Management of Groin Hernia
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | Management of Groin Hernia |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:51 AM |
Description
"last update: 12 May 2025 Download Guideline
- Executive Summary
Clinical practice
guidelines on the management of groin hernia are discussed., laboratory, and
imaging studies are discussed. The different types of treatment of groin
hernia, whether open or laparoscopic are evaluated.
· There is good evidence that surgery
effectively reduces symptoms and prevents complications of groin hernia. We
recommend it, (Strong recommendation).
· We recommend preventive
measures to reduce intra-abdominal pressure to lower the risk of hernia.
(Strong recommendation).
· We recommend appropriate
surgical technique and special post-operative management to reduce the risk of
recurrence of hernia, (conditional recommendation).
· We recommend physical
examination as the primary diagnostic tool for groin hernias, (Strong
recommendation).
· We recommend US, CT or MRI
in certain cases based on clinical circumstances, such as the patient's history
or the need for surgical planning, (Conditional recommendation).
· We recommend proper
clinical differentiation between inguinal and femoral hernias, which is vital
for accurate diagnosis and appropriate management, (Strong recommendation).
· We recommend thorough
distinction between abscesses and groin hernias through clinical examination
and imaging for guiding appropriate treatment, (Conditional recommendation).
· We recommend thorough
distinction between inguinal lymph node or other soft tissue tumors and groin
hernias by clinical examination and imaging for guiding appropriate treatment,
(Conditional recommendation).
· We recommend the use of
classification systems in groin hernia to standardize the management,
(Conditional recommendation).
· We recommend the approach
of tailoring the surgical technique to the individual patient’s needs and
hernia characteristics, (Conditional recommendation).
· We recommend the idea that hernia repair can be
successfully performed in low-resource settings with basic tools and
techniques, including the use of
non-mesh techniques when necessary, and emphasizes the value of training local surgeons
to ensure sustainable healthcare improvements, (Conditional recommendation).
· We recommend the use of
mesh in hernia repairs due to its superior outcomes in preventing recurrence.
(Strong recommendation).
· We recommend the use of
open mesh repairs, such as Lichtenstein and TIPP, as effective and reliable
methods with low recurrence rates, (Strong recommendation).
· We recommend laparoscopic
repair techniques as an option in hernias, (Conditional recommendation).
· We recommend drain after inguinal hernia repair in special
circumstances, (Conditional recommendation).
· We recommend early mobilization as it is beneficial for reducing
the risk of postoperative complications and speeding up recovery, (Conditional
recommendation).
· In cases of intestinal incarceration without strangulation or need for
bowel resection, we recommend the use of mesh-based repair, (Strong
recommendation).
· Mesh-based repair is generally not recommended for patients with
intestinal strangulation or concurrent bowel resection (clean-contaminated
surgical field) or in presence of high risk of infection, (Strong
recommendation).
· Biological mesh could be considered and recommended in very specific
cases, but it is not a routine approach, (Conditional recommendation).
· We recommend the urgent
management of femoral hernias due to the high risk of complications such as
strangulation, (Strong recommendation).
· We recommend the use of
mesh in femoral hernia repair to reduce recurrence, (Strong recommendation).
· We recommend the open anterior approach, (Lockwood) for femoral
hernia repair, particularly in emergency settings or for incarcerated hernias,
(Strong recommendation).
· Open Low, (Lotheissen-McVay) approach, is recommended in
resource-limited settings, (conditional recommendation).
· The plug or patch technique is recommended as it is a simple and
effective method for femoral hernia repair, particularly in elective cases,
(conditional recommendation).
· Open tissue repair without mesh is recommended in specific cases,
(conditional recommendation).
· The laparoscopic TAPP approach is recommended as an option for elective
femoral hernia repair, especially in patients with bilateral hernias or those
requiring concurrent inguinal hernia repairs, (conditional recommendation).
· We recommend the TEP approach for femoral hernia repair in patients
without prior lower abdominal surgery, (conditional recommendation).
· In women with groin hernia,
we recommend surgical repair techniques, including open and laparoscopic approaches,
as those used in men, (Conditional recommendation).
· We recommend the use of advanced
diagnostic tools to detect occult hernias and the preference for simultaneous
repair of bilateral hernias, (Conditional recommendation).
- Recommendations
Section
1: Importance and social impact of groin hernia surgery:
· There is good evidence that surgery
effectively reduces symptoms and prevents complications of groin hernia. We
recommend it, (Strong recommendation, high certainty evidence, (6)).
Section
2: Risk factors of groin hernia:
·
We recommend preventive
measures to reduce intra-abdominal pressure to lower the risk of hernia.
(Strong recommendation, moderate certainty evidence, (6)).
