Transmission Based Precautions
| Site: | EHC | Egyptian Health Council |
| Course: | Infection Prevention and Control Guidelines |
| Book: | Transmission Based Precautions |
| Printed by: | Guest user |
| Date: | Sunday, 26 July 2026, 10:38 AM |
Description
"last update: 28 July 2025" Download Guideline
- Executive Summary
Transmission-based precautions are applied in addition to standard precautions when the patients have suspected or confirmed infectious diseases that are transmitted by the contact, droplet or airborne routes.
Early institution (application) in healthcare settings of transmission-based precautions upon suspicion reduces risk of further transmission of communicable diseases. Isolation decision is based on risk assessment and should be recorded in patient file. Type of transmission-based precautions depends on the mode of transmission of infection: contact, droplet or airborne.
Infection can be transmitted by direct or indirect contact with infected or colonized people. Some infectious diseases can be transmitted before clinical signs and symptoms appear such as influenza and Covid-19. The need to discontinue transmission-based precautions should be reviewed daily.
|
Recommendations |
|
General principles In addition to Standard Precautions, use Transmission-Based Precautions for patients with documented (confirmed) or suspected infection or colonization with highly transmissible or epidemiologically-important pathogens for which additional precautions are needed to prevent transmission (Strong Recommendation) |
|
Extend duration of Transmission-Based Precautions, (e.g., Droplet, Contact) for immunosuppressed patients with viral infections due to prolonged shedding of viral agents that may be transmitted to others (Strong Recommendation) |
|
Consistent with the persons (patients) care needs, minimize the number of healthcare workers and the time healthcare workers are exposed to an infectious patient (Good Practice Statement) |
|
Contact Precautions |
|
Contact precautions, in addition to standard precautions, are implemented in the presence of known or suspected infectious agents that are spread by direct or indirect contact with the patient or the patient's environment (Strong Recommendation) |
|
Patient placement ● Place patients who require Contact Precautions in a single-patient room when available (Strong Recommendation) ● When single-patient rooms are in short supply, apply the following principles for making decisions on patient placement: 1. Prioritize patients with conditions that may facilitate transmission (e.g., uncontained drainage, stool incontinence) for single-patient room placement. (Good Practice Statement) 2. Place together in the same room (cohort) patients who are infected or colonized with the same pathogen and are suitable roommates (Strong Recommendation) |
|
If it becomes necessary to place a patient who requires Contact Precautions in a room with a patient who is not infected or colonized with the same infectious agent: 1. Avoid placing patients on Contact Precautions in the same room with patients who have conditions that may increase the risk of adverse outcome from infection or that may facilitate transmission (e.g., those who are immunocompromised, have open wounds, or have anticipated prolonged lengths of stay) (Good Practice Statement) 2. Ensure that patients are physically separated (i.e., >3 feet/ 1 meter apart) from each other. Draw the privacy curtain between beds to minimize opportunities for direct contact (Good Practice Statement) 3. Change protective attire and perform hand hygiene between contact with patients in the same room, regardless of whether one or both patients are on Contact Precautions (Strong Recommendation) |
|
Use of personal protective equipment ● Gloves Wear gloves whenever touching the patient’s intact skin or surfaces and articles in close proximity to the patient (e.g., medical equipment, bed rails). Don/ put on gloves upon entry into the room or cubicle (Strong Recommendation) ● Gowns Wear a gown whenever anticipating that clothing will have direct contact with the patient or potentially contaminated environmental surfaces or equipment in close proximity to the patient. Don/ put on gown upon entry into the room or cubicle. Remove gown and observe hand hygiene before leaving the patient-care environment (Strong Recommendation) After gown removal, ensure that clothing and skin do not contact potentially contaminated environmental surfaces that could result in possible transfer of microorganism to other patients or environmental surfaces (Good Practice Statement) |
|
Patient transport ● Limit transport and movement of patients outside of the room to medically-necessary purposes. (Good Practice Statement) ● When transport or movement in any healthcare setting is necessary, ensure that infected or colonized areas of the patient’s body are contained and covered. (Good Practice Statement) ● Remove and dispose of contaminated PPE and perform hand hygiene prior to transporting patients on Contact Precautions. (Good Practice Statement) ● Don/ put on clean PPE to handle the patient at the transport destination. (Good Practice Statement) |
|
Patient-care equipment and instruments/devices · Handle patient-care equipment and instruments/devices according to Standard Precautions (Strong Recommendation) · Use disposable noncritical patient-care equipment (e.g., blood pressure cuffs) or implement patient-dedicated use of such equipment. If common use of equipment for multiple patients is unavoidable, clean and disinfect such equipment before use on another patient (Strong Recommendation) |
|
Environmental measures · Ensure that rooms of patients on Contact Precautions are prioritized for frequent cleaning and disinfection (e.g., at least daily) with a focus on frequently-touched surfaces (e.g., bed rails, overbed table, bedside commode, lavatory surfaces in patient bathrooms, doorknobs) and equipment in the immediate vicinity of the patient. (Strong Recommendation) · Discontinue Contact Precautions after signs and symptoms of the infection have resolved or according to pathogen-specific Recommendation (Strong Recommendation)
|
|
Droplet Precautions |
|
Use Droplet Precautions for patients known or suspected to be infected with pathogens transmitted by respiratory droplets (i.e., large-particle droplets >5µ in size) that are generated by a patient who is coughing, sneezing or talking (Strong Recommendation) |
|
Patient placement Place patients who require Droplet Precautions in a single-patient room when available (Good Practice Statement) |
|
