Cough Etiquette and Respiratory Hygiene Practices
| Site: | EHC | Egyptian Health Council |
| Course: | Infection Prevention and Control Guidelines |
| Book: | Cough Etiquette and Respiratory Hygiene Practices |
| Printed by: | Guest user |
| Date: | Sunday, 26 July 2026, 10:41 AM |
Description
"last update: 20 March 2025" Download Guideline
- Executive Summary
Covering your coughs and sneezes limits the spread of germs to protect others. Handwashing with soap removes germs from your hands, making them less likely to infect your respiratory system when you touch your eyes, nose, or mouth. If soap and water are not available, using a hand sanitizer with at least 60 percent alcohol can kill these germs. To remove germs and dirt on surfaces, use household cleaners that contain soap or detergent.
|
Recommendations |
|
Educate healthcare personnel on the importance of source control measures to contain respiratory secretions to prevent droplet and fomite transmission of respiratory pathogens, especially during seasonal outbreaks of viral respiratory tract infections (e.g., influenza, RSV, adenovirus, parainfluenza virus) in communities (Strong recommendation) |
|
Implement the following measures to contain respiratory secretions in patients and accompanying individuals who have signs and symptoms of a respiratory infection, beginning at the point of initial encounter in a healthcare setting (e.g., triage, reception and waiting areas in emergency departments, outpatient clinics and physician offices): 1. Post signs at entrances and in strategic places (e.g., elevators, cafeterias) within ambulatory and inpatient settings with instructions to patients and other persons with symptoms of a respiratory infection to cover their mouths/noses when coughing or sneezing, use and dispose of tissues, and perform hand hygiene after hands have been in contact with respiratory secretions. (Good practice statement) |
|
2. Provide tissues and no-touch receptacles (e.g., foot-pedal-operated lid or open, plastic-lined waste basket) for disposal of tissues (Good practice statement) |
|
3. Provide resources and instructions for performing hand hygiene in or near waiting areas in ambulatory and inpatient settings; provide conveniently located dispensers of alcohol-based hand rubs and, where sinks are available, supplies for handwashing (Strong recommendation) |
|
During periods of increased prevalence of respiratory infections in the community, offer masks to coughing patients and other symptomatic persons (e.g., persons who accompany ill patients) upon entry into the facility or medical office and encourage them to maintain special separation, ideally a distance of at least 3 feet, from others in common waiting areas (Strong recommendation) |
