Acute Appendicitis
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | Acute Appendicitis |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:02 AM |
Description
"last update: 12 May 2025 Download Guideline
- Executive Summary
This guideline offers evidence-based recommendations on the targeted levels of Clinical practice guidelines and provide healthcare professionals with practical guidance on the diagnosis and treatment of acute appendicitis, (AA).
· We recommend to adopt a tailored individualized diagnostic approach for stratifying the risk and disease probability and planning an appropriate stepwise diagnostic pathway in patients with suspected acute appendicitis, depending on age, sex, and clinical signs and symptoms of the patient, (Strong recommendation).
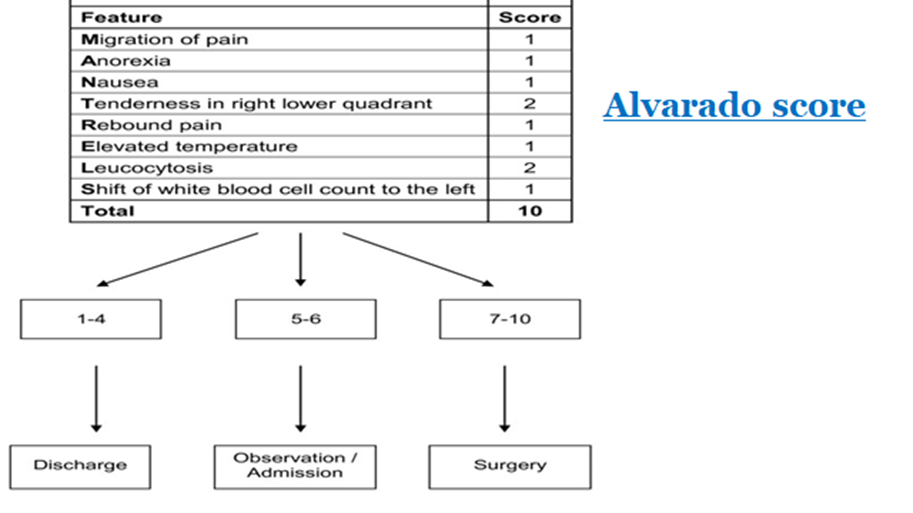
· We recommend the use of clinical scores, (Alvarado score and the new Adult Appendicitis Score) to exclude acute appendicitis and identify intermediate-risk patients needing of imaging diagnostics, (Strong recommendation).
· We recommend the use of biochemical markers as a diagnostic tool for the identification of both negative cases and complicated acute appendicitis in adults, (good practice statement).
· We recommend POCUS (point of care ultrasound) as the most appropriate first-line diagnostic tool in both adults and children, if an imaging investigation is indicated based on clinical assessment, (Strong recommendation).
· We recommend the routine use of a combination of clinical parameters and US to improve diagnostic sensitivity and specificity and reduce the need for CT scan in the diagnosis of acute appendicitis, (Strong recommendation).
· We recommend CT before surgery for patients with normal investigations but non-resolving right iliac fossa pain, (Strong recommendation).
· After negative imaging, initial non-operative treatment may be recommended, (conditional recommendation).
· Explorative laparoscopy is recommended to establish/exclude the diagnosis of acute appendicitis or alternative diagnoses, in patients with progressive or persistent pain, (Strong recommendation).
· We suggest graded compression trans-abdominal ultrasound as the preferred initial imaging method for suspected acute appendicitis during pregnancy, (conditional recommendation).
· We suggest MRI in pregnant patients with suspected appendicitis, if this resource is available, after inconclusive US, (conditional recommendation).
· We recommend discussing NOM with antibiotics as a safe alternative to surgery in selected patients with uncomplicated acute appendicitis and absence of appendicolith, advising of the possibility of failure and misdiagnosing complicated appendicitis, (conditional recommendation).
· We suggest against treating acute appendicitis non-operatively during pregnancy until further high-level evidence is available, (conditional recommendation).
· In the case of NOM, we recommend initial intravenous antibiotics with a subsequent switch to oral antibiotics based on patient's clinical conditions, (Strong recommendation).
· We recommend planning open or laparoscopic appendectomy for the next available operating list within 24 h in case of uncomplicated acute appendicitis, minimizing the delay wherever possible, (Strong recommendation).
· We recommend against delaying appendectomy for acute appendicitis needing surgery beyond 24 h from the admission, (Strong recommendation).
· We recommend laparoscopic appendectomy as the preferred approach over open appendectomy for both uncomplicated and complicated acute appendicitis, where laparoscopic equipment and expertise are available, (Strong recommendation).
