Equine Laminitis
| Site: | EHC | Egyptian Health Council |
| Course: | Equine Surgery Guidelines |
| Book: | Equine Laminitis |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:34 AM |
Description
"last update: 22 Jun 2025" Download Guideline
Table of contents
- - Acknowledgement
- - Scope
- - Definition
- - Anatomical structure of the hoof
- - How laminitis developed
- - Major types of laminitis
- - Risk Factors for Laminitis
- - The clinical Signs of laminitis
- - Obel grading system
- - Diagnosis of laminitis
- - Treatment of laminitis
- - Prognosis of laminitis
- - Trimming and shoeing
- - Aggressive therapies
- - Dietary Management for Laminitic Horses
- - Prevention of laminitis
- - References
- Acknowledgement
We would like to acknowledge the committee of National Egyptian Guidelines for Veterinary Medical Interventions, Egyptian Health Council for adapting this guideline.
Executive Chief of the Egyptian Health Council: Prof. Mohamed Mustafa Lotief.
Head of the Committee: Prof. Ahmed M Byomi
The rapporteur of the Committee: Prof. Mohamed Mohamady Ghanem.
Scientific Group Members: Prof. Nabil Yassien, Prof. Ashraf Aldesoky Shamaa, Prof. Amany Abbass, Prof. Dalia Mansour, Dr. Essam Elmarakby, Dr. Mohamed Elsharkawy, Prof. Gamal A. Sosa., Dr. Naglaa Radwan, Dr. Hend El Sheikh
Authors: Dr. Mohamed Elsharkawy, Prof. Mohamed Ghanem, Prof. Ashraf Aldesoky Shamaa
- Scope
Laminitis is a serious and painful condition affecting the hoof structures; the disease’s potential to cause severe lameness, permanent hoof damage, and even euthanasia in severe cases. so it’s one of the most important equine disorders affecting equine locomotors system with great economic impact .The scope of a study on equine laminitis can vary widely, but generally focuses on understanding the disease's causes, mechanisms, prevention, and management.The goal is to improve equine welfare by promoting evidence-based care practices.
- Definition
Laminitis (Aseptic pododermatitis) is an inflammation and damage and of the tissue between the hoof and the underlying coffin bone (distal phalanx, P3), the failure of the attachment between the distal phalanx (coffin bone) and the inner hoof wall. The terms "laminitis" and "founder" are used interchangeably. However acute laminitis refers to symptoms associated with a sudden initial attack, including pain and inflammation of the laminae. Whereas founder usually refers to a chronic (long-term) condition associated with rotation of the coffin bone.
- Anatomical structure of the hoof
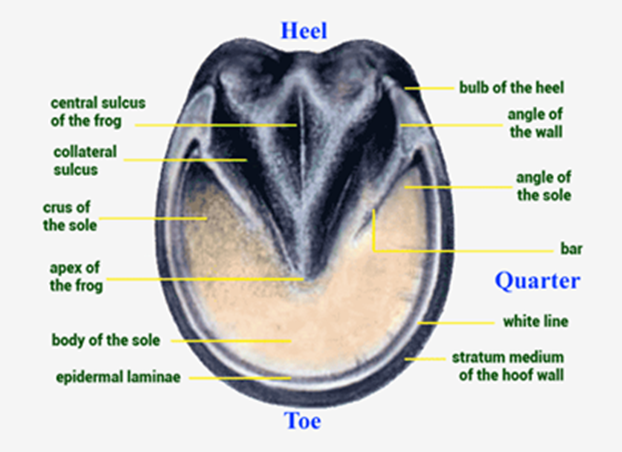
Fig.1 Ventral aspect of the hoof
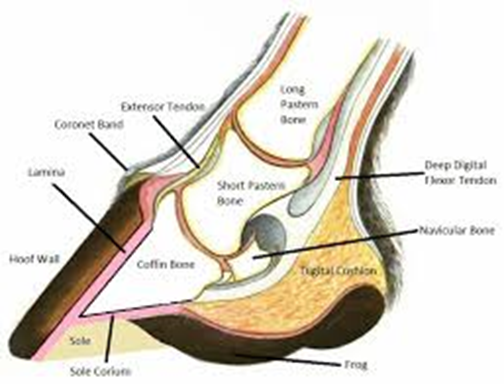
Fig.2 Cross-sectional diagram of a horse hoof (Alderman, 2017)
- How laminitis developed
- the epithelial detachment resulting from inflammation and enzyme activation associated with sepsis and other disease processes, insulin resistance, vascular endothelial dysfunction, and excessive weight bearing are factors at the forefront of current investigations.
