The Management of Hemorrhoids
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | The Management of Hemorrhoids |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:51 AM |
Description
"last update:
22 July 2025" Download Guideline
- Executive Summary
This guideline offers evidence-based recommendations on the targeted levels of Clinical practice guidelines and provide healthcare professionals with practical guidance on the diagnosis and treatment of hemorrhoids.
· We recommend performing a disease-specific history and physical examination emphasizing the degree and duration of symptoms and risk factors, (Strong Recommendation).
· Complete endoscopic evaluation of the colon is recommended in select patients with symptomatic hemorrhoids and rectal bleeding, (Conditional Recommendation).
· Medical therapy for hemorrhoids is preferred as it carries minimal harm and has the potential for symptomatic relief, (Conditional Recommendation).
· Dietary and behavioral modifications are recommended as the primary first-line therapies for patients with symptomatic hemorrhoidal disease, (Strong Recommendation).
· Most patients with symptomatic grade I or II hemorrhoids and selected patients with grade III hemorrhoids refractory to conservative treatment can be effectively treated with office-based procedures. We recommend Haemorrhoid banding as an effective office-based treatment in these patients, (Strong Recommendation).
· We recommend against injection sclerotherapy for treatment of hemorrhoids and recommend RBL instead of it, (Strong Recommendation).
· We recommend against infrared coagulation for treatment of hemorrhoids and recommend RBL instead of it, (Strong Recommendation).
· We recommend early surgical evacuation of thrombosed external hemorrhoids, (Conditional Recommendation).
· Excisional hemorrhoidectomy is recommended for patients with external hemorrhoids or patients with symptomatic combined internal and external hemorrhoids (grades III–IV), (Strong Recommendation).
· Doppler-guided hemorrhoid artery ligation may be recommended for patients with internal hemorrhoids, (Conditional Recommendation).
· Stapled hemorrhoidopexy is not routinely recommended as a first-line surgical treatment for internal hemorrhoids given its marginal efficacy and significant risk, (Conditional Recommendation).
· Laser haemorrhoidoplasty (LHP), if available, is recommended for patients with first-, second-, and third-degree haemorrhoids, seeking a minimally invasive option with potentially reduced postoperative pain and quicker recovery, (Conditional Recommendation).
· Laser haemorrhoidoplasty (LHP) is not recommended for grade 4 haemorrhoids and haemorrhoidal prolapse, (Strong Recommendation).
- Recommendations
Section 1. Clinical diagnosis:
· We recommend performing a disease-specific history and physical examination emphasizing the degree and duration of symptoms and risk factors, (Strong recommendation, low certainty evidence, (2)).
Section 2. The indication for colonoscopy:
· Complete endoscopic evaluation of the colon is recommended in select patients with symptomatic hemorrhoids and rectal bleeding, (conditional recommendation, low certainty evidence, (2)).
Section 3. Medical therapy for hemorrhoids:
· Medical therapy for hemorrhoids is preferred as it carries minimal harm and has the potential for symptomatic relief, (conditional recommendation, low certainty evidence,
(2)).
· Dietary and behavioral modifications are recommended as the primary first-line therapies for patients with symptomatic hemorrhoidal disease, (strong recommendation, moderate certainty evidence, (2)).
Section 4. Non-surgical treatment, (Office treatment):
· Most patients with symptomatic grade I or II hemorrhoids and selected patients with grade III hemorrhoids refractory to conservative treatment can be effectively treated with office-based procedures. We recommend Haemorrhoid banding as an effective office-based treatment in these patients, (strong recommendation, moderate certainty evidence, (2)).
· We recommend against injection sclerotherapy for treatment of hemorrhoids and recommend RBL instead of it, (strong recommendation, moderate certainty evidence, (2)).
· We recommend against infrared coagulation for treatment of hemorrhoids and recommend RBL instead of it, (strong recommendation, moderate certainty evidence, (2)).
Section 5. Urgent manegement:
· We recommend early surgical evacuation of thrombosed external hemorrhoids, (conditional recommendation, low certainty evidence, (2)).
Section 6. Operative, (surgical) treatment:
· Excisional hemorrhoidectomy is recommended for patients with external hemorrhoids or patients with symptomatic combined internal and external hemorrhoids (grades III–IV), (strong recommendation, high certainty evidence, (2)).
· Doppler-guided hemorrhoid artery ligation may be recommended for patients with internal hemorrhoids, (conditional recommendation, moderate certainty evidence, (2)).