When single-patient rooms are in short supply, apply the following principles for making decisions on patient placement: · Prioritize patients who have excessive cough and sputum production for single-patient room placement (Good Practice Statement) · Place together in the same room (cohort) patients who are infected with the same pathogen and are suitable roommates (Strong Recommendation) |
|
If it becomes necessary to place patients who require Droplet Precautions in a room with a patient who does not have the same infection: · Avoid placing patients on Droplet Precautions in the same room with patients who have conditions that may increase the risk of adverse outcome from infection or that may facilitate transmission (e.g., those who are immunocompromised, have or have anticipated prolonged lengths of stay). (Good Practice Statement) · Ensure that patients are physically separated (i.e., >3 feet apart/ 1 meter) from each other. Draw the privacy curtain between beds to minimize opportunities for close contact (Strong Recommendation) · Change protective attire and perform hand hygiene between contact with patients in the same room, regardless of whether one patient or both patients are on Droplet Precautions (Strong Recommendation) |
|
Use of personal protective equipment · Don/ put on a mask upon entry into the patient room or cubicle (Strong Recommendation) |
|
Patient transport · Limit transport and movement of patients outside of the room to medically necessary purposes. (Good Practice Statement) · If transport or movement in any healthcare setting is necessary, instruct patient to wear a mask and follow Respiratory Hygiene/Cough Etiquette. (Strong Recommendation) · Discontinue Droplet Precautions after signs and symptoms have resolved or according to pathogen-specific recommendation. (Strong Recommendation) |
|
Airborne Precautions |
|
Use Airborne Precautions for patients known or suspected to be infected with infectious agents transmitted person-to-person by the airborne route (Strong Recommendation) |
|
Patient placement · Place patients who require Airborne Precautions in an airborne infection isolation room (AIIR) (Strong Recommendation) · Provide at least six (existing facility) or 12 (new construction/renovation) air changes per hour. (Strong Recommendation) · Direct exhaust of air to the outside. If it is not possible to exhaust air from an AIIR directly to the outside, the air may be returned to the air-handling system or adjacent spaces if all air is directed through HEPA filters. (Strong Recommendation) · Whenever an AIIR is in use for a patient on Airborne Precautions, monitor air pressure daily with visual indicators (e.g., smoke tubes, flutter strips), regardless of the presence of differential pressure sensing devices (e.g., manometers). (Strong Recommendation) · Keep the AIIR door closed when not required for entry and exit. (Strong Recommendation) |
|
Develop systems (e.g., triage, signage) to identify patients with known or suspected infections that require Airborne Precautions upon entry into health care setting (Strong Recommendation) |
|
Place the patient in an AIIR as soon as possible. If an AIIR is not available, place a surgical mask on the patient and place him/her in an examination room. Once the patient leaves, the room should remain vacant for the appropriate time, generally one hour, to allow for a full exchange of air (Strong Recommendation) |
|
Instruct patients with a known or suspected airborne infection to wear a surgical mask and observe Respiratory Hygiene/Cough Etiquette. Once in an AIIR, the mask may be removed; the mask should remain on if the patient is not in an AIIR (Strong Recommendation) |
|
Personnel restrictions. Restrict susceptible healthcare personnel from entering the rooms of patients known (confirmed) or suspected to have measles (rubeola), varicella (chickenpox), disseminated zoster, or smallpox if other immune healthcare personnel are available (Strong Recommendation) |
|
Use of PPE Wear a fit-tested NIOSH-approved N95, FFP2 respirator or higher-level respirator for respiratory protection when entering the room of a patient when the following diseases are suspected or confirmed: · Infectious pulmonary or laryngeal tuberculosis or when infectious tuberculosis skin lesions are present and procedures that would aerosolize viable organisms (e.g., irrigation, incision and drainage, whirlpool treatments) are performed (Strong Recommendation) |
|
Patient transport · Limit transport and movement of patients outside of the room to medically necessary purposes. (Good Practice Statement) · If transport or movement outside an AIIR is necessary, instruct patients to wear a surgical mask, and observe Respiratory Hygiene/Cough Etiquette (Good Practice Statement) · For patients with skin lesions associated with varicella or smallpox or draining skin lesions caused by M. tuberculosis, cover the affected areas to prevent aerosolization or contact with the infectious agent in skin lesions (Strong Recommendation) · Discontinue Airborne Precautions according to pathogen-specific Recommendation. (Strong Recommendation) |
- Recommendation
|
General principles In addition to Standard Precautions, use Transmission-Based Precautions for patients with documented or suspected infection or colonization with highly transmissible or epidemiologically-important pathogens for which additional precautions are needed to prevent transmission (Strong Recommendation, High Grade Evidence) |
|
Extend duration of Transmission-Based Precautions, (e.g., Droplet, Contact) for immunosuppressed patients with viral infections due to prolonged shedding of viral agents that may be transmitted to others (Strong Recommendation, High Grade Evidence) |
|
Consistent with the persons care needs, minimize the number of healthcare workers and the time healthcare workers are exposed to an infectious patient. (Good Practice Statement) |
|
Contact Precautions |
|
Contact precautions, in addition to standard precautions, are implemented in the presence of known or suspected infectious agents that are spread by direct or indirect contact with the patient or the patient's environment. (Strong Recommendation, High Grade Evidence)
|
|
Patient placement Place patients who require Contact Precautions in a single-patient room when available (Strong Recommendation, Moderate Grade Evidence) |
|
When single-patient rooms are in short supply, apply the following principles for making decisions on patient placement: · Prioritize patients with conditions that may facilitate transmission (e.g., uncontained drainage, stool incontinence) for single-patient room placement. (Good Practice Statement) · Place together in the same room (cohort) patients who are infected with or colonized with the same pathogen and are suitable roommates. (Strong Recommendation, Moderate Grade Evidence) |