- Colonic fermentation of plant with Nonstructural carbohydrates (NSCs) may cause gastrointestinal disturbances that can lead to laminitis. In addition, intake of feeds rich in NSCs may lead to hyperinsulinemia and insulin resistance in animals with metabolic syndrome. Experimental models leading to hindgut fermentation of carbohydrates and hyperinsulinemia both reliably induce laminitis.
- Laminitis associated with sepsis associated with Leukocyte infiltration, endothelial activation, and increased messenger RNA concentration of pro-inflammatory cytokines and cyclooxygenase (COX)-2 expressions have been documented in experimental models of equine sepsis and gastrointestinal disease.
- Alterations in laminar hemodynamics, including alterations in blood flow and increased venous resistance favoring edema formation, have been documented but may not be the primary events leading to laminar failure.
- Major types of laminitis
1- Metabolic Laminitis
- The horses have abnormal control of carbohydrate metabolism and as a result have abnormally high levels of the insulin. This result in two diseases: pituitary pars intermedia dysfunction (PPID; Cushing’s disease) and equine metabolic syndrome (EMS)
- The abnormal processing of dietary carbohydrates in both of these conditions involves an excessive insulin response to starches (main carbohydrate in grains) or sugars (main carbohydrates in grasses and hay) in horse feed
- Pituitary pars intermedia dysfunction (PPID; Cushing’s disease): PPID is a disease of ageing, where the control of pituitary gland hormone secretion is lost, leading to excessive secretion from a certain part of the gland (the pars intermedia, as in PPID) leading to hyperadrenocorticism. The clinical signs include:
a- A long hair coat due to delayed shedding.
b- Sweating.
c- Loss of muscle mass.
d- Development of a pot belly and drinking excessively.
N.B
- Some of the hormones produced from the pituitary also affect carbohydrate metabolism and can predispose to laminitis.
- Many PPID horses/ponies may have been originally fat, so when they lose muscle their fat often looks strange and lumpy, but PPID is not caused by obesity.
- Equine metabolic syndrome (EMS )
Tend to occur in genetically predisposed breeds and is worsened by obesity. This does not mean that all obese horses or ponies have EMS, but if the horse or pony has EMS then obesity will worsen the carbohydrate metabolism and predispose to laminitis.
2- Sepsis-associated laminitis
Sepsis-associated laminitis, which occurs in cases of severe systemic inflammation, which associated with serious illness and bacterial endotoxin production. Examples include salmonellosis, colic, bastard Strangles, Potomac Horse Fever, and retained placenta.
3- Supporting limb laminitis
Support limb laminitis (SLL), the least common type of laminitis, occurs in horses suffering a non-weight-bearing lameness. Laminitis develops in the opposite supporting limb due to prolonged excessive weight-bearing.
- Risk Factors for Laminitis
While any equine may develop laminitis, some are more vulnerable than others include:
1- Pituitary Pars Intermedia Disease (PPID or Equine Cushing’s Disease) when the horse also has insulin resistance.
2- Equine Metabolic Syndrome (EMS).
3- Horses who have received high or long-term doses of corticosteroids are at increased risk of developing laminitis because these drugs induce insulin resistance.
4- Animals with poor hoof or limb conformation due to abnormal biomechanics.
5- Certain genes may predispose horses to metabolic dysfunction and laminitis. Breeds such as Morgans, Paso Finos, Arabians, Andalusians, and Welsh, Shetland and Dartmoor ponies are considered more vulnerable to equine metabolic syndrome and laminitis.
6- “Road founder” or excessive concussion on hard surfaces, more common in driving horses.
7- Pregnancy-induced insulin resistance.
8- Toxins entering the body, such as from a snake bite.
9- Long courses of Cephalosporin antibiotic.
