Neonatal Jaundice (Newborn Jaundice)
| Site: | EHC | Egyptian Health Council |
| Course: | دلائل الاجراءات التمريضية لقسم حديث الولاده |
| Book: | Neonatal Jaundice (Newborn Jaundice) |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:54 AM |
Description
"last update: 12 February 2025" تحميل الدليل
- Prepared by
NICU guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Professor of Obstetrics and Gynecology Nursing |
Dr. Nagat Salah Shalabi Salama |
12 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Shaima Abdel Basset Ibrahim Salim |
13 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Hoda Al-Sayd Muhammad |
14 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Walaa Ahmed Ali |
15 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Omnia Abdel Qader Muhammad |
16 |
|
member of the Nursing administration at EHA- South Sinai branch |
Mrs. Yasser Abdel Karim Omar Abdel Jawad |
17 |
- Neonatal Jaundice
Neonatal jaundice is a common condition observed during the first week of an infant's life. It affects approximately 80% of preterm infants and more than 50% of full-term newborns. In many cases, treatment is simple and effective. However, the condition can become dangerous if bilirubin levels rise significantly, reaching the brain and potentially causing damage to sensory and motor centers.
Neonatal jaundice is defined as an increase in bilirubin levels in the newborn’s blood exceeding 5-7 mg/100 ml (Indirect bilirubin), which results from the breakdown of red blood cells. It manifests as a yellowish discoloration of the newborn’s skin and the whites of the eyes, gradually spreading downward towards the chest, abdomen, and eventually the feet.
Types of Indirect Hyperbilirubinemia:
- Physiological jaundice
- Pathological jaundice
- Breastfeeding-related jaundice (due to insufficient milk intake)
A. Physiological Jaundice
This type affects around 50% of newborns and appears between the second day and the tenth day of life, usually resolving by 14 days after birth. It generally does not reach dangerous bilirubin levels and does not require treatment except in certain cases as determined by a doctor after medical evaluation and laboratory tests.
Physiological jaundice occurs equally in both male and female newborns and is considered a normal condition due to the natural breakdown of red blood cells. Normally, the liver processes the excess bilirubin, converting it into direct bilirubin, which is then eliminated through stool. However, in newborns, particularly preterm infants, liver function is not yet fully developed. This immaturity makes it difficult for the liver to process bilirubin efficiently, leading to elevated indirect bilirubin levels in the blood.
Preterm infants are more susceptible to physiological jaundice due to their underdeveloped liver. For these infants, treatment is usually required when bilirubin levels reach 14–16 mg/100 ml.
B. Pathological Jaundice (Non-Physiological Jaundice)
This type is less common but far more dangerous than physiological jaundice, as bilirubin levels can rise to over 25 mg/100 ml, potentially leading to brain damage, hearing loss, cerebral palsy, mental retardation, and motor impairment.
Causes of Pathological Jaundice:
- Blood incompatibility between mother and infant, such as:
- Rh incompatibility (Rh–incompatibility)
- ABO blood group incompatibility (ABO–incompatibility)
- This results in the mother's immune system attacking the newborn’s red blood cells, leading to severe hemolysis and dangerously high bilirubin levels. This condition often occurs within the first 24 hours after birth and requires urgent medical treatment.
- Glucose-6-phosphate dehydrogenase (G6PD) deficiency (Favism)
- Neonatal sepsis (blood infection)
- Cephalhematoma (bleeding under the scalp) or bruising under the skin
- Hypothyroidism (low thyroid hormone levels)
- Polycythemia (high red blood cell count), often seen in infants of diabetic mothers or cases of delayed cord clamping
- Liver enzyme deficiency (Glucuronyl transferase enzyme deficiency)
- Prematurity and low birth weight
C. Breastfeeding-Related Jaundice (Not-Enough Breast Milk Jaundice)
This occurs in the first days after birth due to inadequate milk intake, either because of insufficient breastfeeding frequency or the newborn’s difficulty in latching onto the breast properly.
Treatment:
Increasing breastfeeding frequency helps to enhance stool output, thereby
eliminating bilirubin more quickly.
