Intestinal Obstruction Management
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | جراحه عامه |
| كتاب: | Intestinal Obstruction Management |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:02 AM |
الوصف
"last update:
23 July 2025" Download Guideline
- Executive Summary
This guideline offers evidence-based recommendations on the targeted levels of Clinical practice guidelines and provide healthcare professionals with practical guidance on the diagnosis and treatment of acute intestinal obstruction.
· We recommend depending on initial evaluation which include a focused history, physical examination, and basic laboratory assessment, (Strong Recommendation).
· Initial evaluation should be complemented with assessment of the laboratory tests evaluating at least blood count, lactate, and electrolytes, CRP and BUN/Creatinine, (Good Practical Statement).
· Plain X-rays may be recommended in the work-up of patients with small bowel obstruction, (Conditional Recommendation).
· Optimal diagnostic work-up should include CT scan with water soluble oral contrast in the assessment, (Strong Recommendation).
· Ultrasound may be recommended in children in special situations, (Conditional Recommendation).
· MRI may be recommended in recurrent intestinal obstruction, (Conditional Recommendation).
· In the absence of the need to perform immediate surgery, we recommend a follow-up abdominal X-ray after 24 h. (If the contrast has reached the colon, this is indicative for resolution of the bowel obstruction), (Strong Recommendation).
· Colonoscopy may be recommended in LBO to identify tumors, strictures or volvulus, (Conditional Recommendation).
· A trial of non-operative management can be recommended safely for 72 hours, (Conditional Recommendation).
· In the absence of signs that require emergent surgical exploration (i.e., peritonitis, strangulation, or bowel ischemia), non-operative management is recommended, (Conditional Recommendation).
· We recommend the use of naso-gastric tubes or long trilumen naso-intestinal tubes in non-operative management, (Strong Recommendation).
· We recommend conservative treatment for postoperative (paralytic) ileus after abdominal surgery, by implementation of enhanced recovery measures that include early oral feeding, minimizing opioid analgesics and early mobilization, (Good Practical Statement).
· We recommend exploration for patients with plain film or CT finding of SBO and clinical markers, (fever, leukocytosis, tachycardia, metabolic acidosis and continuous pain) or peritonitis on physical examination, (Strong Recommendation).
· We recommend Laparoscopic or open adhesiolysis for treatment of adhesive SBO, (Strong Recommendation).
· We recommend hernia repair with bowel resection for strangulated hernia, (Strong Recommendation).
· We recommend lower endoscopy for patients with sigmoid volvulus and without hemodynamic instability, peritonitis, or evidence of perforation to assess sigmoid colon viability, detorse the anatomy, and decompress the colon, (Conditional Recommendation).
· We recommend urgent sigmoid resection when endoscopic detorsion of the sigmoid colon fails and in cases of nonviable or perforated colon, (Strong Recommendation).
· Patients who undergo successful endoscopic detorsion should be considered for sigmoid colectomy during the same hospital admission to prevent recurrent volvulus, (Strong Recommendation).
· Endoscopic or operative fixation of the sigmoid colon may be recommended in selected patients in whom operative intervention presents a prohibitive risk, (Conditional Recommendation).
· Segmental resection is the recommended treatment for patients with cecal volvulus, (Strong Recommendation).
· We recommend emergency resection with anastomosis or diverting colostomy for patients with acute on top of chronic intestinal obstruction due to colonic cancer, (Strong Recommendation).
· Initial evaluation of ACPO should include a focused history and physical examination, baseline laboratory tests, and diagnostic imaging, (Strong Recommendation).
· We recommend supportive treatment for ACPO which includes eliminating or correcting conditions that predispose patients to ACPO or prolong its course (e.g. immobility, neurological disorders, etc.), (Strong Recommendation).
· Pharmacologic treatment with neostigmine is recommended when ACPO does not resolve with supportive therapy, (Strong Recommendation).
· Endoscopic colonic decompression is recommended in patients with ACPO in whom neostigmine therapy is contraindicated or ineffective, (Strong Recommendation).
· Operative treatment is recommended for ACPO complicated by colon ischemia or perforation or ACPO refractory to pharmacologic and endoscopic therapies, (Conditional Recommendation).
