Traumatic Brain contusions
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | جراحة مخ وأعصاب |
| كتاب: | Traumatic Brain contusions |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:01 AM |
الوصف
"last update: 13 March 2025" Download Guideline
- Executive Summary
This topic is concerned with management guidelines of traumatic cerebral contusions
Recommendations:
Initial Management:
▪️ Avoid hypoxia.
o Strong recommendation.
▪️ Avoid hypotension.
o Strong recommendation
▪️ Secure the airway (endotracheal intubation) in patients with GCS ≤8 who are unable to maintain their airway or who remain hypoxic despite supplemental O2. (if not available refer to a tertiary center)
o Strong recommendation.
▪️ Brain imaging (CT) must be available and repeated as much as needed. (if not available refer to a tertiary center)
o Strong recommendation.
▪️ We recommend ICU admission and close neurological observation with CT monitoring for the development and progression of brain stem compression. ( if not available refer to a tertiary center)
o Strong recommendation.
▪️ Follow-up head CT scan within 6 to 8 hours following brain injury must be obtained. ( if not available refer to a tertiary center)
o Strong recommendation.
▪️ The availability of equipped neurosurgery operating room is essential for management. (if not available refer to a tertiary center)
o Strong recommendation.
➡️Conservative management:
▪️ We recommend seizures prophylaxis in patients with frontal and temporal lobe cerebral contusions
o Strong recommendation
➡️Mechanisms to reduce ICP is divided into 3 tiers:
If elevation of ICP is confirmed clinically and/or radiologically or ICP monitoring (if available) the priority is control of ICP:
Tier 0
Head elevation and the same measures in the initial management
o Strong recommendation
Tier 1
▪️ We recommend mannitol for control of IC-HTN (within hospitals).
▪️ Intermittent boluses may be more effective than continuous infusion
▪️ Effective doses range from 0.25–1 gm/kg body weight
▪️ Avoid hypotension (SBP < 90mm Hg) which may result from the diuretic effect of mannitol, which can lead to decrease circulating fluid volume
o Strong recommendation.
▪️ Try to adjust partial pressure of carbon dioxide (PaCO2) at lower ranges of normal values (i.e. 35-38 mmHg).
o Conditional recommendation.
Tier 2
▪️ Consider the use of neuromuscular blocking agents (NMBAs).
o Conditional recommendation
▪️ We recommend targeting a cerebral perfusion pressure (CPP) of 60-70mm Hg
o Strong recommendation.
▪️ Try to adjust the partial pressure of CO2 at 32-35 mmHg (mild hypocapnia)
o Conditional recommendation
Tier 3
▪️ High-dose barbiturate therapy may be used for IC-HTN refractory to maximal medical and surgical ICP-lowering therapy. Patients should be hemodynamically stable before and during treatment.
o Conditional recommendation
➡️Surgical intervention: surgery may be indicated in the following indications:
▪️ Progressive neurological deterioration referable to the TICH, medically refractory IC-HTN
▪️ Signs of mass effect on CT
▪️ TICH volume > 50cm3 cc or ml
▪️ GCS = 6–8 with frontal or temporal TICH volume > 20 cm3 with midline shift ≥ 5mm and/or compressed basal cisterns on CT
o Conditional recommendation
➡️Types of surgery:
▪️ If the contusion with the surrounding edema cause mass effect according to the site you may do frontopolar lobectomy or tempropolar lobectomy
o Conditional recommendation
▪️ If the hemorrhagic contusion coalesced to form intracerebral hematoma you may do evacuation
o Conditional recommendation
▪️ Decompressive craniotomy with duroplasty may be indicated in cases in which the usual mechanisms to reduce the ICP are uneffective.