Nurse's Assessment of Jaundice:
1. Medical History Collection:
- Mother’s blood type and Rh factor
- Family history of genetic red blood cell disorders (e.g., G6PD deficiency)
- History of jaundice in previous siblings due to blood incompatibility
- Maternal diabetes, infections, or medication use during pregnancy
- Gestational age at birth
- Difficult or prolonged labor, signs of fetal distress (asphyxia)
- Timing of jaundice onset and parental observations
- Associated symptoms (e.g., lethargy, poor feeding, decreased activity)
2. Newborn Examination:
Skin Examination:
- Yellowish or orange discoloration (indicative of indirect bilirubin increase)
- Presence of bruising, scalp bleeding (cephalhematoma), or skin infections
- Areas affected by jaundice indicate bilirubin levels:
|
Area of Jaundice |
Estimated Bilirubin Level (mg/100 ml) |
|
Head & Neck |
5 mg/100 ml |
|
Upper trunk |
10 mg/100 ml |
|
Lower trunk |
12 mg/100 ml |
|
Arms & below the knees |
12-15 mg/100 ml |
|
Hands & feet |
More than 15 mg/100 ml |
Signs of Red Blood Cell Hemolysis:
- Pale skin
- Rapid heartbeat
- Dark urine color
Signs of Bilirubin Deposits in the Brain (Kernicterus):
- Poor sucking and feeding
- Abnormal crying
- Stiff or abnormal body posture
- Altered consciousness (lethargy, stupor)
- Seizures or abnormal movements
Laboratory Tests:
- Total & direct bilirubin levels
- Blood type & Rh factor (mother and infant)
- Direct Coombs test
- Complete blood count (CBC) & red blood cell morphology
- Reticulocyte count
- G6PD enzyme deficiency test
Treatment
- Ensure adequate hydration by:
- Breastfeeding every 1-2 hours
- Administering IV fluids if necessary
- Do not stop breastfeeding
- Do not give glucose solutions orally
- Use phototherapy or exchange transfusion as prescribed by the physician
Direct Hyperbilirubinemia (Conjugated Jaundice):
This occurs due to biliary obstruction, bacterial or viral infections, or metabolic disorders. The newborn may appear greenish-yellow, and stools may be pale-colored (as seen in biliary atresia).
Note: Phototherapy is NOT recommended for direct hyperbilirubinemia
- Phototherapy Treatment
Objective:
To reduce indirect bilirubin levels by exposing the newborn to blue/white
light with a wavelength of 425-475 nm, preventing brain damage.
Effects:
Light converts insoluble bilirubin into a water-soluble form,
allowing easy excretion via urine and stool.
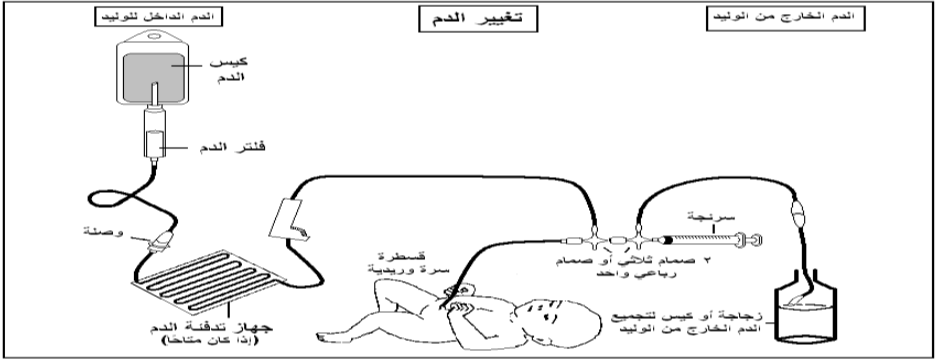
- Exchange Transfusion
Objective:
To remove excess bilirubin and replace damaged red blood cells
covered with antibodies.
Blood Requirements:
- Fresh whole blood (not packed red cells)
- Free from infectious diseases
- Less than 48 hours old
- Compatible with the mother’s blood
Post-Exchange Transfusion Procedures
- Repeat the previous steps until the required blood volume is completely exchanged.
- Periodically mix the blood to prevent red blood cell sedimentation.
- Record every step of blood withdrawal or transfusion, including the exact time and the infant’s vital signs and oxygen concentration in the exchange transfusion chart.
- Notify the doctor after every 100 ml of blood exchange.
- Immediately stop the transfusion if any signs of a blood reaction appear.
- Dispose of waste materials in designated trash bins and safety containers.
- Disinfect the heating device after turning it off.
- Perform routine handwashing after removing gloves.
- Document the procedure and all observations in the nursing records.
Post-Exchange Blood Tests & Monitoring
- Immediately collect a blood sample and send it to the laboratory for:
- Bilirubin level test
- Complete blood count (CBC)
- Calcium, sodium, and potassium levels
- Place the newborn under phototherapy.
- Monitor blood glucose levels every 4-6 hours.
- Measure bilirubin levels every 6 hours.
- Measure abdominal circumference every 6 hours for 24 hours.
- Observe for any signs of bleeding or blood in stool.
- Record all observations in the newborn’s medical file.
Responsible Personnel:
- Nursing Staff