|
If it becomes necessary to place a patient who requires Contact Precautions in a room with a patient who is not infected or colonized with the same infectious agent: · Avoid placing patients on Contact Precautions in the same room with patients who have conditions that may increase the risk of adverse outcome from infection or that may facilitate transmission (e.g., those who are immunocompromised, have open wounds, or have anticipated prolonged lengths of stay). (Good Practice Statement) · Ensure that patients are physically separated (i.e., >3 feet apart) from each other. Draw the privacy curtain between beds to minimize opportunities for direct contact. (Good Practice Statement) · Change protective attire and perform hand hygiene between contact with patients in the same room, regardless of whether one or both patients are on Contact Precautions. (Strong Recommendation, Moderate Grade Evidence)
|
|
Use of personal protective equipment · Gloves Wear gloves whenever touching the patient’s intact skin or surfaces and articles in close proximity to the patient (e.g., medical equipment, bed rails). Don/ put on gloves upon entry into the room or cubicle. (Strong Recommendation, Moderate Grade Evidence) · Gowns Wear a gown whenever anticipating that clothing will have direct contact with the patient or potentially contaminated environmental surfaces or equipment in close proximity to the patient. Don/ put on gown upon entry into the room or cubicle. Remove gown and observe hand hygiene before leaving the patient-care environment (Strong Recommendation, Moderate Grade Evidence) After gown removal, ensure that clothing and skin do not contact potentially contaminated environmental surfaces that could result in possible transfer of microorganism to other patients or environmental surfaces (Good Practice Statement) |
|
Patient transport · Limit transport and movement of patients outside of the room to medically-necessary purposes. (Good Practice Statement) · When transport or movement in any healthcare setting is necessary, ensure that infected or colonized areas of the patient’s body are contained and covered. (Good Practice Statement) · Remove and dispose of contaminated PPE and perform hand hygiene prior to transporting patients on Contact Precautions. (Good Practice Statement) · Don/ put on clean PPE to handle the patient at the transport destination. (Good Practice Statement) |
|
Patient-care equipment and instruments/devices · Handle patient-care equipment and instruments/devices according to Standard Precautions (Strong Recommendation, Moderate Grade Evidence) · Use disposable noncritical patient-care equipment (e.g., blood pressure cuffs) or implement patient-dedicated use of such equipment. If common use of equipment for multiple patients is unavoidable, clean and disinfect such equipment before use on another patient (Strong Recommendation, Moderate Grade Evidence) |
|
Environmental measures • Ensure that rooms of patients on Contact Precautions are prioritized for frequent cleaning and disinfection (e.g., at least daily) with a focus on frequently-touched surfaces (e.g., bed rails, overbed table, bedside commode, lavatory surfaces in patient bathrooms, doorknobs) and equipment in the immediate vicinity of the patient. (Strong Recommendation, Moderate Grade Evidence) • Discontinue Contact Precautions after signs and symptoms of the infection have resolved or according to pathogen-specific Recommendation (Strong Recommendation, Moderate Grade Evidence) |
|
Droplet Precaution |
|
Use Droplet Precautions for patients known or suspected to be infected with pathogens transmitted by respiratory droplets (i.e., large-particle droplets >5µ in size) that are generated by a patient who is coughing, sneezing or talking (Strong Recommendation, Moderate Grade Evidence) |
|
· Patient placement Place patients who require Droplet Precautions in a single-patient room when available (Good Practice Statement) |
|
When single-patient rooms are in short supply, apply the following principles for making decisions on patient placement: · Prioritize patients who have excessive cough and sputum production for single-patient room placement (Good Practice Statement) · Place together in the same room (cohort) patients who are infected with the same pathogen and are suitable roommates (Strong Recommendation, Moderate Grade Evidence) |
|
If it becomes necessary to place patients who require Droplet Precautions in a room with a patient who does not have the same infection: · Avoid placing patients on Droplet Precautions in the same room with patients who have conditions that may increase the risk of adverse outcome from infection or that may facilitate transmission (e.g., those who are immunocompromised, have or have anticipated prolonged lengths of stay). (Good Practice Statement) · Ensure that patients are physically separated (i.e., >3 feet apart) from each other. Draw the privacy curtain between beds to minimize opportunities for close contact (Strong Recommendation, Moderate Grade Evidence) · Change protective attire and perform hand hygiene between contact with patients in the same room, regardless of whether one patient or both patients are on Droplet Precautions (Strong Recommendation, Moderate Grade Evidence) |
|
Use of personal protective equipment • Don/ put on a mask upon entry into the patient room or cubicle (Strong Recommendation, Moderate Grade Evidence) |
|
Patient transport · Limit transport and movement of patients outside of the room to medically-necessary purposes. (Good Practice Statement) · If transport or movement in any healthcare setting is necessary, instruct patient to wear a mask and follow Respiratory Hygiene/Cough Etiquette. (Strong Recommendation, Moderate Grade Evidence) · Discontinue Droplet Precautions after signs and symptoms have resolved or according to pathogen-specific recommendation. (Strong Recommendation, Moderate Grade Evidence) |
|
Airborne Precautions |
|
Use Airborne Precautions for patients known or suspected to be infected with infectious agents transmitted person-to-person by the airborne route (Strong Recommendation, High Grade Evidence)
|
|