· We recommend laparoscopic appendectomy in obese patients, older patients, and patients with high peri- and postoperative risk factors, (conditional recommendation).
· We suggest laparoscopic appendectomy in pregnant patients in the first and second trimesters instead of opens appendectomy when surgery is indicated (conditional recommendation).
· We recommend protection of the edges of the wound by ring protectors in open appendectomy to decrease the risk of SSI, (Strong recommendation).
· We recommend primary skin closure with a unique absorbable intradermal suture for open appendectomy wounds, (conditional recommendation).
· We recommend performing suction alone in complicated appendicitis patients with intra-abdominal collections undergoing laparoscopic appendectomy, (Strong recommendation).
· We suggest appendix removal if the appendix appears “normal” during surgery and no other disease is found in symptomatic patients, (conditional recommendation).
· We suggest the open or laparoscopic approach as treatment of choice for patients with complicated appendicitis with phlegmon or abscess, (conditional recommendation).
· We recommend routine histopathology after appendectomy, (conditional recommendation).
- Recommendations
1. Clinical scores for acute appendicitis
· We recommend to adopt a tailored individualized diagnostic approach for stratifying the risk and disease probability and planning an appropriate stepwise diagnostic pathway in patients with suspected acute appendicitis, depending on age, sex, and clinical signs and symptoms of the patient, (Strong recommendation, moderate certainty evidence, (4)).
· We recommend the use of clinical scores, (Alvarado score and the new Adult Appendicitis Score) to exclude acute appendicitis and identify intermediate-risk patients needing of imaging diagnostics, (Strong recommendation, high certainty evidence, (4)).
2. What is the role of serum biomarkers in evaluating patients presenting with clinical features evocative of acute appendicitis:
· We recommend the use of biochemical markers as a diagnostic tool for the identification of both negative cases and complicated acute appendicitis in adults, (good practice statement, low certainty evidence (6)).
3. Should abdominal CT versus ultrasonography be used for diagnosing acute appendicitis?
· We recommend POCUS (point of care ultrasound) as the most appropriate first-line diagnostic tool in both adults and children, if an imaging investigation is indicated based on clinical assessment, (Strong recommendation, moderate certainty evidence, (6)).
· We recommend the routine use of a combination of clinical parameters and US to improve diagnostic sensitivity and specificity and reduce the need for CT scan in the diagnosis of acute appendicitis, (Strong recommendation, moderate certainty evidence, (6)).
4. Unresolved RT iliac fossa pain:
· We recommend CT before surgery for patients with normal investigations but non-resolving right iliac fossa pain, (Strong recommendation, moderate certainty evidence, (4)).
· After negative imaging, initial non-operative treatment may be recommended, (conditional recommendation, moderate certainty evidence, (6)).
· Explorative laparoscopy is recommended to establish/exclude the diagnosis of acute appendicitis or alternative diagnoses, in patients with progressive or persistent pain, (Strong recommendation, high certainty evidence, (4)).
5. Acute appendicitis with pregnancy:
· We suggest graded compression trans-abdominal ultrasound as the preferred initial imaging method for suspected acute appendicitis during pregnancy, (conditional recommendation, very low certainty evidence, (6)).
· We suggest MRI in pregnant patients with suspected appendicitis, if this resource is available, after inconclusive US, (conditional recommendation, moderate certainty evidence, (6)).
6. Should adult patients with acute, uncomplicated appendicitis be managed nonoperatively versus operatively?
· We recommend discussing NOM with antibiotics as a safe alternative to surgery in selected patients with uncomplicated acute appendicitis and absence of appendicolith, advising of the possibility of failure and misdiagnosing complicated appendicitis, (conditional recommendation, high certainty evidence, (4)).
· We suggest against treating acute appendicitis non-operatively during pregnancy until further high-level evidence is available, (conditional recommendation, very low certainty evidence, (4)).
· In the case of NOM, we recommend initial intravenous antibiotics with a subsequent switch to oral antibiotics based on patient's clinical conditions, (Strong recommendation, moderate certainty evidence, (4)).
7. Should adult with acute, uncomplicated appendicitis undergo delayed (> 12 h) or immediate operation (< 12 h)?
· We recommend planning open or laparoscopic appendectomy for the next available operating list within 24 h in case of uncomplicated acute appendicitis, minimizing the delay wherever possible, (Strong recommendation, moderate certainty evidence, (4)).
· We recommend against delaying appendectomy for acute appendicitis needing surgery beyond 24 h from the admission, (Strong recommendation, moderate certainty evidence, (4)).