· Stapled hemorrhoidopexy is not routinely recommended as a first-line surgical treatment for internal hemorrhoids given its marginal efficacy and significant risk, (conditional recommendation, moderate certainty evidence, (2)).
Section 7. Laser haemorrhoidoplasty (LHP):
· Laser haemorrhoidoplasty (LHP), if available, is recommended for patients with first-, second-, and third-degree haemorrhoids, seeking a minimally invasive option with potentially reduced postoperative pain and quicker recovery, (Conditional Recommendation, moderate certainty evidence (4)).
· Laser haemorrhoidoplasty (LHP) is not recommended for grade 4 haemorrhoids and haemorrhoidal prolapse, (Strong recommendation, moderate certainty evidence (4)).
- Acknowledgement
We would like to acknowledge the guideline general surgery, (GGS) committee for developing this guideline.
Chair of GGS: Mostafa Abdel Hamed Soliman; professor of surgery, Cairo University. Moderator of GGS: Mohamed Ali Mohamed Nada, professor of surgery, Ain Shams University. Members of GGS (Alphabetically):
Abdel Motey Hussein Aly; professor of surgery, Cairo University.
Abdel Wahab Mohamed Ezzat; professor of surgery, Ain-Shams University. Ahmed Abdel Raouf Elgeidie; professor of digestive surgery, Mansoura University. Alaa Abdallah; professor of surgery, Ain-Shams University.
Atef Abdelghani Salem; professor of surgery, Benha University.
Hesham Abdel Raouf Elakad; professor of surgery, Ain Shams University. Khaled Abdallah Elfiky; professor of surgery, Ain Shams University.
Khaled Amer; professor of surgery, Military Medical Academy.
Khaled Safwat; professor of surgical oncology and endoscopy, Zagazig University. Ibrahim Elzayat; head of surgery department, Aswan University.
Mohamed Ibrahim Abdel Hamed Alsaid, professor of surgery, Zagazig University. Tarek Ibrahim; professor of surgery, National Liver Institute Menofia University.
- Abbreviations
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II. |
|
EH |
Excisional Hemorrhoidectomy. |
|
GGS |
Guideline General Surgery. |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation |
|
HAL |
Hemorrhoid Artery Ligation. |
|
ICU |
Intensive Care Unit. |
|
IRC |
Infrared Coagulation. |
|
LHP |
Laser Haemorrhoidoplasty. |
|
RBL |
Rubber Band Ligation. |
|
SH |
Stapled Hemorrhoidepexy. |
- Introduction
Hemorrhoids are vascular structures that arise from a channel of arteriovenous connective tissues and drain into the superior and inferior hemorrhoidal veins. Although hemorrhoids are categorized as external or internal based on their relationship with the dentate line, they communicate with one another and often coexist, (1).
The cardinal sign of internal hemorrhoids is painless bleeding with bowel movements; patients may also complain of intermittent tissue protrusion. Constipation and diarrhea are frequent antecedent historical features, (2).
Symptoms related to hemorrhoids are very common in the Western hemisphere and other industrialized societies. Obtaining a thorough personal and family history and performing an adequate physical examination will identify high-risk patients requiring more extensive evaluation.
Hemorrhoids may be treated medically or surgically. The ultimate judgment regarding the propriety of any specific procedure must be made by the physician in light of all the circumstances presented by the individual patient (3).
- Scope and Purpose
The scope of this guideline is who to diagnose hemorrhoids and what are the different methods to treat it.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target Audience
The principle targeted audiences are the practicing surgeons, however, gynecologists, ICU specialists and nursing staff may be included as well.
- Target Audience
The principle targeted audiences are the practicing surgeons, however, gynecologists, ICU specialists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an
Organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GGS decided to adapt The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum 2024.
