Management of Pilonidal Disease
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | Management of Pilonidal Disease |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:55 AM |
Description
"last update:
22 July 2025" Download Guideline
- Executive Summary
This guideline offers evidence-based recommendations on the targeted levels of Clinical practice guidelines and provide healthcare professionals with practical guidance on the diagnosis and treatment of pilonidal sinus.
· We recommend the diagnosis of pilonidal disease clinically based on history and physical examination, with identification of midline pits, sinus tracts, and/or abscess formation in the sacrococcygeal region, (Strong Recommendation).
· We recommend a thorough patient history including risk factors such as obesity, sedentary lifestyle, family history, and recurrent infections to guide management, (Conditional Recommendation).
· Ultrasound or MRI may be recommended in recurrent or complex cases to assess the extent of sinus tracts and rule out other pathologies (e.g., perianal fistula, hidradenitis suppurativa), (Conditional Recommendation).
· We recommend incision and drainage (I&D) for the treatment of acute pilonidal abscesses, (Strong Recommendation).
· Routine postoperative antibiotics are not recommended unless there is evidence of cellulitis or systemic infection, (Conditional Recommendation).
· In patients with acute or chronic pilonidal disease without abscess, phenol application may be recommended as an effective treatment that may result in rapid and durable healing, (Strong Recommendation).
· In patients with chronic pilonidal disease without abscess, fibrin glue may be recommended as a primary or adjunctive treatment of pilonidal disease, (Conditional Recommendation).
· Endoscopic pilonidal sinus treatment (EPSiT) or pit-picking (Bascom’s procedure) may be recommended for selected patients with limited disease, (Conditional Recommendation).
· Laser surgery may be recommended to patients with PD, (Conditional Recommendation).
· We recommend open healing, (secondary intention), in presence of infection as it has lower recurrence rate, (Conditional Recommendation).
· We recommend closed techniques, (primary closure), in absence of infection as it offer faster healing, (Conditional Recommendation).
· Off-midline closure techniques (e.g., Karydakis flap, Limberg flap) for Chronic/Recurrent Disease are recommended over midline closure due to lower recurrence rates, (Strong Recommendation).
· We recommend proper wound hygiene and follow-up to monitor healing, (Good Practice Statement).
· We recommend regular hair removal (laser or shaving) in the sacrococcygeal region to reduce recurrence, (Good Practice Statement).
- Recommendations
Section 1. Diagnosis of pilonidal disease:
· We recommend the diagnosis of pilonidal disease clinically based on history and physical examination, with identification of midline pits, sinus tracts, and/or abscess formation in the sacrococcygeal region, (Strong recommendation, high certainty evidence, (6)).
· We recommend a thorough patient history including risk factors such as obesity, sedentary lifestyle, family history, and recurrent infections to guide management, (conditional recommendation, low certainty evidence, (6)).
· Ultrasound or MRI may be recommended in recurrent or complex cases to assess the extent of sinus tracts and rule out other pathologies (e.g., perianal fistula, hidradenitis suppurativa), (conditional recommendation, moderate certainty evidence, (1)).
Section 2. Management of acute abscess:
· We recommend incision and drainage (I&D) for the treatment of acute pilonidal abscesses, (Strong recommendation, moderate certainty evidence, (1)).
· Routine postoperative antibiotics are not recommended unless there is evidence of cellulitis or systemic infection, (conditional recommendation, moderate certainty evidence, (6)).
Section 3. Non-operative treatment of PNS:
· In patients with acute or chronic pilonidal disease without abscess, phenol application may be recommended as an effective treatment that may result in rapid and durable healing, (Strong recommendation, moderate certainty evidence, (6)).
· In patients with chronic pilonidal disease without abscess, fibrin glue may be recommended as a primary or adjunctive treatment of pilonidal disease, (conditional recommendation, moderate certainty evidence, (6)).
Section 4. Minimally invasive techniques for treatment of PNS:
· Endoscopic pilonidal sinus treatment (EPSiT) or pit-picking (Bascom’s procedure) may be recommended for selected patients with limited disease, (conditional recommendation, moderate certainty evidence, (6)).
