intensive care unit admission, discharge, and triage.
| Site: | EHC | Egyptian Health Council |
| Course: | Intensive Care Guidelines |
| Book: | intensive care unit admission, discharge, and triage. |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:58 AM |
Description
"last update:
4 August 2025" Download Guideline
- Executive Summary
|
Recommendations |
|
General considerations |
|
We recommend that critically ill patients be transferred from the emergency department ,ward bed or Intermediate Care Units (IMCUs) to an available Intensive Care Unit (ICU) bed as rapidly as possible, ideally in less than or equal to 1 hour from the time the ICU bed is confirmed available and the decision to transfer is finalized. This is to minimize delays in accessing specialized ICU monitoring and interventions and to reduce potential risks associated with prolonged holding in non-ICU environments (Strong recommendation). |
|
We recommend that in circumstances where a critically ill patient requires ICU services that are unavailable within the current hospital or cannot be provided in a timely manner, clinicians immediately utilize officially established national or regional referral pathways to facilitate rapid assessment and transfer to an appropriate ICU. In Egypt, this includes contacting the National Project of Critical Care, Neonatal, and Emergency Services "Rayat Misr" through its designated electronic platform or emergency hotline (137) as per national protocols (Strong recommendation). |
|
We recommend that individual hospitals and their Intensive Care Unit (ICU) leadership formulate and regularly review explicit ICU admission and triage policies follow this guidline. These policies should be tailored to their specific institutional context, including the scope of clinical services provided (e.g., trauma, burn, neurocritical care, hepatic care), the demographic characteristics of their patient population, current ICU capacity, and available therapeutic resources (Strong recommendation). |
|
We suggest that Triage decisions must be made transparently and without any prejudice. Factors like ethnicity, race, sex, social standing, or financial resources are wholly irrelevant. (Good practice statement). |
|
We recommend that hospitals and their ICU leadership develop, implement, and regularly review explicit, transparent, and fair policies for the triage and allocation of ICU beds. These policies should provide a clear framework for balancing scheduled postoperative admissions with emergency admissions. This includes defining a process for temporarily reserving beds for imminent high-risk surgical arrivals while also having a dynamic override mechanism, managed by a designated triage officer or clinical leader (e.g., ICU director), to ensure any patient with an immediate life-threatening condition can access a necessary bed with minimal delay. Unjustified or prolonged reservation of an empty ICU bed in the face of a critically ill patient needing admission is inconsistent with ethical principles of justice and beneficence (Strong recommendation). |
|
We recommend that hospitals, where feasible and appropriate based on patient population needs, establish Intermediate Care Units (IMCUs). These units should serve as a bridge between the general ward and the Intensive Care Unit to provide enhanced monitoring and a higher level of nursing care for two primary patient groups: those who no longer require intensive care but are too unstable for the general ward (step-down), and those who are deteriorating on the ward but may not require immediate ICU-level organ support (step-up). The implementation of IMCUs is intended to improve patient safety, reduce ICU readmissions, optimize the use of critical care beds, and potentially lower overall costs for specific high-risk patient populations. (Strong recommendation). |
|
We recommend that hospitals develop and implement a Rapid Response System to facilitate early identification, bedside assessment, and appropriate triage of clinically deteriorating patients on general wards. This system should include a clear set of vital sign-based trigger criteria (such as: Modified Early Warning Score ) fig. 1 and a designated team with critical care skills to respond promptly Rapid Response Team (RRT). A primary function of this team should be to stabilize the patient and facilitate timely and appropriate admission to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) when indicated (Strong recommendation). |
|
We recommend that RRSs be utilized for early review of acutely ill non-ICU patients to identify patients who need or would benefit from ICU admission and treatment and to prevent unnecessary ICU admissions (Strong recommendation). |
|
We recommend implementing ICU consult teams to support ward/IMCU staff with deteriorating patients, facilitate transfer to ICU, and reduce ICU readmission rates. (Good practice statement). |
|
Admission & Triage |
|
We suggest using the following tools for bed allocation during the admission and triage processes(Good practice statement). : Guide to resource allocation of intensive monitoring and care including levels of monitoring, care, and nursing ratios (table 2) ICU Admission Prioritization framework(table 3) |
|
We suggest using the following tools use as core of addmsion and discharge criteria checklist(Good practice statement): 1-addmsion checklist (table 4,5)
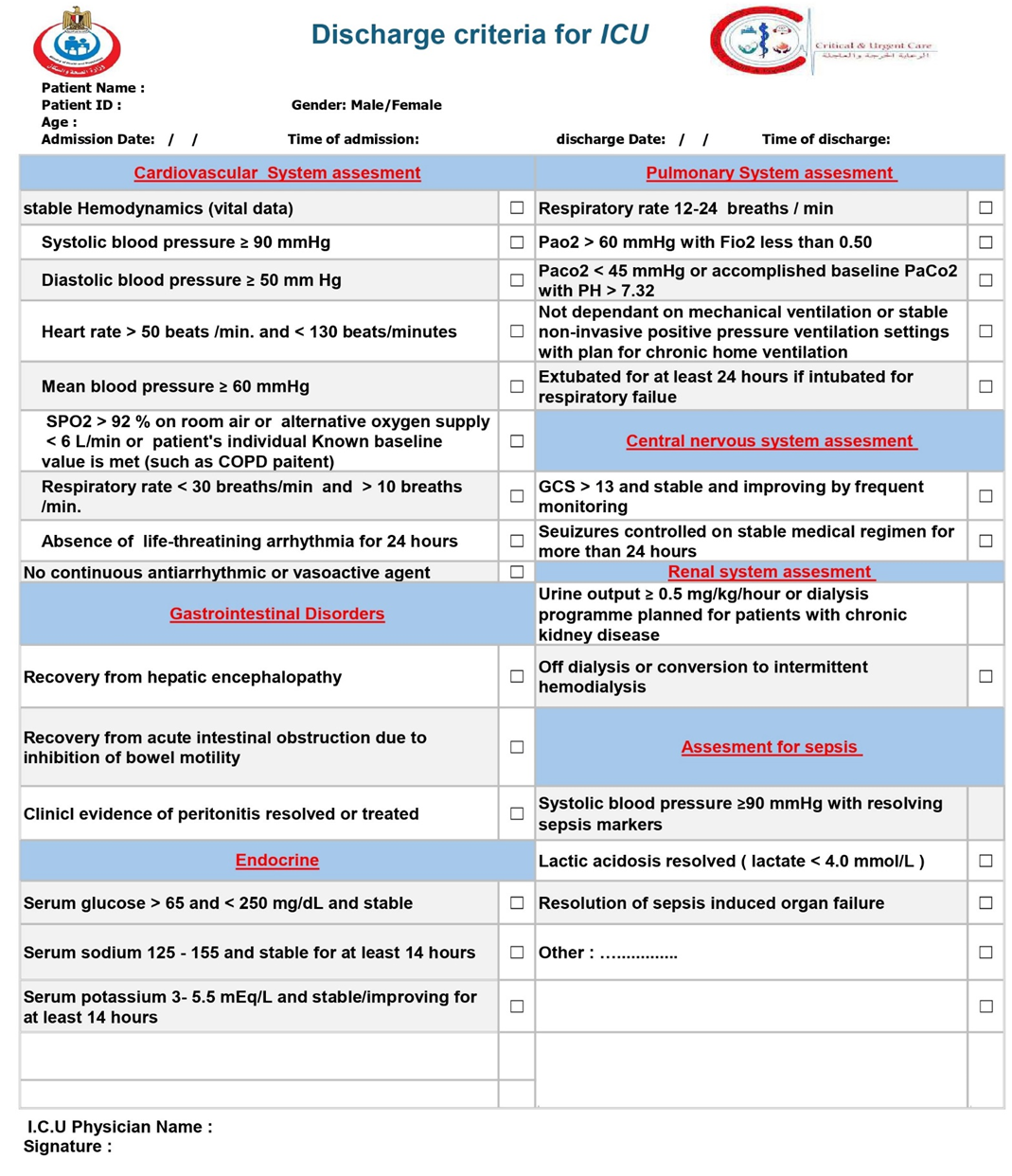
2- discharge criteria checklist (table 6):
|
|
We recommend that the Acute Physiology and Chronic Health Evaluation (APACHE II) score, or a similar validated illness severity scoring system, be used as an adjunct to clinical assessment for patients being considered for Intensive Care Unit (ICU) admission. The calculation of an APACHE score upon presentation to the emergency department or for deteriorating ED/ward patients can provide valuable, objective information regarding the severity of illness and risk of mortality. A high or significantly rising score should be considered a strong indicator for the need for ICU-level care, facilitating timely and appropriate triage, especially for patients with conditions known to have a high mortality risk such as sepsis, acute respiratory distress syndrome (ARDS), and major trauma. It is crucial to emphasize that the APACHE score should not be used in isolation to determine ICU admission or discharge. It is a decision-support tool that, when integrated with a comprehensive clinical evaluation, patient preferences, and the overall clinical context, can lead to more informed and effective patient care.(Good practice statement). |
|
We recommended that patients with invasive mechanical ventilation or complex life-threatening conditions, including sepsis, receive care in an ICU. Additionally, weaning from mechanical ventilation should be restricted to an ICU or In necessities step down to a intermediate care unit (IMCU) , and not take place on a general ward. (Strong recommendation). |
|
We suggest avoiding admitting to a specialized ICU patients with a primary diagnosis not associated with that specialty (i.e., boarding) (Strong recommendation). |
|
Triage |
|
We suggest that hospitals and ICU leaders develop and implement admission and triage policies that are designed to minimize under-triage and overtriage is more acceptable (Good practice statement). |
|
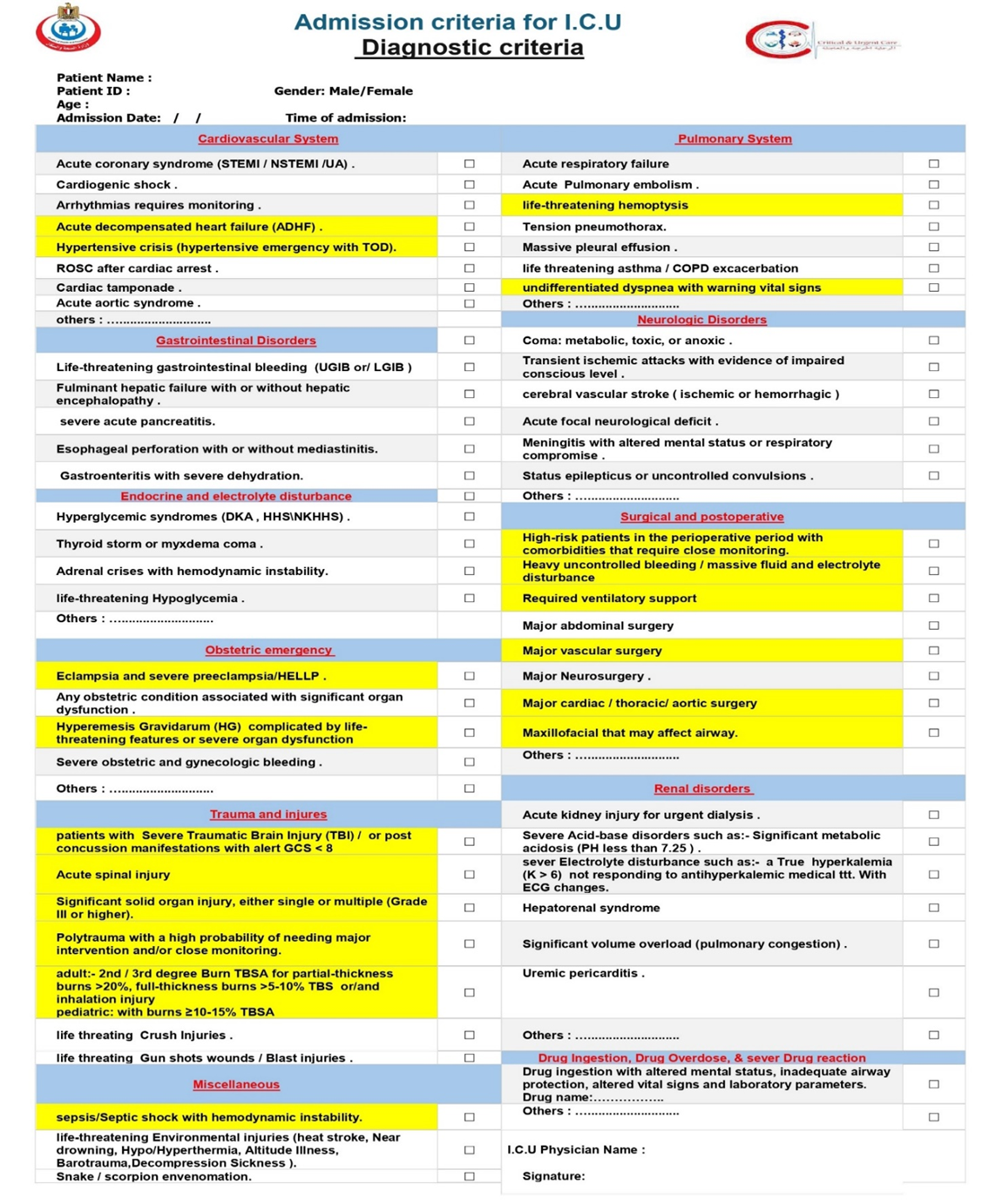
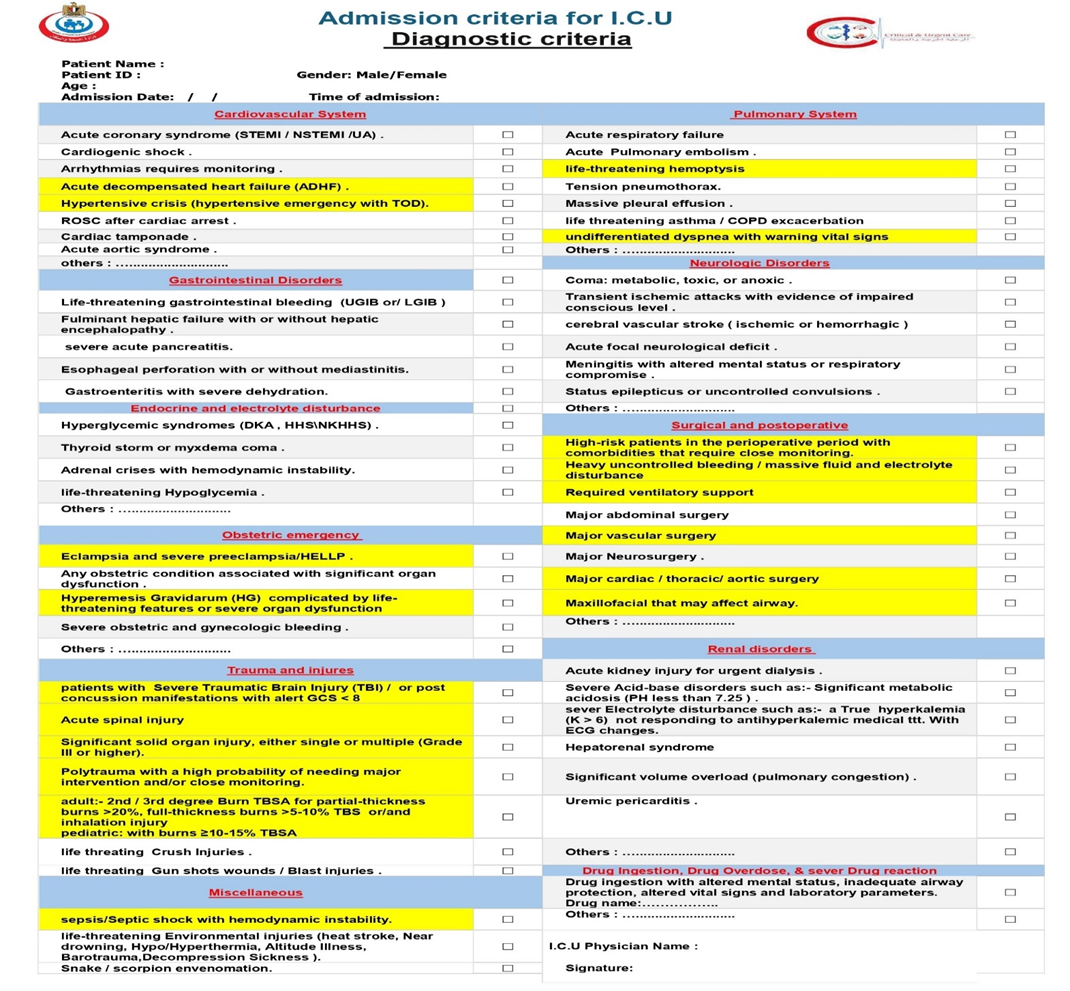
Diagnostic criteria |
|
We recommend that all patients presenting with ST-Elevation Myocardial Infarction (STEMI), ST-Elevation Myocardial Infarction (STEMI), Non-ST-Elevation Myocardial Infarction (NSTEMI) and other patients with Acute Coronary Syndromes (ACS) identified as high-risk (based on clinical features, ECG findings, cardiac biomarkers, hemodynamic instability, life-threatening arrhythmias, ongoing ischemia, acute heart failure and validated risk scores) be admitted to a Coronary Care Unit (CCU) an Intensive Care Unit (ICU), or an intermediate care unit (IMCU) with. This setting is necessary for continuous cardiac and hemodynamic monitoring, prompt management of life-threatening complications facilitation of timely reperfusion or invasive strategies, and optimization of medical therapy that require Intensive care, such as heart failure, cardiogenic shock, or serious arrhythmias, ventricular septal rupture, even if their initial condition appears stable, facilitation of timely reperfusion/revascularization strategies, and optimization of medical therapy (Strong recommendation). |
|
We recommend that all patients diagnosed with cardiogenic shock characterized by persistent hypotension despite adequate fluid status and signs of end-organ hypoperfusion. be immediately admitted to an to a Coronary Care Unit (CCU) or Intensive Care Unit (ICU) or a specialized cardiac/cardiovascular ICU with equivalent capabilities This is to facilitate immediate and continuous hemodynamic monitoring, aggressive management with intravenous vasoactive medications, advanced respiratory support, rapid investigation and treatment of the underlying cause, and consideration for mechanical circulatory support (Strong recommendation). |
|
We recommend that patients presenting with arrhythmias be admitted to an a specialized Coronary Care Unit (CCU) or Intensive Care Unit (ICU) if the arrhythmia is life-threatening (e.g., sustained ventricular tachycardia, ventricular fibrillation, symptomatic high-grade atrioventricular block), causes hemodynamic instability (e.g., hypotension, shock, acute heart failure), is associated with severe symptoms directly attributable to the arrhythmia (e.g., syncope with a high-risk rhythm), or requires urgent electrical interventions (cardioversion, defibrillation, pacing) or pharmacological interventions with intravenous agents that necessitate continuous cardiorespiratory monitoring not feasible or safe in a lower-acuity setting (Strong recommendation). |
|
We recommend that patients with acute decompensated heart failure (ADHF) who exhibit signs of hemodynamic instability (e.g., hypotension, cardiogenic shock), severe respiratory distress or failure (requiring non-invasive or invasive mechanical ventilation), life-threatening arrhythmias, or who require intravenous vasoactive medications or invasive hemodynamic monitoring, be admitted to an Intensive Care Unit (ICU) or a Intensive Coronary Care Unit (CCU) for intensive management and monitoring (Strong recommendation). |
|
We recommend that patients presenting with a hypertensive emergency (defined as severely elevated blood pressure accompanied by acute, ongoing target organ damage) be admitted to an Intensive Care Unit (ICU) or a Intensive Coronary Care Unit (CCU) or a comparable high-acuity monitored setting. This is to facilitate immediate and controlled parenteral antihypertensive therapy, continuous (often invasive) blood pressure monitoring, and close observation and management of specific target organ dysfunction (Strong recommendation). |
|
We recommend that adult patients who achieve Return of Spontaneous Circulation (ROSC) after cardiac arrest and remain comatose or hemodynamically unstable, or who require ongoing ventilatory support, be admitted to an Intensive Care Unit (ICU) or a Coronary Care Unit (CCU) with equivalent ICU capabilities for comprehensive post-resuscitation care (Strong recommendation). |
|
We recommend that patients diagnosed with cardiac tamponade, especially those exhibiting hemodynamic instability or requiring urgent pericardial drainage, be admitted to an Intensive Care Unit (ICU) or a Coronary Care Unit (CCU) with equivalent capabilities for continuous cardiorespiratory monitoring, management of potential complications, and further diagnostic evaluation and treatment of the underlying cause (Strong recommendation) |
|
We recommend that all patients diagnosed with or strongly suspected of having an Acute Aortic Syndrome (including aortic dissection, intramural hematoma, or penetrating atherosclerotic ulcer) be immediately admitted to an Intensive Care Unit (ICU) or a specialized cardiovascular ICU capable of providing comprehensive medical and peri-interventional management (Strong recommendation). |
|
We recommend that adult patients presenting with sever valvular heart disease such as severe acute mitral regurgitation, particularly when characterized by signs of respiratory failure (e.g., pulmonary edema requiring advanced respiratory support) or hemodynamic instability (e.g., hypotension, shock), be promptly admitted to an Intensive Care Unit (ICU) or a specialized Cardiovascular/Coronary Care Unit (CVICU/CCU). This is to facilitate immediate hemodynamic stabilization with intravenous vasoactive medications (vasodilators and/or inotropes), advanced respiratory support (non-invasive or invasive ventilation), intensive monitoring, and optimization as a bridge to urgent surgical intervention, which is the definitive therapy (Strong recommendation). |
|
Gastrointestinal Disorders |
|
We recommend that patients presenting with life-threatening gastrointestinal bleeding (UGIB or LGIB), characterized by hemodynamic instability (e.g., shock, persistent hypotension despite initial resuscitation), ongoing massive hemorrhage requiring significant transfusion, or validated high-risk scores indicating severe bleeding or high re-bleeding risk, be admitted to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive resuscitation, continuous hemodynamic monitoring, urgent diagnostic and therapeutic interventions (often endoscopic), specialized pharmacotherapy, and management of potential complications (Strong recommendation). |
|
We recommend that all patients diagnosed with Acute Liver Failure (ALF) / Fulminant Liver Failure (FLF) – characterized by severe acute liver injury with coagulopathy (INR ≥1.5) and any degree of hepatic encephalopathy (or those without initial encephalopathy but with rapid deterioration of liver function and coagulopathy indicating high risk of imminent ALF/FLF) – be promptly admitted to an Intensive Care Unit (ICU). Ideally, this should be a specialized liver unit or transplant center operating under a high-intensity ICU model, characterized by the intensivist being primarily responsible for or having mandatory daily co-management in the day-to-day care of the patient, ensuring expert critical care input alongside hepatology or/and transplant surgery expertise (Strong recommendation). |
|
We recommend that all patients diagnosed with severe acute pancreatitis, defined by the presence of persistent organ failure (>48 hours), be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This includes, but is not limited to, aggressive goal-directed fluid therapy, management of respiratory and cardiovascular failure, renal replacement therapy if indicated, specialized nutritional support, advanced pain control, and monitoring and management of local and systemic complications (Strong recommendation). |
|
We recommend that patients diagnosed with or strongly suspected of having esophageal perforation, with or without initially evident mediastinitis, be promptly admitted to an Intensive Care Unit (ICU). (Strong recommendation). |
|
We recommend that patients presenting with acute gastroenteritis complicated by severe dehydration leading to hemodynamic instability (e.g., shock, manifested by hypovolemic shock ,persistent hypotension despite initial fluid challenge, significant end-organ hypoperfusion (e.g., oliguria/anuria, altered mental status)), or critical electrolyte or acid-base or acute kidney injury requiring intensive management – be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive and goal-directed fluid resuscitation, continuous hemodynamic and laboratory monitoring, potential vasopressor support, correction of critical electrolyte and acid-base abnormalities, and management of organ dysfunction (Strong recommendation). |
|
Endocrine and electrolyte disturbance |
|
We recommend that adult patients presenting with severe Diabetic Ketoacidosis (DKA) – characterized by criteria such as arterial pH <7.1, serum bicarbonate <10 mEq/L, significant ketonemia/ketonuria with altered mental status (stupor/coma), or hemodynamic instability – and all patients with Hyperosmolar Hyperglycemic State (HHS) – characterized by marked hyperglycemia (often >600 mg/dL or >33.3 mmol/L), high effective serum osmolality (often >320 mOsm/kg), profound dehydration, and altered mental status – be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities. This admission is essential for aggressive intravenous fluid and electrolyte management, continuous intravenous insulin therapy with frequent and precise monitoring, close observation for neurological and cardiovascular complications, and identification and management of precipitating factors or concurrent organ dysfunction (Strong recommendation). |
|
We recommend that all patients diagnosed with or highly suspected of having thyroid storm be promptly admitted to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity and potential for rapid deterioration, we suggest their care be managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists (Strong recommendation). |
|
We recommend that all patients diagnosed with or highly suspected of having myxedema coma be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity and potential for rapid deterioration, we suggest their care be managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists(Strong recommendation). |
|
We recommend that all adult patients presenting with adrenal crisis complicated by hemodynamic instability (e.g., hypotension refractory to initial fluid challenges, signs of shock) be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity of managing shock, electrolyte disturbances, and potential multi-organ involvement, we suggest their care managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists(Strong recommendation) |
|
We recommend that adult patients presenting with life-threatening hypoglycemia – characterized by severe neuroglycopenia (e.g., coma, seizures, significantly altered mental status requiring external assistance for recovery) or those requiring continuous intravenous glucose infusions with very frequent monitoring to prevent relapse and maintain euglycemia – be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. (Strong recommendation). |
|
Obstetric emergency |
|
We recommend that all patients presenting with eclampsia, severe pre-eclampsia with severe features (including but not limited to severe hypertension, evidence of significant end-organ dysfunction), or HELLP syndrome be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the complexity and potential for rapid deterioration, we suggest their care be managed within a high-intensity ICU/ IMCU model, characterized by experienced multidisciplinary input including obstetricians, anesthesiologists, intensivists, and neonatologists, with clear protocols for escalation and management This includes continuous hemodynamic monitoring, seizure prophylaxis with magnesium sulfate, antihypertensive therapy, and preparation for potential delivery. (Strong recommendation). |
|
We recommend that all obstetric patients (pregnant or postpartum) who develop significant acute organ dysfunction (e.g., sever postpartum hemaorage, cardiovascular collapse/shock, severe respiratory failure requiring advanced support, acute kidney injury requiring renal replacement therapy, severe coagulopathy, or profound neurological impairment, sever trauma) be promptly admitted to an an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the unique physiological changes of pregnancy and the need for coordinated multidisciplinary care (obstetrics, critical care, anesthesia, neonatology), we suggest their care be managed within a high-intensity ICU/ IMCU model includes continuous hemodynamic monitoring, respiratory support, renal replacement therapy, and other advanced interventions as necessary. (Strong recommendation). |