Patient placement Place patients who require Airborne Precautions in an air borne infection isolation room (AIIR) · Provide at least six (existing facility) or 12 (new construction/renovation) air changes per hour. (Strong Recommendation, High Grade Evidence) · Direct exhaust of air to the outside. If it is not possible to exhaust air from an AIIR directly to the outside, the air may be returned to the air-handling system or adjacent spaces if all air is directed through HEPA filters. (Strong Recommendation, High Grade Evidence) · Whenever an AIIR is in use for a patient on Airborne Precautions, monitor air pressure daily with visual indicators (e.g., smoke tubes, flutter strips), regardless of the presence of differential pressure sensing devices (e.g., manometers). (Strong Recommendation, High Grade Evidence) · Keep the AIIR door closed when not required for entry and exit. (Strong Recommendation, High Grade Evidence)
|
|
Develop systems (e.g., triage, signage) to identify patients with known or suspected infections that require Airborne Precautions upon entry into health care setting (Strong Recommendation, High Grade Evidence)
|
|
Place the patient in an AIIR as soon as possible. If an AIIR is not available, place a surgical mask on the patient and place him/her in an examination room. Once the patient leaves, the room should remain vacant for the appropriate time, generally one hour, to allow for a full exchange of air (Strong Recommendation, Moderate Grade Evidence) |
|
Instruct patients with a known or suspected airborne infection to wear a surgical mask and observe Respiratory Hygiene/Cough Etiquette. Once in an AIIR, the mask may be removed; the mask should remain on if the patient is not in an AIIR (Strong Recommendation, Moderate Grade Evidence) |
|
Personnel restrictions. Restrict susceptible healthcare personnel from entering the rooms of patients known or suspected to have measles (rubeola), varicella (chickenpox), disseminated zoster, or smallpox if other immune healthcare personnel are available (Strong Recommendation, Moderate Grade Evidence) |
|
Use of PPE Wear a fit-tested NIOSH-approved N95 , FFP2 respirator or higher level respirator for respiratory protection when entering the room or home of a patient when the following diseases are suspected or confirmed: · Infectious pulmonary or laryngeal tuberculosis or when infectious tuberculosis skin lesions are present and procedures that would aerosolize viable organisms (e.g., irrigation, incision and drainage, whirlpool treatments) are performed (Strong Recommendation, Moderate Grade Evidence) |
|
Patient transport Limit transport and movement of patients outside of the room to medically-necessary purposes. (Good Practice Statement) If transport or movement outside an AIIR is necessary, instruct patients to wear a surgical mask, and observe Respiratory Hygiene/Cough Etiquette (Good Practice Statement) For patients with skin lesions associated with varicella or smallpox or draining skin lesions caused by M. tuberculosis, cover the affected areas to prevent aerosolization or contact with the infectious agent in skin lesions (Strong Recommendation, Moderate Grade Evidence) Discontinue Airborne Precautions according to pathogen-specific Recommendation. (Strong Recommendation, Moderate Grade Evidence) |
Rationale
· Transmission of infectious agents within a healthcare setting requires three elements: a source (or reservoir) of infectious agents, a susceptible host with a portal of entry receptive to the agent, and a mode of transmission for the agent
· Standard precautions may be insufficient to prevent cross transmission of specific infectious agents and additional precautions called “Transmission Based Precautions” (TBP) may be required when caring for patients with known / suspected infection or colonisation.
· These measures are designed to protect patients/residents, staff, and visitors from contact with infectious agents.
· Transmission Based Precautions are categorised by the route of transmission of infectious agents (some infectious agents can be transmitted by more than one route).
Contact precautions
· There is supportive evidence and a strong theoretical rationale to support the use of contact precautions with standard precautions for patients known or suspected to be infected with an infectious agent spread via the contact route.
· The rationale for single patient rooms for patients who require contact precautions include:
- It helps to reduce contact between the person in the room and other people.
- Access to a dedicated bathroom which is not shared with other people can reduce the spread of C. difficile and other infectious microorganisms.
- The door and signage can help to remind healthcare workers to adhere to contact precaution.
- It can facilitate greater frequency of cleaning a decontamination as there is limited impact on neighboring patients
- The greater prominence of clinical hand wash facilities or hand hygiene dispensers is likely to improve hand hygiene compliance.
· Limiting movement of the person on contact precautions reduces the risk of environmental contamination.
· If movement is required between care areas within or between facilities it is important to ensure that infected or colonized areas of the person’s body are contained and covered
· The practice of wearing personal protective equipment is suggested for transmission-based precautions, including contact precautions.
· Personal protective equipment can protect healthcare workers against contaminated environmental surfaces and medical equipment, so gloves and gowns should be put on before entry into a patient's room and removed after leaving the patient-care area.
· Effective hand hygiene is particularly important in preventing contact transmission
· Evidence shows that using patient-dedicated equipment has been beneficial for preventing transmission of infectious agents.
· Precautions with respect to patient care equipment are very important in the care of patients on contact precautions. If patient care devices (for example blood pressure cuffs, mobility aids) are shared between people without appropriate cleaning, disinfection or reprocessing between uses, they may transmit infectious. Microorganisms
Droplet precautions
· Droplets precautions are intended to prevent the transmission of pathogens that are spread through respiratory or mucous membrane contact with respiratory secretions.
· Respiratory particles (droplets and aerosols) can be generated by various expiratory activities. Certain conditions, environments and procedures may increase risk to the nature and volume of transmission under certain environmental conditions, particularly indoor environments that are poorly ventilated.
· Placing patients on droplet precautions in single-patient rooms is justified to reduce healthcare associated infection.