- Recommendations
Section I. Clinical Diagnosis of Intestinal Obstruction:
· We recommend depending on initial evaluation which include a focused history, physical examination, and basic laboratory assessment, (Strong recommendation, low certainty evidence, (3)).
Section II. Laboratory Work-Up for Intestinal Obstruction:
· Initial evaluation should be complemented with assessment of the laboratory tests evaluating at least blood count, lactate, electrolytes, CRP and BUN/Creatinine, (Good practical statement).
Section III. Diagnostic imaging for Intestinal Obstruction:
· Plain X-rays may be recommended in the work-up of patients with small bowel obstruction, (Conditional recommendation, low certainty evidence, (7)).
· Optimal diagnostic work-up should include CT scan with water soluble oral contrast in the assessment, (Strong recommendation, moderate certainty evidence, (7)).
· Ultrasound may be recommended in children in special situations, (Conditional recommendation, low certainty evidence, (7)).
· MRI may be recommended in recurrent intestinal obstruction, (Conditional recommendation, low certainty evidence, (7)).
· In the absence of the need to perform immediate surgery, we recommend a follow-up abdominal X-ray after 24 h. (If the contrast has reached the colon, this is indicative for resolution of the bowel obstruction), (Strong recommendation, moderate certainty evidence, (7)).
· Colonoscopy may be recommended in LBO to identify tumors, strictures or volvulus, (Conditional recommendation, low certainty evidence, (7)).
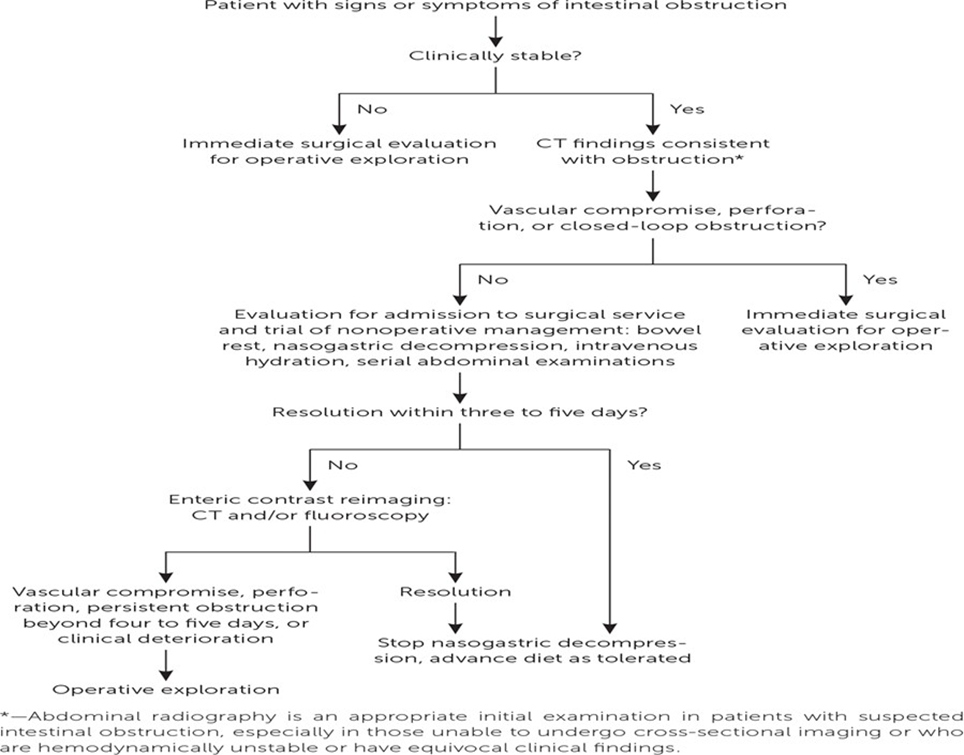
Section IV. Conservative (Non-Operative) Management, (Figure 1)(8):
· A trial of non-operative management can be recommended safely for 72 hours, (Conditional recommendation, moderate certainty evidence, (7)).
· In the absence of signs that require emergent surgical exploration (i.e., peritonitis, strangulation, or bowel ischemia), non-operative management is recommended, (Conditional recommendation, low certainty evidence, (7)).