·
We recommend appropriate
surgical technique and special post-operative management to reduce the risk of
recurrence of hernia, (conditional recommendation, moderate certainty evidence,
(6)).
Section
3: Diagnosis:
·
We recommend physical
examination as the primary diagnostic tool for groin hernias, (Strong
recommendation, high certainty evidence, (6)).
·
We recommend US, CT or MRI in
certain cases based on clinical circumstances, such as the patient's history or
the need for surgical planning, (Conditional recommendation, moderate certainty
evidence, (6)).
·
We recommend proper
clinical differentiation between inguinal and femoral hernias, which is vital
for accurate diagnosis and appropriate management, (Strong recommendation, high
certainty evidence, (6)).
·
We recommend thorough
distinction between abscesses and groin hernias through clinical examination
and imaging for guiding appropriate treatment, (Conditional recommendation,
moderate certainty evidence, (6)).
·
We recommend thorough
distinction between inguinal lymph node or other soft tissue tumors and groin
hernias by clinical examination and imaging for guiding appropriate treatment,
(Conditional recommendation, moderate certainty evidence, (6)).
·
We recommend the use of
classification systems in groin hernia to standardize the management,
(Conditional recommendation, moderate certainty evidence, (6)).
Section
4: Surgical treatment options:
·
We recommend the approach
of tailoring the surgical technique to the individual patient’s needs and
hernia characteristics, (Conditional recommendation, moderate certainty
evidence, (7)).
·
We recommend the idea that hernia repair can be
successfully performed in low-resource settings with basic tools and
techniques, including the use of
non-mesh techniques when necessary, and emphasizes the value of training local
surgeons to ensure sustainable healthcare improvements, (Conditional
recommendation, moderate certainty evidence, (7)).
·
We recommend the use of
mesh in hernia repairs due to its superior outcomes in preventing recurrence.
(Strong recommendation, high certainty evidence, (7)).
·
We recommend the use of
open mesh repairs, such as Lichtenstein and TIPP, as effective and reliable methods
with low recurrence rates, (Strong recommendation, high certainty evidence, (6)).
·
We recommend laparoscopic
repair techniques as an option in hernias, (Conditional recommendation,
moderate certainty evidence, (6)).
·
We recommend drain after inguinal hernia repair in special
circumstances, (Conditional recommendation, moderate certainty evidence,
(6)).
Section 5: Postoperative care:
·
We recommend early
mobilization as it is beneficial for reducing the risk of postoperative
complications and speeding up recovery, (Conditional recommendation, moderate
certainty evidence, (7)).
Section 6: Complicated inguinal hernia:
·
In cases of intestinal incarceration without strangulation or need for
bowel resection, we recommend the use of mesh-based repair, (Strong
recommendation, high certainty evidence, (6)).
·
Mesh-based repair is generally not recommended for patients with intestinal
strangulation or concurrent bowel resection (clean-contaminated surgical field)
or in presence of high risk of infection, (Strong recommendation, high
certainty evidence, (6)).
·
Biological
mesh could be considered and recommended in very specific cases, but it is not
a routine approach,
(Conditional recommendation, moderate certainty evidence, (6)).
Section 7: Special
considerations:
·
We recommend the urgent
management of femoral hernias due to the high risk of complications such as
strangulation, (Strong recommendation, high certainty evidence, (6)).
·
We recommend the use of
mesh in femoral hernia repair to reduce recurrence, (Strong recommendation,
high certainty evidence, (6)).
·
We recommend the open anterior approach, (Lockwood) for femoral
hernia repair, particularly in emergency settings or for incarcerated hernias,
(Strong recommendation, high certainty evidence, (6)).
·
Open Low, (Lotheissen-McVay) approach, is recommended in
resource-limited settings, (conditional recommendation, moderate
certainty evidence, (6)).
· The plug or patch technique is recommended as it is a
simple and effective method for femoral hernia repair, particularly in elective
cases,
(conditional recommendation, moderate certainty evidence, (6)).
·
Open tissue repair without mesh is recommended in specific cases,
(conditional recommendation, low certainty evidence, (6)).
·
The laparoscopic TAPP approach is recommended as an option for elective
femoral hernia repair, especially in patients with bilateral hernias or those
requiring concurrent inguinal hernia repair, (conditional
recommendation, moderate certainty evidence, (7)).
·
We recommend the TEP approach for femoral hernia repair in patients
without prior lower abdominal surgery, (conditional recommendation,
moderate certainty evidence, (7)).
· In women with groin hernia, we recommend surgical repair
techniques, including open and laparoscopic approaches, as those used in men,
(Conditional recommendation, moderate certainty evidence, (7)).