|
We recommend that pregnant patients with Hyperemesis Gravidarum (HG) who develop severe, life-threatening complications. Such complications include, but are not limited to, profound dehydration leading to hypovolemic shock or severe acute kidney injury (AKI), severe refractory electrolyte imbalances (e.g., critically low potassium or sodium) causing cardiac or neurological symptoms, Wernicke's encephalopathy, or esophageal complications. be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the unique physiological changes of pregnancy and the need for coordinated multidisciplinary care (obstetrics, critical care, anesthesia, neonatology), we suggest their care be managed within a high-intensity ICU/ IMCU model includes continuous hemodynamic monitoring, respiratory support, renal replacement therapy, and other advanced interventions as necessary. (Strong recommendation). |
|
We recommend that adult patients presenting with severe obstetric or gynecologic bleeding, characterized by hemodynamic instability (e.g., shock, persistent hypotension despite initial fluid resuscitation), ongoing massive hemorrhage requiring significant transfusion (e.g., activation of massive transfusion protocol), or evidence of significant end-organ hypoperfusion or coagulopathy, be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive resuscitation including balanced blood product replacement, continuous hemodynamic monitoring, urgent interventions for source control (medical, radiological, or surgical), specialized pharmacotherapy (e.g., tranexamic acid, uterotonics), and management of potential complications such as coagulopathy, ARDS, or AKI (Strong recommendation). |
|
Trauma and injures |
|
We recommend that all adult patients presenting with severe traumatic brain injury or post concussion manifestations, defined by a Glasgow Coma Scale (GCS) score of ≤ 8 after initial resuscitation, be promptly admitted to an Intensive Care Unit (ICU) capable of providing comprehensive neurocritical care. This includes airway protection, mechanical ventilation, intracranial pressure monitoring, hemodynamic support, and multidisciplinary care. Given the complexity of managing severe TBI and the potential for rapid neurological deterioration, we suggest their care be managed within a high-intensity neuro-ICU model, characterized by the intensivist (often a neurointensivist or an intensivist with neurocritical care expertise) being primarily responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with neurosurgery and other relevant specialists (Strong recommendation for ICU admission Conditional recommendation for specific ICU model) |
|
We recommend that adult patients with an acute spinal cord injury resulting in significant neurological deficit (e.g., quadriplegia, paraplegia) that causes or poses an imminent risk of respiratory failure (typically injuries at or above the C5 level) or hemodynamic instability (neurogenic shock, typically from injuries at or above the T6 level) be promptly admitted to preferably a specialized Neuro-ICU or Intensive Care Unit (ICU), preferably one with expertise in neurocritical care and trauma. This is to facilitate advanced airway and respiratory support (including mechanical ventilation), intensive hemodynamic monitoring and management to maintain spinal cord perfusion, prevention and treatment of systemic complications, and expert multidisciplinary care in conjunction with neurosurgery and spine surgery teams (Strong recommendation). |
|
We recommend that adult patients presenting with significant solid organ injury, classified as American Association for the Surgery of Trauma (AAST) Grade III or higher (either single or multiple organs), be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for intensive monitoring and management. This is to facilitate continuous hemodynamic and hematological assessment, early detection of bleeding or failure of non-operative management, readiness for urgent angiographic or surgical intervention, aggressive pain control, and management of associated injuries or systemic complications. For patients who are hemodynamically unstable or have evidence of ongoing bleeding despite initial resuscitation, direct ICU admission is strongly recommended (Strong recommendation). |
|
We recommend that all adult patients presenting with polytrauma who have a high probability of needing major intervention (e.g., surgery, angiography) and/or require intensive physiological monitoring and support due to actual or impending organ dysfunction or hemodynamic instability be promptly admitted to an Intensive Care Unit (ICU), preferably one within a designated trauma center with readily available multidisciplinary trauma expertise. (Strong recommendation). |
|
We recommend that decisions regarding ICU admission for adult burn patients should carefully consider factors such as the type of burn, percentage of Total Body Surface Area (%TBSA) affected, presence of inhalation injury, location of burns, associated trauma, patient age, pre-existing comorbidities, and the number of victims in large-scale mass casualty incidents. Specifically, under normal circumstances, we advise that adult patients presenting with severe second- or third-degree burns—including partial-thickness burns exceeding 15–20% TBSA, full-thickness burns exceeding 5–10% TBSA, require mechanical ventilation (eg, significant inhalation injuries, massive fluid resuscitation), electrical or major chemical burns, burns involving critical areas (face, hands, feet, genitalia, perineum, or major joints), or burns in individuals with significant pre-existing medical conditions or accompanying traumatic injuries—be ideally admitted to a dedicated Burn Intensive Care Unit (ICU) within a specialized Burn Center. Given the complex and highly specialized nature of burn care, we strongly suggest that these patients be managed by an experienced multidisciplinary burn team, comprising intensivists, burn surgeons, specialized nurses, respiratory therapists, and nutritionists within an ICU setting. (Strong recommendation). |
|
We recommend that adult patients presenting with severe burns defined by criteria be admitted to an Intensive Care Unit (ICU). While admission to a specialized Burn ICU within a designated Burn Center is the optimal standard of care, a general ICU can and should provide the necessary life-saving critical care for these patients when a specialized Burn ICU is not immediately available or in/During mass casualty scenarios.( Good practice statement). |
|
We recommend that adult patients presenting with life-threatening crush injuries – characterized by extensive muscle damage, prolonged compression, evidence of or high risk for Crush Syndrome (e.g., significant rhabdomyolysis, hyperkalemia, early AKI), severe compartment syndrome, or associated hemodynamic instability – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate aggressive resuscitation including Correction of Metabolic Acidosis and Other Electrolyte Disturbances, balanced blood product replacement, continuous hemodynamic monitoring, urgent interventions for source control (medical, or surgical), Monitoring and Management of Compartment Syndrome , specialized pharmacotherapy (e.g., tranexamic acid, uterotonics), and management of potential complications such as coagulopathy, ARDS, or AKI (Strong recommendation). |
|
We recommend that all patients presenting with life-threatening gunshot wounds or blast injuries, characterized by hemodynamic instability, significant hemorrhage requiring or likely to require massive transfusion, compromised airway or breathing, severe traumatic brain injury (GCS ≤ 8), or evidence of significant penetrating or multi-system trauma, be promptly admitted to an Intensive Care Unit (ICU), ideally within a designated trauma center equipped for comprehensive trauma and critical care. Given the complexity and need for coordinated, multidisciplinary expert care (trauma surgery, critical care, neurosurgery, orthopedic surgery, anesthesia, interventional radiology), we suggest their care be managed within a ICU model, characterized by the intensivist and trauma surgeon having a primary or mandatory and active co-management role (Strong recommendation). |
|
Pulmonary System |
|
We recommend that adult patients presenting with acute respiratory failure, defined by severe hypoxemia (PaO2/FiO2 ratio < 100), hypercapnia (PaCO2 > 50 mmHg with pH < 7.35), or the need for non-invasive or invasive mechanical ventilation, be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate advanced respiratory support (including mechanical ventilation and lung-protective strategies when indicated), continuous respiratory and hemodynamic monitoring, management of the underlying cause of respiratory failure, and treatment of potential complications (Strong recommendation) |
|
We recommend that adult patients presenting with acute pulmonary embolism be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities if they are classified as high-risk (i.e., presenting with hemodynamic instability/shock) or intermediate-high risk (i.e., hemodynamically stable but with evidence of both right ventricular dysfunction and myocardial injury). This is to facilitate immediate hemodynamic and respiratory support, administration and monitoring of reperfusion therapies (e.g., thrombolysis), close observation for clinical deterioration allowing for timely rescue interventions, and management of potential complications (Strong recommendation). |
|
We recommend that patients presenting with life-threatening hemoptysis – characterized by airway compromise, hemodynamic instability, significant respiratory failure, or bleeding volume/rate considered to be high risk – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate immediate airway management, resuscitation, continuous cardiorespiratory monitoring, and urgent diagnostic and therapeutic interventions, most notably bronchoscopy and bronchial artery embolization (BAE), in a coordinated, multidisciplinary fashion involving intensivists, pulmonologists, interventional radiologists, and thoracic surgeons (Strong recommendation). |
|
We recommend that all patients who have been treated for a tension pneumothorax be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This admission is essential for ongoing hemodynamic resuscitation and support, management of respiratory failure (often with mechanical ventilation), monitoring and management of the chest drain and any persistent air leak, observation for complications such as re-expansion pulmonary edema, and diagnosis and treatment of the underlying precipitating cause (Strong recommendation). |
|
We recommend that adult patients presenting with a massive pleural effusion that causes acute respiratory failure (characterized by severe dyspnea, increased work of breathing, or hypoxemia) or hemodynamic compromise be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to treating underlying cause pleural effusion also facilitate treating urgent, controlled therapeutic drainage, provide advanced respiratory and hemodynamic support as needed, allow for intensive monitoring for and management of potential complications (especially re-expansion pulmonary edema), and to diagnose and manage the severe underlying cause of the effusion (Strong recommendation). |
|
We recommend that adult patients presenting with a severe or life-threatening exacerbation of asthma or COPD be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Indications for this level of care include acute respiratory failure requiring non-invasive or invasive mechanical ventilation, severe dyspnea with signs of respiratory muscle fatigue, altered mental status, persistent or worsening hypoxemia, or severe/worsening respiratory acidosis despite initial therapy. This is to facilitate advanced respiratory support, continuous cardiorespiratory monitoring, intensive pharmacotherapy, and management of potential complications (Strong recommendation). |
|
We recommend that adult patients presenting with undifferentiated dyspnea accompanied by warning signs of physiological instability – characterized by severe respiratory distress (e.g., high respiratory rate, accessory muscle use, inability to speak), hypoxemia (e.g., SpO2 <90% on significant oxygen support), hemodynamic compromise (e.g., shock, hypotension), or altered mental status – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate cardiorespiratory stabilization and life support (including non-invasive or invasive mechanical ventilation), continuous intensive monitoring, and a rapid, concurrent diagnostic evaluation to identify and treat the underlying cause (Strong recommendation). |
|
Neurologic Disorders |
|
We recommend that all patients presenting in a coma (defined as a Glasgow Coma Scale [GCS] score of ≤ 8) of a known or suspected metabolic, toxic, or anoxic etiology be promptly admitted to an Intensive Care Unit (ICU). This is to facilitate immediate airway management (endotracheal intubation and mechanical ventilation), continuous cardiorespiratory and neurological monitoring, rapid diagnostic evaluation to determine the specific cause, and administration of specific treatments (e.g., targeted temperature management, metabolic correction, antidotes, enhanced elimination techniques) and comprehensive organ support. Given the complexity and need for multidisciplinary expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with relevant specialists (e.g., neurology, toxicology, endocrinology) (Strong recommendation). |
|
We recommend that adult patients presenting with acute neurological deficits accompanied by an impaired level of consciousness (Glasgow Coma Scale score <15, and especially ≤ 8) be promptly admitted to an Intensive Care Unit (ICU) or a Comprehensive Stroke/neuro Unit with equivalent ICU capabilities. This is to facilitate immediate airway management if necessary, intensive neurological and hemodynamic monitoring, management of intracranial pressure and cerebral edema, and post-procedure care, and management of systemic complications (Strong recommendation). |
|
We recommend that adult patients presenting with a severe acute cerebral vascular stroke (ischemic or hemorrhagic:- ( intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH))be promptly admitted to an Intensive Care Unit (ICU), preferably a specialized Neuro-ICU, or a Comprehensive Stroke Unit with equivalent ICU capabilities. Indications for this level of care include, but are not limited to, an impaired level of consciousness (Glasgow Coma Scale [GCS] score ≤ 8), signs of intracranial hypertension or impending herniation, the need for mechanical ventilation, hemodynamic instability, ongoing management of therapies such as intravenous thrombolysis or post-mechanical thrombectomy care, or management of severe complications such as large or expanding hematomas, intraventricular hemorrhage, or aneurysmal subarachnoid hemorrhage (Strong recommendation). |
|
We recommend that adult patients presenting with an acute focal neurological deficit who also exhibit signs of critical illness – characterized by an impaired level of consciousness (Glasgow Coma Scale score ≤ 13), acute respiratory failure requiring advanced support, hemodynamic instability, signs of increased intracranial pressure or impending herniation, or status epilepticus – be promptly admitted to an Intensive Care Unit (ICU), preferably a specialized Neuro-ICU or a Comprehensive Stroke Unit with equivalent ICU capabilities. This is to facilitate immediate airway management, continuous neurological and hemodynamic monitoring, aggressive management of intracranial pressure and other neurological complications, and rapid investigation and treatment of the underlying life-threatening cause (Strong recommendation). |
|
We recommend that adult patients with Myasthenic Crisis (defined by respiratory failure secondary to myasthenia gravis) and those with severe Guillain-Barré Syndrome (GBS) – characterized by rapid progression of weakness, evidence of respiratory muscle compromise (e.g., vital capacity <20 mL/kg), significant bulbar dysfunction, or severe autonomic instability – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate intensive cardiorespiratory monitoring, timely non-invasive or invasive mechanical ventilation, management of autonomic dysfunction, administration of specific immunotherapies, and comprehensive supportive care. Given the need for specialized neurological and critical care expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with neurology specialists(Strong recommendation). |
|
We recommend that adult patients presenting with neurological infections such as:- meningitis, who also exhibit signs of severe neurological compromise (e.g., altered mental status with a Glasgow Coma Scale [GCS] score ≤ 11, and particularly ≤ 8) or significant systemic organ dysfunction (e.g., respiratory compromise requiring advanced airway or ventilatory support, or hemodynamic instability/septic shock) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This is to facilitate immediate airway management, intensive neurological and hemodynamic monitoring (including management of intracranial pressure), rapid administration of appropriate antimicrobial and adjunctive therapies, and comprehensive management of seizures, shock, and multi-organ failure (Strong recommendation). |
|
We recommend that all adult patients with established convulsive status epilepticus (defined as continuous seizure activity >5 minutes or ≥2 discrete seizures without recovery of consciousness between them) or uncontrolled convulsions be promptly admitted to an Intensive Care Unit (ICU) or specialized Neuro-ICU or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management . This admission is essential to facilitate aggressive, stepwise anticonvulsant therapy (including potential administration of continuous anesthetic infusions for refractory cases), secure and manage the airway (often with mechanical ventilation), provide continuous electroencephalography (cEEG) and hemodynamic monitoring, and manage life-threatening systemic complications. Given the need for specialized neurological and critical care expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with neurology/epileptology specialists (Strong recommendation). |
|
Surgical and postoperative |
|
We recommend that adult surgical patients be admitted to an Intensive Care Unit (ICU) or any specialized ICU or with equivalent capabilities for comprehensive critical care management if they meet one or more of the following criteria: (1) they have undergone a high-risk surgical procedure known to require intensive monitoring and support post-operatively (e.g., major cardiac, thoracic, aortic, neurological, vascular, abdominal, or transplant surgery); (2) they have severe pre-existing comorbidities that significantly impair their physiological reserve to withstand major surgery; or (3) they exhibit evidence of acute organ dysfunction or hemodynamic instability in the immediate postoperative period (e.g., need for mechanical ventilation, vasopressor support, or ongoing massive transfusion). This is to facilitate advanced organ support, continuous cardiorespiratory and neurological monitoring, management of major fluid shifts and bleeding, advanced pain control, and early detection and management of life-threatening postoperative complications (Strong recommendation). |
|