10- Stall Rest.
11- Idiopathic.
- The clinical Signs of laminitis
Laminitis can affect a single foot, all four feet, the forefeet alone, or less commonly, the hind feet alone.
A. Peracute form
Peracute laminitis is a severe, rapid onset form of laminitis, a painful inflammation of the laminae, the sensitive tissues in the hoof that connect the hoof wall to the coffin bone. The third phalanx (coffin bone) can start to rotate or sink within the hoof capsule within hours or a few days of the onset of lameness.
B. Acute form
1- Standing position
Very characteristic for laminitic horses.

Fig.3 typical standing position of acute laminitic horse.
2- Lameness, especially when a horse is turning in circles; shifting lameness when standing.
3- Heat in the feet.
4- Digital pulse can fill in the feet (most easily palpable over the sesamoidal bone at the level of the fetlock).

Fig.4 site of pulse detection.
5- Pain in the toe region when pressure is applied with hoof testers.
6- Reluctant or hesitant gait ("walking on eggshells").
A. in chronic form :
1- Rings in hoof wall that become wider as they are followed from toe to heel.

Fig.5 Rings in hoof wall in chronic case.
2- Bruised soles or "stone bruises."
3- Widened white line, commonly called "seedy toe," with occurrence of seroma (blood pockets) and/or abscesses.
4- Dropped soles or flat feet.
5- Thick, "cresty" neck.
6- Dished hooves, which are the result of unequal rates of hoof growth (the heels grow at a faster rate than the rest of the hoof, resulting in an "Aladdin-slipper" appearance).

Fig.6 Aladdin-slipper appearance.
- Obel grading system
The severity of lameness is qualified using the Obel grading system:
- Obel grade 1: Horse shifts weight between affected feet or continuously lift feet up. It is sound at the walk but displays a shortened stride at the trot.
- Obel grade 2: Horse displays a stilted, stiff gait, although is willing to walk. It is possible to easily lift a front foot and have the horse take all of its weight on the contralateral limb.
- Obel grade 3: Horse displays a stilted, stiff gait, but is reluctant to walk and is difficult when asked to lift a front foot.
- Obel grade 4: Horse is very reluctant to move, or is recumbent.
- Diagnosis of laminitis
A- Case history
By gathering the following information
1- Current diet, including any recent changes in diet.
2- All current medications.
3- Whether this is the first incidence of laminitis or a chronic issue.
4- Any current medical conditions, such as Pituitary Pars Intermedia Dysfunction (PPID) or Equine Metabolic Syndrome (EMS).
5- Current health status including if the horse is being treated for things like diarrhea, infection, or musculoskeletal injury.
B. Radiographic measurement
Several radiographic measurements, made on the lateral view, allow for objective evaluation of the episode:
1- Coronary extensor distance (CE) the vertical distance from the level of the proximal coronary band to the extensor process of P3. It is often used to compare progression of the disease over time, rather than as a stand-alone value. A rapidly increasing CE value can indicate distal displacement (sinking) of the coffin bone, while a more gradual increase in CE can occur with foot collapse. Normal values range from 0–30 mm, with most horses >12–15 mm.
2- Sole depth (SD) the distance from the tip of P3 to the ground (A sole depth at the toe of <15 mm).
3- Digital break over (DB) distance from the tip of P3 to the breakover of the hoof (dorsal toe).
4- Palmar angle (PA) the angle between a line perpendicular to the ground, and a line at the angle of the palmar surface of P3(Solar margin angle 3–8º)
5- Horn lamellar distance (HL) the measurement from the most superficial aspect of the dorsal hoof wall to the face of P3. 2 distances are compared: a proximal measurement made just distal to the extensor process of P3, and a distal measurement made toward the tip of P3.
These two values should be similar. In cases of rotation, the distal measurement will be higher than the proximal. In cases of distal displacement, both values will increase, but may remain equal.

Fig.7 Coronary extensor distance (CE), Horn lamellar distance (HL), Sole depth (SD),
Digital break over (DB) and palmar angle (PA).