·
We recommend the use of advanced diagnostic
tools to detect occult hernias and the preference for simultaneous repair of
bilateral hernias, (Conditional recommendation, moderate certainty evidence, (7)).
- Acknowledgement
We would like to acknowledge the guideline general surgery, (GGS) committee for developing this guideline.
Chair of GGS: Abel Motey Hussein Aly; professor of surgery, Cairo University.
Moderator of GGS: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University
Members of GGS:
Abdelwahab Mohamed Ezzat; professor of surgery, Ain Shams University.
Ahmed Abdel Raouf Elgeidie; professor of digestive surgery, Mansoura University.
Alaa Abdallah; professor of surgery, Ain Shams University.
Atef Abdelghani Salem; professor of surgery, Benha University.
Hesham Abdel Raouf Elakad; professor of surgery, Ain Shams University.
Khaled Abdallah Elfiky; professor of surgery, Ain Shams University.
Khaled Amer; professor of surgery, Military medical academy.
Khaled Safwat; professor of surgical oncology and endoscopy, Zagazig University.
Ibrahim Elzayat; head of surgery department, Aswan University.
Mohamed Ali Mohamed Nada, professor of surgery, Ain Shams University.
Mohamed Ibrahim Abdel Hamed Alsaid, professor of surgery, Zagazig University..
Tarek Ibrahim; professor of surgery, National liver institute Menofia University.
- Abbreviations
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
BMI |
Body Mass Index. |
|
COPD |
Chronic Obstructive Pulmonary Disease. |
|
CT |
Computed Tomography. |
|
DVT |
Deep Venous Thrombosis. |
|
GGS |
Guideline General Surgery. |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation. |
|
MRI |
Magnetic Resonance Imaging. |
|
NSAIDs |
Non-Steroidal Anti-Inflammatory Drugs. |
|
TAPP |
Transabdominal Pre-Peritoneal. |
|
TEP |
Totally Extra-Peritoneal. |
|
TIPP |
Trans-Inguinal Pre-Peritoneal. |
|
US |
Ultrasonography. |
- Introduction
Groin hernia repair is one of the most commonly performed surgeries worldwide. It involves the correction of inguinal hernias, which occur when part of the intestine or abdominal tissue pushes through a weakened area of the abdominal wall. Groin hernias are classified based on their anatomical location and the type of tissue involved, (1). The two primary types of groin hernias are inguinal hernias and femoral hernias. Inguinal hernias are further categorized into direct and indirect hernias, (2).
The surgical repair can be approached in different ways, including open repair, laparoscopic repair, and robotic-assisted surgery. The method chosen often depends on the surgeon's expertise, patient characteristics, and the specific nature of the hernia, (3-5).
- Scope and Purpose
The scope of this guideline is who to diagnose and treat groin hernia and how to manage their complications.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target Audience
The principle targeted audiences are the practicing surgeons.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
·Selecting only national and/or international guidelines
· Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
· Selecting peer reviewed publications only
· Selecting guidelines written in English language
· Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GGS decided to adapt update of the international Hernia Surgery guidelines for groin hernia management, 2023, European Hernia Society guidelines on the treatment of inguinal hernia in adult patients, 2009.
➡️Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org/
· GRADE online training modules: http://cebgrade.mcmaster.ca/
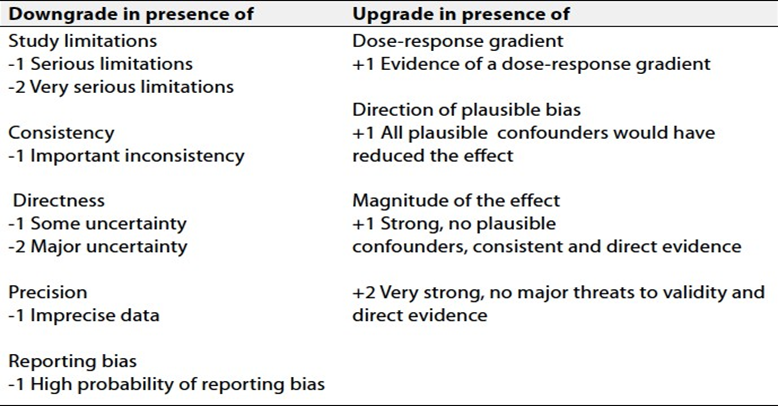
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1& 2).
➡️The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
➡️Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
➡️Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
➡️When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research Needs
1) The management of recurrent inguinal hernias.
2) The management of huge inguinal hernias.
- Clinical Indicators of Monitoring
1. Documentation of the type of hernia, (inguinal or femoral); (direct or indirect); (recurrent or not); (unilateral or bilateral).