· Surgical masks worn by patients with suspected/confirmed infectious agents spread by the droplet or airborne routes, as a form of source control.
Airborne Precaution
· The implementation of airborne precautions in the presence of known or suspected infectious agents that are transmitted by the airborne route is an effective measure to reduce the spread of infection.
· Wearing a correctly fitted P2 respirator when entering the patient-care area of a patient under airborne precautions is justified to reduce healthcare associated infection.
· Placing patients on airborne precautions in a negative pressure room is justified to reduce healthcare associated infection.
- Acknowledgements
We would like to acknowledge the Infection Control Guidelines Committee for developing these guidelines.
Head of IPC Guidelines Committee
Professor Ghada Ismail (Professor of Clinical Pathology (Clinical Microbiology), Faculty of Medicine, Ain Shams University, Secretary of Supreme IPC Committee, SCUH, Member of WHO Global Guidelines Groups (GDG) for Infection Prevention)
Secretary of IPC Guidelines Committee
Professor Walaa Abd El-Latif (Professor of Medical Microbiology and Immunology, Faculty of Medicine Ain Shams University, IPC Consultant)
Members of the Committee
▪ Professor Amal Sayed (Deputy Manager of Environmental Affair, Infection Control Director, Cairo University Hospitals)
▪ Professor Amani El-Kholy (Clinical Pathology Department (Microbiology), Faculty of Medicine, Cairo University, Infection Control Consultant)
▪ Dr Asmaa Mohamed Abdelfatah Mohamed (Lecturer, Faculty of Nursing MTI University)
▪ Dr Gehan Mohamed Fahmy (Professor clinical microbiology ASUSH consultant infection control, Board member of IFIC EMERO region)
▪ Professor Hebatallah Gamal Rashed (Clinical Pathology Department (Microbiology), Faculty of Medicine, Assuit University, Infection Control Consultant)
▪ Dr Iman Afifi (Consultant Clinical Pathology (Microbiology) and IPC, Ain Shams University, Director IPC units of Ain Shams internal medicine and Geriatric hospitals
▪ Professor Maha El Touny (Department of internal medicine. Faculty of Medicine, Ain Shams University. Infection Control Consultant)
▪ Brigadier Dr. Mohamed Bakr Al-Attar (Assistant Commander of Military Fever Hospital for Therapeutic Affairs, Tropical Medicine Consultant)
▪ Professor Nagwa Khamis (Emeritus Consultant Clinical Pathology (Microbiology) and IPC, ASU Director IPC Department and CEO Consultant IPC, CCHE-57357)
▪ Professor Nesrine Fathi Hanafi (Professor in Medical Microbiology and Immunology Faculty of Medicine Alexandria University, Head of Infection Prevention and Control, Alexandria University Hospitals)
▪ Dr. Reham Lotfy Abdel Aziz (Environmental Health Director, EEAA, Hazardous Waste Consultant, WMRA, Ministry of Environment)
▪ Professor Sherin ElMasry (Professor of Clinical Pathology, Ain Shams University, Chief Director of IPC ASU, Health Care Quality & Patient Safety Consultant)
▪ Dr Shimaa El-Garf (Coordinator): Clinical Pathology Specialist, Coordinator of HAI Surveillance and Audit Electronic System for University Hospitals, RLEUH- SCUH
- List of Abbreviations
AIIR: Airborne infection isolation room
C. difficile: Clostridioides difficile
CDC: Centers for Disease Control and Prevention
FFP: Filtering Facepiece
HEPA: High Efficiency Particulate Arresting
IPC: Infection prevention and control
KPIs: Key Performance Indicators.
M. Tuberculosis: Mycobacterium tuberculosis
MRSA: Methicillin-resistant Staphylococcus aureus
NIOSH: National Institute for Occupational Safety and Health
PPE: Personal Protective Equipment
SIPC: Standard infection control precautions
TBPs: Transmission-based precautions
VRE: Vancomycin Resistant Enterococci.
WHO: World Health Organization
- Glossary
1.1.1 Airborne precautions: A group of transmission-based precautions to prevent
the spread of airborne pathogens. Airborne precautions are measures used to
prevent, and control infection spread without necessarily having close patient
contact via aerosols from the respiratory tract of one individual directly onto
a mucosal surface or conjunctivae of another individual.
1.1.2 Airborne transmission: The spread of infection from one individual to
another by airborne particles (aerosols) less than 5
μm in diameter containing infectious
agents. Airborne particles are very small particles that may contain infectious
agents. They can remain in the air for long periods of time and can be carried
over long distances by air currents. Airborne particles can be released when an
individual coughs or sneezes, and during AGPs. ‘Droplet nuclei’ are aerosols
formed from the evaporation of larger droplet particles (see droplet
transmission). Aerosols formed from droplet particles in this way behave as
other aerosols. Aerosols can penetrate the respiratory system to the
alveolar level.
1.1.3 Cohort: Place two or
more patients (a cohort) with the same confirmed infection by pathogen in
the same room/ward. A cohort area should be physically separate from other
patients.
1.1.4 Colonization: The presence of microorganisms on a body surface
(such as the skin, and mucus membrane)
that does not cause disease in the person or signs of infection.
1.1.5 Contact transmission: The spread of infectious agents from one person to
another by contact. When spread occurs through skin-to-skin contact, this is
called direct contact transmission. When spread occurs via a contaminated
object, this is called indirect contact transmission.
1.1.6 Contaminated: The presence of an infectious agent on a body
surface; also, on or in clothes, bedding, surgical instruments or dressings, or
other inanimate articles or substances including water and food.
