Management of Gall Stone Disease
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | جراحه عامه |
| كتاب: | Management of Gall Stone Disease |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:51 AM |
الوصف
"last update: 13 May 2025 Download Guideline
- Executive Summary
This guidelines describes the management of gall stone disease including diagnosis of chronic and acute calculus cholecystitis, (clinically, laboratory, and with image studies) as well as the treatment of gall stone disease with stress on common bile duct (CBD) stones and accidental CBD injury.
· We recommend diagnosing gallbladder stones by the characteristic symptoms of episodic attacks of severe pain in the right upper abdominal quadrant or epigastrium for at least 15-30 minutes with radiation to the right back or shoulder and a positive reaction to analgesics, (Conditional recommendation).
· In a patient with a recent history of biliary pain, abdominal ultrasound should be performed, (Strong recommendation).
· In case of strong clinical suspicion of gallbladder stones and negative abdominal ultrasound, endoscopic ultrasound or magnetic resonance imaging may be performed (Conditional recommendation).
· As no feature has sufficient diagnostic power to establish or exclude the diagnosis of ACC, it is recommended not to rely on a single clinical or laboratory finding, (Strong recommendation).
· For the diagnosis of ACC, we suggest using a combination of detailed history, complete clinical examination, laboratory tests and imaging investigations, (Conditional recommendation).
· We recommend the use of abdominal ultrasound (US) as the preferred initial imaging technique, (Strong recommendation).
· We suggest the use CT & MRI for the diagnosis of ACC, (Conditional recommendation).
· Common bile duct stones should be searched for in patients with jaundice, acute cholangitis or acute pancreatitis, (Strong recommendation).
· We recommend against the use of elevated LFTs or bilirubin as the only method to identify CBDS in patients with CCh, (Strong recommendation).
· Abdominal ultrasound should be the first imaging method when CBD stones are suspected, (Strong recommendation).
· We recommend that patients with moderate risk for CBDS undergo one of the following: preoperative magnetic resonance cholangiopancreatography (MRCP), ERCP, intraoperative cholangiography (IOC), or laparoscopic ultrasound (LUS), depending on local expertise and availability, (Strong recommendation).
· Suspect Cholangitis is in patients with fever and a history of chills, together with abdominal pain and jaundice. White blood cells, C-reactive protein and liver biochemical tests should be determined and abdominal ultrasound should be performed as the initial investigations, (Strong recommendation).
· Suspect acute biliary pancreatitis in the presence of upper abdominal pain and altered pancreatic and liver biochemical tests in patients with gallbladder and/ or common bile duct stones, (Strong recommendation).
· The exclusion of bile duct stones by endoscopic ultrasound (or magnetic resonance cholangiopancreatography) may prevent the potential risks of endoscopic retrograde Cholangiopancreatograph (ERCP) in patients with acute biliary pancreatitis and suspected bile duct stones, (Conditional recommendation).
· We recommend against using bile acids alone or in combination with extracorporeal shock wave lithotripsy for dissolving gallbladder stones, (Strong recommendation).
· We suggest considering NOM, (i.e medical therapy with antibiotics and observation), for patients refusing surgery or those who are not suitable for surgery, (Conditional recommendation).
· We recommend cholecystectomy as the preferred option for treatment of symptomatic gallbladder stones, (Strong recommendation).
· Routine treatment is not recommended for patients with asymptomatic gallbladder stones, (Conditional recommendation).
· Asymptomatic patients with porcelain gallbladder may undergo cholecystectomy, (Conditional recommendation).
· Cholecystectomy is not recommended in patients with gallbladder polyps ≤5 mm, (Strong recommendation).
· Cholecystectomy should be performed in patients with gallbladder polyps ≥1 cm without or with gallstones regardless of their symptoms, (Strong recommendation).
· Cholecystectomy is considered in patients with asymptomatic gallbladder stones and gallbladder polyps 6-10 mm and in case of growing polyps, (Conditional recommendation).
· Cholecystectomy may be recommended for asymptomatic patients with primary sclerosing cholangitis and gallbladder polyps irrespective of size, (Conditional recommendation).
· We recommend laparoscopic cholecystectomy as the first-line treatment for patients with ACC, (Strong recommendation).
