Depressed Skull Fractures
| Site: | EHC | Egyptian Health Council |
| Course: | Neurosurgery Guidelines |
| Book: | Depressed Skull Fractures |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:51 AM |
Description
"last update: 13 March 2025" Download Guideline
- Executive Summary
This topic is concerned with management guidelines of depressed skull fractures.
➡️Recommendations
Initial Management: (as a part of initial TBI management)
▪️ Avoid hypoxia.
² Strong recommendation.
▪️ Secure the airway (endotracheal intubation) in patients with GCS ≤8 who are unable to maintain their airway or who remain hypoxic despite supplemental O2.
² Strong recommendation.
▪️ Avoid hypotension.
² Strong recommendation.
▪️ We recommend ICU admission and close neurosurgical observation with CT monitoring if needed (if not available, refer to a tertiary center).
² Strong recommendation.
▪️ The availability of equipped neurosurgery operating room is essential for management (if not available, refer to a tertiary center).
² Strong recommendation.
▪️ Anti-seizure medications (ASM):
Consider the use of ASMs (e.g., phenytoin, valproate, or carbamazepine) to decrease the incidence of early PTS (within 7 days of TBI).
² Conditional recommendation
➡️Definitive management
▪️ surgical management may be indicated in Patients with open (compound) depressed cranial fractures (evidenced by CT) with:
▪️ Depression greater than the thickness of the cranium.
▪️ Clinical (CSF leak / hernia cerebri) or radiographic (pneumocephalus) evidence of dural violation.
▪️ Underlying significant intracranial hematoma or hemorrhagic contusions.
▪️ Frontal sinus involvement.
▪️ Gross cosmetic deformity.
▪️ Wound infection.
▪️ Dural venous sinuses compromise impeding blood flow as evident in 3D CT and MRV brain.
² Conditional recommendation
▪️ Surgery may be indicated for closed depressed skull fractures if:
- the depression is causing a focal deficit through pressure on the adjacent cortex.
- the closed fracture is depressed and causing a cosmetic abnormality, for example fractures over the forehead.
² Conditional recommendation
▪️ Surgery (if indicated) is recommended as soon as possible after stabilization and coverage of umbrella of antibiotics.
² Strong recommendation
▪️ patients with open (compound) depressed cranial fractures may be treated conservatively in the absence of the previously mentioned surgical indications.
² Conditional recommendation
- Recommendations
Initial management
|
Items: |
Strength of Recommendation |
|
|
▪️ Avoid hypoxia
|
Strong |
Moderate-Quality Evidence4 |
|
▪️ Secure the airway (endotracheal intubation) in patients with GCS ≤8 who are unable to maintain their airway or who remain hypoxic despite supplemental O2 |
Strong |
Moderate-Quality Evidence4 |
|
▪️ avoid hypotension |
Strong |
Moderate-Quality Evidence4 |
|
▪️ We recommend ICU admission and close neurosurgical observation with CT monitoring if needed (if not available, refer to a tertiary center). |
Strong
|
High-Quality Evidence5 |
|
▪️The availability of equipped neurosurgery operating room is essential for management (if not available, refer to a tertiary center). |
Strong
|
High-Quality Evidence5 |
|
▪️ Antiseizure medications (ASM): Consider the use of ASMs (e.g., phenytoin, valproate, or carbamazepine) to decrease the incidence of early PTS (within 7 days of TBI). |
Conditional |
Moderate-Quality Evidence4 |
Definitive management
|
|
Strength of recommendation |
Level of evidence |
|
▪️ surgical management may be indicated in Patients with open (compound) depressed cranial fractures (evidenced by CT) with: - Depression greater than the thickness of the cranium. - Clinical (CSF leak / hernia cerebri) or radiographic (pneumocephalus) evidence of dural violation. - Underlying significant intracranial hematoma or hemorrhagic contusions. - Frontal sinus involvement. - Gross cosmetic deformity. - Wound infection. - Dural venous sinuses compromise impeding blood flow as evident in 3D CT and MRV brain. |
Conditional
|
Moderate certainty evidence2, 3
|
|
▪️ Surgery may be indicated for closed depressed skull fractures if: - the depression is causing a focal deficit through pressure on the adjacent cortex. - the closed fracture is depressed and causing a cosmetic abnormality, for example fractures over the forehead. |
Conditional
|
Moderate certainty evidence2
|
|
▪️ Surgery (if indicated) is recommended as soon as possible after stabilization and coverage of umbrella of antibiotics. |
strong |
Moderate certainty evidence2 |
|
▪️ patients with open (compound) depressed cranial fractures may be treated conservatively in the absence of the previously mentioned surgical indications. |
Conditional |
Moderate certainty evidence2 |
➡️Implementation Considerations:
training for neurosurgeons on guidelines application.
➡️Clinical / Radiological Indicators:
1) Glasgow outcome score on admission and to be repeated every 8 hours.