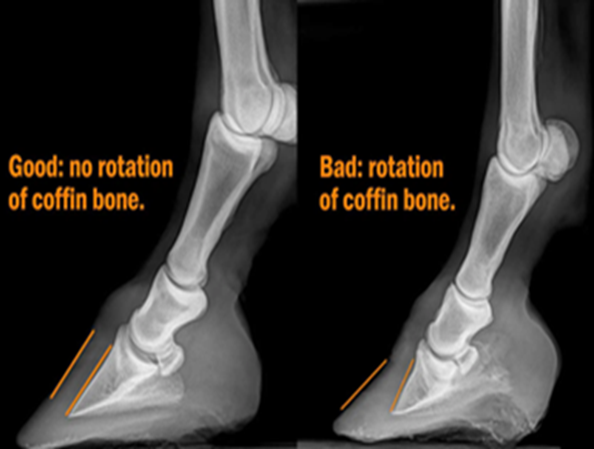
Fig.8 the coffin bone position.
- Treatment of laminitis
The goal of treatment in horses with laminitis was directed to minimize the predisposing factors, reduce the severity of pain and laminar damage, to improve digital and laminar haemo-dynamics and to prevent further rotation and sinking of the pedal bone within the hoof.
1- Management
Initial management usually includes stall rest to minimize movement, and deeply bedding the stall with shavings, straw, or sand. Exercise is slowly increased once the horse has improved, ideally in an area with good (soft) footing, beginning with hand-walking, then turn-out, and finally riding under saddle .
2- Cryotherapy
- Cooling of the hoof. Feet placed in ice slurries were less likely to experience laminitis than "un iced" feet within the first 24 hours.
- Cryotherapy reduces inflammatory events in the lamellae. Ideally, limbs should be placed in an ice bath up to the level of the knee or hock.
- Hooves need to be maintained at a temperature less than 10 °C at the hoof wall, for 24–72 hours.
3-Drug therapies
1- Anti-inflammatories and analgesics
- Nonsteroidal anti-inflammatory medications (NSAIDS) are often the first line of defense. Phenylbutazone is commonly used for its strong effect and relatively low cost (2.2–4.4 mg/kg I.V) for 5 days.
- Flunixin (0.25 mg/kg, IV, q 8 h, or 1.1mg/kg, IV, q 12 h) for 5 days.
- Nonspecific NSAIDs such as suxibuzone, or Firocoxib (0.1 mg/kg PO every 24 hours) for 10 days.
- Dimethyl sulfoxide DMSO (0.1–1.0 g/kg diluted to 10% solution IV every 8–24 hours) for 5 ays.
- Pentoxifylline (8.5–10 mg/kg IV or PO every 12 hours) for 3 days.
2- Vasodilators
- Vasodilators are often used with the goal of improving laminar blood flow Isoxsuprine to increase blood flow; isoxsuprine HClb (0.6 -2 mg/ kg, q 12 h) for 7 days .
- Nitroglycerine d (60 mg as a 2% ointment on the skin over the digital vasculature) has also been applied topically in an attempt to increase blood flow two time daily for 3 days.
3- Anticoagulant
High doses of heparin (100 IU/kg, IV/ day in Ringers solution for 4 days) to prevent or ameliorate signs of laminitis caused by carbohydrate overload Heparin administered to horses intravenously in high doses rapidly results in a marked decrease in the hematocrit caused by agglutination of erythrocytes because the reticuloendothelial system removes the agglutinated erythrocytes from circulation.
4- Systemic antibacterial (Penicillin and Streptomycin 5000 IU and 15 mg /Kg .day .I.M) to 3-5 days.
5- Antihistamines (1mg /Kg / day I.V for 5 days).
6- Electrolyte therapy (Ringers lactate 10-20 ml /kg. I.V) for 5 days.
- Prognosis of laminitis
- Rapid diagnosis of laminitis with modern therapies the most laminitic horses will be able to bear a rider or completely recover, if treated quickly, and if the laminitis was not severe or complicated (e.g. by equine metabolic syndrome or Cushing's disease). Even in these cases, a clinical cure can often be achieved.
- Endotoxic laminitis (e.g. after foaling) tends to be more difficult to treat.
- Successful treatment requires a competent farrier and veterinarian, and success is not guaranteed.