o Conditional recommendation
- Recommendations
Table 4: Conservative Management
|
Items: |
Strength of Recommendations: |
Level of evidence |
|
· Avoid hypoxia |
Strong |
Moderate quality evidance9 |
|
· Avoid hypotension |
Strong |
Moderate quality evidance9 |
|
· Secure the airway (endotracheal intubation) in patients with GCS ≤8 who are unable to maintain their airway or who remain hypoxic despite supplemental O2. (if not available refer to a tertiary center) |
Strong |
Moderate quality evidance9 |
|
· Brain imaging (CT) must be available and repeated as much as needed. (if not available refer to a tertiary center) |
Strong |
Moderate quality evidance9 |
|
· We recommend ICU admission and close neurological observation with CT monitoring for the development and progression of brain stem compression. (if not available refer to a tertiary center) |
Strong |
Moderate quality evidance9 |
|
· Follow-up head CT scan within 6 to 8 hours following brain injury must be obtained. (if not available refer to a tertiary center |
Strong |
Moderate quality evidance9 |
|
· The availability of equipped neurosurgery operating room is essential for management. (if not available refer to a tertiary center) |
Strong |
Moderate quality evidance9 |
|
· We recommend seizures prophylaxis in patients with frontal and temporal lobe cerebral contusions |
Strong |
Moderate quality evidance9 |
|
· Head elevation and the same measures in the initial management |
Strong |
Moderate quality evidance9 |
|
· We recommend mannitol for control of IC-HTN (within hospitals). ▪️ Intermittent boluses may be more effective than continuous infusion ▪️ Effective doses range from 0.25–1 gm/kg body weight ▪️ Avoid hypotension (SBP < 90mm Hg) which may result from the diuretic effect of mannitol, which can lead to decrease circulating fluid volume |
Strong |
Moderate quality evidance9 |
|
· Try to adjust partial pressure of carbon dioxide (PaCO2) at lower ranges of normal values (i.e. 35-38 mmHg). |
Conditional |
Low quality evidance9 |
|
· Consider the use of neuromuscular blocking agents (NMBAs). |
Conditional |
Moderate quality evidance9 |
|
· We recommend targeting a cerebral perfusion pressure (CPP) of 60-70mm Hg |
Strong |
High-Quality Evidence 10 |
|
· Try to adjust the partial pressure of CO2 at 32-35 mmHg (mild hypocapnia) |
Conditional |
High-Quality Evidence 10 |
|
· High-dose barbiturate therapy may be used for IC-HTN refractory to maximal medical and surgical ICP-lowering therapy. Patients should be hemodynamically stable before and during treatment. |
Conditional recommendation.
|
Moderate-Quality Evidence 10
|
Table 5: Surgical Intervention
|
Items:
|
Strength of Recommendations: |
Level of Evidence: |
|
· Surgery may be indicated in the following indications: ▪️ Progressive neurological deterioration referable to the TICH, medically refractory IC-HTN ▪️ Signs of mass effect on CT ▪️ TICH volume > 50cm3 cc or ml ▪️ GCS = 6–8 with frontal or temporal TICH volume > 20cm3 with midline shift ≥ 5mm and/or compressed basal cisterns on CT |
Conditional |
High-Quality Evidence 10 |
|
· If the contusion with the surrounding edema cause mass effect according to the site you may do frontopolar lobectomy or tempropolar lobectomy |
Conditional |
High-Quality Evidence 10 |
|
· If the hemorrhagic contusion coalesced to form intracerebral hematoma you may do evacuation |
Conditional |
High-Quality Evidence 10 |
|
· Decompressive craniectomy with duroplasty may be indicated in cases in which the usual mechanisms to reduce the ICP are uneffective |
Conditional |
High-Quality Evidence 10 |
➡️Implementation Considerations:
Training of neurosurgeons on guideline application
➡️Research gaps:
Outcome of decompressive craniectomy in patients with huge hemorrhagic contusion.
➡️Clinical / Radiological Indicators:
· Glascow coma scale (GCS) recording
· CT brain request.
➡️Updating the guideline:
To keep these recommendations up to date and ensure its validity it will be periodically updated. This will be done whenever strong new evidence is available and necessitates updating.
- Acknowledgement
Chair of the Committee:
Nasser M. F. El-Ghandour, MD
Members: (Alphabetically-arranged)
Abd-Elhafiz Shehab-Eldien, MD
Ahmed S. Kamel AbdelWahed, MD
Ahmed Zohdi, MD
Ayman Mohamed Ismail, MD
Diaa Eldin Galal Radwan, MD
Ihab El Refaee, MD
Mohamed Ahmed Hewedy, MD
Mohamed Khallaf, MD
Mohamed Salah Sedeek, MD
Omar Elwardany, MD
Osama Abdelaziz, MD
Sameh Saleh, MD
Waleed Abbass, MD
Zeiad Yossry Fayed, MD
We acknowledge Osama Ramadan for his collaboration with the committee during writing this chapter.