2) Cranial CT scan on admission to determine the site and extent of the skull fracture, associated hematoma, and to be repeated after surgery.
➡️Research Gaps
Delayed versus early skull bone reconstruction following surgery for compound depressed skull fracture.
➡️Updating the guideline
To keep these recommendations up to date and ensure its validity it will be periodically updated. This will be done whenever strong new evidence is available and necessitates updating.
- Acknowledgement
Chair of the Committee:
Nasser M. F. El-Ghandour, MD
Members: (Alphabetically-arranged)
Abd-Elhafiz Shehab-Eldien, MD
Ahmed S. Kamel AbdelWahed, MD
Ahmed Zohdi, MD
Ayman Mohamed Ismail, MD
Diaa Eldin Galal Radwan, MD
Ihab El Refaee, MD
Mohamed Ahmed Hewedy, MD
Mohamed Khallaf, MD
Mohammed Salah Sedeek, MD
Omar Elwardany, MD
Ossama Abdelaziz, MD
Sameh Saleh, MD
Waleed Abbass, MD
Zeiad Yossry Fayed, MD
- Abbreviations
ASM: Anti-seizure medications
CSF: cerebrospinal fluid
CT: computed tomography
DSF: Depressed skull fracture
GOS: Glasgow outcome score
MRV: magnetic resonance venography
PTS: post-traumatic seizure
TBI: traumatic brain injury
WHO: world health organization
- Glossary
➡️Skull fractures are classified in three ways: by pattern into (linear, comminuted, and depressed), by anatomic location into (vault, basilar), and by skin integrity into (open, and closed).
➡️Depressed skull fractures must by definition have displacement of bone greater than the full thickness of the adjacent calvarial thickness.
➡️Open fractures, by definition, have either a skin laceration over the fracture or the fracture runs through the paranasal sinuses and the middle ear structures, resulting in communication between the external environment and the cranial cavity.
➡️Pneumocephalus is the presence of air within the cranial cavity.it is usually associated with disruption of the skull: after head and facial trauma.
- Introduction
Head Trauma is a serious problem worldwide. Depressed skull fracture accounts for significant morbidity and mortality as it complicates the head injury in up to 6% subjects. Compound fractures account for up to 90%, the associated infection rate of DSF is 1.9 to 10.6%, an average neurological morbidity of approximately 11%, an incidence of late epilepsy of up to 15%, and a mortality rate of 1.4 to 19%.1
Controversy surrounds appropriate management of depressed cranial fractures. The rationale for aggressive treatment of depressed cranial fractures stems from their association with infection and late epilepsy. Cosmetic deformity also plays a role in surgical decision making. Such complications, and their potential sequelae, are well documented.2
Another challenge to traditional thinking that has surfaced in the literature involves the proper surgical management of compound depressed cranial fractures with respect to the bone fragments. Conventional treatment involves operative debridement, elevation of the fracture, removal of bone fragments, and delayed cranioplasty. However, this subjects the patient to a second operation (i.e., cranioplasty), with its attendant risks and complications.2,3
- Scope and Purpose
The purpose of this multidisciplinary guideline is to identify improvement in the diagnostic tools and treatment strategies in managing patients with depressed skull fractures and to create actionable recommendations to implement these strategies in clinical practice. This is targeting adults depressed skull fractures because Management of skull fractures in Pediatrics have special considerations (Growing skull fractures, compound elevated skull fracture, ping pong fractures).
- The target audience
The guideline is intended for all clinicians who are likely to diagnose and manage patients with depressed skull fractures, and it applies to any setting in which patients with skull fractures would be identified, monitored, or managed.
- Methods
A comprehensive online search for guidelines and articles was undertaken to identify the most relevant articles to be reviewed and guidelines to consider for adaptation.
➡️Inclusion/exclusion criteria followed in the search were:
▪️ Selecting only national and/or international guidelines.
▪️ Specific range of dates for publication (using Guidelines published or updated 2005 and later)
▪️ A large series none controlled, prospective clinical trials of treatment using surgical versus nonsurgical management have been reviewed.
▪️ Selecting peer reviewed publications only.
▪️ Selecting guidelines written in English language.
▪️ Papers with the following characteristics were also excluded: case series with less than 10 patients evaluated by CT scan and with incomplete outcome data (mortality or GOS (Glasgow outcome score)), case reports, operative series with operations occurring longer than 14 days from injury.
▪️ Selected articles were evaluated for design, prognostic significance, therapeutic efficacy, and overall outcome.
▪️ Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
▪️ Excluding guidelines published without references
➡️ The following characteristics were summarized in a table:
- Developing organization/authors
- Date of publication, posting, and release
- Country/language of publication
- Date of posting and/or release
- Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using the AGREE II instrument (www.agreetrust.org) by at least two members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigour dimension was retained). we choose for adaptation:
➡️Guidelines for the Management of Severe Traumatic Brain Injury 4th Edition: Brain Trauma Foundation: September 2016.4
➡️Evidence assessment
According to WHO handbook for Guidelines we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations.