- A horse can live with laminitis for many years, and although a single episode of laminitis predisposes to further episodes.
- Most of the horses suffering an acute episode without pedal bone displacement make a complete functional recovery.
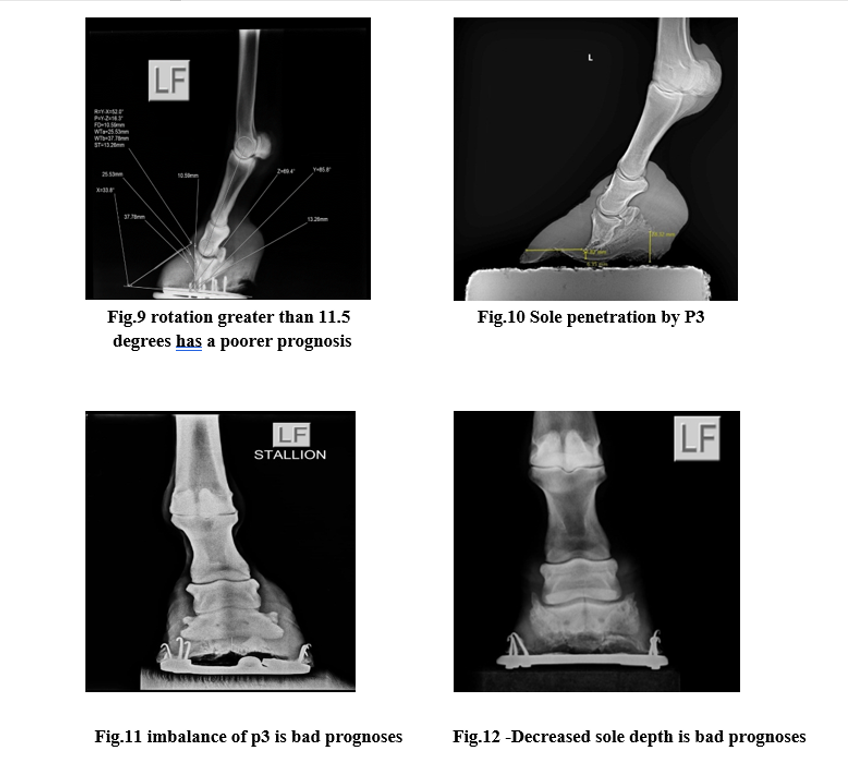
Several radiographic abnormalities can be judged to correlate with a worsened prognosis:
- Increased degree of rotation of P3 relative to the dorsal hoof wall (rotation greater than 11.5 degrees has a poorer prognosis).
- Increased founder distance, the vertical distance from the coronary band (seen with a radio-opaque marker) to the dorsoproximal aspect of P3 (distance greater than 15.2mm has a poorer prognosis).
- Decreased sole depth.
- Sole penetration by P3.
- Trimming and shoeing
Trimming
1- Correct trimming can help improve stabilization. This usually includes bringing the "break over" back to decrease the fulcrum-effect that stresses the laminae.
2- Trimming the heels helps to ensure frog pressure and increases surface area for weight-bearing on the back half of the hoof.
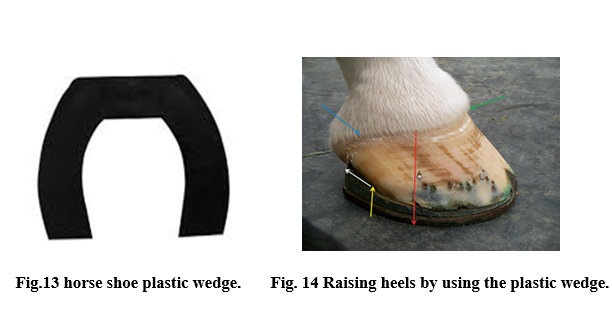
3- Altering the palmar angle. Often with the use of special shoes which have a wedge in the heel of approximately 20 degrees. The position of P3 within the hoof is monitored with radiographs.
4- Corrective hoof trimming will restore proper hoof form and function. Corrective trimming will allow the hooves to be healthy again.