- Abbreviations
CT: computed tomography
CSF: cerebrospinal fluid
GOS: Glasgow outcome score
GRADE: Grading of Recommendations, Assessment, Development and Evaluation
MRV: magnetic resonance venography
TICH: traumatic intracerebral hemorrhage
WHO: world health organization
- Glossary
Brain contusion refers to a focal region of necrosis and hemorrhage, usually involving the cerebral cortex and subcortical white matter.1
- Introduction
Cerebral contusion is the classic example of focal traumatic brain injury (TBI). Before evolution of the CT, cerebral contusion could be diagnosed only in the operating room or during autopsy. Thus, contusion was considered only in cases of severe TBI and was therefore thought to be associated with severe injury.2 Since the advent of CT, contusions have commonly been observed in patients with mild and moderate TBI. It is now recognized that there is a wide range of severity associated with cerebral contusion.3
Tiny punctate contusions in patients with mild TBI have little or no clinical significance . At the other end of the spectrum, large contusions with significant mass effect in patients with severe TBI can be life-threatening and need emergent intervention.4
Contusions can be classified as coup or contrecoup injuries. Coup contusions occur at the location of impact, whereas contrecoup contusions occur on the opposite side or at a point distant from the impact.5
Frontal and temporal lobes are the most common sites for brain contusion. However, brain contusion can be present in any site in the brain.6
Contusions often enlarge during the first week after injury. Repeated CT should be considered if the patient shows clinical deterioration. 7
Surgery may be necessary to resect areas of contused brain if there is significant mass effect with raised ICP. Temporal lobe contusions are particularly ominous because of their proximity to the brainstem and risk of herniation.8
- Purpose
The purpose of this multidisciplinary guideline is to identify improvement in the diagnostic tools and treatment strategies in managing patients with cerebral contusion and to create actionable recommendations to implement these strategies in clinical practice.
- Scope
The guidelines is concerned with recommendation for traumatic brain contusion . selection of management approach (conservative - surgical) is defined. The aim is to achieve clear decision regarding each management line.
- The target audience
The guideline is intended for all neurosurgeons who are likely to diagnose and manage patients with post traumatic brain contusions, and it applies to any setting in which patients with post traumatic brain contusions would be identified, monitored, or managed.
- Methods
A comprehensive online search for guidelines and articles was undertaken to identify the most relevant articles to be reviewed and guidelines to consider for adaptation.
Inclusion/exclusion criteria followed in the search were:
▪️ Selecting only national and/or international guidelines.
▪️ Specific range of dates for publication (using Guidelines published or updated 2005 and later)
▪️ A large series none controlled, prospective clinical trials of treatment using surgical versus nonsurgical management have been reviewed.
▪️ Selecting peer reviewed publications only.
▪️ Selecting guidelines written in English language.
▪️ Papers with the following characteristics were also excluded: case series with less than 10 patients evaluated by CT scan and with incomplete outcome data (mortality or GOS (Glasgow outcome score)), case reports, operative series with operations occurring longer than 14 days from injury.
▪️ Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