1.1.7 Cough etiquette/respiratory
hygiene: Measures that are taken to
minimize the spread of respiratory infections to others.
1.1.8 Droplet precautions: Measures used to prevent, and control infections
spread over short distances (at least 1 meter) via droplets larger than 5 or 10 µmfrom
the respiratory tract of one individual directly onto a mucosal surface or
conjunctivae of another individual. Droplets penetrate the respiratory system
to above the alveolar level.
1.1.9 Droplet transmission: The spread of infection from one individual to another
by droplets containing infectious agents.
1.1.10 High-touch
surfaces: Surfaces, often in patient care areas, that are frequently
touched by healthcare workers and patients (e.g. overbed table, IV pole,
doorknobs, medication carts).
1.1.11 Immunocompromised patient/individual: Any individual whose immune response is reduced or
deficient, usually because they have a disease or are undergoing treatment.
Individuals who are immunocompromised are more vulnerable to infection.
1.1.12 Infection: Invasion of the body by a harmful organism or
infectious agent such as a virus, parasite, bacterium or fungus.
1.1.13 Standard infection control
precautions (SICPs): SICPs are the basic
IPC measures necessary to reduce the risk of transmitting infectious agents
from both recognized and unrecognized sources of infection. Sources of
(potential) infection include blood and other body fluids secretions or
excretions (excluding sweat), non-intact skin or mucous membranes and any
equipment or items in the care environment that could have become contaminated.
1.1.14 Transmission-based precautions
(TBPs): Additional precautions to be used
in addition to SICPs when caring for patients with suspected or confirmed
infection or colonization that could be transmitted by contact, droplet or
airborne routes.
1.1.15 Personal protective equipment (PPE): Equipment an individual wears to protect themselves
from risks to their health or safety, including exposure to infection agents.
The level of PPE required depends on the:
● suspected or confirmed infectious agent
● severity of the illness caused
● transmission route of the infectious agent
● procedure or task being undertaken
- Introduction
Transmission-based precautions are a set of infection control measures designed to prevent the spread of infectious diseases in healthcare settings. They are used in addition to standard precautions, which are the basic infection prevention practices applied to all patients, regardless of their diagnosis.
Standard precautions alone may not be sufficient to prevent the transmission of certain infectious agents. Transmission-based precautions are implemented when there is a known or suspected infection with a pathogen that requires additional measures to prevent its spread. These pathogens can be transmitted through various routes, including:
· Contact: Direct or indirect contact with the patient or their environment.
· Droplets: Large respiratory droplets generated when a person coughs, sneezes, or talks.
· Airborne: Small particles containing infectious agents that can remain suspended in the air for extended periods.
Types of Transmission-Based Precautions:
There are three main types of transmission-based precautions:
1. Contact Precautions: Used for infections that can be transmitted by direct or indirect contact with the patient or their environment. Examples include MRSA, VRE, and C. difficile.
2. Droplet Precautions: Used for infections that can be transmitted by large respiratory droplets. Examples include influenza, pertussis, and group A streptococcus.
3. Airborne Precautions: Used for infections that can be transmitted by small airborne particles. Examples include tuberculosis, measles, and varicella.
N.B: Some infections require more than one type of precautions e.g. contact and droplet.
Key Elements of Transmission-Based Precautions:
· Hand Hygiene: Frequent and thorough handwashing with soap and water or the use of alcohol-based hand rub.
· PPE: Wearing appropriate PPE, such as gloves, gowns, masks, eye protection, and face shields, to protect healthcare workers from exposure to infectious agents.
· Patient Placement: Isolating patients in single rooms or cohorting them with other patients infected with the same pathogen.
· Respiratory Hygiene and Cough Etiquette: Encouraging patients to cover their mouths and noses when coughing or sneezing and to dispose of tissues properly.
· Environmental Cleaning and Disinfection: Implementing thorough cleaning and disinfection procedures for patient rooms and equipment.
Transmission-based precautions are essential tools for preventing the spread of infectious diseases in healthcare settings. By understanding and implementing these precautions, healthcare workers can protect themselves and their patients from infection.
- Scope and Purpose
· Healthcare Settings: Transmission-based precautions are implemented in various healthcare settings, including hospitals, clinics, long-term care facilities, ambulatory care centers, and dental offices.
· Infectious Diseases: These precautions apply to patients with known or suspected infections that can be transmitted through contact, droplets, or airborne routes.
Purpose
· Prevent Disease Transmission: The primary purpose is to prevent the spread of infectious diseases within the healthcare setting. This protects:
o Patients: Minimizes the risk of patients acquiring infections from other patients or healthcare workers.
o Healthcare Workers: Protects healthcare professionals from exposure to infectious agents.
o Visitors: Reduces the risk of infection transmission to visitors of the healthcare facility.
· Maintain a Safe Environment: Contributes to a safer and healthier environment for all individuals within the healthcare setting.
- Target Audience
· Infection prevention and
control team
· All health care
workers including clinicians , nurses ,
Head nurses, environmental workers ,
technicians (lab – radiology department….)
· Department managers
· medical supply manager
· Isolated Patients
· Visitors
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual Recommendation and their supporting evidence)
· Selecting only national and/or international guidelines
· Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
· Selecting peer reviewed publications only
· Selecting guidelines written in English language
· Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input.
· Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the Recommendation.
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers.
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The committee decided to adapt from:
1. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and control of infection in healthcare. 2019:134.
2. Centers for Disease Control and Prevention (CDC). Guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. 2007 [updated Nov 27, 2023].