· We recommend avoiding laparoscopic cholecystectomy in case of septic shock or absolute anesthesiology contraindications, (Strong recommendation).
· We recommend laparoscopic cholecystectomy as the first-choice treatment in high risk patients with ACC. Immediate laparoscopic cholecystectomy is superior to percutaneous trans-hepatic gallbladder drainage (PTGBD) in this group of patients, (Strong recommendation).
· We suggest performing laparoscopic cholecystectomy for CCh patients with Child’s A and B cirrhosis, patients with advanced age (including more than 80 years old) and patients who are pregnant, (Conditional recommendation).
· We recommend performing gallbladder drainage in patients with ACC who are not suitable for surgery, as it converts a septic patient with ACC into a non-septic patient, (Strong recommendation).
· Delayed laparoscopic cholecystectomy is suggested after reduction of perioperative risks to decrease readmission for ACC relapse or gallstone-related disease, (conditional recommendation).
· In patients with ACC who are not suitable for surgery, endoscopic trans-papillary gallbladder drainage (ETGBD) or ultrasound-guided transmural gallbladder drainage (EUS-GBD) should be considered safe and effective alternatives to PTGBD, if performed in high-volume centers by skilled endoscopists, (Strong recommendation).
· Cholecystectomy should be performed as early as possible for patients with biliary colic, (Strong recommendation).
· In ACC, in the presence of adequate surgical expertise, we recommend ELC be performed as soon as possible, within 7 days from hospital admission and within 10 days from the onset of symptoms, (Strong recommendation).
· In ACC, we suggest DLC to be performed beyond 6 weeks from the first clinical presentation, in case ELC cannot be performed (within 7 days of hospital admission and within 10 days of onset of symptoms), (conditional recommendation).
· Endoscopic sphincterotomy and stone extraction is a recommended treatment of bile duct stones, (Strong recommendation).
· Intraoperative endoscopic retrograde cholangiopancreatography or laparoscopic bile duct exploration in combination with cholecystectomy are recommended as alternatives when adequate expertise is available, (conditional recommendation).
· In case of failed standard stone extraction, electrohydraulic or laser lithotripsy may be performed, (conditional recommendation).
· In the case of altered anatomy (e.g. previous Roux-en-Y anastomosis, bariatric surgery) percutaneous or endoscopic (balloon endoscopy-assisted) treatment of bile duct stones can be considered, (conditional recommendation).
· In the case of failed ERCP therapy, cholecystectomy combined with bile duct exploration should be performed, (Strong recommendation).
· In case of intraoperative detection of bile duct stones, we recommend bile duct exploration, trans-cystic stone extraction or endoscopic clearance as alternative treatment options, (conditional recommendation).
· Upon postoperative diagnosis of bile duct stones, endoscopic sphincterotomy and stone extraction are recommended, (strong recommendation).
· In case of surgical bile duct exploration, primary closure may be preferred over T-tube drainage in low risk cases, (conditional recommendation).
· In patients with simultaneous gallbladder and bile duct stones, early laparoscopic cholecystectomy should be performed within 72 h after preoperative ERCP for choledocholithiasis, (Strong recommendation).
· Treatment of cholangitis should include immediate broad spectrum antibiotics and biliary drainage, (Strong recommendation).
· Timing of biliary drainage depends on severity of the cholangitis and effects of medical therapy including antibiotics and may preferably be performed within 24 h; urgent drainage should be considered in case of severe cholangitis not responding to fluid resuscitation and intravenous antibiotics, (conditional recommendation).
· For biliary pancreatitis with suspected coexistent acute cholangitis antibiotics should be initiated, and endoscopic retrograde cholangiopancreatography with sphincterotomy and stone extraction should be performed, with timing depending on the severity of cholangitis but preferably within 24 hours, (Strong recommendation).
· An endoscopic retrograde cholangiopancreatography is probably indicated in patients with biliary pancreatitis and obstructed bile duct, (conditional recommendation).
· An early endoscopic retrograde cholangiopancreatography is probably not indicated in patients with predicted severe biliary pancreatitis in the absence of cholangitis or obstructed bile duct, (conditional recommendation).