- Recommendations
|
Recommendations |
|
Educate healthcare personnel on the importance of source control measures to contain respiratory secretions to prevent droplet and fomite transmission of respiratory pathogens, especially during seasonal outbreaks of viral respiratory tract infections (e.g., influenza, RSV, adenovirus, parainfluenza virus) in communities (Strong recommendation, Moderate grade evidence) |
|
Implement the following measures to contain respiratory secretions in patients and accompanying individuals who have signs and symptoms of a respiratory infection, beginning at the point of initial encounter in a healthcare setting (e.g., triage, reception and waiting areas in emergency departments, outpatient clinics and physician offices): 1. Post signs at entrances and in strategic places (e.g., elevators, cafeterias) within ambulatory and inpatient settings with instructions to patients and other persons with symptoms of a respiratory infection to cover their mouths/noses when coughing or sneezing, use and dispose of tissues, and perform hand hygiene after hands have been in contact with respiratory secretions. (Good practice statement) |
|
2. Provide tissues and no-touch receptacles (e.g., foot-pedal-operated lid or open, plastic-lined wastebasket) for disposal of tissues (Good practice statement) |
|
3. Provide resources and instructions for performing hand hygiene in or near waiting areas in ambulatory and inpatient settings; provide conveniently-located dispensers of alcohol-based hand rubs and, where sinks are available, supplies for handwashing (Strong recommendation, Moderate grade evidence) |
|
During periods of increased prevalence of respiratory infections in the community, offer masks to coughing patients and other symptomatic persons (e.g., persons who accompany ill patients) upon entry into the facility or medical office and encourage them to maintain special separation, ideally a distance of at least 3 feet, from others in common waiting areas (Strong recommendation, Moderate grade evidence) |
➡️Remarks
The elements of Respiratory Hygiene/Cough Etiquette include:
1. Education of healthcare facility staff, patients, and visitors that anyone with signs and symptoms of a respiratory infection, regardless of the cause, should follow or be instructed to follow respiratory hygiene and cough etiquette as follows:
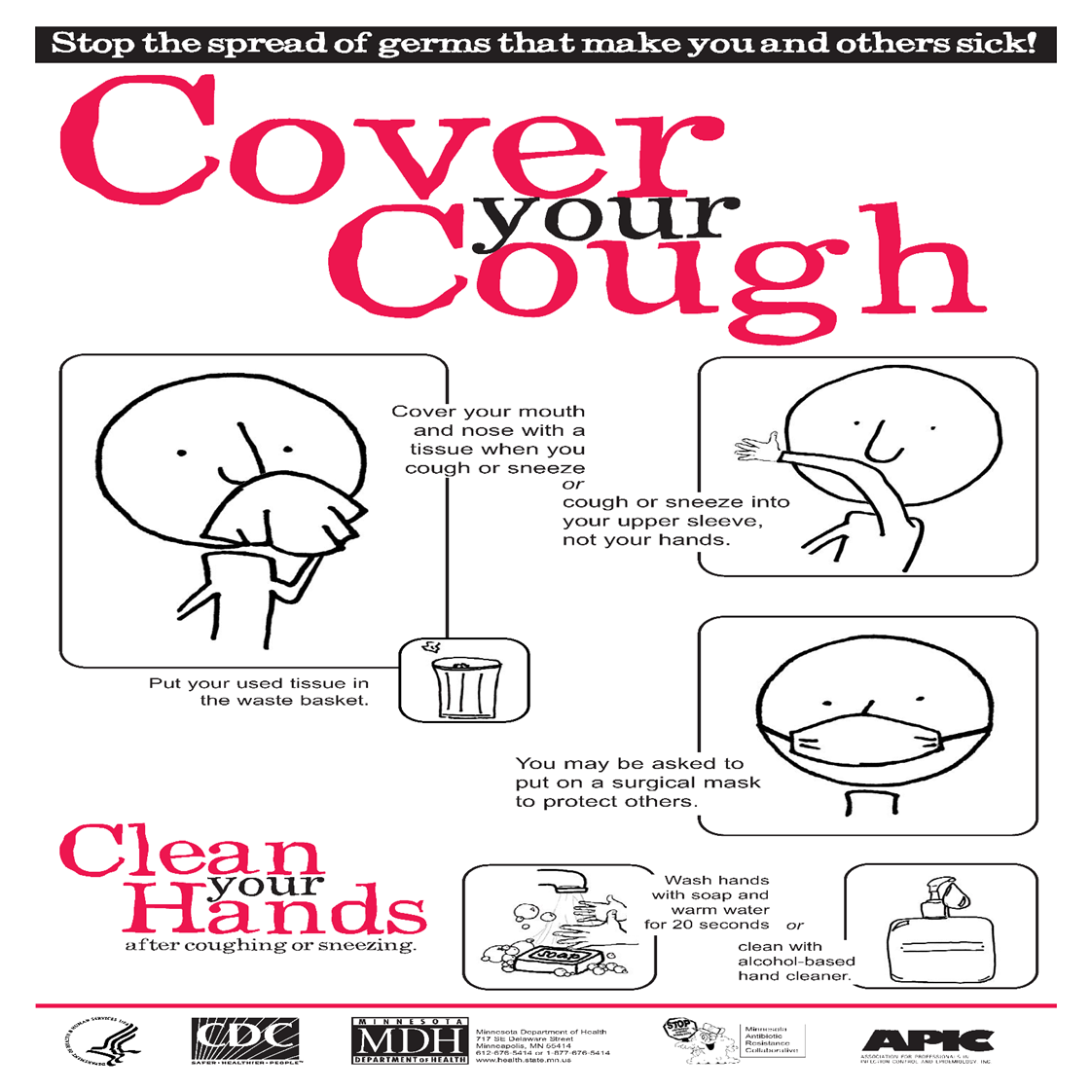
● Cover the nose/mouth with disposable single-use tissues when coughing, sneezing, wiping and blowing noses. (Annex 1. Cover your Cough, CDC)
● Use tissues to contain respiratory secretions.
● Dispose of tissues in the nearest waste receptacle or bin after use.
