Management of Anal Fissures
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | Management of Anal Fissures |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:01 AM |
Description
"last update: 12 May 2025 Download Guideline
- Executive Summary
This guideline offers evidence-based recommendations on the targeted levels of Clinical practice guidelines and provide healthcare professionals with practical guidance on the diagnosis and treatment of anal fissure.
· Non-operative treatment of acute anal fissures continues to be safe, has few side effects, and should typically be recommended as the first-line treatment, (Strong recommendation).
· Treatment of anal fissures with topical nitrates is recommended, although side effects may limit their efficacy, (Strong recommendation).
· The use of calcium channel blockers for chronic anal fissures has a similar efficacy to topical nitrates, with a superior side effect profile, and can be recommended as first-line treatment, (Strong recommendation).
· We recommend Botulinum toxin as second-line therapy following treatment with topical therapies in treatment of chronic anal fissure, (Conditional recommendation).
· We recommend internal sphincterotomy, (IS) in the treatment of chronic anal fissures as first line of treatment or as a second line of treatment after failure of medical treatment, (Strong recommendation).
· Laser therapy is not routinely recommended for the treatment of anal fissures due to limited evidence supporting its efficacy in this context, (Good practice statement).
· We recommend to repeat IS or botulinum toxin injection for recurrent anal fissure, (conditional recommendation).
· In recurrent anal fissure the use of an ano-cutaneous flap may be recommended to decreases postoperative pain and allows for primary wound healing, (conditional recommendation).
· In the presence of multiple anal fissures or abnormal sites of fissure or recurrent fissure, we recommend excluding other causes of anal fissure: such as Crohn’s disease or sexually transmitted diseases, (conditional recommendation).
- Recommendations
Section1. Non-operative treatment of acute anal fissures:
· Non-operative treatment of acute anal fissures continues to be safe, has few side effects, and should typically be recommended as the first-line treatment, (Strong recommendation, moderate certainty evidence(6)).
Section2: Treatment of chronic anal fissures:
· Treatment of anal fissures with topical nitrates is recommended, although side effects may limit their efficacy, (Strong recommendation, high certainty evidence (6)).
· The use of calcium channel blockers for chronic anal fissures has a similar efficacy to topical nitrates, with a superior side effect profile, and can be recommended as first-line treatment, (Strong recommendation, high certainty evidence(6) ).
Section3: Botulinum toxin
· We recommend Botulinum toxin as second-line therapy following treatment with topical therapies in treatment of chronic anal fissure, (Conditional recommendation, very low certainty evidence (6)).
Section4: Surgical treatment of anal fissures:
· We recommend internal sphincterotomy, (IS) in the treatment of chronic anal fissures as first line of treatment or as a second line of treatment after failure of medical treatment, (Strong recommendation, high certainty evidence (6)).
Section 5: Laser fissurectomy
· Laser therapy is not routinely recommended for the treatment of anal fissures due to limited evidence supporting its efficacy in this context, (Good practice statement).
Section 6: Recurrent chronic anal fissures:
· We recommend to repeat IS or botulinum toxin injection for recurrent anal fissure, (conditional recommendation, low certainty evidence (6)).
· In recurrent anal fissure the use of an ano-cutaneous flap may be recommended to decreases postoperative pain and allows for primary wound healing, (conditional recommendation, low certainty evidence (6)).
Section 7: Miscellaneous causes of anal fissures:
· In the presence of multiple anal fissures or abnormal sites of fissure or recurrent fissure, we recommend to exclude other causes of anal fissure: such as Crohn’s disease or sexually transmitted diseases, (conditional recommendation, low certainty evidence (6)).
- Acknowledgement
We would like to acknowledge the guideline general surgery, (GGS) committee for developing this guideline.
Chair of GGS: Abel Motey Hussein Aly; professor of surgery, Cairo University.
Moderator of GGS: Mostafa Abdel Hamed Soliman; professor of surgery, Cairo University.
Members of GGS:
Abdelwahab Mohamed Ezzat; professor of surgery, Ain Shams University.
Ahmed Abdel Raouf Elgeidie; professor of digestive surgery, Mansoura University.