We suggest that surgical patients who are hemodynamically stable at the conclusion of surgery, successfully extubated, and require only enhanced monitoring (e.g., continuous electrocardiography, invasive arterial pressure monitoring) or low-level therapeutic support (e.g., non-invasive ventilation, single low-dose vasopressor) may be admitted to a designated Intermediate Care Unit (IMCU) with appropriate nurse-to-patient ratios and protocols for rapid escalation of care if needed. This strategy can optimize critical care resource allocation without compromising patient safety. (Good practice statement). |
|
Renal disorders |
|
We recommend that adult patients with acute kidney injury (AKI) who require urgent renal replacement therapy be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate the safe initiation and management of renal replacement therapy (including continuous modalities like Continuous Renal Replacement Therapy for hemodynamically unstable patients), provide continuous monitoring for and treatment of life-threatening electrolyte and acid-base disturbances, and deliver comprehensive organ support for the underlying critical illness that precipitated the AKI such as:(CKD, sepsis, shock, tumor lysis syndrome or rhabdomyolysis etc.) (Strong recommendation). |
|
We recommend that adult patients presenting with a severe acid-base disorder – characterized by extreme derangement in arterial pH (e.g., acidemia with pH < 7.20 or alkalemia with pH > 7.55) or a less extreme derangement accompanied by evidence of significant organ dysfunction (e.g., shock, altered mental status, respiratory failure) – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate continuous cardiorespiratory and neurological monitoring, aggressive management of the underlying cause, advanced respiratory and hemodynamic support as needed, and frequent biochemical monitoring to guide therapy (Strong recommendation). |
|
We recommend that adult patients presenting with severe hyperkalemia (e.g., serum K+ > 6.0-6.5 mmol/L) that is accompanied by any new ECG changes attributable to hyperkalemia, or that is refractory to initial medical therapies, be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU)/High-Dependency Unit (HDU) with continuous cardiac monitoring capabilities. This is to facilitate immediate and ongoing cardiac monitoring, administration of emergency medical therapies, urgent initiation of renal replacement therapy (dialysis) for definitive potassium removal, frequent laboratory monitoring, and management of the underlying cause (Strong recommendation). |
|
We recommend that adult patients presenting with significant volume overload causing acute pulmonary edema and respiratory distress (characterized by severe dyspnea, increased work of breathing, and/or hypoxemia) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate advanced respiratory support (most notably non-invasive ventilation), aggressive and monitored fluid removal with intravenous diuretics or renal replacement therapy, administration of vasoactive medications as needed, and continuous cardiorespiratory monitoring (Strong recommendation). |
|
We recommend that adult patients with uremic pericarditis who present with cardiac tamponade or evidence of significant hemodynamic compromise (e.g., hypotension, shock) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate urgent pericardiocentesis or surgical drainage, safe initiation and management of intensive renal replacement therapy (dialysis) in an unstable patient, continuous cardiorespiratory and hemodynamic monitoring, and comprehensive management of the underlying severe renal failure (Strong recommendation). |
|
We recommend that adult patients diagnosed with Hepatorenal Syndrome-Acute Kidney Injury (HRS-AKI) be promptly admitted to an Intensive Care Unit (ICU), preferably one with expertise in hepatology and liver transplantation. This is to facilitate the administration and intensive monitoring of vasoconstrictor and albumin therapy, aggressive management of hemodynamic instability and other complications of decompensated cirrhosis (e.g., hepatic encephalopathy, bleeding), delivery of renal replacement therapy if indicated, and comprehensive multi-organ support as a bridge to potential liver transplantation (Strong recommendation). |
|
Drug Ingestion, Drug Overdose, & sever Drug reaction |
|
We recommend that patients presenting with a known or suspected drug ingestion who exhibit signs of life-threatening toxicity – characterized by altered mental status with inadequate airway protection (e.g., Glasgow Coma Scale score ≤ 8), hemodynamic instability (e.g., shock, life-threatening arrhythmias, severe hypertension), respiratory failure requiring advanced support, ongoing seizures, or severe metabolic/laboratory abnormalities – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate life support (airway, breathing, circulation), continuous cardiorespiratory and neurological monitoring, administration of antidotes, consideration of enhanced elimination techniques (e.g., hemodialysis), and management of multi-organ complications (Strong recommendation). |
|
Miscellaneous |
|
We recommend that all adult patients presenting with septic shock (defined by persisting hypotension requiring vasopressors to maintain MAP ≥65 mmHg and serum lactate >2 mmol/L despite adequate volume resuscitation) and patients with sepsis accompanied by significant hemodynamic instability (e.g., hypotension responsive only to ongoing aggressive fluid resuscitation, or other signs of organ hypoperfusion such as persistently elevated lactate despite initial fluids) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This admission is essential to facilitate timely implementation of sepsis management bundles, including rapid administration of appropriate antimicrobials, aggressive hemodynamic resuscitation with fluids and vasoactive agents, source control measures, potential advanced respiratory support, and continuous monitoring and management of organ dysfunction (Strong recommendation). |
|
We recommend that adult patients presenting with life-threatening environmental injuries – specifically heat stroke (core temperature >40°C with CNS dysfunction), severe complications of drowning (e.g., significant hypoxemia, ARDS, altered mental status), severe hypothermia (core temperature <32°C with cardiovascular instability or coma), severe environmentally-induced hyperthermia with organ dysfunction, severe altitude illness (High Altitude Cerebral Edema [HACE] or High Altitude Pulmonary Edema [HAPE] with respiratory failure or coma), severe barotrauma (especially pulmonary barotrauma with Arterial Gas Embolism [AGE]), or severe Decompression Sickness (Type II DCS with neurological or cardiorespiratory compromise) – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This is to facilitate aggressive specific therapies (e.g., rapid cooling/rewarming, hyperbaric oxygen coordination, specific pharmacotherapies), advanced respiratory and hemodynamic support, continuous multi-organ monitoring, and management of potential complications we suggest their care be managed within ICU model, characterized by the intensivist having a primary or mandatory and active co-management role in conjunction with relevant specialists (Strong recommendation) |
|
We recommend that adult patients presenting with signs of severe systemic envenomation from a snakebite or scorpion sting be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. Signs of severe envenomation requiring such admission include, but are not limited to: respiratory failure or compromise (e.g., neurotoxic paralysis, pulmonary edema), hemodynamic instability (e.g., shock, severe hypertension), venom-induced consumptive coagulopathy with active bleeding, significant neurological impairment (e.g., altered mental status, seizures), or evidence of severe end-organ damage such as acute kidney injury or severe rhabdomyolysis. This is to facilitate timely administration and monitoring of antivenom (including management of adverse reactions), advanced respiratory and hemodynamic support, management of coagulopathy, and comprehensive multi-organ supportive care (Strong recommendation). |
|
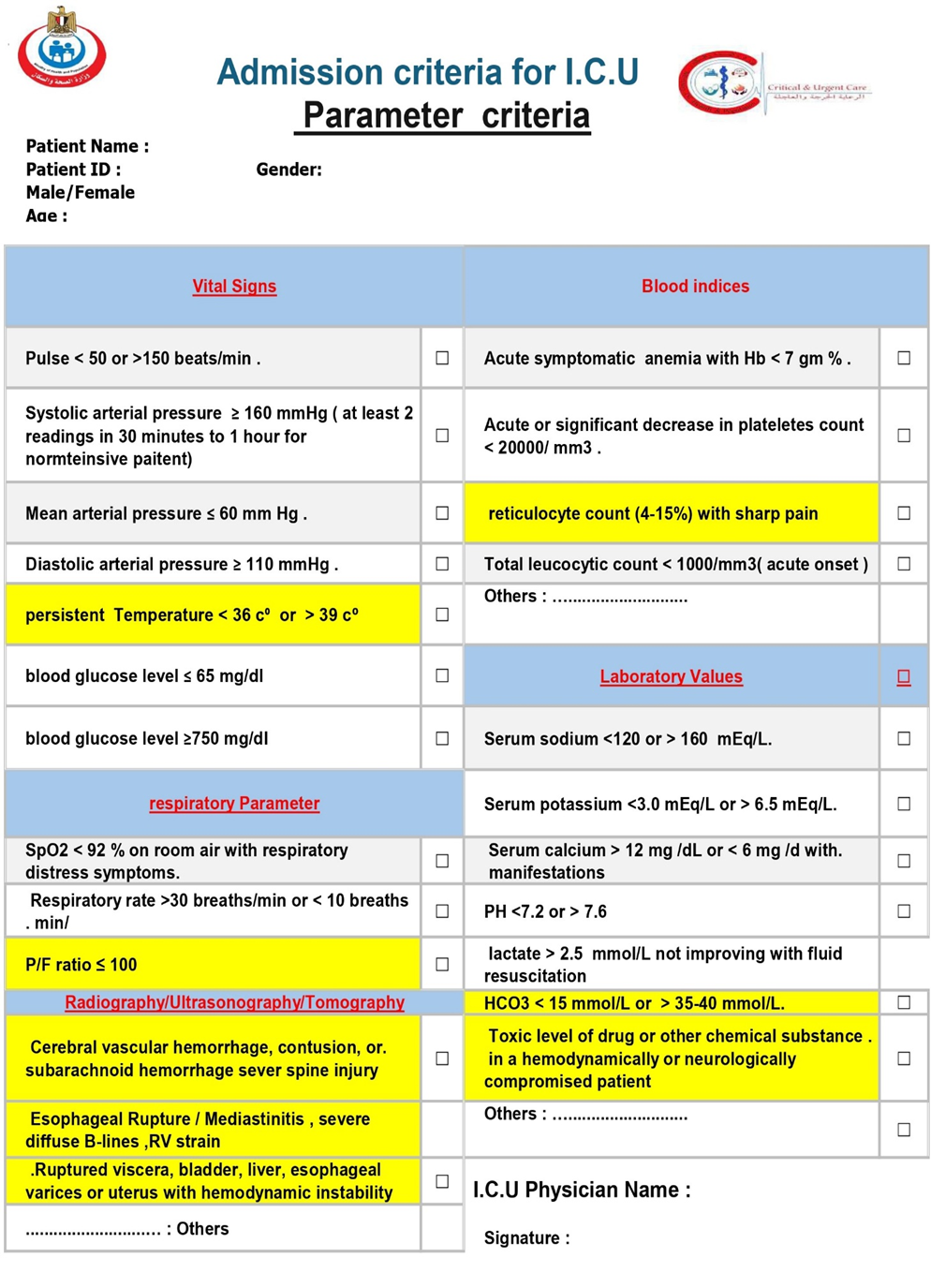
Parameter criteria |
|
Vital Signs |
|
We recommend that adult patients presenting with warning vital signs indicating acute or impending critical illness be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such warning signs include, but are not limited to, evidence of a compromised airway; severe respiratory distress (e.g., respiratory rate >30 or <10 breaths/min, SpO2 <90% on significant oxygen support); hemodynamic instability (e.g., HR <40 or >130, shock with Systolic arterial pressure ≤ 90 mm Hg or ≥ 160 mmHg or requiring vasopressors) (Mean arterial pressure ≤ 60 mm Hg or Diastolic arterial pressure > 110 mmHg ). ; life-threatening arrhythmias; or a new, significant alteration in level of consciousness (e.g., GCS drop, new-onset coma). This is to facilitate continuous cardiorespiratory and neurological monitoring, immediate life support, and a rapid, concurrent diagnostic evaluation to identify and treat the underlying cause (Strong recommendation). |
|
We recommend that adult patients with a persistent core body temperature of < 36°C (hypothermia) or > 39°C (high fever), particularly when associated with other signs of organ dysfunction (e.g., hemodynamic instability, respiratory distress, altered mental status) or a high clinical suspicion of severe infection/sepsis, be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate aggressive investigation and treatment of the underlying cause, continuous cardiorespiratory monitoring, management of the systemic effects of the temperature derangement, and comprehensive organ support (Strong recommendation). |
|
respiratory Parameter |
|
We recommend that adult patients whose imaging studies (radiography, ultrasonography, or tomography) reveal a critical finding be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such critical findings include, but are not limited to, those indicating acute respiratory failure (e.g., diffuse bilateral opacities consistent with moderate/severe ARDS), obstructive shock (e.g., cardiac tamponade, massive pulmonary embolism with right ventricular strain, tension pneumothorax), catastrophic vascular events (e.g., acute aortic dissection, ruptured aneurysm), severe neurological compromise (e.g., large intracranial hemorrhage or infarct with mass effect, Cerebral vascular hemorrhage, contusion, subarachnoid haemorrhage, or sever spine injury), or major visceral injury (e.g., perforated viscus, severe solid organ injury with hemorrhage). This is to facilitate immediate life support, intensive monitoring for deterioration, management of organ dysfunction, and timely therapeutic interventions (surgical, radiological, or medical) (Strong recommendation). |
|
abnormalities in blood indices |
|
We recommend that adult patients presenting with critical abnormalities in blood indices that signify or pose an immediate risk of life-threatening organ dysfunction, hemorrhage, or severe systemic illness. T be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such critical findings include, but are not limited to, evidence; severe anemia (Hb < 7 gm % ) causing hemodynamic instability or myocardial ischemia or resulting from massive hemorrhage. severe coagulopathy (INR (>5-6)) or severe thrombocytopenia (< 20000/ mm3) with bleeding (e.g., DIC, Thrombotic Thrombocytopenic Purpura (TTP), or HELLP syndrome.) with active bleeding or Severe Leukopenia / severe neutropenia with sepsis or shock or Hyperleukocytosis/Leukostasis (>100,000/µL) leading to respiratory failure or stroke. This is to facilitate aggressive resuscitation (including massive transfusion), continuous monitoring, treatment of the underlying cause, management of organ failure, and reversal or control of the hematologic or biochemical derangement (Strong recommendation) |
|
Laboratory Values (critical biochemical indices) |
|
We recommend that adult patients presenting with a severe electrolyte disturbance – characterized by an extreme laboratory value posing immediate risk (e.g., K+ >6.5 mmol/L, K+ <2.5 mmol/L, Na+ <120 mmol/L, Na+ >160 mmol/L, elevated serum lactate (e.g., >2-4 mmol/L) Serum calcium > 12 mg /dL or < 6 mg /d with manifestations, severe symptomatic abnormalities of magnesium, or phosphate) or by life-threatening clinical manifestations such as cardiac arrhythmias, tissue hypoperfusion ,seizures, coma, or respiratory muscle failure – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate continuous cardiac and neurological monitoring, frequent laboratory testing, controlled intravenous administration of corrective therapies, management of organ dysfunction, and treatment of the underlying cause (Strong recommendation). |
|
We recommend that adult patients presenting with a life-threatening glycemic crisis be promptly admitted to an Intensive Care Unit (ICU) or or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This includes patients with: (1) severe hypoglycemia (e.g., blood glucose <65 mg/dL or 3.6 mmol/L) causing significant neurological impairment (e.g., coma, seizures) or requiring a continuous intravenous glucose infusion for stabilization; and (2) severe hyperglycemia (e.g., blood glucose >750 mg/dL or 41.6 mmol/L) consistent with severe Diabetic Ketoacidosis (DKA) or Hyperosmolar Hyperglycemic State (HHS). This admission is to facilitate intensive monitoring of neurological, metabolic, and hemodynamic status; aggressive and controlled intravenous fluid, electrolyte, and insulin/glucose therapy; and management of underlying causes and systemic complications (Strong recommendation). |
|
Addmsion & Triage of mass casualty incidents , Pandemic and Epidemic |
|
We recommend that intensive care units be prepared to handle victims of external and internal disasters, including the collapse of surrounding services due to natural or man-made disasters. Every intensive care unit should have general disaster and evacuation plans within the hospital's plans. (Strong recommendation). |
|
We recommend that the declaration of a Mass Casualty Incident (MCI) be followed by the immediate activation of the institutional disaster plan and a coordinated response from the complete healthcare team. This team must ensure the readiness of the institution and its critical care areas—notably the Emergency Department, operating rooms, and the ICU—to efficiently transition from routine to emergency operations and to augment their capacity for a significant influx of critically ill patients. (Strong recommendation). |
|
We suggest at Mass Casualty Incident (MCI) that the emergncy and inetnsive care physicians identify all patients in need of ICU care and those already hospitalized who could be discharged, and then triage and transfer the incoming patients to the most appropriate setting as soon as possible (Strong recommendation). |
|
We recommend that national and regional regulatory bodies, in collaboration with hospitals leadership, develop, fund, and regularly exercise comprehensive plans to enable a rapid and surge in intensive care capacity. These plans should aim to accommodate a significant increase over baseline ICU capacity (with models for extreme events targeting at least 300% expansion) by identifying convertible spaces, pre-allocating necessary resources (equipment, supplies, staffing protocols), and integrating flexible design considerations into healthcare building codes. Furthermore, these plans should establish a clear crisis management authority with the mandate to coordinate resources and patient flow across a region during a declared emergency (Strong recommendation). |
|
We suggest that during mass casualty scenarios, adult patients with severe burns—based on established clinical criteria—may be appropriately managed in general ICU settings to preserve specialized Burn ICU capacity for the most critically injured cases. This approach should be guided by well-coordinated regional and national triage systems to ensure optimal allocation of resources and timely care delivery. (Good practice statement). |
|
We recommend that national and regional regulatory bodies, in collaboration with hospitals leadership, develop, fund, and regularly exercise comprehensive plans for Pandemic & epidemics. These plans should cover national and hospital level. plans should include both triage and dissemination of patients throughout the hospital.Furthermore, these plans should establish a clear crisis management authority with the mandate to coordinate resources and patient flow across a region during a declared epidemics(Strong recommendation). |
|
We suggest during Pandemic and Epidemic not using routine laboratory studies alone in determining the nature of illness. (Good practice statement). |
|
We suggest during Pandemic and Epidemic not using scoring systems alone to determine level of care or removal from higher levels of care because these are not accurate in predicting individual mortality(Good practice statement). |
|
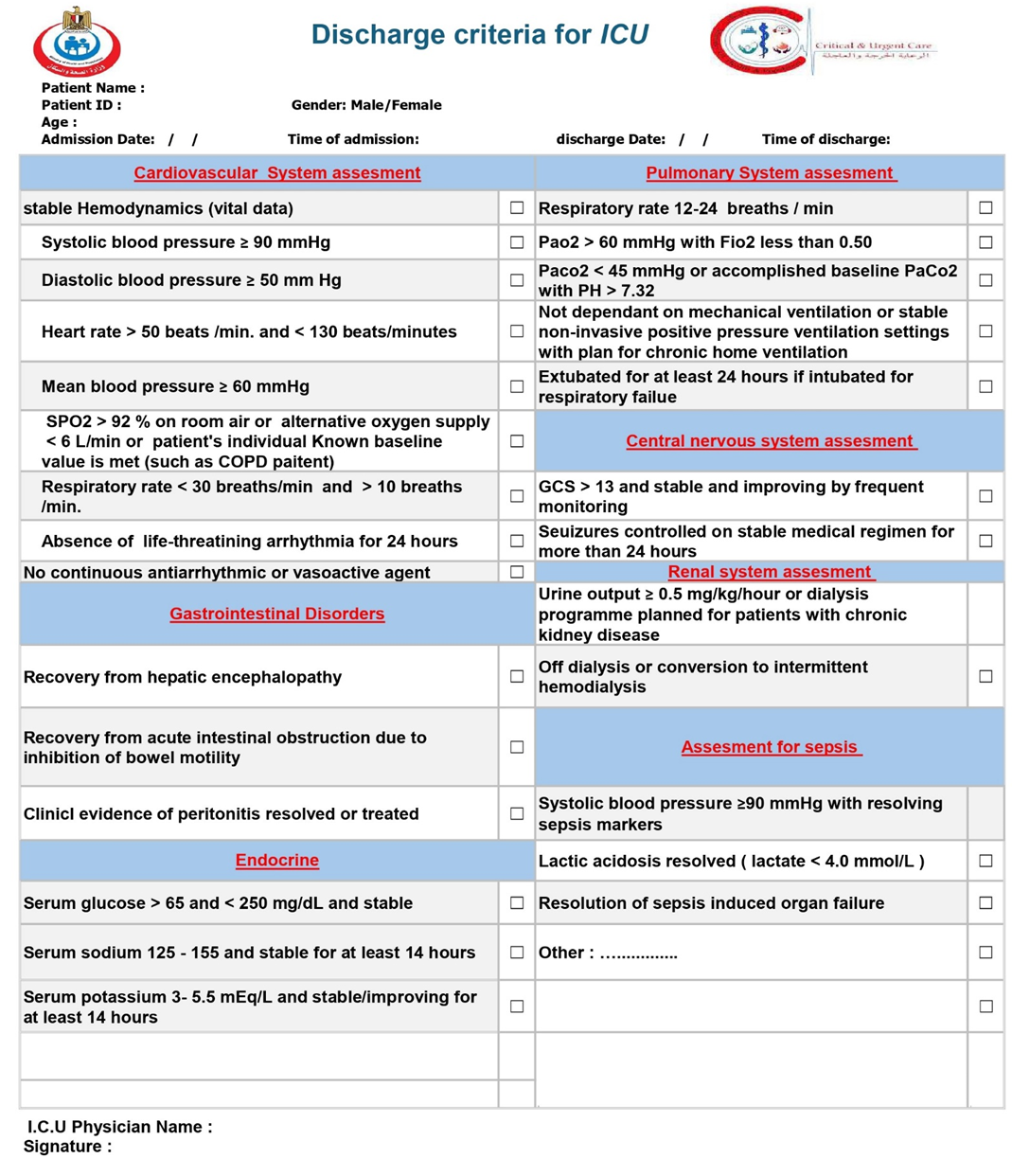
ICU discharge |
|
We recommend avoiding discharge from ICU “after hours” (“night shift”, after 7 pm in institutions with 12-hr shifts). In addition, best practice would seek to optimize evening and night coverage and services(Good practice statement). |
|
We suggest discharging patients at high risk for mortality and readmission (high severity of illness, multiple comorbidities, physiologic instability, and ongoing organ support) to a step-down unit intermediate care units (IMCU) then to the regular ward (Good practice statement). |
|
We recommend that the decision to discharge a patient from an Intensive Care Unit (ICU) be based on a structured, multi-domain assessment. This assessment should be guided by institutional policies that are based on a framework of objective criteria. Key domains to consider include: · the resolution of the acute life-threatening condition that prompted admission · the achievement of physiological stability · Neurological status: be adequately handled and monitored at the receiving unit · Genanral status of the patient be adequately handled and monitored at the receiving unit · able to protect their airway (unless there is a chronic baseline deficit) · Respiratory status: Stable RR 12-24 breaths / min & SpO2 ≥ 92% on room air OR patient's individual Known baseline value is met. · Cardiovascular status:stable hemodynamics, HR, BP, (OR patient's individual Known baseline value) with no arrhythmia or tolerable intermittent arrhythmia for at least 24 hr, with no signs of active bleeding or hypervolemia / hypovolemia · the absence of need for ongoing ICU-specific interventions · with adequately urine output, electrolyte level, and renal function and if need renal replacement therapy is possible outside the ICU · the patient's prognosis and goals of care · the capabilities and availability of resources at the next appropriate level of care (e.g., an intermediate care unit or general ward). This is to facilitate a safe, timely, and appropriate transition of care that minimizes the risk of clinical deterioration and ICU readmission (Strong recommendation). |
|
We suggest that patients with cardiovascular disorders be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to, stable hemodynamics without the need for intravenous vasopressor or inotropic support(Systolic blood pressure ≥ 90 mmHg - Diastolic blood pressure ≥ 50 mm Hg -Heart rate > 50 beats /min. and < 130 beats/minutes) (OR patient's individual Known baseline value); stable respiratory status (OR patient's individual Known baseline value), having been weaned from invasive mechanical ventilation and requiring a low level of oxygen support manageable on a ward or IMCU (SPO2 > 92 % on room air or alternative oxygen supply < 6 L/min- Respiratory rate < 30 breaths/min and > 10 breaths /min.); and the absence of life-threatening cardiac arrhythmias or ongoing myocardial ischemia(Absence of life-threatining arrhythmia for 24 hours -No continuous antiarrhythmic or vasoactive agent) and Resolution of the Acute Insult. This is to ensure a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation). |