· In patients with suspected biliary pancreatitis without cholangitis, endoscopic ultrasound or magnetic resonance cholangiopancreatography may prevent potential endoscopic retrograde cholangiopancreatography and prevent its risks if no stones are detected, (conditional recommendation).
· Cholecystectomy during the same hospital admission is recommended as the preferred option in patients with mild acute biliary pancreatitis, (Strong recommendation).
· We recommend removing CBDS, either preoperatively, intraoperatively, or postoperatively, according to the local expertise and the availability of several techniques, (conditional recommendation).
· Suspected bile duct injury after surgery warrants urgent investigation including laboratory tests (white blood count, bilirubin, liver enzymes) and imaging (abdominal ultrasound, contrast-enhanced CT, magnetic resonance cholangiopancreatography) to detect bile leak and/or intra-abdominal fluid, (Strong recommendation).
· Primary surgical repair of intraoperatively recognized bile duct lesions A, B or C (Table 3) can be carried out, if surgical expertise is available. For type D lesions intraoperative consultation of an expert center is mandatory; merely sub-hepatic drainage is advised and the patient is referred to an expert center. Late reconstruction (after 6-8 weeks) is advised, often with hepatico-jejunostomy, (conditional recommendation).
- Recommendations
Section 1:Diagnosis of gallbladder stones:
· We recommend to diagnose gallbladder stones by the characteristic symptoms of episodic attacks of severe pain in the right upper abdominal quadrant or epigastrium for at least 15-30 minutes with radiation to the right back or shoulder and a positive reaction to analgesics, (Conditional recommendation, very low certainty evidence,(1)).
· In a patient with a recent history of biliary pain, abdominal ultrasound should be performed, (Strong recommendation, high certainty evidence, (1)).
· In case of strong clinical suspicion of gallbladder stones and negative abdominal ultrasound, endoscopic ultrasound or magnetic resonance imaging may be performed, (Conditional recommendation, low certainty evidence, (1)).
Section 2. Diagnosis of ACC:
· As no feature has sufficient diagnostic power to establish or exclude the diagnosis of ACC, it is recommended not to rely on a single clinical or laboratory finding, (Strong recommendation, high certainty evidence, (7)).
· For the diagnosis of ACC, we suggest using a combination of detailed history, complete clinical examination, laboratory tests and imaging investigations, (Conditional recommendation, very low certainty evidence, (7)).
· We recommend the use of abdominal ultrasound (US) as the preferred initial imaging technique, (Strong recommendation, high certainty evidence, (7) ).
· We suggest the use CT & MRI for the diagnosis of ACC, (Conditional recommendation, moderate certainty evidence, (7) ).
Section 3. Associated common bile duct stones: which tools to use for suspicion and diagnosis at presentation?
· Common bile duct stones should be searched for in patients with jaundice, acute cholangitis or acute pancreatitis, (Strong recommendation, high certainty evidence, (1)).
· We recommend against the use of elevated LFTs or bilirubin as the only method to identify CBDS in patients with CCh, (Strong recommendation, moderate certainty evidence, (1)).
· Abdominal ultrasound should be the first imaging method when CBD stones are suspected, (Strong recommendation, and moderate certainty evidence, (1)).
· We recommend that patients with moderate risk for CBDS undergo one of the following: preoperative magnetic resonance cholangiopancreatography (MRCP), ERCP, intraoperative cholangiography (IOC), or laparoscopic ultrasound (LUS), depending on local expertise and availability, (Strong recommendation, moderate certainty evidence, (3)).
· Suspect Cholangitis is in patients with fever and a history of chills, together with abdominal pain and jaundice. White blood cells, C-reactive protein and liver biochemical tests should be determined and abdominal ultrasound should be performed as the initial investigations, (Strong recommendation, moderate certainty evidence, (1)).
· Suspect acute biliary pancreatitis in the presence of upper abdominal pain and altered pancreatic and liver biochemical tests in patients with gallbladder and/ or common bile duct stones, (Strong recommendation, moderate certainty evidence, (3)).
· The exclusion of bile duct stones by endoscopic ultrasound (or magnetic resonance cholangiopancreatography) may prevent the potential risks of endoscopic retrograde Cholangiopancreatograph (ERCP) in patients with acute biliary pancreatitis and suspected bile duct stones, (Conditional recommendation, low certainty evidence, (3)).