8. Does laparoscopic appendectomy confer superior outcomes compared with open appendectomy for adult patients with acute appendicitis
· We recommend laparoscopic appendectomy as the preferred approach over open appendectomy for both uncomplicated and complicated acute appendicitis, where laparoscopic equipment and expertise are available, (Strong recommendation, high certainty evidence, (4)).
· We recommend laparoscopic appendectomy in obese patients, older patients, and patients with high peri- and postoperative risk factors, (conditional recommendation, moderate certainty evidence, (4)).
· We suggest laparoscopic appendectomy in pregnant patients in the first and second trimesters instead of open appendectomy when surgery is indicated, (conditional recommendation, moderate certainty evidence, (4)).
9. What are the best methods to reduce the risk of SSI in open appendectomies with contaminated/dirty wounds?
· We recommend protection of the edges of the wound by ring protectors in open appendectomy to decrease the risk of SSI, (Strong recommendation, moderate certainty evidence (6)).
· We recommend primary skin closure with a unique absorbable intradermal suture for open appendectomy wounds, (conditional recommendation, moderate certainty evidence (6)).
10. In patients undergoing appendectomy for perforated appendicitis, should suction and lavage versus suction alone be used?
· We recommend performing suction alone in complicated appendicitis patients with intra-abdominal collections undergoing laparoscopic appendectomy, (Strong recommendation, moderate certainty evidence, (6)).
11. Should the macroscopically normal appendix be removed during laparoscopy for acute right iliac fossa pain when no other explanatory pathology is found?
· We suggest appendix removal if the appendix appears “normal” during surgery and no other disease is found in symptomatic patients, (conditional recommendation, low certainty evidence, (6)).
12. Management of perforated appendicitis with phlegmon or abscess
· We suggest the open or laparoscopic approach as treatment of choice for patients with complicated appendicitis with phlegmon or abscess, (conditional recommendation, moderate certainty evidence, (6)).
13. Is histopathology is needed
· We recommend routine histopathology after appendectomy, (conditional recommendation, moderate certainty evidence, (6)).
- Acknowledgement
We would like to acknowledge the guideline general surgery, (GGS) committee for developing this guideline.
Chair of GGS: Abel Motey Hussein Aly; professor of surgery, Cairo University.
Moderator of GGS: Mostafa Abdel Hamed Soliman; professor of surgery, Cairo University.
Members of GGS:
Abdelwahab Mohamed Ezzat; professor of surgery, Ain Shams University.
Ahmed Abdel Raouf Elgeidie; professor of digestive surgery, Mansoura University.
Alaa Abdallah; professor of surgery, Ain Shams University.
Atef Abdelghani Salem; professor of surgery, Benha University.
Hesham Abdel Raouf Elakad; professor of surgery, Ain Shams University.
Khaled Abdallah Elfiky; professor of surgery, Ain Shams University.
Khaled Amer; professor of surgery, Military medical academy.
Khaled Safwat; professor of surgical oncology and endoscopy, Zagazig University.
Ibrahim Elzayat; head of surgery department, Aswan University..
Mohamed Ali Mohamed Nada, professor of surgery, Ain Shams University.
Mohamed Ibrahim Abdel Hamed Alsaid, professor of surgery, Zagazig University.
Tarek Ibrahim; professor of surgery, National liver institute Menofia University.
- Abbreviations
|
AA |
Acute Appendicitis. |
|
AAS |
Adult Appendicitis Score. |
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
CRP |
Serum C Reactive Protein. |
|
CT |
Cross Section Tomography. |
|
GGS |
Guideline General Surgery. |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation. |
|
NOM |
Non Operative Management. |
|
POCUS |
Point of Care Ultrasound. |
|
RLQ |
Right Lower Quadrant. |
|
SAGES |
Society of American Gastro-Intestinal and Endoscopic Surgeons. |
|
WBC |
White Blood Cell Count. |
|
WSES |
World Society of Emergency Surgeons. |
- Introduction
Acute abdominal pain accounts for 7–10% of all emergency department accesses. Acute appendicitis (AA) is among the most common causes of lower abdominal pain leading patients to attend the emergency department and the most common diagnosis made in young patients admitted to the hospital with an acute abdomen(1).
The rate of perforation varies from 16% to 40%, with a higher frequency occurring in younger age groups (40–57%) and in patients older than 50 years (55–70%) (1).
Appendiceal perforation is associated with increased morbidity and mortality compared with non-perforating AA. The mortality risk of acute but not gangrenous AA is less than 0.1%, but the risk rises to 0.6% in gangrenous AA. On the other hand, perforated AA carries a higher mortality rate of around 5% (2).