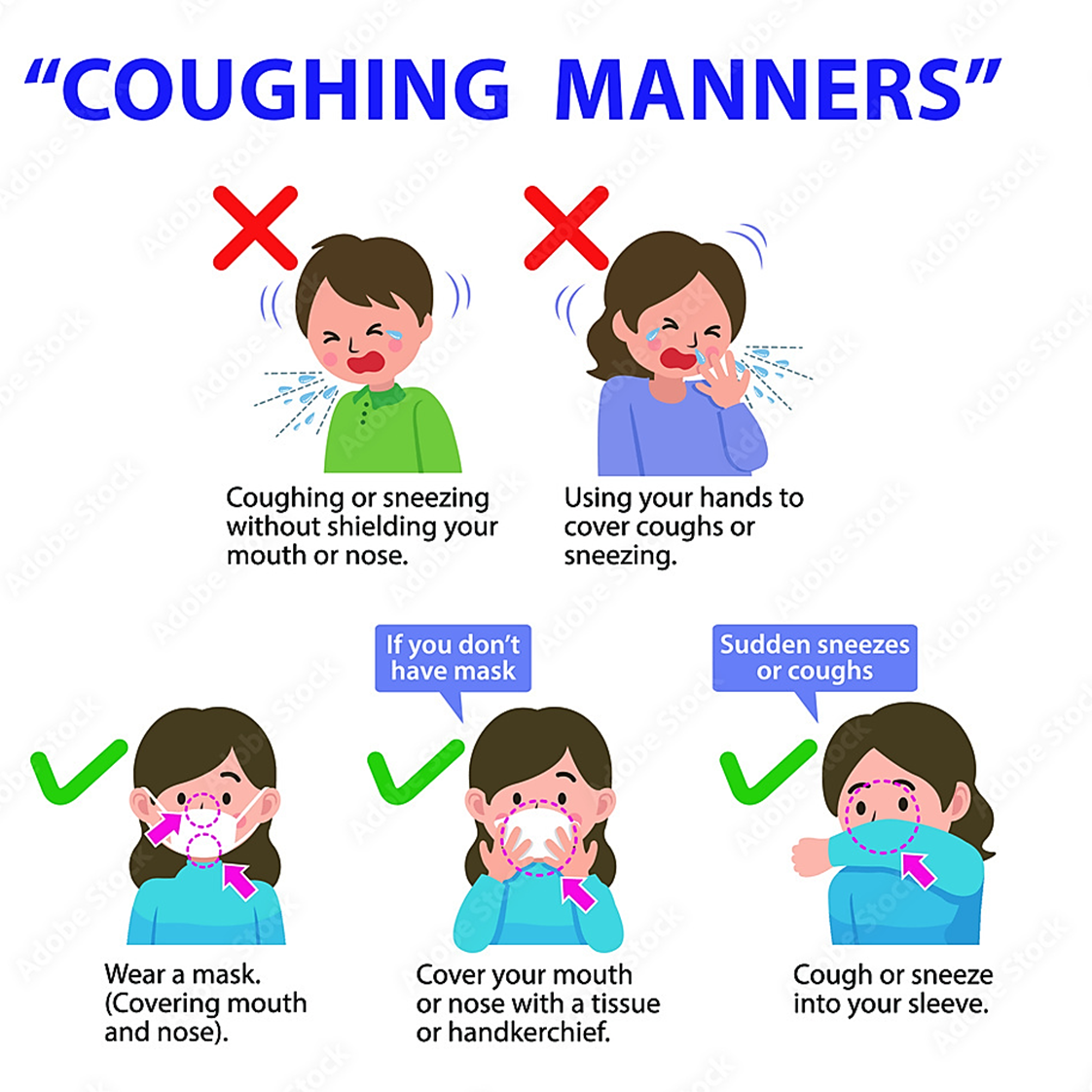
● If no tissues are available, cough or sneeze into the inner elbow rather than the hand (Annex 2. Cough manner).
● Practice hand hygiene after contact with respiratory secretions and contaminated objects/materials.
● Keep contaminated hands away from the mucous membranes of the mouth, eyes and nose.
● In healthcare facilities, patients with symptoms of respiratory infections should sit as far away from others as possible. If available, healthcare facilities may place these patients in a separate area while waiting for care.