Section 4:Medical therapy of gallstones:
· We recommend against using bile acids alone or in combination with extracorporeal shock wave lithotripsy for dissolving gallbladder stones, (Strong recommendation, moderate certainty evidence, (3)).
· We suggest considering NOM, (i.e medical therapy with antibiotics and observation), for patients refusing surgery or those who are not suitable for surgery, (Conditional recommendation, low certainty evidence, (7)).
Section 5. Surgical treatment of gallbladder stones:
· We recommend cholecystectomy as the preferred option for treatment of symptomatic gallbladder stones, (Strong recommendation, moderate certainty evidence, (3)).
· Routine treatment is not recommended for patients with asymptomatic gallbladder stones, (Conditional recommendation, very low certainty evidence, (3)).
· Asymptomatic patients with porcelain gallbladder may undergo cholecystectomy, (Conditional recommendation, very low certainty evidence, (3)).
· Cholecystectomy is not recommended in patients with gallbladder polyps ≤5 mm, (Strong recommendation, moderate certainty evidence, (3)).
· Cholecystectomy should be performed in patients with gallbladder polyps ≥1 cm without or with gallstones regardless of their symptoms, (Strong recommendation, moderate certainty evidence, (3)).
· Cholecystectomy is considered in patients with asymptomatic gallbladder stones and gallbladder polyps 6-10 mm and in case of growing polyps, (Conditional recommendation, very low certainty evidence, (3)).
· Cholecystectomy may be recommended for asymptomatic patients with primary sclerosing cholangitis and gallbladder polyps irrespective of size, (Conditional recommendation, low certainty evidence, (3)).
· We recommend laparoscopic cholecystectomy as the first-line treatment for patients with ACC, (Strong recommendation, high certainty evidence, (7)).
· We recommend avoiding laparoscopic cholecystectomy in case of septic shock or absolute anaesthesiology contraindications, (Strong recommendation, high certainty evidence, (8)).
· We recommend laparoscopic cholecystectomy as the first-choice treatment in high risk patients with ACC. Immediate laparoscopic cholecystectomy is superior to percutaneous trans-hepatic gallbladder drainage (PTGBD) in this group of patients, (Strong recommendation, high certainty evidence, (8).
· We suggest performing laparoscopic cholecystectomy for CCh patients with Child’s A and B cirrhosis, patients with advanced age (including more than 80 years old) and patients who are pregnant, (Conditional recommendation, low certainty evidence, (8)).
· We recommend performing gallbladder drainage in patients with ACC who are not suitable for surgery, as it converts a septic patient with ACC into a non-septic patient, (Strong recommendation, moderate certainty evidence, (9)).
· Delayed laparoscopic cholecystectomy is suggested after reduction of perioperative risks to decrease readmission for ACC relapse or gallstone-related disease, (conditional recommendation, very low certainty evidence, (9)).
· In patients with ACC who are not suitable for surgery, endoscopic trans-papillary gallbladder drainage (ETGBD) or ultrasound-guided transmural gallbladder drainage (EUS-GBD) should be considered safe and effective alternatives to PTGBD, if performed in high-volume centers by skilled endoscopists, (Strong recommendation, high certainty evidence, (9)).
Section 6. Timing of cholecystectomy in people with CCh:
· Cholecystectomy should be performed as early as possible for patients with biliary colic, (Strong recommendation, moderate certainty evidence, (3)).
· In ACC, in the presence of adequate surgical expertise, we recommend ELC be performed as soon as possible, within 7 days from hospital admission and within 10 days from the onset of symptoms, (Strong recommendation, moderate certainty evidence, (7)).
· In ACC, we suggest DLC to be performed beyond 6 weeks from the first clinical presentation, in case ELC cannot be performed (within 7 days of hospital admission and within 10 days of onset of symptoms), (conditional recommendation, very low certainty evidence, (7)).
7: Endoscopic and surgical therapy of bile duct stones:
· Endoscopic sphincterotomy and stone extraction is a recommended treatment of bile duct stones, (Strong recommendation, moderate certainty evidence, (3)).