Shoeing
There are three main considerations involved in shoe selection and shoeing technique these principles based on history, physical examination, and radiographs:
(1) The position of the breakover point
To improve the ease of movement by decreasing the stresses within the dorsal lamellae, the optimal position for the point of breakover should really be in horses can be obtained by drawing a line on the radiograph from the dorsal margin of the distal phalanx to the line indicating the desired plane of the trim and perpendicular to it . The point of breakover is positioned ~6-9 mm dorsal to the junction of the two lines which can significantly decrease the amount of weight-bearing ground surface of the foot.
(2) Whether to provide support for the ground surface of the frog and sole.
(3) Whether to elevate the heels.
- To decrease the tension in the DDFT, which the decreases the pressure of the distal interphalangeal joint with the intention of decreasing the stresses within the dorsal lamellae.
-This is usually most appropriate in horses with phalangeal rotation that are landing toe first.
- The amount of heel elevation varies between 2° and 4°. Heel elevation may be obtained with wedged shoes, bar wedge inserts, or rails.
- The efficacy of heel elevation is best judged by the comfort of the horse, after trimming at rest and walking.
- Ideally, the heel elevation is such that the horse just lands heel first. If a horse lands markedly heel first, there is too much heel elevation, and if it lands toe first, there is not enough heel elevation.
- Unfortunately, prolonged heel elevation may result in heel contracture, which potentially causes the heels themselves to become painful. Thus, it is prudent, if using heel elevation, to remove it as rapidly as possible compatible with the improvement in lameness.
Types of Shoes can be used with laminitic horses
Success technique increases with the experience of both the veterinarian and the farrier.
1- Egg-Bar Shoe:
- The egg-bar shoe is a closed heel shoe in which the bar extends palmarly.
- This palmar extension act as a lever if the shoe extends too far beyond the heels. Specifically, if the horse is kept on deep soft bedding, it causes the heels to remain higher on the bedding than the toe and can act as a heel wedge.
- In horses with chronic laminitis, egg-bar shoes should be used in conjunction with a synthetic polymer to provide support to the ground surface of the foot depending on the degree of stability of the distal phalanx, heel elevation may be obtained by using a wedged rim pad or a manufactured wedge shoe.
- The disadvantage to this shoe is that it does not ease mediolateral breakover.

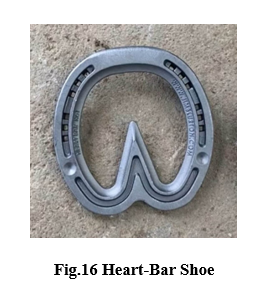
2- Heart-Bar Shoe
-The heart-bar shoe should be positioned in relation to the solar margin of the distal phalanx.
- The apex of the bar should extend to a point 9 mm palmar to the trimmed apex of the frog.
- The heart-bar is thought to enable the frog to load and redistribute some of the weight born by the limb away from the wall.
- Heart-bar shoes are increasingly used in combination with other forms of sole support that are either poured or pressed into the cavity formed between the branches of the shoe and the bar to provide additional support to the ground surface of the foot.
- Disadvantages of this shoe are that its application demands skill, it is difficult to apply heel elevation; the shoe does not address mediolateral breakover.
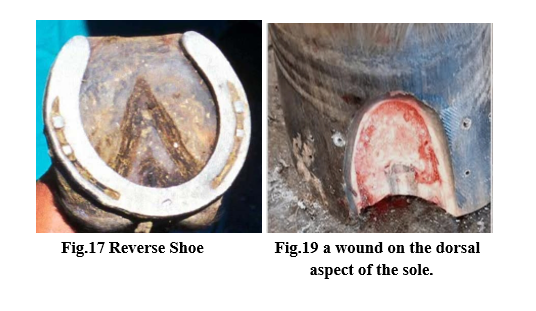
3- Reverse Shoe
- The principle benefits of a reverse shoe are that it moves the breakover palmarly. Because the toe of the shoe is absent, it puts no pressure on the dorsal sole, and it functions as an egg-bar shoe at the heels.
- Depending on the degree of stability within the foot, it must be used with appropriate sole and frog support.
- The principle disadvantage is that it concentrates stress where the dorsal margins of the branches of the shoe contact the wall.
- This shoe is most useful in horses in which there is a wound on the dorsal aspect of the sole that requires treatment and would be covered up by the toe of other shoe types.