● Healthcare workers should also assist patients (e.g. elderly, children) who need assistance with containment of respiratory secretions. Those who are immobile will need a receptacle (e.g. plastic bag) readily at hand for the immediate disposal of used tissues and will need to be offered hand hygiene facilities.
2. Posted signs, in language(s) appropriate to the population served, with instructions to patients and accompanying family members or friends.
3. Source control measures (e.g., covering the mouth/nose with a tissue when coughing and prompt disposal of used tissues, using surgical masks on the coughing person when tolerated and appropriate)
4. Hand hygiene after contact with respiratory secretions.
5. Spatial separation, ideally equal or more than 3 feet (1 meter) of persons with respiratory infections in common waiting areas when possible.
Covering sneezes and coughs and placing masks on coughing patients are proven means of source containment that prevent infected persons from dispersing respiratory secretions into the air. These measures should be effective in decreasing the risk of transmission of pathogens contained in large respiratory droplets (e.g., influenza virus, adenovirus, B. pertussis and Mycoplasma pneumoniae).
Hands can become contaminated through contact with respiratory secretions when coughing or sneezing. Contaminated hands can lead to the cross-transmission of infectious agents in non-outbreak situations. The patient and visitors should also be aware of their role in minimizing risks by being instructed on how to perform hand hygiene after coughing or contact with respiratory secretions.
Healthcare personnel are advised to observe Droplet Precautions (i.e., wear a mask) and hand hygiene when examining and caring for patients with signs and symptoms of a respiratory infection.
Healthcare personnel who have a respiratory infection are advised to avoid direct patient contact, especially with high-risk patients. If this is not possible, then a mask should be worn while providing patient care.
1.2 Indicators for Monitoring
Cough etiquette is assessed among elements of standard precautions during audit. Presence of posters, hand sanitizers, tissues, masks and waste bins are an indicator of proper implementation.
1.3 Plan to Update this National Clinical Guideline
This guideline will be reviewed and updated when new
evidence emerges that is likely to influence the recommendations.
- Acknowledgements
We would like to acknowledge the Infection Control Guidelines Committee for developing these guidelines.
Head of IPC Guidelines Committee
Professor Ghada Ismail (Professor of Clinical Pathology (Clinical Microbiology), Faculty of Medicine, Ain Shams University, Secretary of Supreme IPC Committee, SCHUH, Member of WHO Global Guidelines Groups (GDG) for Infection Prevention)
Secretary of IPC Guidelines Committee
Professor Walaa Abd El-Latif (Professor of Medical Microbiology and Immunology, Faculty of Medicine Ain Shams University, IPC Consultant)
Members of the Committee
▪ Professor Amal Sayed (Deputy Manager of Environmental Affair, Infection Control Director, Cairo University Hospitals)
▪ Professor Amani El-Kholy (Clinical Pathology Department (Microbiology), Faculty of Medicine, Cairo University, Infection Control Consultant)
▪ Dr Asmaa Mohamed Abdelfatah Mohamed (Lecturer, Faculty of Nursing MTI University)
▪ Dr Gehan Mohamed Fahmy (Professor clinical microbiology ASUSH consultant infection control, Board member of IFIC EMERO region)
▪ Professor Hebatallah Gamal Rashed (Clinical Pathology Department (Microbiology), Faculty of Medicine, Assiut University, Infection Control Consultant)
▪ Dr Iman Afifi (Consultant Clinical Pathology (Microbiology) and IPC, Ain Shams University, Director IPC units of Ain Shams internal medicine and Geriatric hospitals
▪ Professor Maha El Touny (Department of internal medicine. Faculty of Medicine, Ain Shams University. Infection Control Consultant)
▪ Professor Nagwa Khamis (Emeritus Consultant Clinical Pathology (Microbiology) and IPC, ASU Director IPC Department and CEO Consultant IPC, CCHE-57357)
▪ Professor Nesrine Fathi Hanafi (Professor in Medical Microbiology and Immunology Faculty of Medicine Alexandria University, Head of Infection Prevention and Control, Alexandria University Hospitals)
▪ Dr. Reham Lotfy Abdel Aziz (Environmental Health Director, EEAA, Hazardous Waste Consultant, WMRA, Ministry of Environment)
▪ Professor Sherin ElMasry (Professor of Clinical Pathology, Ain Shams University, Chief Director of IPC ASU, Health Care Quality & Patient Safety Consultant)
▪ Dr Shimaa El-Garf (Coordinator): Clinical Pathology Specialist, Coordinator of HAI Surveillance and Audit Electronic System for University Hospitals, RLEUH- SCUH
- Glossary
1.1.1 Cluster: An aggregation of cases grouped in place and time that
are suspected to be greater than the number expected ,even though the expected
number may not be known.