· Intraoperative endoscopic retrograde cholangiopancreatography or laparoscopic bile duct exploration in combination with cholecystectomy are recommended as alternatives when adequate expertise is available, (conditional recommendation, moderate certainty evidence, (3)).
· In case of failed standard stone extraction, electrohydraulic or laser lithotripsy may be performed, (conditional recommendation, low certainty evidence, (3)).
· In the case of altered anatomy (e.g. previous Roux-en-Y anastomosis, bariatric surgery) percutaneous or endoscopic (balloon endoscopy-assisted) treatment of bile duct stones can be considered, (conditional recommendation, low certainty evidence, (3)).
· In the case of failed ERCP therapy, cholecystectomy combined with bile duct exploration should be performed, (Strong recommendation, moderate certainty evidence, (3)).
· In case of intraoperative detection of bile duct stones, we recommend bile duct exploration, trans-cystic stone extraction or endoscopic clearance as alternative treatment options, (conditional recommendation, moderate certainty evidence, (3)).
· Upon postoperative diagnosis of bile duct stones, endoscopic sphincterotomy and stone extraction are recommended, (strong recommendation, moderate certainty evidence, (3)).
· In case of surgical bile duct exploration, primary closure may be preferred over T-tube drainage in low risk cases, (conditional recommendation, low certainty evidence, (3)).
· In patients with simultaneous gallbladder and bile duct stones, early laparoscopic cholecystectomy should be performed within 72 h after preoperative ERCP for choledocholithiasis, (Strong recommendation, moderate certainty evidence, (3)).
· Treatment of cholangitis should include immediate broad spectrum antibiotics and biliary drainage, (Strong recommendation, moderate certainty evidence, (3)).
· Timing of biliary drainage depends on severity of the cholangitis and effects of medical therapy including antibiotics and may preferably be performed within 24 h; urgent drainage should be considered in case of severe cholangitis not responding to fluid resuscitation and intravenous antibiotics, (conditional recommendation, low certainty evidence, (3)).
· For biliary pancreatitis with suspected coexistent acute cholangitis antibiotics should be initiated, and endoscopic retrograde cholangiopancreatography with sphincterotomy and stone extraction should be performed, with timing depending on the severity of cholangitis but preferably within 24 hours, (Strong recommendation, high certainty evidence, (3)).
· An endoscopic retrograde cholangiopancreatography is probably indicated in patients with biliary pancreatitis and obstructed bile duct, (conditional recommendation, low certainty evidence, (3)).
· An early endoscopic retrograde cholangiopancreatography is probably not indicated in patients with predicted severe biliary pancreatitis in the absence of cholangitis or obstructed bile duct, (conditional recommendation, low certainty evidence, (3)).
· In patients with suspected biliary pancreatitis without cholangitis, endoscopic ultrasound or magnetic resonance cholangiopancreatography may prevent potential endoscopic retrograde cholangiopancreatography and prevent its risks if no stones are detected, (conditional recommendation, low certainty evidence, (3)).
· Cholecystectomy during the same hospital admission is recommended as the preferred option in patients with mild acute biliary pancreatitis, (Strong recommendation, high certainty evidence, (3)).
· We recommend removing CBDS, either preoperatively, intraoperatively, or postoperatively, according to the local expertise and the availability of several techniques, (conditional recommendation, high certainty evidence, (8)).
Section 8: Bile duct injuries:
· Suspected bile duct injury after surgery warrants urgent investigation including laboratory tests (white blood count, bilirubin, liver enzymes) and imaging (abdominal ultrasound, contrast-enhanced CT, magnetic resonance cholangiopancreatography) to detect bile leak and/or intra-abdominal fluid, (Strong recommendation, moderate certainty evidence, (3)).
· Primary surgical repair of intraoperatively recognized bile duct lesions A, B or C (Table 3) can be carried out, if surgical expertise is available. For type D lesions intraoperative consultation of an expert center is mandatory; merely sub-hepatic drainage is advised and the patient is referred to an expert center. Late reconstruction (after 6-8 weeks) is advised, often with hepatico-jejunostomy, (conditional recommendation, low certainty evidence, (3)).