· We recommend the use of naso-gastric tubes or long trilumen naso-intestinal tubes in non-operative management, (Strong recommendation, high certainty evidence, (7)).
· We recommend conservative treatment for postoperative (paralytic) ileus after abdominal surgery, by implementation of enhanced recovery measures that include early oral feeding, minimizing opioid analgesics and early mobilization, (Good practical statement).
Section V. Surgical management:
· We recommend exploration for patients with plain film or CT finding of SBO and clinical markers, (fever, leukocytosis, tachycardia, metabolic acidosis and continuous pain) or peritonitis on physical examination, (Strong recommendation, high certainty evidence, (7)).
· We recommend Laparoscopic or open adhesiolysis for treatment of adhesive SBO, (Strong recommendation, high certainty evidence, (7)).
Section VI. Special considerations:
· We recommend hernia repair with bowel resection for strangulated hernia, (Strong recommendation, high certainty evidence, (7)).
· We recommend lower endoscopy for patients with sigmoid volvulus and without hemodynamic instability, peritonitis, or evidence of perforation to assess sigmoid colon viability, detorse the anatomy, and decompress the colon, (Conditional recommendation, low certainty evidence, (3)).
· We recommend urgent sigmoid resection when endoscopic detorsion of the sigmoid colon fails and in cases of nonviable or perforated colon, (Strong recommendation, moderate certainty evidence, (3)).
· Patients who undergo successful endoscopic detorsion should be considered for sigmoid colectomy during the same hospital admission to prevent recurrent volvulus, (Strong recommendation, moderate certainty evidence, (3)).
· Endoscopic or operative fixation of the sigmoid colon may be recommended in selected patients in whom operative intervention presents a prohibitive risk, (Conditional recommendation, low certainty evidence, (3)).
· Segmental resection is the recommended treatment for patients with cecal volvulus, (Strong recommendation, moderate certainty evidence, (3)).
· We recommend emergency resection with anastomosis or diverting colostomy for patients with acute on top of chronic intestinal obstruction due to colonic cancer, (Strong recommendation, moderate certainty evidence, (7)).
Section VII. Acute colonic pseudo-obstruction:
· Initial evaluation of ACPO should include a focused history and physical examination, baseline laboratory tests, and diagnostic imaging, (Strong recommendation, moderate certainty evidence, (3)).
· We recommend supportive treatment for ACPO which includes eliminating or correcting conditions that predispose patients to ACPO or prolong its course (e.g. immobility, neurological disorders, etc.), (Strong recommendation, moderate certainty evidence, (7)).
· Pharmacologic treatment with neostigmine is recommended when ACPO does not resolve with supportive therapy, (Strong recommendation, moderate certainty evidence, (7)).
· Endoscopic colonic decompression is recommended in patients with ACPO in whom neostigmine therapy is contraindicated or ineffective, (Strong recommendation, moderate certainty evidence, (7)).
· Operative treatment is recommended for ACPO complicated by colon ischemia or perforation or ACPO refractory to pharmacologic and endoscopic therapies, (Conditional recommendation, low certainty evidence, (7)).
- Acknowledgement
We would like to acknowledge the Guideline General Surgery, (GGS) committee for developing this guideline.
Chair of GGS: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University. Moderator of GGS: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University. Members of GGS (Alphabetically):
Abel-Motey Hussein Aly, Professor of Surgery, Cairo University.