1.1.2 Cough
etiquette/respiratory hygiene: Measures that are taken to minimize the spread of
respiratory infections to others.
1.1.3 Infectious agent: Any
organism, such as a virus, parasite, bacterium or fungus, that is capable of
causing an infection or infectious disease.
1.1.4
Outbreak:
Occurrence of cases of disease that is more than expected, or cases
clustered by time, space, or common behaviors.
1.1.5 Secretions: Any
bodily fluid that is produced by a cell
or gland, e.g saliva, or mucous, for a particular function in the organism or
for excretion e.g urine.
1.1.6 Source control: Source control refers to use of well-fitting
masks to cover a person’s mouth and nose to prevent spread of respiratory
secretions when they are breathing, talking, sneezing, or coughing.
- Abbreviations
1.1.1 CDC: Centers for Disease Control and Prevention
1.1.2 COVID-19: Coronavirus disease of 2019
1.1.3 RSV: Respiratory Syncytial Virus
1.1.4 WHO: World Health Organization
- Introduction
Cough
etiquette and respiratory hygiene are elements of the infection prevention and
control standard precautions, and they are essential practices that help
prevent the spread of respiratory infections, such as the flu, common cold, and
more serious diseases like COVID-19 etc.
These
practices involve simple actions that can significantly reduce the transmission
of harmful germs to others in public spaces, workplaces, and at home. Proper
cough etiquette includes covering the mouth and nose when coughing or sneezing,
using tissues or the elbow to contain respiratory droplets, and disposing of
tissues properly. Respiratory hygiene also emphasizes regular handwashing,
wearing masks when appropriate, and maintaining good personal hygiene. By
adopting these habits, individuals can play an active role in reducing the
spread of infectious diseases and promoting public health, particularly in
crowded or high-risk environments.
- Scope and Purpose
1.1.1 Scope of Cough Etiquette and Respiratory Hygiene
Cough etiquette should be applied by all attendees to
healthcare settings staff, public and community.
1.1.2 Purpose of Cough Etiquette and Respiratory Hygiene
The primary purpose of cough etiquette and respiratory hygiene is
to prevent the spread of respiratory infections and protect public health.
These practices are designed to reduce the transmission of harmful pathogens,
such as viruses and bacteria, that are commonly spread through coughing,
sneezing, and other respiratory actions. By following
these practices, individuals can minimize their risk of becoming infected and
help reduce the burden on healthcare systems:
1.1.2.1 Preventing the Spread of Infectious Diseases: Respiratory infections are highly contagious and primarily transmitted through respiratory droplets. Proper cough etiquette and respiratory hygiene, including covering the mouth and nose, disposing of tissues correctly, and washing hands, help to contain and reduce the spread of these droplets, thus limiting the transmission of pathogens.
1.1.2.2 Protecting Vulnerable Populations: practicing good respiratory hygiene is to safeguard these vulnerable populations from exposure to harmful pathogens. By reducing transmission in the community, the risk to these high-risk groups is significantly diminished.
1.1.2.3 Reducing the Burden on Healthcare Systems: The widespread transmission of respiratory infections can overwhelm healthcare systems, leading to increased hospitalizations, emergency visits, and healthcare resource demands. Following cough etiquette and respiratory hygiene practices can reduce the overall incidence of infection, preventing healthcare facilities from becoming overloaded. This is especially critical during flu seasons or in the event of a respiratory pandemic.
1.1.2.4 Limiting the Spread in Crowded or Shared Spaces: Respiratory infections can spread quickly in crowded environments, such as schools, public transportation, workplaces, and healthcare settings. Cough etiquette and respiratory hygiene serve to protect individuals in these spaces by minimizing the airborne spread of germs. For example, covering coughs, wearing masks, and maintaining good hand hygiene can significantly reduce the likelihood of infecting coworkers, classmates, or the general public.