|
We suggest that adult patients admitted to the ICU for a pulmonary disorder be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to, successful liberation from invasive mechanical ventilation (as demonstrated by passing a spontaneous breathing trial and successful extubation or stable non-invasive positive pressure ventilation settings with plan for chronic home ventilation) ; stable and adequate gas exchange (e.g., SpO2 ≥ 92% on a low level of oxygen support [FiO2 ≤ 0.4]); absence of respiratory distress (e.g., respiratory rate <25/min, no accessory muscle use); and an effective cough with the ability to manage secretions. This is to ensure a safe transition of care and minimize the risk of respiratory decompensation and ICU readmission (Strong recommendation). |
|
We suggest that adult patients admitted to the ICU for a severe gastrointestinal disorder be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate resolution of the acute crisis and have achieved physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: cessation of life-threatening bleeding with no evidence of re-bleeding; control of intra-abdominal sepsis source; resolution of shock with discontinuation of intravenous vasopressor/inotropic support; stable respiratory status after liberation from mechanical ventilation; and improving or stable organ function. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation). |
|
We suggest that adult patients admitted to the ICU for a severe neurologic disorder be considered for discharge when they demonstrate sufficient neurological and physiological stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: a stable and protected airway (e.g., patient is successfully extubated with adequate consciousness and protective reflexes, or has a stable tracheostomy with manageable respiratory needs); controlled intracranial pressure without need for intensive medical or surgical intervention; cessation of status epilepticus with seizures controlled on a stable medication regimen; and resolution of associated hemodynamic shock and respiratory failure. This is to facilitate a safe transition of care and minimize the risk of neurological deterioration or other complications requiring ICU readmission (Strong recommendation). |
|
We suggest that adult patients admitted to the ICU for a severe endocrine or electrolyte disorder be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: resolution of hemodynamic shock with discontinuation of intravenous vasopressor/inotropic support; neurological stability with the patient being conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit); stable respiratory function after liberation from mechanical ventilation; and correction of the life-threatening metabolic or electrolyte derangement to a safe level that can be managed with oral, subcutaneous, or intermittent intravenous therapies on a ward. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation). |
|
We suggest that adult patients admitted to the ICU for a severe renal disorder be considered for discharge when they demonstrate resolution of the acute life-threatening uremic complications and have achieved hemodynamic and respiratory stability. Key criteria for discharge readiness include, but are not limited to: correction of severe metabolic acidosis and life-threatening hyperkalemia; resolution of severe volume overload and its associated respiratory compromise; neurological stability with resolution of uremic encephalopathy; and stabilization of renal replacement therapy status (either recovery of native kidney function no longer requiring renal replacement therapy, or hemodynamic stability sufficient to transition from continuous to intermittent dialysis manageable in a non-ICU setting). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation). |
|
We recommend that adult patients admitted to the ICU for sepsis or septic shock be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: resolution of shock with discontinuation of intravenous vasopressor or inotropic support; stable respiratory status after liberation from mechanical ventilation and on minimal oxygen support; evidence of adequate source control of the infection; and a clear trajectory of improvement or stabilization of other organ dysfunctions (e.g., neurological, renal, hepatic, hematological, as may be reflected in a decreasing SOFA score). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation). |
|
We recommend that adult patients admitted to the ICU for severe trauma and injuries be considered for discharge when they demonstrate resolution of the acute life-threatening crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: control of hemorrhage with resolution of shock and discontinuation of intravenous vasopressor/inotropic support; stable respiratory status after liberation from mechanical ventilation and with a secure, protected airway; neurological stability with controlled intracranial pressure and cessation of status epilepticus; and evidence that the underlying injuries have been definitively managed or stabilized such that immediate re-operation is not anticipated. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation). |
|
We recommend that adult patients admitted to the ICU for surgical or postoperative care be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability, including neurological stability (e.g., conscious, alert, and able to protect their airway, unless there is a chronic baseline deficit), and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: control of surgical hemorrhage with no evidence of ongoing bleeding; control of any surgical sepsis source; resolution of shock with discontinuation of intravenous vasopressor or inotropic support; stable respiratory status after liberation from mechanical ventilation; and evidence of improving or stable organ function. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation). |
|
We recommend that adult patients admitted to the ICU for severe snake or scorpion envenomation be considered for discharge when they demonstrate resolution of the acute life-threatening systemic envenomation syndrome and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: for neurotoxic envenomation, recovery of respiratory muscle function with successful liberation from mechanical ventilation and a secure airway; for hemotoxic envenomation, cessation of bleeding and sustained normalization of coagulation parameters; for cardiotoxic envenomation, resolution of shock with discontinuation of intravenous vasopressor/inotropic support and absence of life-threatening arrhythmias; and improvement or stabilization of any associated organ dysfunction (e.g., acute kidney injury). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence of toxicity in ICU then step down to IMCU if need this level of care then A period of observation (e.g., 12-24 hours) befor discharge to ward or home. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation). |
- Recommendations
|
Recommendations |
Reference |
|
General considerations |
|
|
We recommend that critically ill patients be transferred from the emergency department ,ward bed or Intermediate Care Units (IMCUs) to an available Intensive Care Unit (ICU) bed as rapidly as possible, ideally in less than or equal to 1 hour from the time the ICU bed is confirmed available and the decision to transfer is finalized. This is to minimize delays in accessing specialized ICU monitoring and interventions and to reduce potential risks associated with prolonged holding in non-ICU environments (Strong recommendation, low-quality evidence). |
1,2 |
|
We recommend that in circumstances where a critically ill patient requires ICU services that are unavailable within the current hospital or cannot be provided in a timely manner, clinicians immediately utilize officially established national or regional referral pathways to facilitate rapid assessment and transfer to an appropriate ICU. In Egypt, this includes contacting the National Project of Critical Care, Neonatal, and Emergency Services "Rayat Misr" through its designated electronic platform or emergency hotline (137) as per national protocols (Strong recommendation, low -quality evidence). |
1,2,3,4,5,6,7 |
|
We recommend that individual hospitals and their Intensive Care Unit (ICU) leadership formulate and regularly review explicit ICU admission and triage policies follow this guidline. These policies should be tailored to their specific institutional context, including the scope of clinical services provided (e.g., trauma, burn, neurocritical care, hepatic care), the demographic characteristics of their patient population, current ICU capacity, and available therapeutic resources (Strong recommendation, moderate-quality evidence). |
1,8,9,10 |
|
We suggest that Triage decisions must be made transparently and without any prejudice. Factors like ethnicity, race, sex, social standing, or financial resources are wholly irrelevant. (Good practice statement, low-quality evidence). |
1,8,9,10 |
|
We recommend that hospitals and their ICU leadership develop, implement, and regularly review explicit, transparent, and fair policies for the triage and allocation of ICU beds. These policies should provide a clear framework for balancing scheduled postoperative admissions with emergency admissions. This includes defining a process for temporarily reserving beds for imminent high-risk surgical arrivals while also having a dynamic override mechanism, managed by a designated triage officer or clinical leader (e.g., ICU director), to ensure any patient with an immediate life-threatening condition can access a necessary bed with minimal delay. Unjustified or prolonged reservation of an empty ICU bed in the face of a critically ill patient needing admission is inconsistent with ethical principles of justice and beneficence (Strong recommendation, moderate-quality evidence). The core issue is one of triage and resource allocation. An ICU bed is a scarce, high-cost resource. A structured, transparent policy is essential to:
|
1,2, 11 |
|
We recommend that hospitals, where feasible and appropriate based on patient population needs, establish Intermediate Care Units (IMCUs). These units should serve as a bridge between the general ward and the Intensive Care Unit to provide enhanced monitoring and a higher level of nursing care for two primary patient groups: those who no longer require intensive care but are too unstable for the general ward (step-down), and those who are deteriorating on the ward but may not require immediate ICU-level organ support (step-up). The implementation of IMCUs is intended to improve patient safety, reduce ICU readmissions, optimize the use of critical care beds, and potentially lower overall costs for specific high-risk patient populations. (Strong recommendation, moderate-quality evidence). The optimization of hospital resources while ensuring patient safety represents a significant challenge in modern healthcare. A critical gap often exists between the high-intensity, resource-heavy environment of the Intensive Care Unit (ICU) and the standard monitoring available on a general medical or surgical ward. Intermediate Care Units (IMCUs), also known as Step-Down or High-Dependency Units, are designed to bridge this gap, offering a level of care for patients who are too ill or unstable for the general ward but do not require the advanced organ support of an ICU. |
12,13,14,15, 390 |
|
We recommend that hospitals develop and implement a Rapid Response System to facilitate early identification, bedside assessment, and appropriate triage of clinically deteriorating patients on general wards. This system should include a clear set of vital sign-based trigger criteria (such as: Modified Early Warning Score ) Fig. 1 and a designated team with critical care skills to respond promptly Rapid Response Team (RRT). A primary function of this team should be to stabilize the patient and facilitate timely and appropriate admission to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) when indicated (Strong recommendation, High-quality evidence). A key element of contemporary patient safety programs is the Rapid Response System (RRS). Its purpose is to recognize and intervene with patients whose condition is worsening, aiming to prevent serious adverse events like cardiac arrest. This forward-thinking strategy has demonstrated a reduction in hospital deaths and an enhancement of patient results. Putting a successful RRS into practice involves several key aspects: straightforward activation standards, a specialized and capable response team, thorough training for all staff, and a dedication to ongoing quality enhancement. This guide details the fundamental elements and stages for creating and rolling out a successful Rapid response System in a hospital environment. The Four Cornerstones of a Rapid Response System An effective RRS is founded on four interrelated cornerstones:
|
16, 17, 18 ,19 ,20, 21, 22, 23,26, 27, 353, 391 |
|
We recommend that RRSs be utilized for early review of acutely ill non-ICU patients to identify patients who need or would benefit from ICU admission and treatment and to prevent unnecessary ICU admissions (Strong recommendation, moderate-quality evidence). When a patient on a general ward triggers the RRS—often due to concerning changes in vital signs, respiratory distress, or altered mental status—a team of critical care experts, typically including an ICU nurse, a respiratory therapist, and sometimes a critical care physician or advanced practice provider, is dispatched to the patient's bedside. The RRS team conducts a rapid but comprehensive assessment that goes beyond a simple review of vital signs. This evaluation is tailored to the patient's specific presentation and may include:
The decision to transfer a patient to the ICU is not based on a single parameter but is a complex clinical judgment made by the RRS team in collaboration with the primary medical team. The core of this decision-making process revolves around three key questions: 1. Does the patient require advanced organ support? This is a primary driver for ICU admission and includes the need for mechanical ventilation, vasopressors to support blood pressure, or renal replacement therapy. The RRS team's critical care expertise is vital in identifying the subtle signs that a patient is heading towards requiring such interventions. 2. Would the patient benefit from the level of monitoring available only in the ICU? Some patients may not immediately require invasive interventions but are at high risk of rapid deterioration. The continuous monitoring of vital signs, cardiac rhythms, and other physiological parameters in the ICU can be life-saving for these individuals. A key function of the RRS is to act as an "ICU without walls," bringing critical care expertise to the patient's bedside and often preventing the need for a physical transfer to the ICU. The RRS can achieve this through several interventions:
|
23, 24, 25, 26, 27, 391 |
|
We recommend implementing ICU consult teams to support ward/IMCU staff with deteriorating patients, facilitate transfer to ICU, and reduce ICU readmission rates. (Good practice statement, low-quality evidence). |
1, 26, 27, 28, 29, 30 |
|
Admission & Triage |
|
|
We suggest using the following tools for bed allocation during the admission and triage processes(Good practice statement, low-quality evidence). : Guide to resource allocation of intensive monitoring and care including levels of monitoring, care, and nursing ratios (table 2) ICU Admission Prioritization framework(table 3) |
1, 17, 18, 31, 32 |
|
We suggest using the following tools as core of addmsion and discharge criteria checklist(Good practice statement, low-quality evidence): 1- addmsion checklist (table 4,5)
2- discharge criteria checklist(table 6):
|
1, 13, 27, 33, 35, 418 |
|
We recommend that the Acute Physiology and Chronic Health Evaluation (APACHE II) score, or a similar validated illness severity scoring system, be used as an adjunct to clinical assessment for patients being considered for Intensive Care Unit (ICU) admission. The calculation of an APACHE score upon presentation to the emergency department or for deteriorating ED/ward patients can provide valuable, objective information regarding the severity of illness and risk of mortality. A high or significantly rising score should be considered a strong indicator for the need for ICU-level care, facilitating timely and appropriate triage, especially for patients with conditions known to have a high mortality risk such as sepsis, acute respiratory distress syndrome (ARDS), and major trauma. It is crucial to emphasize that the APACHE score should not be used in isolation to determine ICU admission or discharge. It is a decision-support tool that, when integrated with a comprehensive clinical evaluation, patient preferences, and the overall clinical context, can lead to more informed and effective patient care.(Good practice statement, low-quality evidence). |
34 ,36, 37, 38 |
|
We recommended that patients with invasive mechanical ventilation or complex life-threatening conditions, including sepsis, receive care in an ICU. Additionally, weaning from mechanical ventilation should be restricted to an ICU or In necessities step down to a intermediate care unit (IMCU) , and not take place on a general ward. (Strong recommendation, moderate-quality evidence). |
1, 33, 39 |
|
We suggest avoiding admitting to a specialized ICU patients with a primary diagnosis not associated with that specialty (i.e., boarding) (Strong recommendation, moderate-quality evidence). |
1, 40, 285 |
|
Triage |
|
|
We suggest that hospitals and ICU leaders develop and implement admission and triage policies that are designed to minimize under-triage and overtriage is more acceptable (Good practice statement, low-quality evidence). Rationale for the Principle of Preferring Over-Triage: This principle is a cornerstone of patient safety in emergency and critical care triage. It acknowledges the different consequences of the two types of triage errors:
|
1, 2, 17, 24, 41 |
|
Diagnostic criteria |
|
|
We recommend that all patients presenting with ST-Elevation Myocardial Infarction (STEMI), ST-Elevation Myocardial Infarction (STEMI), Non-ST-Elevation Myocardial Infarction (NSTEMI) and other patients with Acute Coronary Syndromes (ACS) identified as high-risk (based on clinical features, ECG findings, cardiac biomarkers, hemodynamic instability, life-threatening arrhythmias, ongoing ischemia, acute heart failure and validated risk scores) be admitted to a Coronary Care Unit (CCU) an Intensive Care Unit (ICU), or an intermediate care unit (IMCU) with. This setting is necessary for continuous cardiac and hemodynamic monitoring, prompt management of life-threatening complications facilitation of timely reperfusion or invasive strategies, and optimization of medical therapy that require Intensive care, such as heart failure, cardiogenic shock, or serious arrhythmias, ventricular septal rupture, even if their initial condition appears stable, facilitation of timely reperfusion/revascularization strategies, and optimization of medical therapy (Strong recommendation, moderate-quality evidence). The primary purpose of admitting high-risk ACS patients to an ICU/CCU is to provide intensive monitoring and immediate intervention for life-threatening complications that are most common in the early hours and days after the acute event.