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org/
· GRADE online training modules: http://cebgrade.mcmaster.ca/
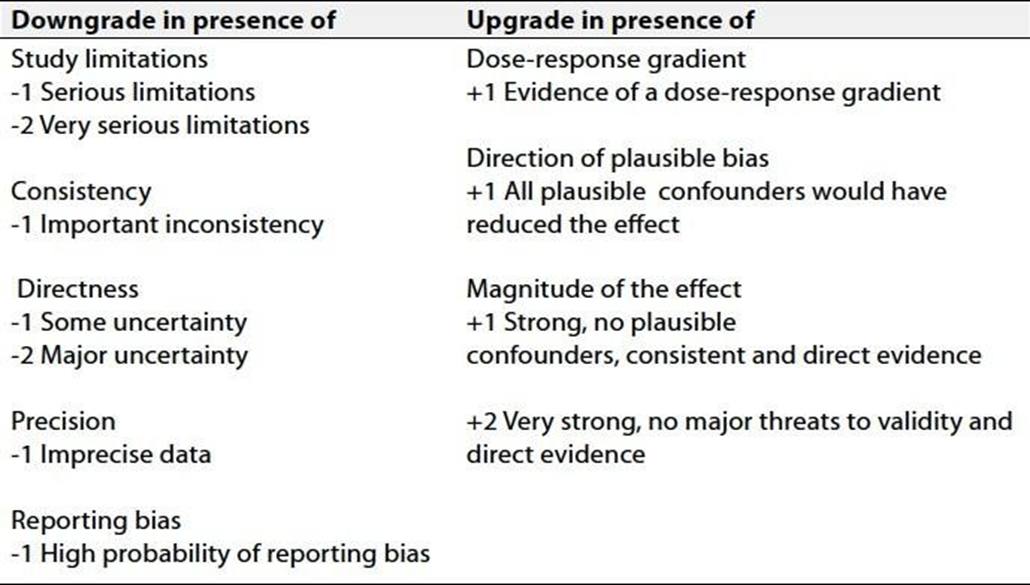
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1& 2).
The Strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research Needs
1) Non-surgical treatment of hemorrhoids.
2) The role of Laser haemorrhoidoplasty (LHP) in treatment of different degrees of hemorrhoids.
- Clinical Indicators for Monitoring
1) Documentation of the degree of hemorrhoids.
2) Documentation of the type of non-surgical treatment, (RBL, Injection Sclerotherapy, IRC, LHP).
3) Documentation of the type of surgical treatment, (EH, HAL, SH).
- Updating of the Guideline
The GGS committee for guidelines development is responsible for the continuous evaluation of evidence available about hemorrhoids. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Quality and Significance of the four levels of evidence in GRADE:
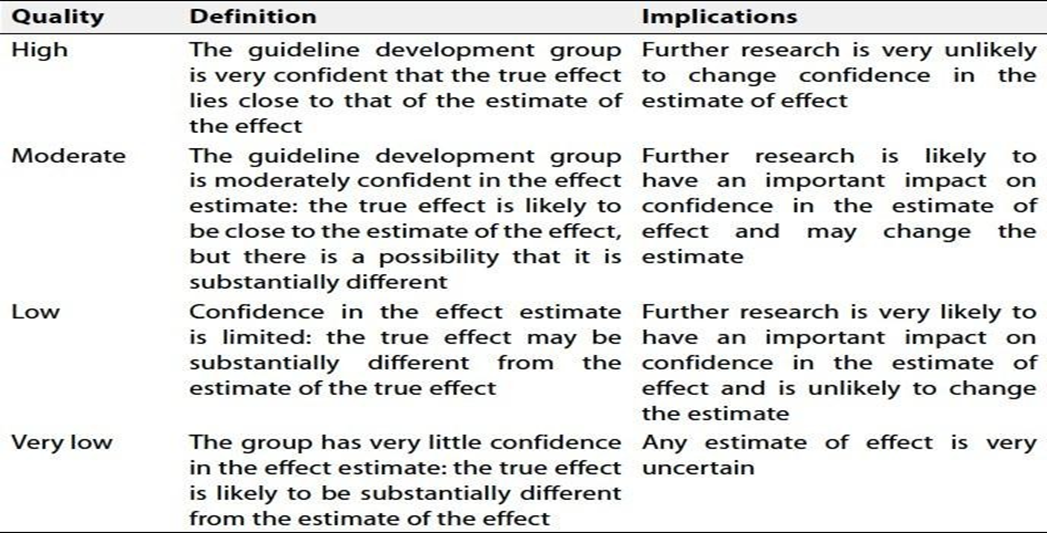
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
- References
1. Wald A; Bharucha AE; Cosman BC; and Whitehead WE.ACG clinical guideline management of benign anorectal disorders.Am J Gastroenterol.2014;109:1141-1157;quiz 1058.
2. Hawkins AT; Davis BR; Bhama AR et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum 2024; 67: 614–623: © The ASCRS 2024.
3. Davis BR; Lee-Kong SA; Migaly J; Feingold DL; and Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum 2018; 61: 284–292.
4. Lei Jin, Kaijian Qin, Renjie Wu, and Jiong Wu. Laser hemorrhoidoplasty vs. rubber band ligation: a randomized trial comparing two mini-invasive treatments for grade II hemorrhoids. BMC Surgery. 2024.(1) 24:164-169. DOI: 10.1186/s12893-024-02425-z.