3. National Infection Prevention and Control (IPC) Clinical Guideline. Infection prevention and control (IPC) national clinical guideline No. 30, Volume 1. May 2023.
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendation, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report Recommendation. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent Recommendation. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org/
· GRADE online training modules: http://cebgrade.mcmaster.ca/
Table (1) Quality and Significance of the four levels of evidence in GRADE
|
Quality |
Definition |
Implications |
|
High |
The guideline development group is very confident that the true effect lies close to that of the estimate of the effect |
Further research is very unlikely to change confidence in the estimate effect |
|
Moderate |
The guideline development group is moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibly that it is substantially different |
Further research is likely to have an important impact on confidence in the estimate of the effect and may change the estimate |
|
Low |
Confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the true effect |
Further research is very likely to have an important on confidence in the estimate of effect and is unlikely to change the estimate |
|
Very low |
The group has very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of the effect |
Any estimate of the effect is very uncertain |
Table (2) Factors that determine How to upgrade or downgrade the quality of evidence.
|
Downgrade in presence of |
Upgrade in presence of |
|
Study limitations. 1- Serious limitations 2- Very serious limitations |
Dose- response gradient. +1 Evidence of a dose-response gradient |
|
Consistency 1- Important inconsistency |
Direction of plausible bias + All plausible confounders would have reduced the effect |
|
Directness 1- Some uncertainty 2- Major uncertainty |
Magnitude of the effect +1 Strong, no plausible Confounder, consistent and direct evidence |
|
Precision 1- Imprecise data |
+2 very strong, no major threats to validity and direct evidence |
|
Reporting bias 1- High probability of reporting bias |
|
The strength of the Recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
● Strong Recommendation
With strong Recommendation, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
● Conditional Recommendation
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make Recommendation?
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Indicators for Monitoring
To ensure the effectiveness of transmission based precautions practices in hospitals and reduce the risk of HAIs, specific indicators should be monitored regularly. These are some indicators which can provide measurable data to assess compliance, identify areas for improvement, and guide interventions. Here are some key indicators that can be included in hospital guidelines for monitoring transmission based precautions implementation:
· Adherence to Transmission-Based Precautions
- Definition: Percentage of patients requiring isolation who are placed in the appropriate isolation setting (e.g., airborne, droplet, or contact precautions) within 1 hour of identification.
- Formula: (Number of patients placed in correct isolation / Total number of patients requiring isolation) × 100
· Percentage of isolation compliance:
- Definition: Percentage of eligible healthcare workers complying with isolation precautions needed according to transmission type.
- Formula: (Number of workers complying with isolation precautions/ Total eligible workers) × 100
· Staff training completion rate:
- Definition: Percentage of healthcare workers trained in transmission-based precautions annually.