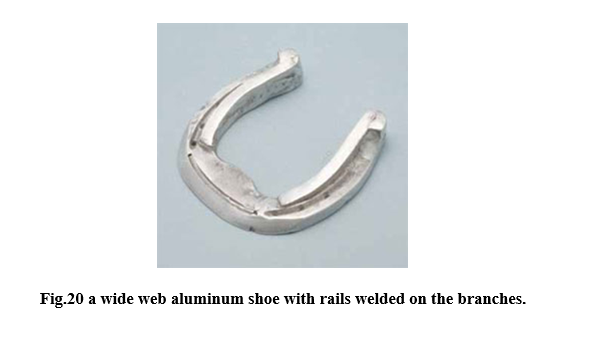
4- Wide Web Aluminum Rail Shoe
- It’s based on an open heeled pattern with square, blunt, or heavily rolled toes.
- This type of shoe makes use of "rails." Rails are narrow, wedge-shaped distal extensions that are applied to the axial side of the ground surface of the shoe.
- They elevate the heels and ease medial and lateral breakover.
- The advantage of the commercial system is that the rails can be changed to alter the height after the shoe has been applied to the horse's foot.
- When using the aluminum rail shoe, the sole and frog support is achieved by applying silicone putty between the branches of the shoe.
- The shoe provides improved breakover, heel elevation, and sole and frog support.
- The wide web aluminum shoe can also be used with a 2° or 3° bar wedge substituted for the rails.
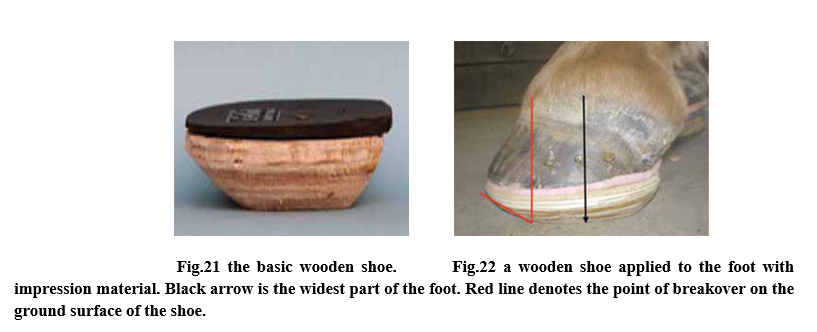
5 - Wooden Shoe
- Is generally fabricated from plywood.
- It is shaped based either on the natural shape of the foot or the closest fitting natural Balance shoe.
- The principle layer is cut out of 3/4-in plywood, and the perimeter is beveled at an angle of 45°.
- This not only moves the breakover palmarly but also moves the medial and lateral weight-bearing surfaces axially enhancing medial and lateral breakover.
- Two main modifications of this pattern have been described. In one, a second layer of 3/4-in thick rubber matting, cut to match the ground surface of the block, is screwed to the ground surface of the shoe.
- The margins of the rubber are beveled in a similar manner to the wood to further enhance breakover.
- In the second modification, a second layer of 1/2- or 3/8-in plywood is cut to match the foot side of the shoe and attached to it with glue and screws. The bevel on the front of the shoe is then increased with a rasp until the point of breakover is positioned to correspond to vertical line drawn from the coronary band.
- A layer of silicone putty is applied between the ground surface of the foot and shoe and allowed to set with the horse in a weight-bearing position.
- The shoe is attached with screws inserted through pilot holes drilled in the distal hoof wall and into the shoe.
- Alternatively, screws can be screwed into the plywood adjacent to the margin of the distal hoof wall and the shoe secured by incorporating the screw heads in a synthetic adhesive applied to the adjacent wall or by placing 2in casting tape around the perimeter of the foot.
- A wedge pad may be applied to the foot surface of the shoe to provide heel elevation if needed.
- If the sole has prolapsed below the level of the wall or if the distal phalanx has penetrated the sole, the foot surface of the shoe is recessed to remove any direct pressure from the sole and the silicone putty removed from that area.