Currently, growing evidence suggests that perforation is not necessarily the inevitable result of appendiceal obstruction, and an increasing amount of evidence now suggests not only that not all patients with AA will progress to perforation, but even that resolution may be a common event(3).
- Scope and Purpose
The scope of this guideline is who to diagnose and treat AA and how to manage their complications.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target Audience
The principle targeted audiences are the practicing surgeons, however, ICU specialists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines
· Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
· Selecting peer reviewed publications only
· Selecting guidelines written in English language
· Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GGS decided to adapt Guidelines for the diagnosis and treatment of appendicitis. This is posted by the Society of American Gastrointestinal and Endoscopic Surgeons; 2025 and diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines.
➡️Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org/
· GRADE online training modules: http://cebgrade.mcmaster.ca/
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1& 2).
➡️The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
➡️Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
➡️Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
➡️When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research Needs
1) The indication for non-operative management of acute appendicitis.
2) Studies with long term outcomes in patients that do not undergo interval appendectomy to determine the recurrence rate and the rate of any future complications.
- Clinical Indicators for Monitoring
1. Documentation of the clinical assessment.
2. CBC & CRP.
3. US and may be CT & MRI in special circumstances.
4. Documentation of the type of operation, (Appendectomy or drainage of an abscess).
- Updating of the Guidelines
The GGS committee for guidelines development is responsible for the continuous evaluation of evidence available about acute appendicitis. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Quality and Significance of the four levels of evidence in GRADE
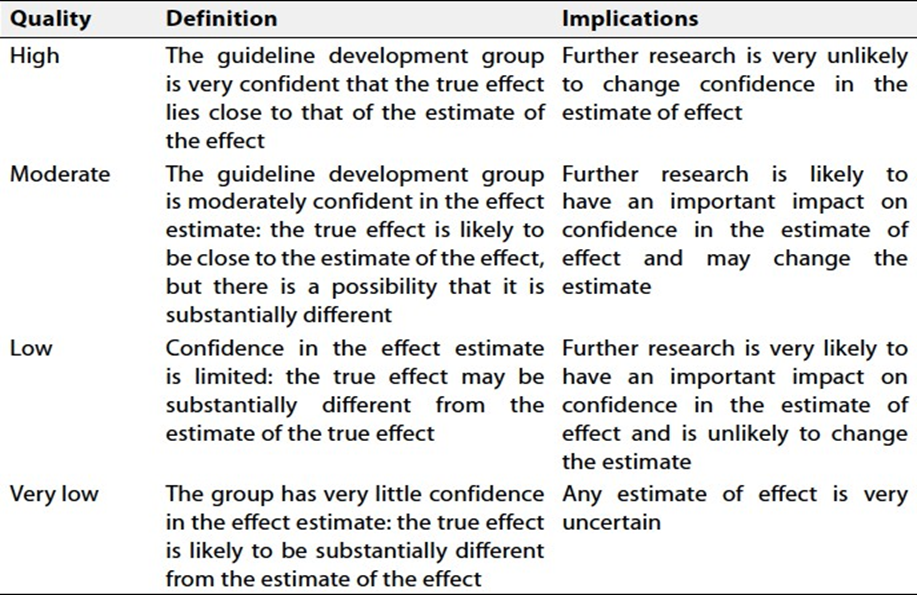
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
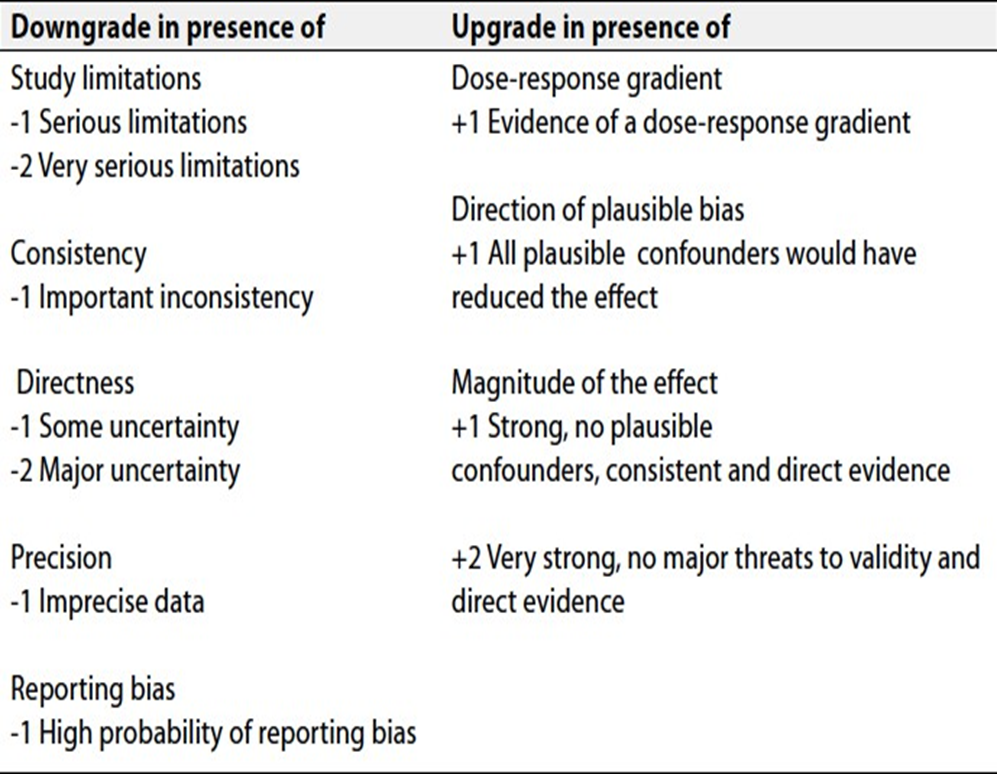
Table 3: Adult appendicitis score (AAS).