- Formula: (Number of healthcare workers trained in transmission-based precautions / Total number of healthcare requiring training) × 100
·Patient and Family Compliance rate
- Definition: Percentage of patients and visitors adhering to precaution protocols (e.g., wearing masks, avoiding restricted areas.
- Formula: (Number of patients and visitors adhering to precaution protocols / Total eligible persons) × 100
1.1 Plan to Update this National Clinical Guideline
This guideline will be reviewed and updated at least every three years, or when new evidence emerges that is likely to influence the Recommendation.
- Annex
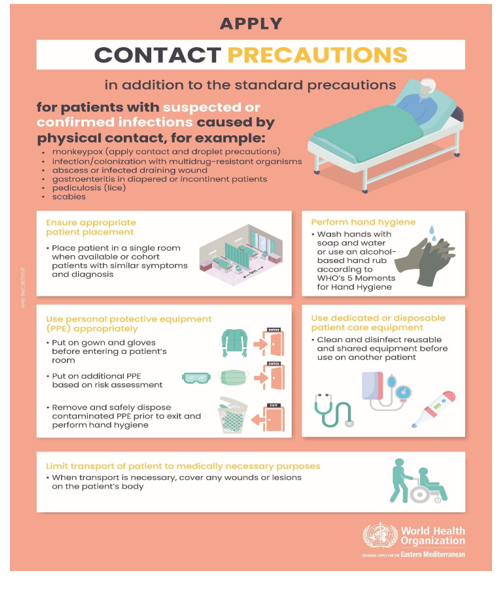
Annex1. Contact precautions poster, WHO Campaign
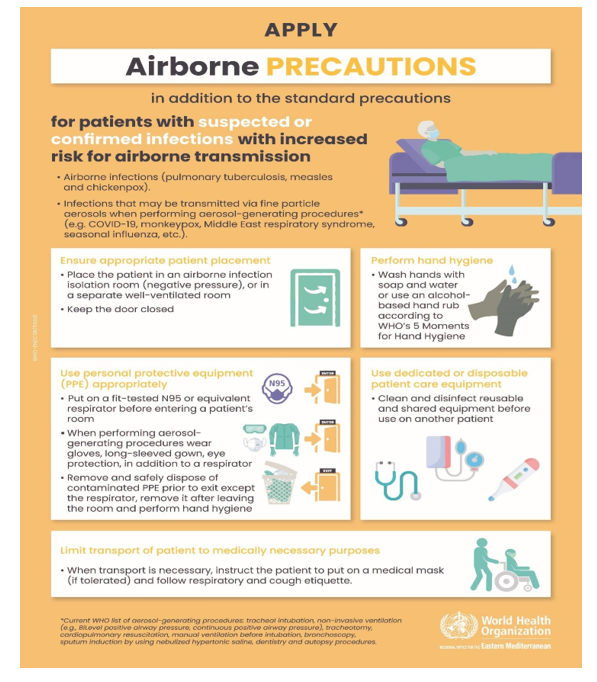
Annex 2. Airborne precautions poster, WHO Campaign
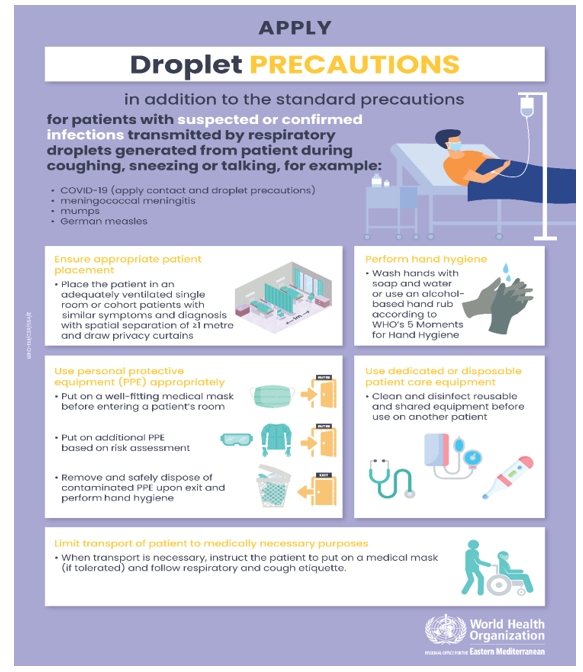
Annex 3. Droplet precautions poster, WHO Campaign
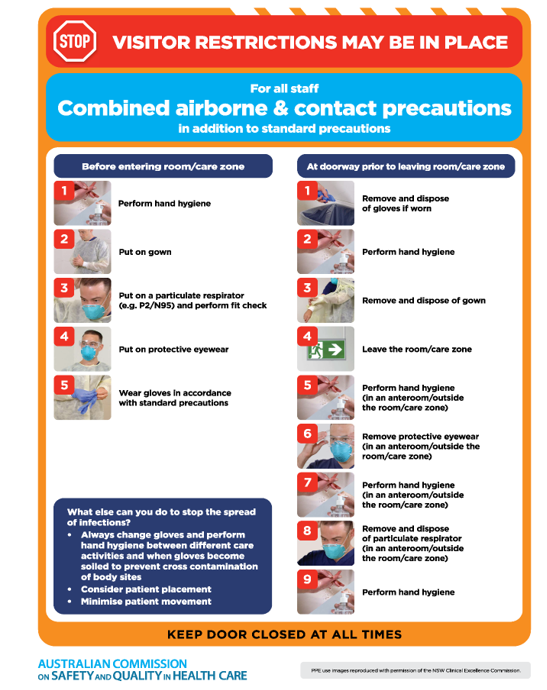
Annex 4. Combined airborne and contact precautions, Australian Commission on Safety and Quality in Health Care
- References
1. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and control of infection in healthcare. 2019:134.
2. Centers for Disease Control and Prevention (CDC). Guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. 2007 [updated Nov 27, 2023].
3. National Infection Prevention and Control (IPC) Clinical Guideline. Infection prevention and control (IPC) national clinical guideline No. 30, Volume 1. May 2023.
4. Mannion R, Freeman T, Millar R, Davies H. Effective board governance of safe care: a (theoretically underpinned) cross-sectioned examination of the breadth and depth of relationships through national quantitative surveys and in-depth qualitative case studies. Health Serv Deliv Res. 2016;4(4).
5. Bismark MM, Studdert DM. Governance of quality of care: a qualitative study of health service boards in Victoria, Australia. BMJ Qual Saf. 2014;23(6):474–82.
6. Pannick S, Davis R, Ashrafian H, Byrne BE, Beveridge I, Athanasiou T, et al. Effects of interdisciplinary team care interventions on general medical wards: a systematic review. JAMA Intern Med. 2015;175(8):1288–98.
7. Australian Commission on Safety and Quality in Health Care. National Model Clinical Governance Framework. Sydney: ACSQHC; 2017.
8. Australian Commission on Safety and Quality in Health Care. Australian Open Disclosure Framework. Sydney: ACSQHC; 2013 [accessed Oct 2017].
9. Roughead EE, Semple SJ, Rosenfeld E. Literature review: medication safety in Australia. Sydney: Australian Commission on Safety and Quality in Health Care; 2013 [accessed Sep 2017].
10. Australian Technical Advisory Group on Immunization. Australian immunization handbook. Canberra: Australian Government Department of Health; 2018 [cited 2021 Apr].
11. Mitchell BG, Shaban RZ, MacBeth D, Wood CJ, Russo PL. The burden of healthcare-associated infection in Australian hospitals: a systematic review of the literature. Infect Dis Health. 2017;22(3):117–28.
12. National Health and Medical Research Council Centre of Research Excellence in Suicide Prevention. Care after a suicide attempt. Sydney: National Mental Health Commission; 2015.
13. Posters for contact, airborne and droplet precautions available at https://www.emro.who.int/world-hand-hygiene-day/2023/index.html
14. Posters for Combined airborne and contact precautions, Australian Commission on Safety and Quality in Health Care available on “ https://www.safetyandquality.gov.au/sites/default/files/2023-04/Combined%20airborne%20and%20contact%20precautions.pdf”
15. Appendix A. : Further details on type and duration of precautions recommended for selected infections and conditions available on “ https://www.cdc.gov/infection-control/hcp/isolation-precautions/appendix-a-type-duration.html#print”