Section 5. Laser treatment of PNS:
· Laser surgery may be recommended to patients with PD, (conditional recommendation, very low certainty evidence, (1)).
Section 6. Surgical treatment of PNS:
· We recommend open healing, (secondary intention), in presence of infection as it has lower recurrence rate, (conditional recommendation, moderate certainty evidence, (1)).
· We recommend closed techniques, (primary closure), in absence of infection as it offer faster healing, (conditional recommendation, moderate certainty evidence, (1)).
· Off-midline closure techniques (e.g., Karydakis flap, Limberg flap) for Chronic/Recurrent Disease are recommended over midline closure due to lower recurrence rates, (Strong recommendation, high certainty evidence, (6)).
Section 7. Post-operative care of PNS:
· We recommend proper wound hygiene and follow-up to monitor healing, (Good practice statement).
· We recommend regular hair removal (laser or shaving) in the sacrococcygeal region to reduce recurrence, (Good practice statement).
- Acknowledgement
We would like to acknowledge the Guideline General Surgery, (GGS) committee for developing this guideline.
Chair of GGS: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University. Moderator of GGS: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University. Members of GGS (Alphabetically):
Abel-Motey Hussein Aly, Professor of Surgery, Cairo University.
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University. Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University. Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University. Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University. Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University. Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II. |
|
ASCRS |
American Society of Colon and Rectal Surgeons. |
|
EPSiT |
Endoscopic Pilonidal Sinus Treatment. |
|
ESCP |
European Society of Coloproctology. |
|
GGS |
Guideline General Surgery. |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation. |
|
I & D |
Incision and Drainage. |
|
MRI |
Magnetic Resonance Imaging. |
|
PD |
Pilonidal Disease. |
|
PNS |
Pilonidal Sinus. |
- Introduction
Pilonidal disease (PD) is a benign condition affecting the natal cleft in young men and women usually between the ages of 20 and 40 years, (1). Although there are conflicting etiological theories, the current consensus holds that pilonidal disease is an acquired condition intimately related to the presence of hair in the gluteal cleft. Loose hairs trapped in the natal cleft traumatize and penetrate the skin, creating a foreign body reaction that may ultimately lead to formation of midline pits and, in some cases, secondary infection, (2). The spectrum of pilonidal disease presentation varies from a chronic cyst and/or sinus with persistent drainage and/ or extensive subcutaneous tracts to the more acute presentation of an associated abscess, (3). Numerous treatment options are available that include gluteal cleft hair removal, tract ablation, simple excision, and wide excision with flap reconstruction, (4 & 5).
This clinical practice guideline will focus on the evaluation and management of pilonidal disease.
- Scope and Purpose
The scope of this guideline is who to diagnose and treat pilonidal sinus and how to manage its complications.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target Audience
The principle targeted audiences are the practicing surgeons; however, nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence).
• Selecting only national and/or international guidelines.
• Specific range of dates for publication (using Guidelines published or updated in 2015 and later).
• Selecting peer reviewed publications only.
• Selecting guidelines written in English language.
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input.
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations.
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors.
• Date of publication, posting, and release.
• Country/language of publication
• Date of posting and/or release.
• Dates of the search used by the source guideline developers.
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GGS decided to adapt ESCP (European Society of Coloproctology) Guidelines for the Management of Pilonidal Sinus Disease, 2024 and The American Society of Colon and Rectal Surgeons, (ASCRS), Clinical Practice Guidelines for the Management of Pilonidal Disease, 2019.