- Acknowledgement
We would like to acknowledge the guideline general surgery, (GGS) committee for developing this guideline.
Chair of GGS: Abel Motey Hussein Aly; professor of surgery, Cairo University.
Moderator of GGS: Mostafa Abdel Hamed Soliman; professor of surgery, Cairo University.
Members of GGS:
Abdelwahab Mohamed Ezzat; professor of surgery, Ain Shams University.
Ahmed Abdel Raouf Elgeidie; professor of digestive surgery, Mansoura University.
Alaa Abdallah; professor of surgery, Ain Shams University.
Atef Abdelghani Salem; professor of surgery, Benha University.
Hesham Abdel Raouf Elakad; professor of surgery, Ain Shams University.
Khaled Abdallah Elfiky; professor of surgery, Ain Shams University.
Khaled Amer; professor of surgery, Military Medical Academy.
Khaled Safwat; professor of surgical oncology and endoscopy, Zagazig University.
Ibrahim Elzayat; head of surgery department, Aswan University.
Mohamed Ali Mohamed Nada, professor of surgery, Ain Shams University.
Mohamed Ibrahim Abdel Hamed Alsaid, professor of surgery, Zagazig University.
Tarek Ibrahim; professor of surgery, National Liver Institute Menofia University.
- Abbreviations
|
ACC |
Acute Calculus Cholecystitis. |
|
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
|
AIDS |
Acquired Immuno-Deficiency Syndrome. |
|
|
ALT |
Alanine Transaminase. |
|
|
ALP |
Alkaline Phosphatase. |
|
|
AUC |
Area Under the Curve. |
|
|
CBD |
Common Bile Duct. |
|
|
CBDS |
Common Bile Duct Stone. |
|
|
CC |
Consensus Conference. |
|
|
CCC |
Chronic Calculus Cholecystitis. |
|
|
CCh |
Calculus Cholecystitis |
|
|
CT |
Computed Tomography. |
|
|
DLC |
Delayed Laparoscopic Cholecystectomy. |
|
|
EHC |
Egyptian Health Council. |
|
|
ELC |
Early Laparoscopic Cholecystectomy. |
|
|
ERCP |
Endoscopic Retrograde Colangio-Pancreatography |
|
|
ETGBD |
Endoscopic Transpapillary Gallbladder Drainage |
|
|
EUS |
Endoscopic Ultrasound. |
|
|
EUS-GBD |
Endoscopic Ultrasound-Guided Gallbladder Drainage |
|
|
GGS |
Guideline General Surgery. |
|
|
GGT |
Gamma-Glutamyl Transferase. |
|
|
GRADE |
Grading of Recommendations Assessment Development and Evaluation. |
|
|
ICU |
Intensive Care Unit. |
|
|
ILC |
Intermediate Laparoscopic Cholecystectomy. |
|
|
IOC |
Intra-Operative Cholangiography. |
|
|
LFTs |
Liver Function Tests. |
|
|
LR |
Likelihood Ratio |
|
|
LUS |
Laparoscopic Ultrasound |
|
|
MRCP |
Magnetic Resonance Colangio-Pancreatography |
|
|
MRI |
Magnetic Resonance Imaging |
|
|
NOM |
Non Operative Management |
|
|
NPV |
Negative Predictive Value |
|
|
OR |
Odds Ratio |
|
|
RCT |
Randomized Controlled Trial |
|
|
SEMS |
Self-Expanding Metal Stents |
|
|
SMI |
Superb Microvascular Imaging |
|
|
pSWE |
Point Shear-Wave Elastography. |
|
|
PTGBD |
Percutaneous Transhepatic Gallbladder Drainage. |
|
|
PPV |
Positive Predictive Value. |
|
|
TG |
Tokyo Guidelines. |
|
|
TPN |
Total Parenteral Nutrition. |
|
|
US |
Ultrasound |
|
|
95% CI |
95% Confidence Interval |
|
- Introduction
Gallstone disease occurs when hard fatty or mineral deposits (gallstones) form in the gallbladder. Approximately 15% of the adult population is thought to have gallstone disease, (1 & 2).