|
33, 42, 43, 44, 45, 46, 47, 48 |
|
We recommend that all patients diagnosed with cardiogenic shock characterized by persistent hypotension despite adequate fluid status and signs of end-organ hypoperfusion. be immediately admitted to an to a Coronary Care Unit (CCU) or Intensive Care Unit (ICU) or a specialized cardiac/cardiovascular ICU with equivalent capabilities This is to facilitate immediate and continuous hemodynamic monitoring, aggressive management with intravenous vasoactive medications, advanced respiratory support, rapid investigation and treatment of the underlying cause, and consideration for mechanical circulatory support (Strong recommendation, moderate-quality evidence). Admition is considered essential due to the need for:
|
33, 42, 43, 44, 45, 46, 47,49, 50, 51, 52, 53, 54 |
|
We recommend that patients presenting with arrhythmias be admitted to an a specialized Coronary Care Unit (CCU) or Intensive Care Unit (ICU) if the arrhythmia is life-threatening (e.g., sustained ventricular tachycardia, ventricular fibrillation, symptomatic high-grade atrioventricular block), causes hemodynamic instability (e.g., hypotension, shock, acute heart failure), is associated with severe symptoms directly attributable to the arrhythmia (e.g., syncope with a high-risk rhythm), or requires urgent electrical interventions (cardioversion, defibrillation, pacing) or pharmacological interventions with intravenous agents that necessitate continuous cardiorespiratory monitoring not feasible or safe in a lower-acuity setting (Strong recommendation, moderate-quality evidence). Patients with specific arrhythmias are admitted to an ICU/CCU due to:
|
33, 55, 56, 57, 58, 358 |
|
We recommend that patients with acute decompensated heart failure (ADHF) who exhibit signs of hemodynamic instability (e.g., hypotension, cardiogenic shock), severe respiratory distress or failure (requiring non-invasive or invasive mechanical ventilation), life-threatening arrhythmias, or who require intravenous vasoactive medications or invasive hemodynamic monitoring, be admitted to an Intensive Care Unit (ICU) or a Intensive Coronary Care Unit (CCU) for intensive management and monitoring (Strong recommendation, moderate-quality evidence). ADHF represents a spectrum of clinical severity. While many patients can be managed on general medical wards, those with severe ADHF require ICU/CCU admission due to:
|
33, 48, 49, 59, 60, 358 |
|
We recommend that patients presenting with a hypertensive emergency (defined as severely elevated blood pressure accompanied by acute, ongoing target organ damage) be admitted to an Intensive Care Unit (ICU) or a Intensive Coronary Care Unit (CCU) or a comparable high-acuity monitored setting. This is to facilitate immediate and controlled parenteral antihypertensive therapy, continuous (often invasive) blood pressure monitoring, and close observation and management of specific target organ dysfunction (Strong recommendation, moderate-quality evidence). It is vital to differentiate:
Patients with hypertensive emergencies require ICU admission due to the need for:
|
33, 61, 62, 63, 64, 65 |
|
We recommend that adult patients who achieve Return of Spontaneous Circulation (ROSC) after cardiac arrest and remain comatose or hemodynamically unstable, or who require ongoing ventilatory support, be admitted to an Intensive Care Unit (ICU) or a Coronary Care Unit (CCU) with equivalent ICU capabilities for comprehensive post-resuscitation care (Strong recommendation, moderate-quality evidence). Patients who achieve ROSC after cardiac arrest are critically ill and suffer from post-cardiac arrest syndrome. This complex syndrome includes:
Management of these patients in an ICU is essential for:
|
33, 66, 67, 68, 69 |
|
We recommend that patients diagnosed with cardiac tamponade, especially those exhibiting hemodynamic instability or requiring urgent pericardial drainage, be admitted to an Intensive Care Unit (ICU) or a Coronary Care Unit (CCU) with equivalent capabilities for continuous cardiorespiratory monitoring, management of potential complications, and further diagnostic evaluation and treatment of the underlying cause (Strong recommendation, moderate-quality evidence) Admission to an ICU/CCU is generally indicated for patients with cardiac tamponade, particularly if they exhibit hemodynamic compromise, due to the need for:
|
33, 70, 71, 72 |
|
We recommend that all patients diagnosed with or strongly suspected of having an Acute Aortic Syndrome (including aortic dissection, intramural hematoma, or penetrating atherosclerotic ulcer) be immediately admitted to an Intensive Care Unit (ICU) or a specialized cardiovascular ICU capable of providing comprehensive medical and peri-interventional management (Strong recommendation, moderate-quality evidence). AAS encompasses a group of life-threatening conditions including aortic dissection (AD), intramural hematoma (IMH), and penetrating atherosclerotic ulcer (PAU). These conditions are medical emergencies due to the high risk of aortic rupture, end-organ malperfusion, and death. Patients diagnosed with or strongly suspected of having AAS require immediate admission to an ICU or a specialized cardiovascular ICU. This is critical due to the need for:
|
33, 73, 74, 75, 76, 77, 78 |
|
We recommend that adult
patients presenting with sever valvular heart disease such as severe
acute mitral regurgitation, particularly when characterized by signs of
respiratory failure (e.g., pulmonary edema requiring advanced respiratory
support) or hemodynamic instability (e.g., hypotension, shock), be promptly
admitted to an Intensive Care Unit (ICU) or a specialized Cardiovascular/Coronary
Care Unit (CVICU/CCU). This is to facilitate immediate hemodynamic
stabilization with intravenous vasoactive medications (vasodilators and/or
inotropes), advanced respiratory support (non-invasive or invasive
ventilation), intensive monitoring, and optimization as a bridge to urgent
surgical intervention, which is the definitive therapy (Strong
recommendation, moderate-quality evidence). ICU/CCU admission is critical for patients with hemodynamically significant AMR due to the need for:
|
33,53, 54, 420, 421, 422, 423, 424, 425 |
|
Gastrointestinal Disorders |
|
|
We recommend that patients presenting with life-threatening gastrointestinal bleeding (UGIB or LGIB), characterized by hemodynamic instability (e.g., shock, persistent hypotension despite initial resuscitation), ongoing massive hemorrhage requiring significant transfusion, or validated high-risk scores indicating severe bleeding or high re-bleeding risk, be admitted to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive resuscitation, continuous hemodynamic monitoring, urgent diagnostic and therapeutic interventions (often endoscopic), specialized pharmacotherapy, and management of potential complications (Strong recommendation, moderate-quality evidence). Admission to an ICU (or a high-dependency unit with equivalent capabilities) is crucial for such patients due to the need for:
|
33, 79, 80, 81, 82, 83, 84, 85, 86, 87 |
|
We recommend that all patients diagnosed with Acute Liver Failure (ALF) / Fulminant Liver Failure (FLF) – characterized by severe acute liver injury with coagulopathy (INR ≥1.5) and any degree of hepatic encephalopathy (or those without initial encephalopathy but with rapid deterioration of liver function and coagulopathy indicating high risk of imminent ALF/FLF) – be promptly admitted to an Intensive Care Unit (ICU). Ideally, this should be a specialized liver unit or transplant center operating under a high-intensity ICU model, characterized by the intensivist being primarily responsible for or having mandatory daily co-management in the day-to-day care of the patient, ensuring expert critical care input alongside hepatology or/and transplant surgery expertise (Strong recommendation, moderate-quality evidence). Acute Liver Failure is a critical medical emergency characterized by rapid and severe liver injury, impaired liver synthetic function (coagulopathy with INR ≥1.5), and the development of hepatic encephalopathy (any degree of altered mental status) in individuals without pre-existing cirrhosis. The condition is associated with a high risk of life-threatening complications, including:
|
33, 88, 89, 90, 91, 92, 93 |
|
We recommend that all patients diagnosed with severe acute pancreatitis, defined by the presence of persistent organ failure (>48 hours), be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This includes, but is not limited to, aggressive goal-directed fluid therapy, management of respiratory and cardiovascular failure, renal replacement therapy if indicated, specialized nutritional support, advanced pain control, and monitoring and management of local and systemic complications (Strong recommendation, moderate-quality evidence). Severe acute pancreatitis, as defined by the Revised Atlanta Classification and other international guidelines, is characterized by persistent organ failure (lasting >48 hours), which may involve one or multiple organ systems (respiratory, cardiovascular, renal). It is often associated with pancreatic necrosis and a profound systemic inflammatory response syndrome (SIRS), leading to multi-organ dysfunction syndrome (MODS). This life-threatening condition necessitates ICU admission for:
|
33, 94, 95, 96, 97, 98, 99, 100, 101 |
|
We recommend that patients diagnosed with or strongly suspected of having esophageal perforation, with or without initially evident mediastinitis, be promptly admitted to an Intensive Care Unit (ICU). (Strong recommendation, moderate-quality evidence). Esophageal perforation is a highly lethal surgical emergency. The breach in esophageal integrity allows immediate and continued contamination of the mediastinum and/or pleural or peritoneal cavities with oropharyngeal secretions, gastric contents, and bacteria. This leads to:
Given these life-threatening sequelae, patients with esophageal perforation almost invariably require admission to an ICU or a specialized high-acuity surgical unit. This is essential for:
|
33, 102, 103, 104, 105, 106, 107 |
|
We recommend that patients presenting with acute gastroenteritis complicated by severe dehydration leading to hemodynamic instability (e.g., shock, manifested by hypovolemic shock ,persistent hypotension despite initial fluid challenge, significant end-organ hypoperfusion (e.g., oliguria/anuria, altered mental status)), or critical electrolyte or acid-base or acute kidney injury requiring intensive management – be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive and goal-directed fluid resuscitation, continuous hemodynamic and laboratory monitoring, potential vasopressor support, correction of critical electrolyte and acid-base abnormalities, and management of organ dysfunction (Strong recommendation, moderate-quality evidence). gastroenteritis are self-limiting, severe dehydration is a life-threatening complication that can lead to:
Admission to an ICU is typically indicated when severe dehydration leads to these complications, requiring:
|
33, 108, 109, 110 |
|
Endocrine and electrolyte disturbance |
|
|
We recommend that adult patients presenting with severe Diabetic Ketoacidosis (DKA) – characterized by criteria such as arterial pH <7.1, serum bicarbonate <10 mEq/L, significant ketonemia/ketonuria with altered mental status (stupor/coma), or hemodynamic instability – and all patients with Hyperosmolar Hyperglycemic State (HHS) – characterized by marked hyperglycemia (often >600 mg/dL or >33.3 mmol/L), high effective serum osmolality (often >320 mOsm/kg), profound dehydration, and altered mental status – be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities. This admission is essential for aggressive intravenous fluid and electrolyte management, continuous intravenous insulin therapy with frequent and precise monitoring, close observation for neurological and cardiovascular complications, and identification and management of precipitating factors or concurrent organ dysfunction (Strong recommendation, moderate-quality evidence). severe DKA and virtually all cases of HHS are life-threatening metabolic emergencies. Admission to an ICU/HDU is generally indicated for these severe presentations due to:
|
33, 111, 112, 113, 114, 115, 116 |
|
We recommend that all patients diagnosed with or highly suspected of having thyroid storm be promptly admitted to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity and potential for rapid deterioration, we suggest their care be managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists (Strong recommendation, moderate-quality evidence). Thyroid storm is a rare but life-threatening exacerbation of hyperthyroidism, characterized by acute and severe multisystem decompensation. It carries a significant mortality rate (10-30%) even with treatment. Admission to an ICU is considered essential due to the need for:
|
33, 117, 118, 119, 120, 121 |
|
We recommend that all patients diagnosed with or highly suspected of having myxedema coma be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity and potential for rapid deterioration, we suggest their care be managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists(Strong recommendation, moderate-quality evidence). Myxedema coma is a rare, life-threatening, extreme manifestation of decompensated hypothyroidism. It is a medical emergency with a high mortality rate (historically 25-60%, though improving with early recognition and aggressive management). Admission to an ICU is considered essential due to the profound multi-system derangements and the need for intensive monitoring and support, including:
|
33, 122, 123, 124, 125, 126, 127 |
|
We recommend that all adult patients presenting with adrenal crisis complicated by hemodynamic instability (e.g., hypotension refractory to initial fluid challenges, signs of shock) be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity of managing shock, electrolyte disturbances, and potential multi-organ involvement, we suggest their care managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists(Strong recommendation, moderate-quality evidence). Adrenal crisis (acute adrenal insufficiency) is a life-threatening endocrine emergency characterized by an acute deficiency of cortisol, often accompanied by aldosterone deficiency in primary adrenal insufficiency. When complicated by hemodynamic instability (i.e., hypotension progressing to shock, often refractory to initial fluid resuscitation alone), it signifies a state of severe physiological decompensation with high mortality if not recognized and treated promptly and aggressively. ICU admission is essential for such patients due to the need for:
|
33, 128, 129, 130, 131 |
|
We recommend that adult patients presenting with life-threatening hypoglycemia – characterized by severe neuroglycopenia (e.g., coma, seizures, significantly altered mental status requiring external assistance for recovery) or those requiring continuous intravenous glucose infusions with very frequent monitoring to prevent relapse and maintain euglycemia – be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. (Strong recommendation, moderate-quality evidence). Admission to an ICU is typically indicated for such patients due to the need for:
|
33, 132, 133, 134, 135, 136, 137, 138 |
|
Obstetric emergency |
|
|
We recommend that all patients presenting with eclampsia, severe pre-eclampsia with severe features (including but not limited to severe hypertension, evidence of significant end-organ dysfunction), or HELLP syndrome be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the complexity and potential for rapid deterioration, we suggest their care be managed within a high-intensity ICU/ IMCU model, characterized by experienced multidisciplinary input including obstetricians, anesthesiologists, intensivists, and neonatologists, with clear protocols for escalation and management This includes continuous hemodynamic monitoring, seizure prophylaxis with magnesium sulfate, antihypertensive therapy, and preparation for potential delivery. (Strong recommendation, moderate-quality evidence). These conditions represent the most severe end of the spectrum of hypertensive disorders of pregnancy and are major causes of maternal and perinatal morbidity and mortality. Admission to an ICU/ IMCU is crucial due to the need for:
|
33, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148 |
|
We recommend that all obstetric patients (pregnant or postpartum) who develop significant acute organ dysfunction (e.g., sever postpartum hemaorage, cardiovascular collapse/shock, severe respiratory failure requiring advanced support, acute kidney injury requiring renal replacement therapy, severe coagulopathy, or profound neurological impairment, sever trauma) be promptly admitted to an an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the unique physiological changes of pregnancy and the need for coordinated multidisciplinary care (obstetrics, critical care, anesthesia, neonatology), we suggest their care be managed within a high-intensity ICU/ IMCU model includes continuous hemodynamic monitoring, respiratory support, renal replacement therapy, and other advanced interventions as necessary. (Strong recommendation, moderate-quality evidence). Obstetric patients can develop significant organ dysfunction due to a variety of pregnancy-specific conditions (e.g., obstetric hemorrhage, amniotic fluid embolism, acute fatty liver of pregnancy, peripartum cardiomyopathy) or non-obstetric conditions occurring during or aggravated by pregnancy (e.g., sepsis, pneumonia/ARDS, cardiac disease, trauma). "Significant organ dysfunction" implies failure of one or more vital organ systems (cardiovascular, respiratory, renal, hepatic, neurological, hematological) that threatens the mother's life and often the fetus's well-being. Admission to an ICU/ IMCU is crucial in such cases for:
|
33, 139, 140, 141, 149, 150, 151, 152, 153 |
|
We recommend that pregnant patients with Hyperemesis Gravidarum (HG) who develop severe, life-threatening complications. Such complications include, but are not limited to, profound dehydration leading to hypovolemic shock or severe acute kidney injury (AKI), severe refractory electrolyte imbalances (e.g., critically low potassium or sodium) causing cardiac or neurological symptoms, Wernicke's encephalopathy, or esophageal complications. be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the unique physiological changes of pregnancy and the need for coordinated multidisciplinary care (obstetrics, critical care, anesthesia, neonatology), we suggest their care be managed within a high-intensity ICU/ IMCU model includes continuous hemodynamic monitoring, respiratory support, renal replacement therapy, and other advanced interventions as necessary. (Strong recommendation, moderate-quality evidence). While most cases of HG are managed on general inpatient wards or as outpatients, a small but critical subset can develop severe, life-threatening complications requiring ICU admission. These complications include:
|
33, 139, 140, 154, 155, 156, 157 |
|
We recommend that adult patients presenting with severe obstetric or gynecologic bleeding, characterized by hemodynamic instability (e.g., shock, persistent hypotension despite initial fluid resuscitation), ongoing massive hemorrhage requiring significant transfusion (e.g., activation of massive transfusion protocol), or evidence of significant end-organ hypoperfusion or coagulopathy, be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive resuscitation including balanced blood product replacement, continuous hemodynamic monitoring, urgent interventions for source control (medical, radiological, or surgical), specialized pharmacotherapy (e.g., tranexamic acid, uterotonics), and management of potential complications such as coagulopathy, ARDS, or AKI (Strong recommendation, moderate-quality evidence). every obstetric bleeding (e.g., postpartum hemorrhage (PPH), placental abruption, ruptured ectopic pregnancy, placenta accreta spectrum) and severe acute gynecologic bleeding (e.g., from ruptured ovarian cysts, advanced gynecologic cancers, severe abnormal uterine bleeding, postoperative hemorrhage) are major causes of maternal/female morbidity and mortality. "Severe" bleeding implies hemodynamic instability (hypovolemic shock), the need for massive transfusion, or evidence of end-organ hypoperfusion and coagulopathy. Admission to an ICU or a unit with intermediate care capabilities is crucial for such patients due to the need for:
|
33, 139, 140, 141, 149, 158, 159, 160, 161, 162, 163, 164 |
|
Trauma and injures |
|
|
We recommend that all adult patients presenting with severe traumatic brain injury or post concussion manifestations, defined by a Glasgow Coma Scale (GCS) score of ≤ 8 after initial resuscitation, be promptly admitted to an Intensive Care Unit (ICU) capable of providing comprehensive neurocritical care. This includes airway protection, mechanical ventilation, intracranial pressure monitoring, hemodynamic support, and multidisciplinary care. Given the complexity of managing severe TBI and the potential for rapid neurological deterioration, we suggest their care be managed within a high-intensity neuro-ICU model, characterized by the intensivist (often a neurointensivist or an intensivist with neurocritical care expertise) being primarily responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with neurosurgery and other relevant specialists (Strong recommendation for ICU admission, moderate-quality evidence Conditional recommendation for specific ICU model,low quality evidence) Patients with severe TBI (GCS ≤ 8) are at high risk of mortality and severe long-term disability. ICU admission is critical for:
|
33, 165, 166, 167, 168, 169 |
|
We recommend that adult patients with an acute spinal cord injury resulting in significant neurological deficit (e.g., quadriplegia, paraplegia) that causes or poses an imminent risk of respiratory failure (typically injuries at or above the C5 level) or hemodynamic instability (neurogenic shock, typically from injuries at or above the T6 level) be promptly admitted to preferably a specialized Neuro-ICU or Intensive Care Unit (ICU), preferably one with expertise in neurocritical care and trauma. This is to facilitate advanced airway and respiratory support (including mechanical ventilation), intensive hemodynamic monitoring and management to maintain spinal cord perfusion, prevention and treatment of systemic complications, and expert multidisciplinary care in conjunction with neurosurgery and spine surgery teams (Strong recommendation, moderate-quality evidence). acute SCI, particularly injuries affecting the cervical or high thoracic spinal cord, often leads to life-threatening physiological derangements that necessitate admission to an ICU. The primary drivers for ICU admission are:
|
33, 165, 170, 171, 172, 173, 174, 175 |
|