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org/
· GRADE online training modules: http://cebgrade.mcmaster.ca/
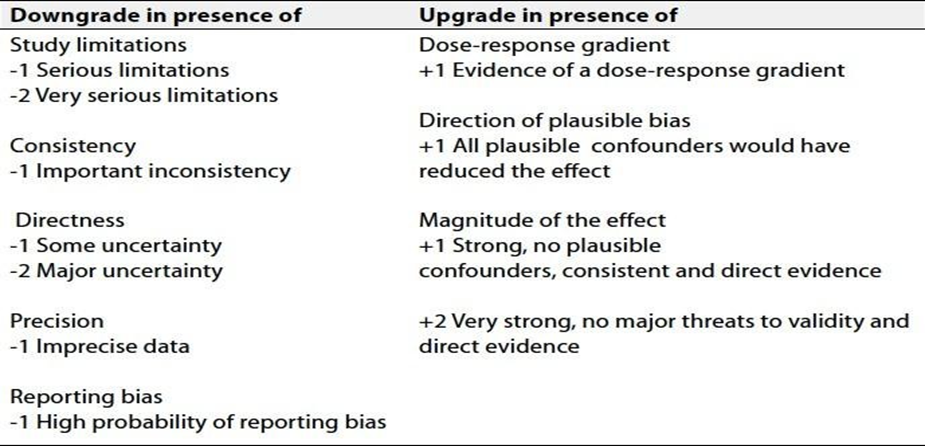
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1& 2).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research Needs
1) Role of minimally invasive technique for treatment of PNS.
2) Evaluation of simple closure versus rotation flaps in the treatment of PNS.
- Clinical Indicators for Monitoring
1) Documentation of the clinical assessment. (Acute, chronic, recurrent).
2) Documentation of the type of operation, (Open, simple closure, flap).
- Updating of the Guideline
The GGS committee for guidelines development is responsible for the continuous evaluation of evidence available about pilonidal sinus disease. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Quality and Significance of the four levels of evidence in GRADE:
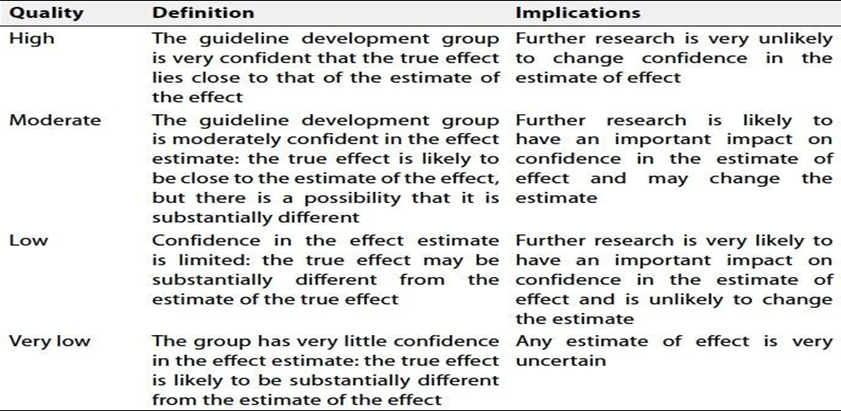
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
- Referrences
1. Ojo D, Gallo G, Kleijnen J et al. European Society of Coloproctology guidelines for the management of pilonidal disease. 2024; Br J S. 111 (10); 1- 22.
2. da Silva JH. Pilonidal cyst: cause and treatment. Dis Colon Rec- tum. 2000; 43:1146–1156.
3. Hull TL, Wu J. Pilonidal disease. Surg Clin North Am. 2002; 82:1169–1185.
4. Segre D, Pozzo M, Perinotti R, Roche B (2015) Italian Society of Colorectal Surgery: the treatment of pilonidal disease: guide- lines of the Italian Society of Colorectal Surgery (SICCR). Tech Coloproctol 19(10):607–613.
5.Iesalnieks I, Ommer A, Peterson S, Doll D, Herold A (2016) German national guideline on the management of pilonidal dis- ease. Langenbecks Arch Surg 401(5):599–609.
6. Johnson EK, Vogel JD, Cowan ML, Feingolod DL and Steele SR. Clinical practice guidelines. The American Society of Colon and Rectal Surgeons’. Clinical practice guidelines for the management of pilonidal disease. Dis Colon recum,2019; 62: 146– 157