▪️ Excluding guidelines published without references
▪️ Selected articles were evaluated for design, prognostic significance, therapeutic efficacy, and overall outcome.
▪️ All retrieved Guidelines were screened and appraised using the AGREE II instrument (www.agreetrust.org) by at least two members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigour dimension was retained). Subsequently. We selected:
Konar SK, Shukla D, Agrawal A. Posttraumatic brain edema: Pathophysiology, management, and current concept. Apollo Medicine. 2019 Jan 1;16(1):2-7.8
Hawryluk GW, Rubiano AM, Totten AM, O’Reilly C, Ullman JS, Bratton SL, Chesnut R, Harris OA, Kissoon N, Shutter L, Tasker RC. Guidelines for the management of severe traumatic brain injury: 2020 update of the decompressive craniectomy recommendations. Neurosurgery. 2020 Sep;87(3): 427. 9
➡️ Evidence assessment:
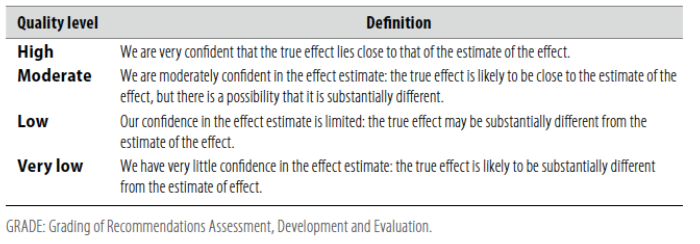
▪️ According to the WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
■ GRADE working group:https://www.gradeworkinggroup.org/
■ GRADE online training modules: http://cebgrade.mcmaster.ca/
▪️ Table 1: Quality of evidence in GRADE
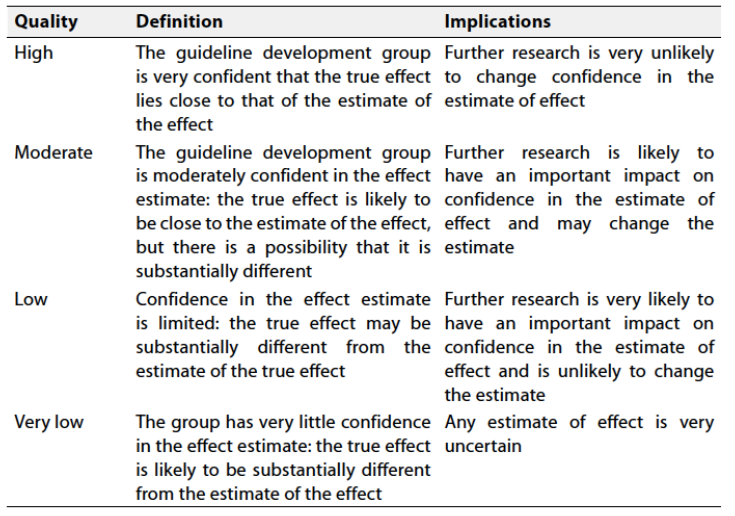
▪️Table 2: Significance of the four levels of evidence
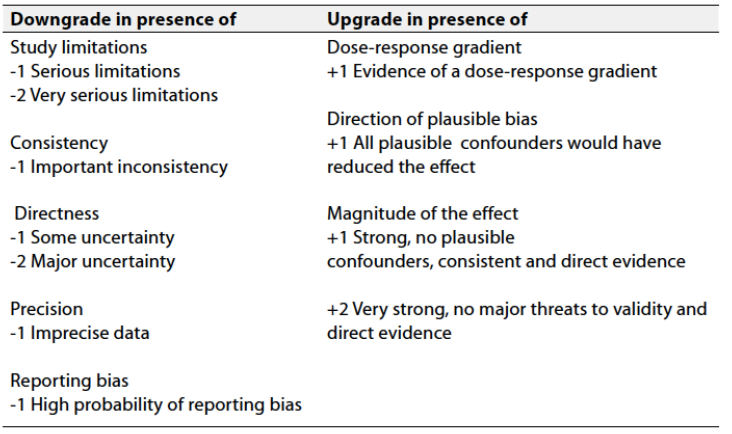
▪️ Table 3: Factors that determine How to upgrade or downgrade the quality of Evidence
- The strength of the recommendation
- The strength of a recommendation communicates the importance of adherence to the recommendation.
- Strong recommendations
- With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
- Conditional recommendations
- These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
- When not to make recommendations
- When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- References
1. Iaccarino C, Schiavi P, Picetti E, Goldoni M, Cerasti D, Caspani M, Servadei F. Patients with brain contusions: predictors of outcome and relationship between radiological and clinical evolution. Journal of neurosurgery. 2014 Apr;120(4):908-18.
2. Ragaišis V. Brain contusion: morphology, pathogenesis, and treatment. Medicina. 2002;38(3).
3. Alahmadi H, Vachhrajani S, Cusimano MD. The natural history of brain contusion: an analysis of radiological and clinical progression. Journal of neurosurgery. 2010 May 1;112(5):1139-45.
4. Zare MA, Ahmadi K, Zadegan SA, Farsi D, Rahimi-Movaghar V. Effects of brain contusion on mild traumatic brain-injured patients. International journal of neuroscience. 2012 Nov 21;123(1):65-9.
5. Adatia K, Newcombe VF, Menon DK. Contusion progression following traumatic brain injury: a review of clinical and radiological predictors, and influence on outcome. Neurocritical care. 2021 Feb; 34:312-24.
6. Bullock, M Ross; Chesnut, Randall; Ghajar, Jamshid; Gordon, David M.D.; Hartl, Roger; Newell, David W.; Servadei, Franco.; Walters, Beverly C; Wilberger, Jack. Surgical Management of Traumatic Parenchymal Lesions. Neurosurgery 58(3): p S2-25-S2-46, March 2006.
7. Robba C, Iannuzzi F, Taccone FS. Tier-three therapies for refractory intracranial hypertension in adult head trauma. Minerva Anestesiologica. 2021 Aug;87(12):1359-66.
8. Konar SK, Shukla D, Agrawal A. Posttraumatic brain edema: Pathophysiology, management, and current concept. Apollo Medicine. 2019 Jan 1;16(1):2-7.
9. Hawryluk GW, Rubiano AM, Totten AM, O’Reilly C, Ullman JS, Bratton SL, Chesnut R, Harris OA, Kissoon N, Shutter L, Tasker RC. Guidelines for the management of severe traumatic brain injury: 2020 update of the decompressive craniectomy recommendations. Neurosurgery. 2020 Sep;87(3): 427.
10. Guidelines for the Management of Severe Traumatic Brain Injury 4th Edition: Brain Trauma Foundation: September 2016.