We recommend that adult patients presenting with significant solid organ injury, classified as American Association for the Surgery of Trauma (AAST) Grade III or higher (either single or multiple organs), be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for intensive monitoring and management. This is to facilitate continuous hemodynamic and hematological assessment, early detection of bleeding or failure of non-operative management, readiness for urgent angiographic or surgical intervention, aggressive pain control, and management of associated injuries or systemic complications. For patients who are hemodynamically unstable or have evidence of ongoing bleeding despite initial resuscitation, direct ICU admission is strongly recommended (Strong recommendation, moderate-quality evidence). Patients sustaining solid organ injuries (e.g., to the liver, spleen, kidneys, pancreas, urogenital ) classified as American Association for the Surgery of Trauma (AAST) Grade III or higher are at substantial risk for serious complications, even if initially hemodynamically stable and selected for non-operative management (NOM). Admission to an ICU or a closely monitored environment like an IMCU is often crucial for:
|
33, 165, 176, 178, 179, 180, 181, 182, 183 |
|
We recommend that all adult patients presenting with polytrauma who have a high probability of needing major intervention (e.g., surgery, angiography) and/or require intensive physiological monitoring and support due to actual or impending organ dysfunction or hemodynamic instability be promptly admitted to an Intensive Care Unit (ICU), preferably one within a designated trauma center with readily available multidisciplinary trauma expertise. (Strong recommendation, moderate-quality evidence). Admission to an ICU is crucial for such patients due to the need for: Management of Hemorrhagic Shock and Trauma-Induced Coagulopathy (TIC): Aggressive resuscitation with blood products according to massive transfusion protocols (MTPs), control of ongoing hemorrhage (surgical, angiographic), and specific management of TIC. Airway Management and Advanced Respiratory Support: Many polytrauma patients require endotracheal intubation and mechanical ventilation due to traumatic brain injury (TBI with GCS ≤ 8), thoracic trauma (e.g., flail chest, pulmonary contusions, hemopneumothorax), altered mental status from shock, or for operative procedures. ARDS is a common complication requiring specialized ventilator strategies. Intensive Neurological Monitoring and Management: For patients with associated TBI, including monitoring for and management of intracranial hypertension (ICHtn) and optimization of cerebral perfusion pressure (CPP). Support for Multiple Organ Dysfunction Syndrome (MODS): Polytrauma frequently leads to SIRS and MODS, affecting cardiovascular, respiratory, renal, hepatic, and coagulation systems, requiring integrated organ support. Continuous Hemodynamic Monitoring: Often invasive (arterial line, central venous catheter, advanced cardiac output monitoring) to guide resuscitation and vasoactive drug therapy. Post-Operative Critical Care: Following damage control surgery or other major operative interventions. Pain Management: Complex pain management strategies are often required for multiple injuries. Monitoring for Missed Injuries and Complications: Such as compartment syndromes, sepsis, venous thromboembolism (VTE), fat embolism syndrome. Coordination of Multidisciplinary Care: Involving trauma surgeons, intensivists, orthopedic surgeons, neurosurgeons, anesthesiologists, interventional radiologists, and other specialists. |
33, 165, 176, 178, 179, 180, 184, 185, 186, 187 |
|
We recommend that decisions regarding ICU admission for adult burn patients should carefully consider factors such as the type of burn, percentage of Total Body Surface Area (%TBSA) affected, presence of inhalation injury, location of burns, associated trauma, patient age, pre-existing comorbidities, and the number of victims in large-scale mass casualty incidents. Specifically, under normal circumstances, we advise that adult patients presenting with severe second- or third-degree burns—including partial-thickness burns exceeding 15–20% TBSA, full-thickness burns exceeding 5–10% TBSA, require mechanical ventilation (eg, significant inhalation injuries, massive fluid resuscitation), electrical or major chemical burns, burns involving critical areas (face, hands, feet, genitalia, perineum, or major joints), or burns in individuals with significant pre-existing medical conditions or accompanying traumatic injuries—be ideally admitted to a dedicated Burn Intensive Care Unit (ICU) within a specialized Burn Center. Given the complex and highly specialized nature of burn care, we strongly suggest that these patients be managed by an experienced multidisciplinary burn team, comprising intensivists, burn surgeons, specialized nurses, respiratory therapists, and nutritionists within an ICU setting. (Strong recommendation, moderate-quality evidence). Not all 2nd or 3rd-degree burns necessitate ICU admission. The decision is critically dependent on Burn Center care for severe injuries inherently involves ICU-level management for the acute phase. Criteria typically include:
Severe burns are profound injuries leading to complex pathophysiological changes that require intensive, multidisciplinary care. ICU admission is crucial for:
|
33, 188, 189, 190, 191, 192, 193, 194 |
|
We recommend that adult patients presenting with severe burns defined by criteria be admitted to an Intensive Care Unit (ICU). While admission to a specialized Burn ICU within a designated Burn Center is the optimal standard of care, a general ICU can and should provide the necessary life-saving critical care for these patients when a specialized Burn ICU is not immediately available or in/During mass casualty scenarios.( Good practice statement, low-quality evidence). |
33, 191, 192, 193, 194 |
|
We recommend that adult patients presenting with life-threatening crush injuries – characterized by extensive muscle damage, prolonged compression, evidence of or high risk for Crush Syndrome (e.g., significant rhabdomyolysis, hyperkalemia, early AKI), severe compartment syndrome, or associated hemodynamic instability – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate aggressive resuscitation including Correction of Metabolic Acidosis and Other Electrolyte Disturbances, balanced blood product replacement, continuous hemodynamic monitoring, urgent interventions for source control (medical, or surgical), Monitoring and Management of Compartment Syndrome , specialized pharmacotherapy (e.g., tranexamic acid, uterotonics), and management of potential complications such as coagulopathy, ARDS, or AKI (Strong recommendation, moderate-quality evidence). Life-threatening crush injuries, particularly those leading to or at high risk of Crush Syndrome or severe Compartment Syndrome, are medical emergencies with significant morbidity and mortality. Crush Syndrome is a systemic manifestation of muscle cell damage resulting from prolonged pressure, leading to rhabdomyolysis (release of myoglobin, potassium, phosphate, uric acid), which can cause:
Compartment syndrome, if not promptly treated by fasciotomy, leads to irreversible muscle and nerve damage and can contribute to systemic complications. ICU admission is crucial for such patients due to the need for:
|
33, 188, 189, 190, 191, 192, 193, 194, 195, 196, 197, 198, 199 |
|
We recommend that all patients presenting with life-threatening gunshot wounds or blast injuries, characterized by hemodynamic instability, significant hemorrhage requiring or likely to require massive transfusion, compromised airway or breathing, severe traumatic brain injury (GCS ≤ 8), or evidence of significant penetrating or multi-system trauma, be promptly admitted to an Intensive Care Unit (ICU), ideally within a designated trauma center equipped for comprehensive trauma and critical care. Given the complexity and need for coordinated, multidisciplinary expert care (trauma surgery, critical care, neurosurgery, orthopedic surgery, anesthesia, interventional radiology), we suggest their care be managed within a ICU model, characterized by the intensivist and trauma surgeon having a primary or mandatory and active co-management role (Strong recommendation, moderate-quality evidence). life-threatening gunshot wounds and blast injuries represent severe forms of trauma, often resulting in polytrauma with complex injury patterns and a high risk of mortality and significant morbidity. ICU admission is critical for these patients due to:
|
33, 165, 176, 178, 179, 181, 182, 183, 184, 186, 200, 201 |
|
Pulmonary System |
|
|
We recommend
that adult patients presenting with acute respiratory failure, defined by
severe hypoxemia (PaO2/FiO2 ratio < 100), hypercapnia (PaCO2 > 50 mmHg
with pH < 7.35), or the need for non-invasive or invasive mechanical
ventilation, be promptly admitted to an Intensive Care Unit (ICU) or an intermediate
care unit (IMCU) with equivalent capabilities. This is to facilitate advanced
respiratory support (including mechanical ventilation and lung-protective
strategies when indicated), continuous respiratory and hemodynamic
monitoring, management of the underlying cause of respiratory failure, and
treatment of potential complications (Strong recommendation, high-quality
evidence). ICU admission is crucial for patients with ARF due to:
|
33, 225, 226, 227, 228, 229, 230, 231, 232, 233, 234, 235 |
|
We recommend that adult patients presenting with acute pulmonary embolism be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities if they are classified as high-risk (i.e., presenting with hemodynamic instability/shock) or intermediate-high risk (i.e., hemodynamically stable but with evidence of both right ventricular dysfunction and myocardial injury). This is to facilitate immediate hemodynamic and respiratory support, administration and monitoring of reperfusion therapies (e.g., thrombolysis), close observation for clinical deterioration allowing for timely rescue interventions, and management of potential complications (Strong recommendation, moderate-quality evidence). Not all patients with acute PE require ICU admission. The decision is critically dependent on risk stratification, which primarily assesses the short-term risk of death or hemodynamic decompensation. This is based on hemodynamic stability, markers of right ventricular (RV) dysfunction, and myocardial injury. Admission to an ICU/IMCU is crucial for:
|
33, 236, 237, 238, 239 |
|
We recommend that patients presenting with life-threatening hemoptysis – characterized by airway compromise, hemodynamic instability, significant respiratory failure, or bleeding volume/rate considered to be high risk – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate immediate airway management, resuscitation, continuous cardiorespiratory monitoring, and urgent diagnostic and therapeutic interventions, most notably bronchoscopy and bronchial artery embolization (BAE), in a coordinated, multidisciplinary fashion involving intensivists, pulmonologists, interventional radiologists, and thoracic surgeons (Strong recommendation, moderate-quality evidence). Life-threatening hemoptysis (often also termed "massive hemoptysis") is a medical emergency with high mortality. While definitions vary regarding the volume of expectorated blood (e.g., >100-600 mL/24h), a more clinically relevant definition focuses on any amount of bleeding that causes physiological compromise. The primary cause of death is asphyxiation from blood filling the airways, rather than exsanguination from blood loss. Admission to an ICU is crucial for patients with life-threatening hemoptysis due to the need for:
|
33, 240, 241, 242, 243, 244, 245 |
|
We recommend that all patients who have been treated for a tension pneumothorax be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This admission is essential for ongoing hemodynamic resuscitation and support, management of respiratory failure (often with mechanical ventilation), monitoring and management of the chest drain and any persistent air leak, observation for complications such as re-expansion pulmonary edema, and diagnosis and treatment of the underlying precipitating cause (Strong recommendation, moderate-quality evidence). A tension pneumothorax is an immediate, life-threatening emergency where air progressively accumulates in the pleural space, causing complete lung collapse, mediastinal shift, and compression of the great vessels. This leads to acute respiratory failure and obstructive shock, which can rapidly progress to cardiac arrest. While the immediate life-saving intervention is rapid decompression (via needle thoracostomy followed by definitive tube thoracostomy/chest drain), subsequent admission to an ICU or Intermediate Care Unit (IMCU) is crucial. The initial event is a sign of severe underlying injury or pathology, and these patients remain critically ill. ICU admission is necessary for:
|
33, 246, 247, 248, 249, 250, 251 |
|
We recommend that adult patients presenting with a massive pleural effusion that causes acute respiratory failure (characterized by severe dyspnea, increased work of breathing, or hypoxemia) or hemodynamic compromise be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to treating underlying cause pleural effusion also facilitate treating urgent, controlled therapeutic drainage, provide advanced respiratory and hemodynamic support as needed, allow for intensive monitoring for and management of potential complications (especially re-expansion pulmonary edema), and to diagnose and manage the severe underlying cause of the effusion (Strong recommendation, moderate-quality evidence). A massive pleural effusion is typically defined radiologically as opacification of most or all of a hemithorax, often with contralateral mediastinal shift. While the underlying cause can vary (e.g., malignancy, infection/empyema, heart failure, trauma/hemothorax, liver cirrhosis), the need for ICU admission is not determined by the effusion itself, but by its acute physiological consequences or the severity of the underlying illness. ICU or Intermediate Care Unit (IMCU) admission is crucial for patients with a massive pleural effusion who present with:
|
33, 253, 254, 255, 256, 257, 258, 259, 260, 261, 262 |
|
We recommend that adult patients presenting with a severe or life-threatening exacerbation of asthma or COPD be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Indications for this level of care include acute respiratory failure requiring non-invasive or invasive mechanical ventilation, severe dyspnea with signs of respiratory muscle fatigue, altered mental status, persistent or worsening hypoxemia, or severe/worsening respiratory acidosis despite initial therapy. This is to facilitate advanced respiratory support, continuous cardiorespiratory monitoring, intensive pharmacotherapy, and management of potential complications (Strong recommendation, moderate-to-high quality evidence). While most exacerbations of asthma and COPD are managed in outpatient or general ward settings, severe exacerbations can lead to life-threatening acute respiratory failure. Admission to an ICU or an intermediate (IMCU) is crucial for patients with signs of severe distress or impending respiratory arrest. For Severe Asthma Exacerbation (Status Asthmaticus), ICU admission is indicated for:
For Severe COPD Exacerbation, ICU admission is indicated for:
|
33, 263, 264, 265, 265, 266, 267, 268, 269, 270 |
|
We recommend that adult patients presenting with undifferentiated dyspnea accompanied by warning signs of physiological instability – characterized by severe respiratory distress (e.g., high respiratory rate, accessory muscle use, inability to speak), hypoxemia (e.g., SpO2 <90% on significant oxygen support), hemodynamic compromise (e.g., shock, hypotension), or altered mental status – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate cardiorespiratory stabilization and life support (including non-invasive or invasive mechanical ventilation), continuous intensive monitoring, and a rapid, concurrent diagnostic evaluation to identify and treat the underlying cause (Strong recommendation, moderate-quality evidence). "Undifferentiated dyspnea" refers to severe shortness of breath where the underlying cause is not immediately clear. When accompanied by "warning vital signs" or other objective signs of severe distress, it represents a state of active or impending cardiorespiratory collapse and is a medical emergency. The need for ICU admission is not driven by the specific diagnosis (which is unknown) but by the severity of the physiological derangement, which requires immediate stabilization, intensive monitoring, and rapid diagnostic evaluation. Warning Vital Signs and Clinical Features Indicating Need for ICU: These include, but are not limited to:
ICU admission is crucial for:
|
33, 271, 272, 273 |
|
Neurologic Disorders |
|
|
We recommend that all patients presenting in a coma (defined as a Glasgow Coma Scale [GCS] score of ≤ 8) of a known or suspected metabolic, toxic, or anoxic etiology be promptly admitted to an Intensive Care Unit (ICU). This is to facilitate immediate airway management (endotracheal intubation and mechanical ventilation), continuous cardiorespiratory and neurological monitoring, rapid diagnostic evaluation to determine the specific cause, and administration of specific treatments (e.g., targeted temperature management, metabolic correction, antidotes, enhanced elimination techniques) and comprehensive organ support. Given the complexity and need for multidisciplinary expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with relevant specialists (e.g., neurology, toxicology, endocrinology) (Strong recommendation, moderate-quality evidence). Coma, a state of unarousable unresponsiveness, is a medical emergency regardless of its cause. The primary and most immediate life-threat for any comatose patient is the loss of airway protective reflexes, leading to a high risk of airway obstruction, aspiration of gastric contents, and respiratory arrest. Therefore, admission to an ICU is essential for all patients in a coma to provide:
|
33, 274, 275, 276, 277, 278, 279, 285 |
|
We recommend that adult patients presenting with acute neurological deficits accompanied by an impaired level of consciousness (Glasgow Coma Scale score <15, and especially ≤ 8) be promptly admitted to an Intensive Care Unit (ICU) or a Comprehensive Stroke/neuro Unit with equivalent ICU capabilities. This is to facilitate immediate airway management if necessary, intensive neurological and hemodynamic monitoring, management of intracranial pressure and cerebral edema, and post-procedure care, and management of systemic complications (Strong recommendation, low-quality evidence). |
33, 280, 281, 282, 283, 284, 285 |
|
We recommend that adult patients presenting with a severe acute cerebral vascular stroke (ischemic or hemorrhagic:- ( intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH))be promptly admitted to an Intensive Care Unit (ICU), preferably a specialized Neuro-ICU, or a Comprehensive Stroke Unit with equivalent ICU capabilities. Indications for this level of care include, but are not limited to, an impaired level of consciousness (Glasgow Coma Scale [GCS] score ≤ 8), signs of intracranial hypertension or impending herniation, the need for mechanical ventilation, hemodynamic instability, ongoing management of therapies such as intravenous thrombolysis or post-mechanical thrombectomy care, or management of severe complications such as large or expanding hematomas, intraventricular hemorrhage, or aneurysmal subarachnoid hemorrhage (Strong recommendation, moderate-quality evidence). While not all stroke patients require ICU admission (many are managed in dedicated Stroke Units), those with severe strokes or life-threatening complications need the level of monitoring and intervention that only an ICU can provide. The specific indications vary slightly between ischemic and hemorrhagic stroke, but the overarching need is driven by actual or potential neurological and systemic decompensation. ICU admission is crucial for:
|
33, 280, 281, 282, 285, 286, 287, 288, 289 , 290, 291 |
|
We recommend that adult patients presenting with an acute focal neurological deficit who also exhibit signs of critical illness – characterized by an impaired level of consciousness (Glasgow Coma Scale score ≤ 13), acute respiratory failure requiring advanced support, hemodynamic instability, signs of increased intracranial pressure or impending herniation, or status epilepticus – be promptly admitted to an Intensive Care Unit (ICU), preferably a specialized Neuro-ICU or a Comprehensive Stroke Unit with equivalent ICU capabilities. This is to facilitate immediate airway management, continuous neurological and hemodynamic monitoring, aggressive management of intracranial pressure and other neurological complications, and rapid investigation and treatment of the underlying life-threatening cause (Strong recommendation, moderate-quality evidence). ICU admission is not indicated for the focal deficit itself, but for the severity of the underlying cause or for associated life-threatening complications. Therefore, this response focuses on patients presenting with an AFND who also have signs of critical illness requiring ICU-level care. Patients with an AFND require ICU admission when the underlying condition leads to or poses an immediate risk of:
|
33, 280, 281, 282, 285, 288, 289, 290, 292, 293, 294 |
|
We recommend that adult patients with Myasthenic Crisis (defined by respiratory failure secondary to myasthenia gravis) and those with severe Guillain-Barré Syndrome (GBS) – characterized by rapid progression of weakness, evidence of respiratory muscle compromise (e.g., vital capacity <20 mL/kg), significant bulbar dysfunction, or severe autonomic instability – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate intensive cardiorespiratory monitoring, timely non-invasive or invasive mechanical ventilation, management of autonomic dysfunction, administration of specific immunotherapies, and comprehensive supportive care. Given the need for specialized neurological and critical care expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with neurology specialists(Strong recommendation, moderate-quality evidence). Both Myasthenic Crisis and severe Guillain-Barré Syndrome are acute neuromuscular emergencies where the primary life-threat is acute respiratory failure due to weakness of the respiratory muscles (diaphragm and intercostal muscles). ICU admission is crucial for:
|
33, 295, 296, 297, 298, 299, 300, 301, 302, 303, 304, 305 |
|
We recommend that adult patients presenting with neurological infections such as:- meningitis, who also exhibit signs of severe neurological compromise (e.g., altered mental status with a Glasgow Coma Scale [GCS] score ≤ 11, and particularly ≤ 8) or significant systemic organ dysfunction (e.g., respiratory compromise requiring advanced airway or ventilatory support, or hemodynamic instability/septic shock) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This is to facilitate immediate airway management, intensive neurological and hemodynamic monitoring (including management of intracranial pressure), rapid administration of appropriate antimicrobial and adjunctive therapies, and comprehensive management of seizures, shock, and multi-organ failure (Strong recommendation, high-quality evidence).
