inflammation (redness) around the catheter site.
- Local blood clots (thrombosis).
- Swelling due to fluid leakage under the skin.
2. Metabolic Complications:
- High or low blood glucose levels.
- Electrolyte imbalances.
- Increased blood urea levels.
- Metabolic acidosis (increased blood acidity).
- Liver dysfunction leading to jaundice.