Gallstones or cholelithiasis are a major public health problem and affect up to 20% of the population. Gallstone disease is the most common gastrointestinal disorder for which patients are admitted to hospitals in the majority of people with gallbladder stones remain asymptomatic (3 &4). For a small proportion of people with gallstone disease, the stones irritate the gallbladder or block part of the biliary system, and this can cause symptoms. If these symptoms are left untreated, gallstones can cause more serious and, in some cases, life-threatening conditions such as cholecystitis, cholangitis, pancreatitis and jaundice (4).
Cholecystitis is defined as an inflammation of the gallbladder. Ninety percent of cases are due to stones in the gallbladder (i.e., calculus cholecystitis), with the other 10% of cases representing acalculus cholecystitis (5).
Calculus cholecystitis is related to the presence of stones in the gallbladder or an obstruction of the cystic duct from cholelithiasis, while acalculous cholecystitis is related to conditions associated with biliary stasis, such as debilitation, major surgery, severe trauma, sepsis, long-term total parenteral nutrition (TPN), and prolonged fasting. Other causes of acalculous cholecystitis include cardiac events; sickle cell disease; Salmonella infections; diabetes mellitus; and cytomegalovirus, cryptosporidiosis, or microsporidiosis infections in patients with acquired immunodeficiency syndrome (AIDS) (5 &6).
Uncomplicated cholecystitis has an excellent prognosis, with a very low mortality rate. Once complications such as perforation/gangrene develop, the prognosis becomes less favorable (6).
Delays in making the diagnosis of acute cholecystitis result in a higher incidence of morbidity and mortality. This is especially true for intensive care unit (ICU) patients who develop calculus cholecystitis (6).
- Scope and Purpose
The scope of this guideline is who to diagnose and treat acute and chronic cholecystitis and how to manage their complications.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target Audience
The principle targeted audiences are the practicing surgeons, however, ICU specialists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GGS decided to adapt the Gallstone disease: diagnosis and management Clinical guideline, 2014; EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones, 2016; Useful of Tokyo guidelines in the diagnosis of acute cholecystitis. Anatomopathologie correlationship, 2017; and Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis, 2018.
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org/
· GRADE online training modules: http://cebgrade.mcmaster.ca/
· GRADE profile software: http://ims.cochrane.org/revman/gradepro
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1& 2).
➡️The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