➡️The four levels of evidence are:
- High certainty evidence
- Moderate certainty evidence
- Low certainty evidence
- Very low certainty evidence
Table (1): Quality of evidence in GRADE
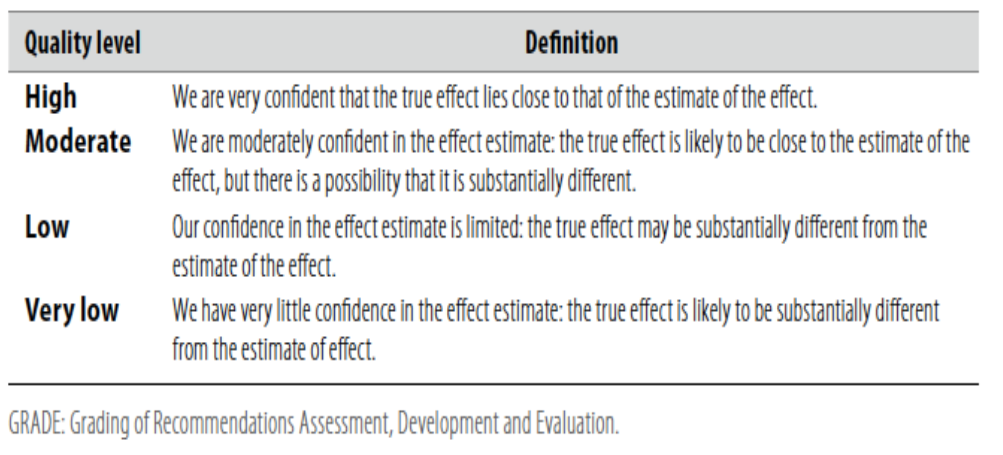

Table (2): Factors that determine How to upgrade or downgrade the quality of
Evidence.
➡️The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
➡️Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
➡️Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
➡️When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
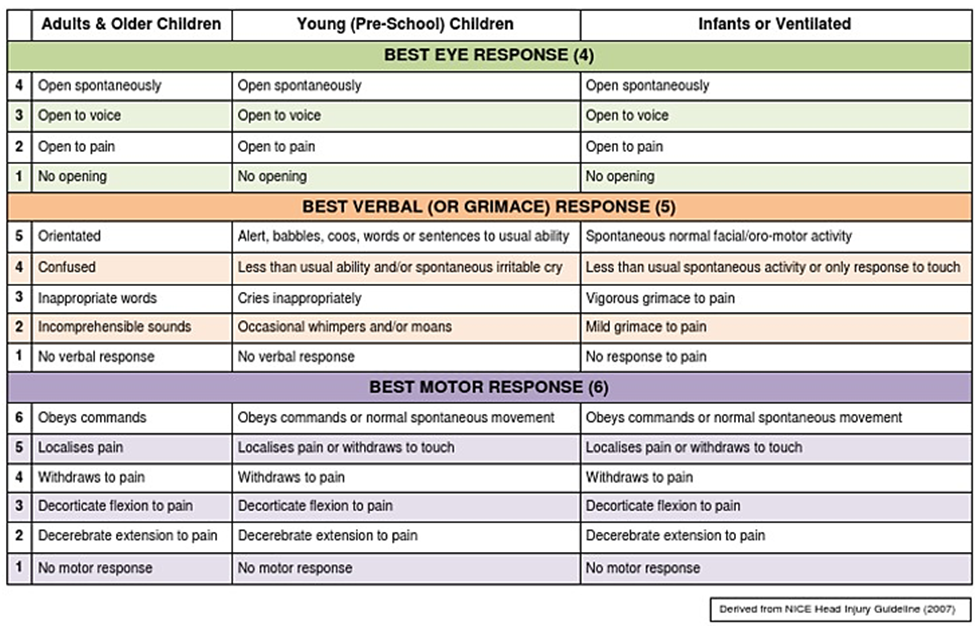
- Annexes
Glasgow Coma Scale
- References
1. Amir S: Depressed skull fracture: surgical management and outcome. In J. Med. Sci. (Peshawar, Print) July 2017, Vol. 25, No. 3.
2. Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW, et al: Surgical Management of Depressed Cranial Fractures. In Neurosurgery, 2006. 58: S2-56-S2-60.
3. Ali M, Ali L, Roghani IS: Surgical management of depressed skull fracture. J Postgrad Med Inst 2011; 17: 17-20.
4. Guidelines for the Management of Severe Traumatic Brain Injury 4th Edition: Brain Trauma Foundation: September 2016.
5. Greenberg’s Handbook of Neurosurgery: Head Trauma – General Information, Grading, Initial Management July 2022; 53: e1000–e1018.