|
Symptoms and findings |
Score |
|
|
Pain in RLQ |
2 |
|
|
Pain relocation |
2 |
|
|
RLQ tenderness |
3/1 |
|
|
Guarding |
Mild |
2 |
|
Moderate or severe |
4 |
|
|
Laboratory tests |
||
|
Blood leukocyte count (×109) |
≥7.2 and <10.9 |
1 |
|
≥10.9 and <14.0 |
2 |
|
|
≥14.0 |
3 |
|
|
The proportion of neutrophils (%) |
≥62 and <75 |
2 |
|
≥75 and <83 |
3 |
|
|
≥83 |
4 |
|
|
CRP (mg/l), symptoms < 24 h |
≥4 and <11 |
2 |
|
≥11 and <25 |
3 |
|
|
≥25 and <83 |
5 |
|
|
≥83 |
1 |
|
|
CRP (mg/l), symptoms > 24 h |
≥12 and <53 |
2 |
|
≥53 and <152 |
2 |
|
|
≥152 |
1 |
|
AAS Risk Stratification: Score 0–10 For Low Probability. Score 11–15 for Intermediate Probability. Score ≥ 16 for High Probability of AA. Men and women age 50+/women, age 16–49.
Table 4: Alvarado score.
- References
1. Addiss,DG; Shaffer,N; Fowler, BS; Tauxe, RV: (1990) The epidemiology of appendicitis and appendectomy in the United States. American Journal of epidemiology. 132:910-925.
2. Lamm,R; Kumar,SS; Collings,AT; et al.:(2023) Diagnosis and treatment of appendicitis: systematic review and meta-analysis. Surg Endosc 37:8923-8990.
3. Findlay,JM; El Kafsi,J; Hammer,C; Gilmour,J; Gillies,RS; and Maynard,ND: (2016) Nonoperative management of appendicitis in adults, a systematic review and meta-analysis of randomized controlled trials. J Am Coll Surg 223:814-824-e.
4. Kumar, S.S; Cololings, A.T.; Lamm,R. et al.: Guidelines for the diagnosis and treatment of appendicitis. This is posted by the Society of American Gastrointestinal and Endoscopic Surgeons; 2025.
5. Coleman,JJ; Carr,BW; Rogers,T et al. The Alvarado score should be used to reduce emergency department length of stay and radiation exposure in select patients with abdominal pain. J Trauma Acute Care Surg. 2018;84:946-950.
6. Di Saverio,S.; Podda,M.; De Simone,B. et al.: Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World Journal of Emergency Surgery. https://doi.org/10.1186/s13017-020-00306-3.(2020) 15:27.
7. Sola R; Theut SB; Sinclair KW; Rivard DC; Johanson KM; ZhuH; St Peter SD and Shan SR. Standardized reporting of appendicitis-related finding reliability of ultrasound in diagnosing appendicitis in children. J Pediatr Surg. 2018;53:984-987.
8. Liao Y; Huang J; Wu C; Chen P; Hsieh T; Lai F; Chen T; and Liang J. The necessity of abdominal drainage for patients with complicated appendicitis undergoing laparoscopic appendectomy: a retrospective cohort stydy. World Journal of Emergency Surgery. 2022;17:1-8.
9. Sawyer RG; Claridge JA; Nathens AB; et al.Trial of short-course antimicrobial therapy for intra-abdominal infection. N Engl J Med. 2015;372:1996-2005.