Alaa Abdallah; professor of surgery, Ain Shams University.
Atef Abdelghani Salem; professor of surgery, Benha University.
Hesham Abdel Raouf Elakad; professor of surgery, Ain Shams University.
Khaled Abdallah Elfiky; professor of surgery, Ain Shams University.
Khaled Amer; professor of surgery, Military medical academy.
Khaled Safwat; professor of surgical oncology and endoscopy, Zagazig University.
Ibrahim Elzayat; head of surgery department, Aswan University.
Mohamed Ali Mohamed Nada, professor of surgery, Ain Shams University.
Mohamed Ibrahim Abdel Hamed Alsaid, professor of surgery, Zagazig University.
Tarek Ibrahim; professor of surgery, National liver institute Menofia University.
- Abbreviations
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
GGS |
Guideline General Surgery. |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation. |
|
IBD |
Irritable Bowel Disease. |
|
IS |
Internal Sphincterotomy. |
|
LIS |
Lateral Internal Sphincterotomy. |
|
PIS |
Posterior Internal Sphincterotomy. |
- Glossary
Acute fissures: defined as symptoms present for fewer than 8 weeks, will appear as a longitudinal tear.
Chronic fissures: (of a longer duration), will manifest one or more stigmata of chronicity, including a hypertrophied anal papilla at the proximal aspect of the fissure, a sentinel tag at the distal aspect of the fissure, and exposed internal anal sphincter muscle within the base of the fissure.
- Introduction
The term anal fissure most commonly refers to a longitudinal tear within the anal canal, one that typically extends from the dentate line toward the anal verge. This benign anorectal ailment is quite common, although there have been virtually no published population-level data describing its incidence, (1). Constipation and diarrhea are frequent antecedent historical features. The primary symptom associated is anal pain, which is often provoked by defecation and may last for several hours following defecation. Anorectal bleeding may also be associated with fissures, and, when this symptom is present, it can contribute to a misdiagnosis of symptomatic hemorrhoids. (2)
Anal fissure may be treated medically or surgically. The ultimate judgment regarding the propriety of any specific procedure must be made by the physician in light of all the circumstances presented by the individual patient, (3 & 4).
Up to 90% of cases, the anal fissure is located within the posterior midline of the anal canal. Fissures are located in the anterior midline in as many as 25% of female patients and in as many as 8% of male subjects. In3% of patients, fissures can be located at posterior and anterior positions simultaneously.
Fissures located at lateral locations within the anal canal, and multiple fissures, are considered to be atypical and require careful evaluation because of their association with such diseases as HIV infection, Crohn’s disease, syphilis, tuberculosis, and hematologic malignancies (5).
- Scope and Purpose
The scope of this guideline is who to diagnose and treat anal fissure.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
➡️Target Audience:
The principle targeted audiences are the practicing surgeons.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GGS decided to adapt update of the Clinical Practice Guidelines Committee of the American society of Colon and Rectal surgeons, 20
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org/
· GRADE online training modules: http://cebgrade.mcmaster.ca/
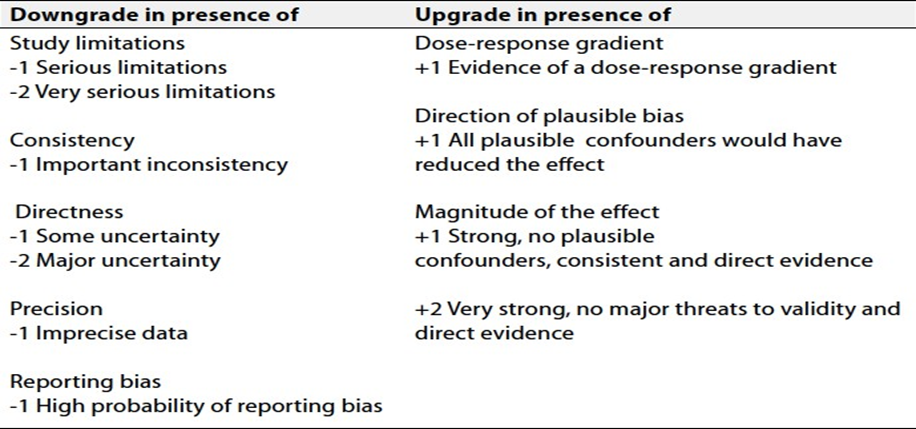
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1 & 2).