1.1.2.5 Promoting Personal and Public Hygiene: By emphasizing the importance of handwashing, covering coughs, and using tissues, these practices foster a culture of health-conscious behavior. Over time, this leads to broader societal benefits, such as reduced absenteeism in schools and workplaces, improved quality of life, and lower overall healthcare costs.
1.1.2.6 Preventing Cross-Contamination in Healthcare Settings: In healthcare environments, where patients may already be suffering from compromised health, it is crucial to prevent the spread of infection between patients, healthcare workers, and visitors.
1.1.2.7 Supporting Global Health Efforts: On a larger scale, proper cough etiquette and respiratory hygiene contribute to global health initiatives aimed at controlling the spread of infectious diseases. During outbreaks or pandemics, such as COVID-19, these practices play a vital role in controlling the transmission of the virus, slowing the spread, and preventing widespread illness.
1.1.2.8 Enhancing Public Awareness: One of the key purposes of cough etiquette and respiratory hygiene is to educate individuals about how easily respiratory infections are transmitted and the simple measures they can take to protect themselves and others.
- Target Audience
All Healthcare setting staff
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
● Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
● Selecting only national and/or international guidelines
● Specific range of dates for publication (using Guidelines published or updated in 2013 and later)
● Selecting peer reviewed publications only
● Selecting guidelines written in English language
● Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input.
● Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations.
The following characteristics of the retrieved guidelines were summarized in:
● Developing organization/authors
● Date of publication, posting, and release
● Country/language of publication
● Date of posting and/or release
● Dates of the search used by the source guideline developers.
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The committee decided to adapt from:
1. CDC Hygiene and Respiratory Viruses Prevention March 1, 2024
2. CDC Cough Etiquette and Respiratory Hygiene [Fact Sheet], 2023
3. CDC Summary of Recommendations Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings (2007) November 27, 2023
➡️Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
● GRADE working group: https://www.gradeworkinggroup.org/
● GRADE online training modules: http://cebgrade.mcmaster.ca/
Table (1) Quality and Significance of the four levels of evidence in GRADE
|
Quality |
Definition |
Implications |
|
High |
The guideline development group is very confident that the true effect lies close to that of the estimate of the effect |
Further research is very unlikely to change confidence in the estimate effect |
|
Moderate |
The guideline development group is moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibly that it is substantially different |
Further research is likely to have an important impact on confidence in the estimate of the effect and may change the estimate |
|
Low |
Confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the true effect |
Further research is very likely to have an important on confidence in the estimate of effect and is unlikely to change the estimate |
|
Very low |
The group has very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of the effect |
Any estimate of the effect is very uncertain |
Table (2) Factors that determine How to upgrade or downgrade the quality of evidence.
|
Downgrade in presence of |
Upgrade in presence of |
|
Study limitations. 1- Serious limitations 2- Very serious limitations |
Dose- response gradient. +1 Evidence of a dose-response gradient |
|
Consistency 1- Important inconsistency |
Direction of plausible bias + All plausible confounders would have reduced the effect |
|
Directness 1- Some uncertainty 2- Major uncertainty |
Magnitude of the effect +1 Strong, no plausible Confounder, consistent and direct evidence |
|
Precision 1- Imprecise data |
+2 very strong, no major threats to validity and direct evidence |
|
Reporting bias 1- High probability of reporting bias |
|
➡️The strength of the recommendations
The strength of a recommendation communicates the importance of adherence to the recommendation.
● Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
● Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations?
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Annexes
Annex 1. Cover your Cough, CDC
Annex 2. Coughing Manners
- References
- Centers for Disease Control and Prevention (CDC). Hygiene and Respiratory Viruses Prevention (2024). Available at: https://www.cdc.gov/respiratory-viruses/prevention/index.html.
- Centers for Disease Control and Prevention (CDC). Cough Etiquette and Respiratory Hygiene, Fact Sheet (2023). Available at: https://www.cdc.gov.
- Centers for Disease Control and Prevention (CDC). Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings (2023). Available at: https://www.cdc.gov/infection-control/media/pdfs/Guideline-Isolation-H.pdf.
- World Health Organization (WHO). COVID-19: How to Protect Yourself and Others. (2020). Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
- National Health and Medical Research Council (nhmrc). Australian Guidelines for the Prevention and Control of Infection in Healthcare (2019). Available at: https://www.nhmrc.gov.au/about-us/publications/australian-guidelines-prevention-and-control-infection-healthcare-2019