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University. Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University. Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University. Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University. Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University. Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
ASBO |
Adhesive Small Bowel Obstruction |
|
ACPO |
Acute Colonic Pseudo-Obstruction |
|
CT |
Computerized Tomography. |
|
GGS |
Guideline General Surgery |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation |
|
ICU |
Intensive Care Unit |
|
LBO |
Large Bowel Obstruction |
|
NGT |
Naso-Gastric Tube |
|
SBO |
Small Bowel Obstruction |
|
WHO |
World Health Organization |
- Introduction
Intestinal obstruction is a critical surgical emergency that requires timely and effective management to prevent complications such as ischemia, perforation, sepsis, and mortality. Acute intestinal obstruction occurs when a mechanical obstruction disrupts or blocks the normal movement of intestinal contents. It is estimated to affect 2% to 8% of patients who visit the emergency department. While the rates of morbidity and mortality related to acute intestinal obstruction have decreased, managing the condition remains complex. The choice between non- operative management and surgical intervention should be made cautiously by skilled healthcare providers, (1). The primary causes of acute intestinal obstruction are adhesions, neoplasms, and herniation. Adhesions, typically resulting from previous abdominal surgeries, are the leading cause of small bowel obstruction (SBO), responsible for 60% to 75% of cases. Lower abdominal and pelvic surgeries, such as appendectomy, colorectal, gynecologic surgeries, and hernia repairs, carry a higher risk of adhesive SBO. Obstructions caused by neoplasms are uncommon and are more frequently seen in the large bowel. Other potential causes include inflammatory bowel disease, intestinal intussusception, volvulus, intra-abdominal collections, gallstones, and foreign bodies, (2). This document serves as a comprehensive guideline for surgeons, providing an evidence-based approach to the classification, diagnosis, and treatment of intestinal obstruction.
- Scope and Purpose
The scope of this guideline is to set recommendations for the diagnose and treatment of acute intestinal obstruction.
The main purpose of these guidelines is to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the good surgical practice to our patients, and finally to be cost effective.
- Target Audience
The principle targeted candidates are the practicing surgeons, however endoscopists, radiologists, ICU specialists and nursing staff may be included.
- Methods
A comprehensive search for guidelines was undertaken to identify the relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines
· Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
· Selecting peer reviewed publications only
· Selecting guidelines written in English language
· Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GGS decided to adapt the Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2013 update of the evidence-based guidelines from the World Society of Emergency Surgery ASBO Working Group and guidelines for management of small bowel obstruction, 2008.
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org/
· GRADE online training modules: http://cebgrade.mcmaster.ca/
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1& 2).
The strength of the recommendation
The
strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong
recommendations, the guideline communicates the message that the desirable
effects of adherence to the recommendation outweigh the undesirable effects.