➡️The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
➡️Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
➡️Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
➡️When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research Needs
Non operative methods to treat anal fissure.
- Clinical Indicators for Monitoring
1) Documentation of the type and site of fissure.
2) Documentation of the type of non-surgical treatment, (topical nitroglycerin, nifedipine or botulinum toxin).
3) Documentation of the type of operation, (LIS, PIS, Flap).
- Updating of the Guidelines
The GGS committee for guidelines development is responsible for the continuous evaluation of evidence available about anal fissure. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Quality and Significance of the four levels of evidence in GRADE:
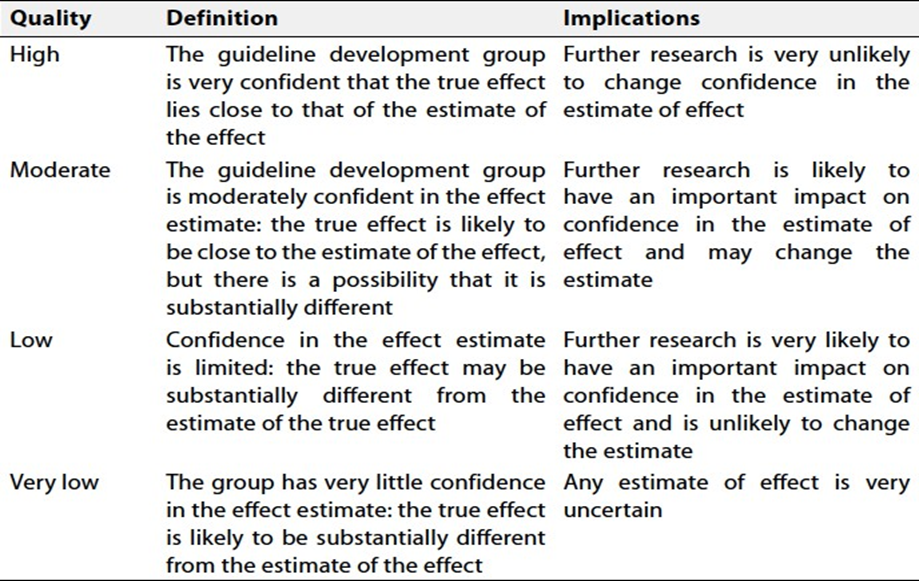
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
- References
1. Shub,HA; Salvati,EP and Rubin,RI: Conservative treatment of anal fissure: an unselected retrospective and continuous study. Dis Colon Rectum. 1972; 21:582-583.
2. Berry,SM; Barish,CF; Bhandari,R et al. Nitroglycerine 0.4% ointment vs placebo in the treatment of pain resulting from chronic anal fissure: A randomized double-blind placebo-controlled study. BMC Gastroenterol. 2013;13:106.
3. Lysy,J; Israeli,E; Rozentzweig,G; Struss-Liviatan,N and Golden,E. Long term results of chemical sphincterotomy for chronic anal fissure: a prospective study. Dis Colon Rectum. 2006; 49:858-864.
4. Richard,CS; Gregoire,R; Plewes,EA et al. Internal shincterotomy is superior to topical nitroglycerin in the treatment of chronic anal fissure results of randomized controlled trial by the Canadian Colorectal Surgical Trials Group. Dis Colon Rectum. 2000;43:1048-1057.
5. D,Ugo,S; Franceschilli,L; Cadeddu,F et al. Medical and surgical treatment of haemorrhoids and anal fissure in Crohn,s disease: a critical appraisal. BMC Gastroenterol. 2013;13:47
6. David B. Stewart, Sr., M.D. • Wolfgang Gaertner, M.D. • Sean Glasgow, M.D. John Migaly, M.D. • Daniel Feingold, M.D. • Scott R. Steele, M.D. Prepared on behalf of the Clinical Practice Guidelines Committee of the american society of Colon and Rectal surgeons Diseases of the Colon & ReCtum Volume 60: 1 (2017).