Meningitis, particularly acute bacterial meningitis, can be a rapidly progressive and life-threatening infection. While uncomplicated cases may be managed on a general ward, admission to an ICU is crucial when patients develop severe complications. The primary drivers for ICU admission are:
|
33, 285, 292, 306, 307, 308, 309, 310, 311, 312, 313, 314, 315, 316, 317 |
|
We recommend that all adult patients with established convulsive status epilepticus (defined as continuous seizure activity >5 minutes or ≥2 discrete seizures without recovery of consciousness between them) or uncontrolled convulsions be promptly admitted to an Intensive Care Unit (ICU) or specialized Neuro-ICU or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management . This admission is essential to facilitate aggressive, stepwise anticonvulsant therapy (including potential administration of continuous anesthetic infusions for refractory cases), secure and manage the airway (often with mechanical ventilation), provide continuous electroencephalography (cEEG) and hemodynamic monitoring, and manage life-threatening systemic complications. Given the need for specialized neurological and critical care expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with neurology/epileptology specialists (Strong recommendation, high-quality evidence). Status Epilepticus (SE) is a neurological emergency defined as a continuous seizure lasting longer than 5 minutes, or two or more seizures without a full recovery of consciousness in between. "Uncontrolled convulsions" are functionally equivalent to convulsive status epilepticus. SE is associated with significant morbidity (including permanent neuronal injury) and mortality. ICU admission is critical for patients with established or refractory SE due to the need for:
|
33, 285, 318, 319, 320, 321, 322, 323, 324, 325, 326, 327, 328, 329 |
|
Surgical and postoperative |
|
|
We recommend that adult surgical patients be admitted to an Intensive Care Unit (ICU) or any specialized ICU or with equivalent capabilities for comprehensive critical care management if they meet one or more of the following criteria: (1) they have undergone a high-risk surgical procedure known to require intensive monitoring and support post-operatively (e.g., major cardiac, thoracic, aortic, neurological, vascular, abdominal, or transplant surgery); (2) they have severe pre-existing comorbidities that significantly impair their physiological reserve to withstand major surgery; or (3) they exhibit evidence of acute organ dysfunction or hemodynamic instability in the immediate postoperative period (e.g., need for mechanical ventilation, vasopressor support, or ongoing massive transfusion). This is to facilitate advanced organ support, continuous cardiorespiratory and neurological monitoring, management of major fluid shifts and bleeding, advanced pain control, and early detection and management of life-threatening postoperative complications (Strong recommendation, high-quality evidence). Admission to an ICU is not required for all surgical patients. It is reserved for a high-risk population whose physiological reserve is, or is expected to be, overwhelmed by the combined stress of their underlying disease, comorbidities, and the surgical procedure itself. The decision is based on a combination of pre-operative patient factors, the nature of the surgery, and the patient's immediate postoperative physiological state. ICU admission is crucial for:
|
1, 33, 168, 330, 331, 332, 333, 334, 335, 336, 353 |
|
We suggest that surgical patients who are hemodynamically stable at the conclusion of surgery, successfully extubated, and require only enhanced monitoring (e.g., continuous electrocardiography, invasive arterial pressure monitoring) or low-level therapeutic support (e.g., non-invasive ventilation, single low-dose vasopressor) may be admitted to a designated Intermediate Care Unit (IMCU) with appropriate nurse-to-patient ratios and protocols for rapid escalation of care if needed. This strategy can optimize critical care resource allocation without compromising patient safety. (Good practice statement, moderate -quality evidence). |
12, 13, 14, 15, 33, 330, 390 |
|
Renal disorders |
|
|
We recommend that adult patients with acute kidney injury (AKI) who require urgent renal replacement therapy be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate the safe initiation and management of renal replacement therapy (including continuous modalities like Continuous Renal Replacement Therapy for hemodynamically unstable patients), provide continuous monitoring for and treatment of life-threatening electrolyte and acid-base disturbances, and deliver comprehensive organ support for the underlying critical illness that precipitated the AKI such as:(CKD, sepsis, shock, tumor lysis syndrome or rhabdomyolysis etc.) (Strong recommendation, moderate-to-high quality evidence). AKI signifies that the kidney failure has led to life-threatening metabolic or fluid balance derangements that are refractory to medical management. The indications for urgent urgent renal replacement therapy are themselves critical conditions requiring an ICU level of care. Furthermore, the initiation of renal replacement therapy, especially intermittent hemodialysis, in a physiologically unstable patient can cause hemodynamic compromise and requires intensive monitoring. ICU admission is crucial for:
|
33, 237, 238, 239, 240, 241, 242, 243, 344, 349 |
|
We recommend that adult patients presenting with a severe acid-base disorder – characterized by extreme derangement in arterial pH (e.g., acidemia with pH < 7.20 or alkalemia with pH > 7.55) or a less extreme derangement accompanied by evidence of significant organ dysfunction (e.g., shock, altered mental status, respiratory failure) – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate continuous cardiorespiratory and neurological monitoring, aggressive management of the underlying cause, advanced respiratory and hemodynamic support as needed, and frequent biochemical monitoring to guide therapy (Strong recommendation, moderate-quality evidence). A severe acid-base disorder is a life-threatening condition where the blood pH moves to extreme levels, causing profound dysfunction of multiple organ systems. It is not a standalone diagnosis but rather a manifestation of a critical underlying illness (e.g., shock, sepsis, respiratory failure, renal failure, diabetic ketoacidosis, poisoning). The need for ICU admission is driven by the direct physiological consequences of the pH derangement and the intensity of care required to manage both the acid-base disorder and its underlying cause. ICU admission is crucial for managing:
|
33, 337, 344, 345, 346, 347, 348, 349, 350, 351 |
|
We recommend that adult patients presenting with severe hyperkalemia (e.g., serum K+ > 6.0-6.5 mmol/L) that is accompanied by any new ECG changes attributable to hyperkalemia, or that is refractory to initial medical therapies, be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU)/High-Dependency Unit (HDU) with continuous cardiac monitoring capabilities. This is to facilitate immediate and ongoing cardiac monitoring, administration of emergency medical therapies, urgent initiation of renal replacement therapy (dialysis) for definitive potassium removal, frequent laboratory monitoring, and management of the underlying cause (Strong recommendation, moderate-quality evidence). Severe hyperkalemia (generally defined as serum potassium [K+] > 6.0-6.5 mmol/L) is life-threatening primarily due to its effects on cardiac myocyte membrane potential, leading to lethal cardiac arrhythmias. The presence of ECG changes (from peaked T waves to QRS widening, sine wave pattern, and ultimately ventricular fibrillation or asystole) signifies significant cardiotoxicity. When this condition is refractory to initial medical therapies (e.g., calcium for membrane stabilization, insulin/dextrose and beta-agonists to shift potassium intracellularly), the patient is at immediate risk of cardiac arrest. ICU admission is crucial for:
|
33, 337, 350, 351, 352, 353, 354, 355, 356 |
|
We recommend that adult patients presenting with significant volume overload causing acute pulmonary edema and respiratory distress (characterized by severe dyspnea, increased work of breathing, and/or hypoxemia) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate advanced respiratory support (most notably non-invasive ventilation), aggressive and monitored fluid removal with intravenous diuretics or renal replacement therapy, administration of vasoactive medications as needed, and continuous cardiorespiratory monitoring (Strong recommendation, low-quality evidence). Significant volume overload becomes life-threatening when it leads to acute pulmonary edema (the accumulation of fluid in the lung's interstitial and alveolar spaces), causing severe gas exchange abnormalities and acute hypoxemic respiratory failure. This is a medical emergency regardless of the underlying cause (e.g., acute decompensated heart failure [ADHF], acute kidney injury [AKI] with anuria, iatrogenic fluid overload). Admission to an ICU or Intermediate Care Unit (IMCU) is crucial for:
|
33, 337, 357, 358 |
|
We recommend that adult patients with uremic pericarditis who present with cardiac tamponade or evidence of significant hemodynamic compromise (e.g., hypotension, shock) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate urgent pericardiocentesis or surgical drainage, safe initiation and management of intensive renal replacement therapy (dialysis) in an unstable patient, continuous cardiorespiratory and hemodynamic monitoring, and comprehensive management of the underlying severe renal failure (Strong recommendation, moderate-quality evidence). Uremic pericarditis is inflammation of the pericardium in patients with severe acute or end-stage kidney disease. While uncomplicated uremic pericarditis can sometimes be managed on a specialized nephrology ward with intensive dialysis, admission to an ICU becomes necessary when life-threatening complications arise. ICU care is crucial for:
|
33, 337, 359, 360, 361, 362 |
|
We recommend that adult patients diagnosed with Hepatorenal Syndrome-Acute Kidney Injury (HRS-AKI) be promptly admitted to an Intensive Care Unit (ICU), preferably one with expertise in hepatology and liver transplantation. This is to facilitate the administration and intensive monitoring of vasoconstrictor and albumin therapy, aggressive management of hemodynamic instability and other complications of decompensated cirrhosis (e.g., hepatic encephalopathy, bleeding), delivery of renal replacement therapy if indicated, and comprehensive multi-organ support as a bridge to potential liver transplantation (Strong recommendation, moderate-quality evidence). |
337, 363, 364, 365, 366, 367, 368, 369 |
|
Drug Ingestion, Drug Overdose, & sever Drug reaction |
|
|
We recommend that patients presenting with a known or suspected drug ingestion who exhibit signs of life-threatening toxicity – characterized by altered mental status with inadequate airway protection (e.g., Glasgow Coma Scale score ≤ 8), hemodynamic instability (e.g., shock, life-threatening arrhythmias, severe hypertension), respiratory failure requiring advanced support, ongoing seizures, or severe metabolic/laboratory abnormalities – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate life support (airway, breathing, circulation), continuous cardiorespiratory and neurological monitoring, administration of antidotes, consideration of enhanced elimination techniques (e.g., hemodialysis), and management of multi-organ complications (Strong recommendation, moderate-quality evidence). The primary principle of managing severe poisoning is aggressive supportive care, alongside specific antidotes and enhanced elimination techniques where indicated. ICU admission is crucial for:
|
33, 353, 370, 371, 372, 373, 374, 375, 376, |
|
Miscellaneous |
|
|
We recommend that all adult patients presenting with septic shock (defined by persisting hypotension requiring vasopressors to maintain MAP ≥65 mmHg and serum lactate >2 mmol/L despite adequate volume resuscitation) and patients with sepsis accompanied by significant hemodynamic instability (e.g., hypotension responsive only to ongoing aggressive fluid resuscitation, or other signs of organ hypoperfusion such as persistently elevated lactate despite initial fluids) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This admission is essential to facilitate timely implementation of sepsis management bundles, including rapid administration of appropriate antimicrobials, aggressive hemodynamic resuscitation with fluids and vasoactive agents, source control measures, potential advanced respiratory support, and continuous monitoring and management of organ dysfunction (Strong recommendation, moderate-quality evidence). ICU admission is crucial for these patients due to the need for:
|
1, 33, 104, 202, 203, 204, 205, 353 |
|
We recommend that adult patients presenting with life-threatening environmental injuries – specifically heat stroke (core temperature >40°C with CNS dysfunction), severe complications of drowning (e.g., significant hypoxemia, ARDS, altered mental status), severe hypothermia (core temperature <32°C with cardiovascular instability or coma), severe environmentally-induced hyperthermia with organ dysfunction, severe altitude illness (High Altitude Cerebral Edema [HACE] or High Altitude Pulmonary Edema [HAPE] with respiratory failure or coma), severe barotrauma (especially pulmonary barotrauma with Arterial Gas Embolism [AGE]), or severe Decompression Sickness (Type II DCS with neurological or cardiorespiratory compromise) – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This is to facilitate aggressive specific therapies (e.g., rapid cooling/rewarming, hyperbaric oxygen coordination, specific pharmacotherapies), advanced respiratory and hemodynamic support, continuous multi-organ monitoring, and management of potential complications we suggest their care be managed within ICU model, characterized by the intensivist having a primary or mandatory and active co-management role in conjunction with relevant specialists (Strong recommendation, moderate-quality evidence). patients with life-threatening Environmental Injuries – specifically Heat Stroke, severe complications of Drowning, severe Hypo/Hyperthermia, severe Altitude Illness (HACE/HAPE), severe Barotrauma (especially with Arterial Gas Embolism), and severe Decompression Sickness These conditions, when severe, are medical emergencies associated with high risk of multi-organ dysfunction and mortality. ICU admission is crucial for intensive monitoring, aggressive supportive care, and specific interventions.
|
33, 206, 207, 208, 209, 210, 211, 212, 213, 214, 215, 353 |
|
We recommend that adult patients presenting with signs of severe systemic envenomation from a snakebite or scorpion sting be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. Signs of severe envenomation requiring such admission include, but are not limited to: respiratory failure or compromise (e.g., neurotoxic paralysis, pulmonary edema), hemodynamic instability (e.g., shock, severe hypertension), venom-induced consumptive coagulopathy with active bleeding, significant neurological impairment (e.g., altered mental status, seizures), or evidence of severe end-organ damage such as acute kidney injury or severe rhabdomyolysis. This is to facilitate timely administration and monitoring of antivenom (including management of adverse reactions), advanced respiratory and hemodynamic support, management of coagulopathy, and comprehensive multi-organ supportive care (Strong recommendation, moderate-quality evidence). While many snakebites and scorpion stings cause only local effects, a significant number, depending on the species and venom dose, can cause severe, life-threatening systemic toxicity requiring ICU admission. The specific indications vary between snake and scorpion envenomation due to different venom pathophysiologies. For Snake Envenomation, ICU admission is crucial for managing:
For Scorpion Envenomation, ICU admission is crucial for managing:
|
33, 216, 217, 218, 219, 220, 221, 222, 223, 224, 353 |
|
Parameter criteria |
|
|
Vital Signs |
|
|
We recommend that adult patients presenting with warning vital signs indicating acute or impending critical illness be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such warning signs include, but are not limited to, evidence of a compromised airway; severe respiratory distress (e.g., respiratory rate >30 or <10 breaths/min, SpO2 <90% on significant oxygen support); hemodynamic instability (e.g., HR <40 or >130, shock with Systolic arterial pressure ≤ 90 mm Hg or ≥ 160 mmHg or requiring vasopressors) (Mean arterial pressure ≤ 60 mm Hg or Diastolic arterial pressure > 110 mmHg ). ; life-threatening arrhythmias; or a new, significant alteration in level of consciousness (e.g., GCS drop, new-onset coma). This is to facilitate continuous cardiorespiratory and neurological monitoring, immediate life support, and a rapid, concurrent diagnostic evaluation to identify and treat the underlying cause (Strong recommendation, moderate-quality evidence). ICU admission is often triggered not by a specific diagnosis, but by the degree of physiological derangement, which is directly measured by vital signs. "Warning vital signs" are objective indicators of actual or impending organ failure and a high risk of deterioration or cardiac arrest. The key vital signs and their "warning" thresholds that often necessitate ICU/IMCU admission include:
ICU admission is crucial for these patients for continuous cardiorespiratory monitoring, immediate life support (e.g., mechanical ventilation, vasopressors), and rapid diagnostic investigation to identify and treat the underlying cause. |
16, 32, 33, 35, 417 |
|
We recommend that adult patients with a persistent core body temperature of < 36°C (hypothermia) or > 39°C (high fever), particularly when associated with other signs of organ dysfunction (e.g., hemodynamic instability, respiratory distress, altered mental status) or a high clinical suspicion of severe infection/sepsis, be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate aggressive investigation and treatment of the underlying cause, continuous cardiorespiratory monitoring, management of the systemic effects of the temperature derangement, and comprehensive organ support (Strong recommendation, low-quality evidence). A persistent and severe abnormality in body temperature is rarely an isolated finding. It is a cardinal vital sign and a key indicator of a significant underlying systemic process, most commonly sepsis. It can also be caused by severe environmental injuries, central nervous system catastrophe, or severe endocrine emergencies. The decision for ICU admission is driven by the fact that the temperature derangement signifies a critical illness that requires intensive monitoring and management of its cause and consequences. ICU admission is crucial for managing:
o Sepsis and Septic Shock: This is the most common cause. A temperature <36°C (hypothermia) or >38.3°C (fever) is part of the diagnostic criteria for Systemic Inflammatory Response Syndrome (SIRS), a component of older sepsis definitions. Hypothermia in sepsis is often a marker of severe illness and poor prognosis. Management requires aggressive resuscitation, antibiotics, source control, and organ support in an ICU. o Severe Environmental Injuries: As detailed previously, heat stroke or severe accidental hypothermia requires specialized temperature management and multi-organ support in an ICU. o Central Nervous System Emergencies: Brain injury (traumatic or stroke) can disrupt thermoregulation, and fever in this context can worsen secondary brain injury, requiring aggressive temperature control in a Neuro-ICU.
|
33, 377, 378, 379, 380, 381 |
|
respiratory Parameter |
|
|
We recommend that adult patients presenting with severe derangements in respiratory parameters indicating acute or impending respiratory failure be promptly admitted to an Intensive Care Unit (ICU) or or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Indications for this level of care include, but are not limited to: clinical signs of severe respiratory distress (e.g., Respiratory rate >30 breaths/min tachypnea or < 10 breaths /min, use of accessory muscles, inability to speak); evidence of severe gas exchange abnormalities (e.g., PaO2/FiO2 ratio <200 SpO2 < 92 % on room air, or SpO2 <90% on high-flow oxygen; acute hypercapnia with respiratory acidosis [pH <7.30]); or evidence of respiratory muscle weakness indicating impending respiratory arrest (e.g., vital capacity <20 mL/kg). This is to facilitate advanced respiratory support (including non-invasive or invasive mechanical ventilation), continuous cardiorespiratory monitoring, management of the underlying cause, and treatment of potential complications (Strong recommendation, moderate-to-high quality evidence). The key respiratory parameters indicating a need for ICU-level care fall into three main categories:
|
33, 225, 226, 227, 228, 229, 230, 231, 263, 264, 361 |
|
Radiography/Ultrasonography/Tomography |
|
|
We recommend that adult patients whose imaging studies (radiography, ultrasonography, or tomography) reveal a critical finding be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such critical findings include, but are not limited to, those indicating acute respiratory failure (e.g., diffuse bilateral opacities consistent with moderate/severe ARDS), obstructive shock (e.g., cardiac tamponade, massive pulmonary embolism with right ventricular strain, tension pneumothorax), catastrophic vascular events (e.g., acute aortic dissection, ruptured aneurysm), severe neurological compromise (e.g., large intracranial hemorrhage or infarct with mass effect, Cerebral vascular hemorrhage, contusion, subarachnoid haemorrhage, or sever spine injury), or major visceral injury (e.g., perforated viscus, severe solid organ injury with hemorrhage). This is to facilitate immediate life support, intensive monitoring for deterioration, management of organ dysfunction, and timely therapeutic interventions (surgical, radiological, or medical) (Strong recommendation, moderate-quality evidence). A patient with a critical imaging finding is admitted to the ICU to:
Warning Imaging Findings Often Requiring ICU Admission (such as): 1. Chest Imaging (CXR, CT, Ultrasound):
2. Head Imaging (CT, MRI):
3. Abdominal Imaging (CT, Ultrasound):
|
33, 165, 168, 194, 195, 196, 170, 171, 172, 173, 174, 175, 382, 383, 384 |
|
abnormalities in blood indices |
|
|
We recommend that adult patients presenting with critical abnormalities in blood indices that signify or pose an immediate risk of life-threatening organ dysfunction, hemorrhage, or severe systemic illness. T be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such critical findings include, but are not limited to, evidence; severe anemia (Hb < 7 gm % ) causing hemodynamic instability or myocardial ischemia or resulting from massive hemorrhage. severe coagulopathy (INR (>5-6)) or severe thrombocytopenia (< 20000/ mm3) with bleeding (e.g., DIC, Thrombotic Thrombocytopenic Purpura (TTP), or HELLP syndrome.) with active bleeding or Severe Leukopenia / severe neutropenia with sepsis or shock or Hyperleukocytosis/Leukostasis (>100,000/µL) leading to respiratory failure or stroke. This is to facilitate aggressive resuscitation (including massive transfusion), continuous monitoring, treatment of the underlying cause, management of organ failure, and reversal or control of the hematologic or biochemical derangement (Strong recommendation, moderate-quality evidence)
ICU admission is crucial for patients with severe abnormalities in blood indices to:
Key Blood Indices and Associated Critical Conditions Requiring ICU Admission: 1. Hematology (Complete Blood Count):
2. Coagulation:
|
33, 385, 386, 387,388 |
|
Laboratory Values (critical biochemical indices) |
|
|
We recommend that adult patients presenting with a severe electrolyte disturbance – characterized by an extreme laboratory value posing immediate risk (e.g., K+ >6.5 mmol/L, K+ <2.5 mmol/L, Na+ <120 mmol/L, Na+ >160 mmol/L, elevated serum lactate (e.g., >2-4 mmol/L) Serum calcium > 12 mg /dL or < 6 mg /d with manifestations, severe symptomatic abnormalities of magnesium, or phosphate) or by life-threatening clinical manifestations such as cardiac arrhythmias, tissue hypoperfusion ,seizures, coma, or respiratory muscle failure – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate continuous cardiac and neurological monitoring, frequent laboratory testing, controlled intravenous administration of corrective therapies, management of organ dysfunction, and treatment of the underlying cause (Strong recommendation, moderate-quality evidence). A severe electrolyte disturbance is a life-threatening condition where the concentration of one or more electrolytes in the blood is abnormal to a degree that causes or poses an immediate risk of severe organ dysfunction. Admission to an ICU or intermediate care unit (IMCU) is crucial because these conditions can lead to:
ICU care is essential for:
|
33, 344, 344, 345, 346, 347, 348, 349, 350, 351, 352, 353, 354, 355, 356, 375 |
|
We recommend that adult patients presenting with a life-threatening glycemic crisis be promptly admitted to an Intensive Care Unit (ICU) or or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This includes patients with: (1) severe hypoglycemia (e.g., blood glucose <65 mg/dL or 3.6 mmol/L) causing significant neurological impairment (e.g., coma, seizures) or requiring a continuous intravenous glucose infusion for stabilization; and (2) severe hyperglycemia (e.g., blood glucose >750 mg/dL or 41.6 mmol/L) consistent with severe Diabetic Ketoacidosis (DKA) or Hyperosmolar Hyperglycemic State (HHS). This admission is to facilitate intensive monitoring of neurological, metabolic, and hemodynamic status; aggressive and controlled intravenous fluid, electrolyte, and insulin/glucose therapy; and management of underlying causes and systemic complications (Strong recommendation, moderate-quality evidence). While a glucose of <70 mg/dL is the alert value, and <65 mg/dL is clinically significant, ICU admission is reserved for life-threatening hypoglycemia. This is characterized by severe neuroglycopenia (brain dysfunction due to glucose deprivation) or a situation where prolonged or recurrent hypoglycemia is highly likely. ICU care is crucial for:
|
33, 111, 112, 113, 114, 115, 116, 132, 133, 134, 135, 136, 137, 138, 392, 393, 394, 395 |
|
Addmsion & Triage of mass casualty incidents , Pandemic and Epidemic |
|
|
We recommend that intensive care units be prepared to handle victims of external and internal disasters, including the collapse of surrounding services due to natural or man-made disasters. Every intensive care unit should have general disaster and evacuation plans within the hospital's plans. (Strong recommendation, moderate -quality evidence). |
1, 33, 188, 189, 190, 396, 398 ,399, 401 |
|
We recommend that the declaration of a Mass Casualty Incident (MCI) be followed by the immediate activation of the institutional disaster plan and a coordinated response from the complete healthcare team. This team must ensure the readiness of the institution and its critical care areas—notably the Emergency Department, operating rooms, and the ICU—to efficiently transition from routine to emergency operations and to augment their capacity for a significant influx of critically ill patients. (Strong recommendation, moderate -quality evidence). |
1, 33, 188, 189, 190, 396, 397, 398, 399, 400, 401, 402 |
|
We suggest at Mass Casualty Incident (MCI) that the emergncy and inetnsive care physicians identify all patients in need of ICU care and those already hospitalized who could be discharged, and then triage and transfer the incoming patients to the most appropriate setting as soon as possible (Strong recommendation, moderate -quality evidence). |
1, 33, 188, 189, 190, 396, 398, 402, 407, 408, 411, 412 |
|
We recommend that national and regional regulatory bodies, in collaboration with hospitals leadership, develop, fund, and regularly exercise comprehensive plans to enable a rapid and surge in intensive care capacity. These plans should aim to accommodate a significant increase over baseline ICU capacity (with models for extreme events targeting at least 300% expansion) by identifying convertible spaces, pre-allocating necessary resources (equipment, supplies, staffing protocols), and integrating flexible design considerations into healthcare building codes. Furthermore, these plans should establish a clear crisis management authority with the mandate to coordinate resources and patient flow across a region during a declared emergency (Strong recommendation, moderate-quality evidence). Major disasters (e.g., severe pandemics, mass casualty incidents from natural disasters or armed conflict) can overwhelm healthcare systems by creating a sudden, massive influx of critically ill patients. The COVID-19 pandemic provided a stark, real-world demonstration of this. A lack of preparedness leads to rationing of care, preventable morbidity and mortality, and collapse of healthcare infrastructure. Therefore, proactive planning is a cornerstone of national health security and public health preparedness. This involves a multi-pronged strategy:
|
1, 10, 33, 188, 189, 190, 397, 399, 400, 401, 403, 410, 411, 412 |
|
We suggest that during mass casualty scenarios, adult patients with severe burns—based on established clinical criteria—may be appropriately managed in general ICU settings to preserve specialized Burn ICU capacity for the most critically injured cases. This approach should be guided by well-coordinated regional and national triage systems to ensure optimal allocation of resources and timely care delivery. (Good practice statement, low-quality evidence). |
1, 33, 188, 189, 190 |
|
We recommend that national and regional regulatory bodies, in collaboration with hospitals leadership, develop, fund, and regularly exercise comprehensive plans for Pandemic & epidemics. These plans should cover national and hospital level. plans should include both triage and dissemination of patients throughout the hospital.Furthermore, these plans should establish a clear crisis management authority with the mandate to coordinate resources and patient flow across a region during a declared epidemics(Strong recommendation, moderate-quality evidence). |
1, 10, 33, 397, 399, 401, 403, 406, 409, 410 |
|
We suggest during Pandemic and Epidemic not using routine laboratory studies alone in determining the nature of illness. (Good practice statement, low-quality evidence). |
1, 36, 38, 402, 404, 405, 406, 407, 408, 414, 415, 416 |
|
We suggest during Pandemic and Epidemic not using scoring systems alone to determine level of care or removal from higher levels of care because these are not accurate in predicting individual mortality(Good practice statement, low-quality evidence). |
1, 36, 38, 402, 403, 404, 405, 406, 407, 408, 413 |
|
ICU discharge |
|
|
We recommend avoiding discharge from ICU “after hours” (“night shift”, after 7 pm in institutions with 12-hr shifts). In addition, best practice would seek to optimize evening and night coverage and services(Good practice statement, low-quality evidence). |
1, 36, 419 |
|
We suggest discharging patients at high risk for mortality and readmission (high severity of illness, multiple comorbidities, physiologic instability, and ongoing organ support) to a step-down unit intermediate care units (IMCU) then to the regular ward |
1, 27, 33, 36, 419 |
|
We recommend that the decision to discharge a patient from an Intensive Care Unit (ICU) be based on a structured, multi-domain assessment. This assessment should be guided by institutional policies that are based on a framework of objective criteria. Key domains to consider include: · the resolution of the acute life-threatening condition that prompted admission · the achievement of physiological stability · Neurological status: be adequately handled and monitored at the receiving unit · Genanral status of the patient be adequately handled and monitored at the receiving unit · able to protect their airway (unless there is a chronic baseline deficit) · Respiratory status: Stable RR 12-24 breaths / min & SpO2 ≥ 92% on room air OR patient's individual Known baseline value is met. · Cardiovascular status:stable hemodynamics, HR, BP, (OR patient's individual Known baseline value) with no arrhythmia or tolerable intermittent arrhythmia for at least 24 hr, with no signs of active bleeding or hypervolemia / hypovolemia · the absence of need for ongoing ICU-specific interventions · with adequately urine output, electrolyte level, and renal function and if need renal replacement therapy is possible outside the ICU · the patient's prognosis and goals of care · the capabilities and availability of resources at the next appropriate level of care (e.g., an intermediate care unit or general ward). This is to facilitate a safe,
timely, and appropriate transition of care that minimizes the risk of
clinical deterioration and ICU readmission (Strong recommendation,
moderate-quality evidence).