This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are
made when there is greater uncertainty about the four factors above or if local
adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention
suitable for some, but not for other locations. This means that there is a need
for substantial debate and involvement of stakeholders before this recommendation
can be adopted as policy.
When not to make
recommendations
When there is lack of evidence
on the effectiveness of an intervention, it may be appropriate not to
make a recommendation.
- Research Needs
1. Non operative management of SBO.
2. Management of ACPO.
- Clinical Indicators for Monitoring
1. Documentation of symptoms and signs of ABO.
2. CBC, Serum electrolytes, lactate.
3. CT.
4. Documentation of the type of treatment, (Non-operative, endoscopic, operative).
- Updating of the Guideline
The GGS committee for guidelines development is responsible for the continuous evaluation of evidence available about acute intestinal obstruction. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Quality
and Significance of the four levels of evidence in GRADE
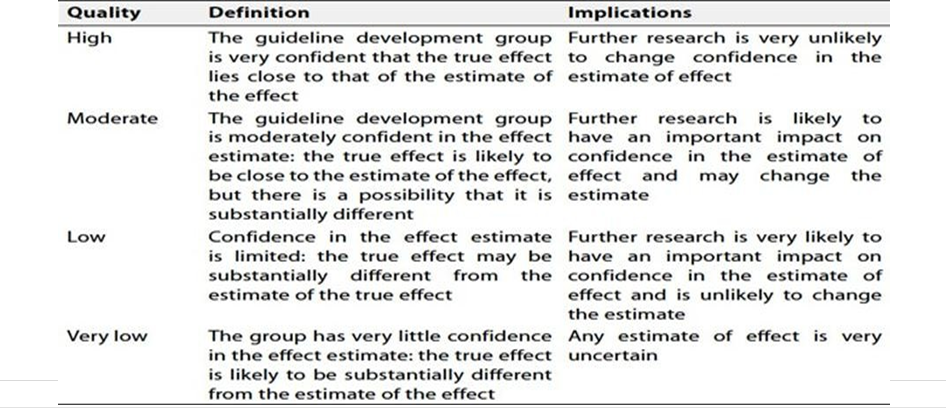
Table 2 factors that determine How to upgrade or downgrade the quality of evidence
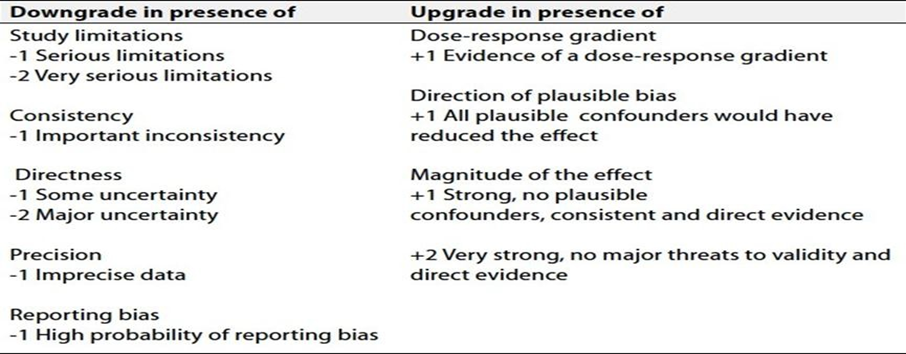
Table 3 Causes of intestinal obstruction, (1, 4, 6)
|
1. Adhesive disease |
60- 75% |
|
2. Neoplasm |
13- 20% |
|
3. Herniation |
2- 15% |
|
4. Inflammatory bowel disease |
5- 7% |
|
5. Volvulus |
<5% |
|
6. Others |
5- 7% |
Table 4 Differential diagnosis of intestinal obstruction
|
Diagnosis |
Clues |
|
Medication adverse effects (diagnosis of exclusion) |
Review of medication (tricyclic antidepressant, narcotics, etc) |
|
Mesenteric ischemia |
History of peripheral vascular disease or postprandial abdominal angina, hypercoagulable state recent use of vasopressor |
|
Perforated viscus Intra-abdominal sepsis |
Ever, leukocytosis, peritonitis pneumoperitoneum |
|
Post-operative paralytic ileus |
Recent abdominal surgery with no post- operative flatus or bowel movement |
|
Pseudo-obstruction (Ogilvie syndrome) |
Acutely dilated large intestine, Diabetes Mellitus, history of intestinal dysmotility, sclerderma |
Figure 1 Management of acute intestinal obstruction (8)
- References
1.
Jackson P, Vigiola Cruz M. Intestinal Obstruction:
Evaluation and Management. Am Fam Physician. 2018 Sep 15;98(6):362-367. PMID:
30215917.
2.
Taylor MR, Lalani
N. Adult small
bowel obstruction. Acad Emerg Med. 2013; 20(6):528-544.
3. Di Saverio S, Coccolini F, Galati M, et al. Bologna
guidelines for diagnosis and management of adhesive small bowel obstruction
(ASBO): 2013 update of the evidence-based guidelines from the World Society
of Emergency Surgery
ASBO Working Group. World J Emerg Surg. 2013
4. Leung AM, Vu H. Factors predicting need for and delay in surgery in small bowel obstruction. Am Surg. 2012;78(4):403-407.
5. ten Broek RP, Issa Y, van Santbrink EJ, et al. Burden of adhesions in abdominal and pelvic surgery: systematic review and meta-analysis. BMJ. 2013; 347:f5588.
6. Branco BC, Barmparas G, Schnüriger B, Inaba K, Chan LS, Demetriades D. Systematic review and meta-analysis of the diagnostic and therapeutic role of water-soluble contrast agent in adhesive small bowel obstruction. Br J Surg. 2010;97(4):470-478.
7. Diaz JJ Jr, Bokhari F, Mowery NT, Acosta JA, Block EF, Bromberg WJ, Collier BR, Cullinane DC, Dwyer KM, Griffen MM, Mayberry JC, Jerome R. Guidelines for management of small bowel obstruction. J Trauma. 2008 Jun; 64(6):1651-64. doi: 10.1097/TA.0b013e31816f709e. PMID: 18545135.
8. Jackson PG and Raiji M. Evaluation and management of intestinal obstruction. American Family Physician. 2011; 83 (2): 159- 165