➡️Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
➡️Conditional recommendations
these are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
➡️When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research Needs
1) The management of difficult operative scenarios during laparoscopic cholecystectomy, (e.g. adhesions with hollow viscus, difficulties in grasping the gallbladder, difficulties in view of safety, gangrene of the cystic duct, etc.).
2) Different modalities for the management in case of difficult cholecystectomy.
- Clinical Indicators for Monitoring
1. Liver function tests.
2. US.
3. MRCP in case of biliary obstruction.
- Updating of the Guidelines
The GGS committee for guidelines development is responsible for the continuous evaluation of evidence available about acute cholecystitis. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Quality and Significance of the four levels of evidence in GRADE
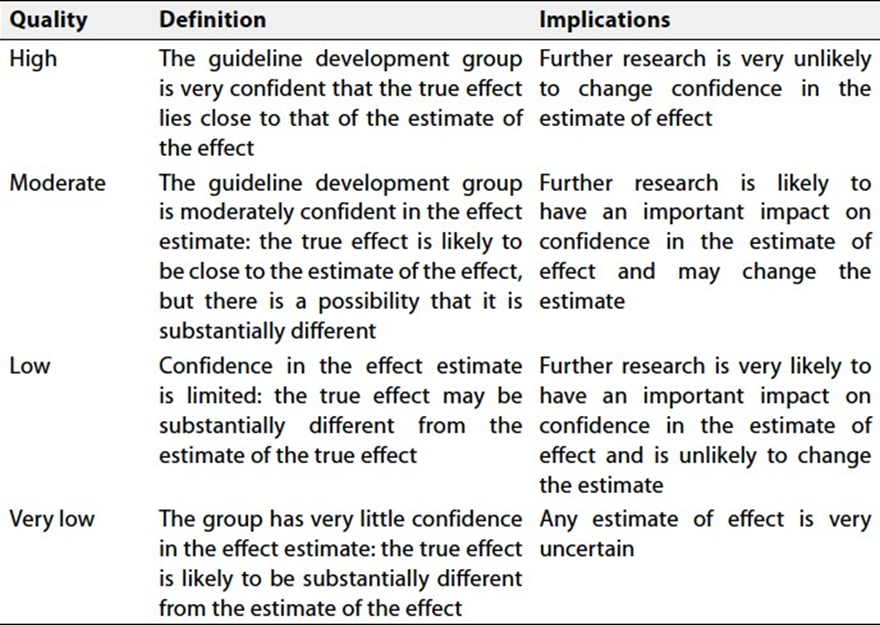
Table 2 Factors that determine How to upgrade
or downgrade the quality of evidence
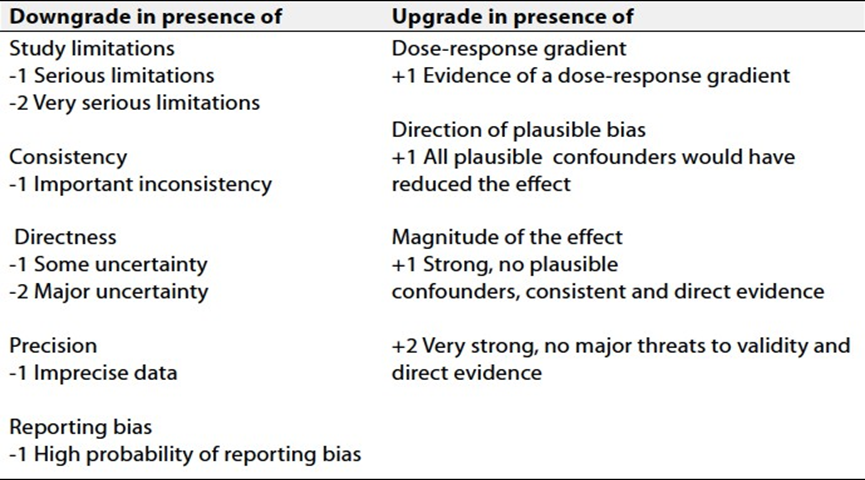
Table 3.
Classification of bile duct injuries
|
A |
Cystic duct or aberrant bile duct leakage |
|
B |
CBD leakage, with or without stricture |
|
C |
CBD stricture without leakage |
|
D |
Complete CBD transection with or without tissue loss |
- References
1. Gallstone disease: diagnosis and management Clinical guideline [Internet]. 2014. Available from: www.nice.org.uk/guidance/cg188
2. Shaffer EA. Epidemiology and risk factors for gallstone disease: Has the paradigm changed in the 21st century? Curr Gastroenterol Rep. 2005;7(2):132–40.
3. Lammert F, Acalovschi M, Ercolani G, van Erpecum KJ, Gurusamy KS, van Laarhoven CJ, et al. EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol [Internet]. 2016 Jul 1 [cited 2025 Feb 27];65(1):146–81. Available from: https://www.journal-of-hepatology.eu/article/s0168-8278(16)30032-0/fulltext
4. Kratzer W, Mason RA, Kächele V. Prevalence of gallstones in sonographic surveys worldwide. J Clin Ultrasound. 1999;27(1):1–7.
5. Commissioning guide: Gallstone disease Sponsoring Organisation: Association of Upper gastrointestinal Surgeons [Internet]. Available from: www.nice.org.uk/accreditation
6. Friedman GD. Natural history of asymptomatic and symptomatic gallstones. Am J Surg. 1993;165(4):399–404.
7. Janikow C, Corti E, Menso N, et al. Useful of Tokyo guidelines in the diagnosis of acute cholecystitis. Anatomopathologie correlationship. Rev Fac Cien Med Univ Nac Cordoba. 2017;74(2):88–92.
8. Okamoto K, Suzuki K, Takada T, Strasberg SM, Asbun HJ, Endo I. Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):55–72.
9. SAGES Guidelines for the Clinical Application of Laparoscopic Biliary Tract Surgery [Internet]. [cited 2025 Mar 10]. Available from: https://www.sages.org/publications/guidelines/guidelines-for-the-clinical-application-of-laparoscopic-biliary-tract-surgery/