- Aggressive therapies
1- Coronary grooving
Coronary grooving involves removing a groove of hoof wall just distal to the coronary band. It is thought to encourage dorsal hoof wall growth and improve alignment of the wall.
2- Deep digital flexor tenotomy
The approach to therapy has been to cut this tendon, either in the cannon region (mid-metacarpus) or in the pastern region. Over a time period of 6 weeks, tenotomy is thought to allow P3 to realign with the ground surface.
- Dietary Management for Laminitic Horses
1- A horse with known or suspected metabolic syndrome should be placed on the emergency diet described by the Equine Cushing’s and Insulin Resistance group.
2- Endocrinopathic laminitis is caused by high intakes of starch or simple sugars triggering elevated insulin levels in equids that have metabolic syndrome. Equines with metabolic syndrome need carbohydrate limited to 10% or less of the diet.
- Prevention of laminitis
1- A modified diet that provides adequate nutrition based on high-quality forage, digestible fiber and oil. Avoid excess carbohydrates, especially grain.
2- Routine hoof care, including regular trimming and, in some cases, therapeutic shoeing (additional radiographs may be needed to monitor progress).
3- A good health-maintenance schedule, including parasite control and vaccinations.
4- Possibly a nutritional supplement formulated to promote hoof health (biotin supplements are popular for promoting hoof growth).
5- Avoid grazing lush pastures, especially between late morning and late afternoon hours, since plant sugars are the highest during these times. Restrict pasture intake during spring or anytime the pasture suddenly greens up.
6- Avoid long standing stall rest.
7- Providing good bedding especially rubber or straw and wood shavings.
- References
1- Al-Agele R, Paul E, Dvojmoc VK, Sturrock CJ, Rauch C, Rutland CS. The anatomy, histology and physiology of the healthy and lame equine hoof. In: Rutland C, ed. Veterinary Anatomy and Physiology. London: IntechOpen; 2019.
2- Alderman, L. (2017). Everything you need to know about laminitis [Review of Everything you need to know about laminitis]. Irongate Equine Clinic. Retrieved from https://www.irongateequine.com/education/laminitis.
3- Aoun, Rita; Charles, Iyana; DeRouen, Abigail; Takawira, Catherine; Lopez, Mandi J. (2023). "Shoe configuration effects on third phalanx and capsule motion of unaffected and laminitic equine hooves in-situ". PLOS ONE. 18 (5): e0285475.
4- de Laat MA, Pollitt C. Ultrastructural examination of basement membrane pathology in horses with insulin-induced laminitis. Domest Anim Endocrinol. 2019;69: 30–34.
5- https://www.farriersformula.com.au/images/LDL/anatomy3.png.
6- Jacobs, Carrie C.; Schnabel, Lauren V.; McIlwraith, C. Wayne; Blikslager, Anthony T. (2022). "Non‐steroidal anti‐inflammatory drugs in equine orthopaedics". Equine Veterinary Journal. 54 (4): 636–648.
7- Luthersson N, Mannfalk M, Parkin TD, Harris P (2017). "Laminitis: Risk Factors and Outcome in a Group of Danish Horses" (PDF). Journal of Equine Veterinary Science. 53: 68–73.
8- MA, Christa Lesté-Lasserre (2023-10-10). "Researchers Compare Therapeutic Shoes for Horses with Laminitis". The Horse. Retrieved 2023-11-30.
9- Pollard D, Wylie C, Verheyen K, Newton J. Identification of modifiable factors associated with owner-reported equine laminitis in Britain using a web-based cohort study approach. BMC Vet Res. 2019;15(1):59.
10- Pollitt C. Lamellar function at the cellular level. In: Belknap JK, Geor RJ, eds. Equine Laminitis. 1st ed. Hoboken, NJ: JohnWiley & Sons, Inc; 2017:22–38.
11- Shulman L. "Making of a Miracle" (PDF). vet.osu.edu (reprint from The Blood-Horse). Archived (PDF) from the original on 17 December 2016. Retrieved 20 March 2017.
12- Stokes SM, Belknap JK, Engiles JB, et al. Continuous digital hypothermia prevents lamellar failure in the euglycaemic hyperinsulinaemic clamp model of equine laminitis. Equine Vet J. 2019;51(5):658–664.