2. Documentation of the type of operation, (open or laparoscopic) and surgical steps.
3. Documentation of the type of mesh, (if used).
- Updating of the Guidelines
The GGS committee for guidelines development is responsible for the continuous evaluation of evidence available about groin hernia. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Quality and Significance of the four levels of evidence in GRADE:
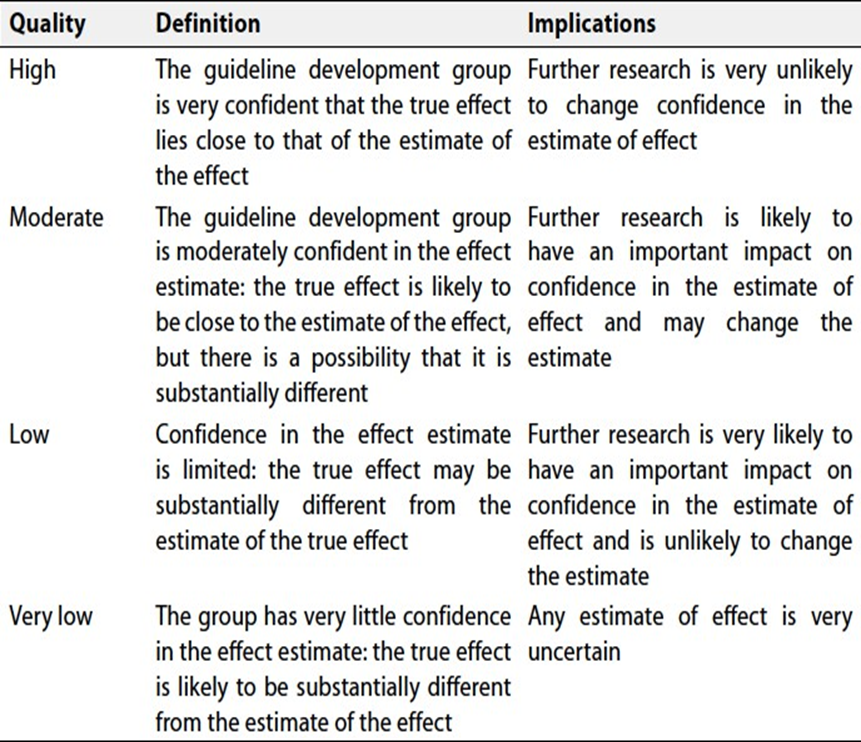
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
- References
1. Decker E, Currie A, Baig MK. Prolene hernia system versus Lichtenstein repair for inguinal hernia: a meta-analysis. Hernia. 2019 Jun;23(3):541-546. [PubMed]
2. Muschaweck U, Koch A. [Sportsmen's groin : Definition, differential diagnosis and treatment]. Radiologe. 2019 Mar;59(3):224-233. [PubMed]
3. Sun L, Shen YM, Chen J. Laparoscopic versus Lichtenstein hernioplasty for inguinal hernias: a systematic review and Meta-analysis of randomized controlled trials. Minim Invasive Ther Allied Technol. 2020 Feb;29(1):20-27.[PubMed]
4. Li J, Gong W, Liu Q. Intraoperative adjunctive techniques to reduce seroma formation in laparoscopic inguinal hernioplasty: a systematic review. Hernia. 2019 Aug;23(4):723-731. [PubMed]
5. Fernando H, Garcia C, Hossack T, Ahmadi N, Thanigasalam R, Gillatt D, Leslie S, Doeuk N, Smith I, Woo HH. Incidence, Predictive Factors and Preventive Measures for Inguinal Hernia following Robotic and Laparoscopic Radical Prostatectomy: A Systematic Review. J Urol. 2019 Jun;201(6):1072-1079. [PubMed]
6. Cesare Stabilini, Nadine van Veenendaal, Eske Aasvang, Ferdinando Agresta, Theo Aufenacker, Frederik Berrevoet, Ine Burgmans, David Chen, Andrew de Beaux, Barbora East et.al.: Update of the international HerniaSurge guidelines for groin hernia management. BJS Open, Volume 7, Issue 5, October 2023, zrad080, https://doi.org/10.1093/bjsopen/zrad080
7. M P Simons, T Aufenacker, M Bay-Nielsen, J L Bouillot, G Campanelli, J Conze, D de Lange, R Fortelny, T Heikkinen, A Kingsnorth, J Kukleta, S Morales-Conde, P Nordin, V Schumpelick, S Smedberg, M Smietanski, G Weber, M Miserez: European Hernia Society guidelines on the treatment of inguinal hernia in adult patients Hernia 13, 343–403 (2009). https://doi.org/10.1007/s10029-009-0529-7