|
1, 27, 33, 419 |
|
We suggest that patients with cardiovascular disorders be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to, stable hemodynamics without the need for intravenous vasopressor or inotropic support(Systolic blood pressure ≥ 90 mmHg - Diastolic blood pressure ≥ 50 mm Hg -Heart rate > 50 beats /min. and < 130 beats/minutes) (OR patient's individual Known baseline value); stable respiratory status (OR patient's individual Known baseline value), having been weaned from invasive mechanical ventilation and requiring a low level of oxygen support manageable on a ward or IMCU (SPO2 > 92 % on room air or alternative oxygen supply < 6 L/min- Respiratory rate < 30 breaths/min and > 10 breaths /min.); and the absence of life-threatening cardiac arrhythmias or ongoing myocardial ischemia(Absence of life-threatining arrhythmia for 24 hours -No continuous antiarrhythmic or vasoactive agent) and Resolution of the Acute Insult. This is to ensure a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence).
|
1, 33 |
|
We suggest that adult patients admitted to the ICU for a pulmonary disorder be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to, successful liberation from invasive mechanical ventilation (as demonstrated by passing a spontaneous breathing trial and successful extubation or stable non-invasive positive pressure ventilation settings with plan for chronic home ventilation) ; stable and adequate gas exchange (e.g., SpO2 ≥ 92% on a low level of oxygen support [FiO2 ≤ 0.4]); absence of respiratory distress (e.g., respiratory rate <25/min, no accessory muscle use); and an effective cough with the ability to manage secretions. This is to ensure a safe transition of care and minimize the risk of respiratory decompensation and ICU readmission (Strong recommendation, moderate quality evidence). |
1, 33 |
|
We suggest that adult patients admitted to the ICU for a severe gastrointestinal disorder be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate resolution of the acute crisis and have achieved physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: cessation of life-threatening bleeding with no evidence of re-bleeding; control of intra-abdominal sepsis source; resolution of shock with discontinuation of intravenous vasopressor/inotropic support; stable respiratory status after liberation from mechanical ventilation; and improving or stable organ function. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
1, 33 |
|
We suggest that adult patients admitted to the ICU for a severe neurologic disorder be considered for discharge when they demonstrate sufficient neurological and physiological stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: a stable and protected airway (e.g., patient is successfully extubated with adequate consciousness and protective reflexes, or has a stable tracheostomy with manageable respiratory needs); controlled intracranial pressure without need for intensive medical or surgical intervention; cessation of status epilepticus with seizures controlled on a stable medication regimen; and resolution of associated hemodynamic shock and respiratory failure. This is to facilitate a safe transition of care and minimize the risk of neurological deterioration or other complications requiring ICU readmission (Strong recommendation, moderate-quality evidence). |
1, 33 |
|
We suggest that adult patients admitted to the ICU for a severe endocrine or electrolyte disorder be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: resolution of hemodynamic shock with discontinuation of intravenous vasopressor/inotropic support; neurological stability with the patient being conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit); stable respiratory function after liberation from mechanical ventilation; and correction of the life-threatening metabolic or electrolyte derangement to a safe level that can be managed with oral, subcutaneous, or intermittent intravenous therapies on a ward. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
1, 33 |
|
We suggest that adult patients admitted to the ICU for a severe renal disorder be considered for discharge when they demonstrate resolution of the acute life-threatening uremic complications and have achieved hemodynamic and respiratory stability. Key criteria for discharge readiness include, but are not limited to: correction of severe metabolic acidosis and life-threatening hyperkalemia; resolution of severe volume overload and its associated respiratory compromise; neurological stability with resolution of uremic encephalopathy; and stabilization of renal replacement therapy status (either recovery of native kidney function no longer requiring renal replacement therapy, or hemodynamic stability sufficient to transition from continuous to intermittent dialysis manageable in a non-ICU setting). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
1, 33 |
|
We recommend that adult patients admitted to the ICU for sepsis or septic shock be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: resolution of shock with discontinuation of intravenous vasopressor or inotropic support; stable respiratory status after liberation from mechanical ventilation and on minimal oxygen support; evidence of adequate source control of the infection; and a clear trajectory of improvement or stabilization of other organ dysfunctions (e.g., neurological, renal, hepatic, hematological, as may be reflected in a decreasing SOFA score). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
33, 27 |
|
We recommend that adult patients admitted to the ICU for severe trauma and injuries be considered for discharge when they demonstrate resolution of the acute life-threatening crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: control of hemorrhage with resolution of shock and discontinuation of intravenous vasopressor/inotropic support; stable respiratory status after liberation from mechanical ventilation and with a secure, protected airway; neurological stability with controlled intracranial pressure and cessation of status epilepticus; and evidence that the underlying injuries have been definitively managed or stabilized such that immediate re-operation is not anticipated. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
33, 27 |
|
We recommend that adult patients admitted to the ICU for surgical or postoperative care be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability, including neurological stability (e.g., conscious, alert, and able to protect their airway, unless there is a chronic baseline deficit), and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: control of surgical hemorrhage with no evidence of ongoing bleeding; control of any surgical sepsis source; resolution of shock with discontinuation of intravenous vasopressor or inotropic support; stable respiratory status after liberation from mechanical ventilation; and evidence of improving or stable organ function. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
33, 27 |
|
We recommend that adult patients admitted to the ICU for severe snake or scorpion envenomation be considered for discharge when they demonstrate resolution of the acute life-threatening systemic envenomation syndrome and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: for neurotoxic envenomation, recovery of respiratory muscle function with successful liberation from mechanical ventilation and a secure airway; for hemotoxic envenomation, cessation of bleeding and sustained normalization of coagulation parameters; for cardiotoxic envenomation, resolution of shock with discontinuation of intravenous vasopressor/inotropic support and absence of life-threatening arrhythmias; and improvement or stabilization of any associated organ dysfunction (e.g., acute kidney injury). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence of toxicity in ICU then step down to IMCU if need this level of care then A period of observation (e.g., 12-24 hours) befor discharge to ward or home. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
33, 27 |
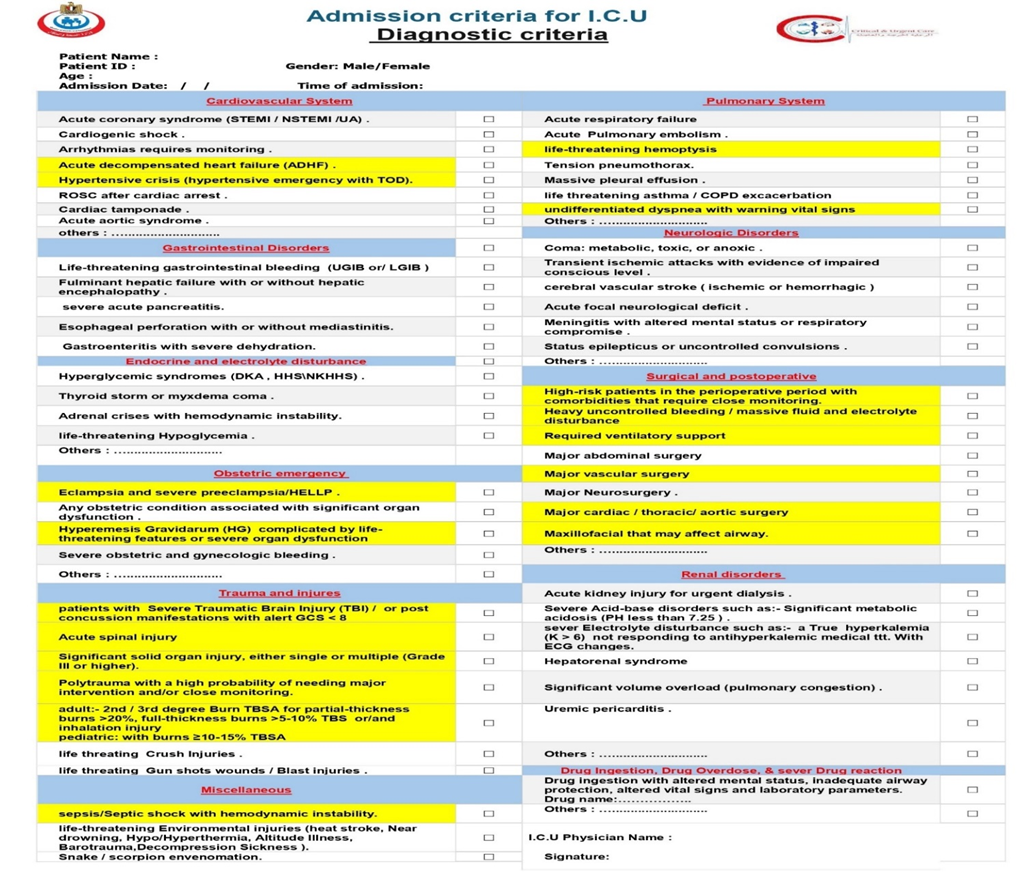
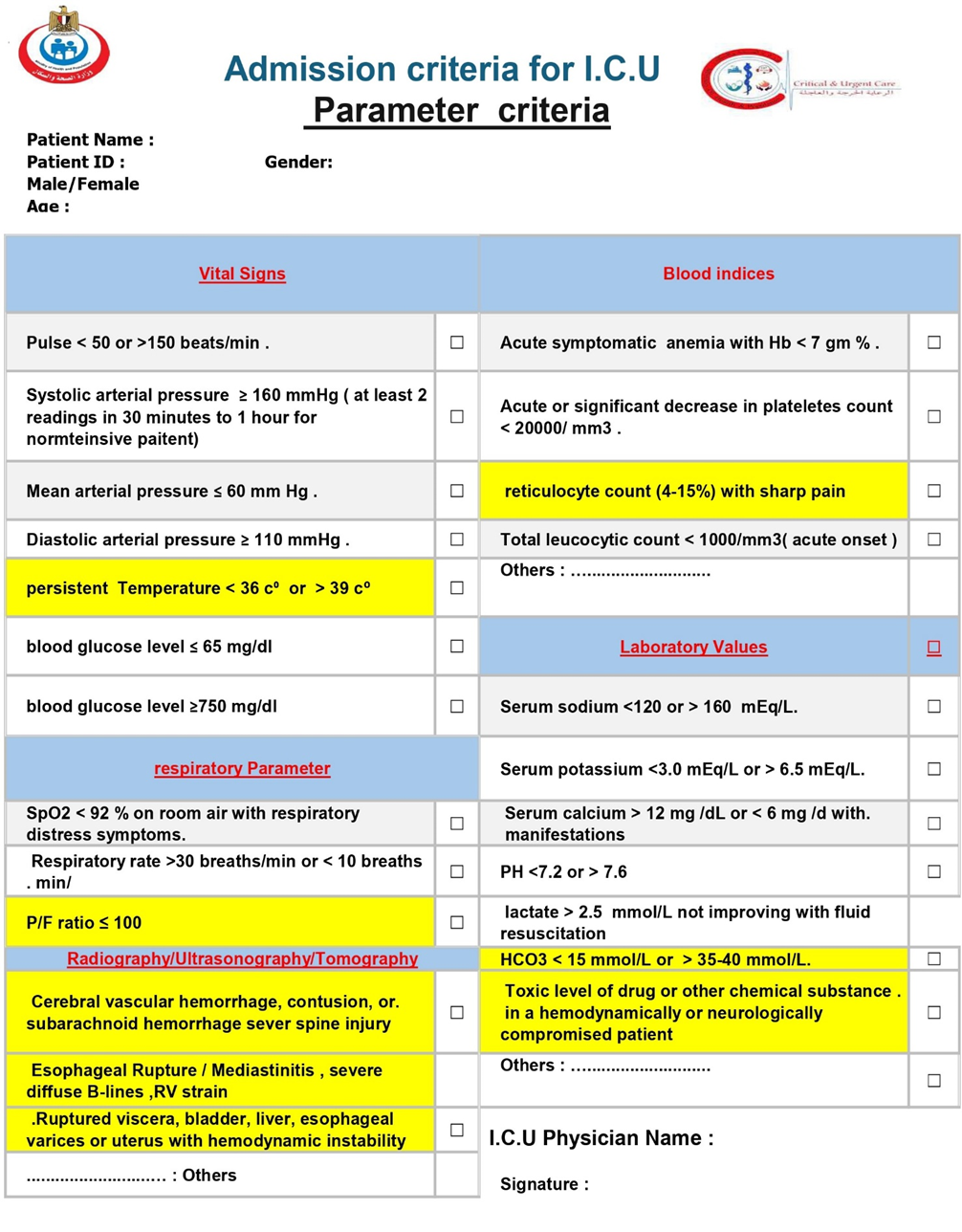
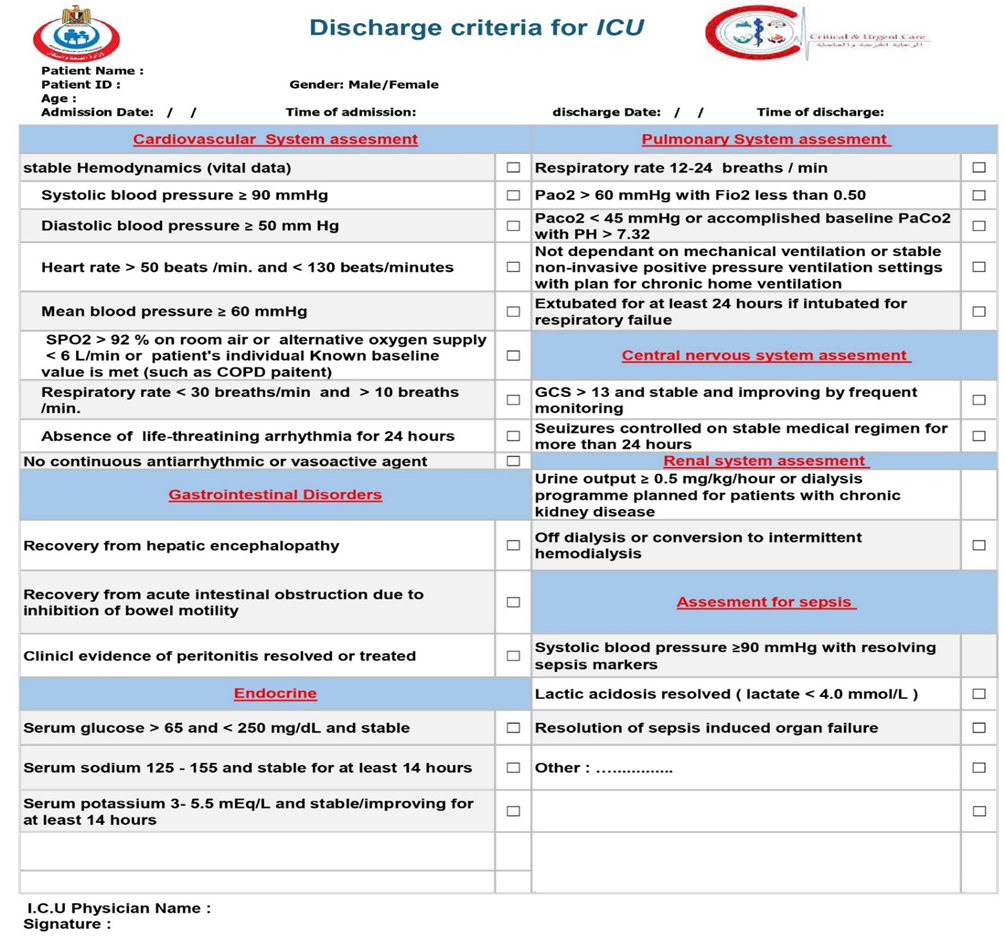
- Acknowledgements
|
Contribution |
Affiliation, Area of expertise / Primary location [work] |
Name |
|
Chairperson of Committee |
Adviser to the Minister of Health for Emergency and Urgent Care, Professor of Intensive Care, Faculty of Medicine, Ain Shams University, and Consultant of Internal Medicine and Cardiology |
Prof. Sherif Wadih Nashed |
|
Member |
Professor of Critical Care - Faculty of Medicine- Ain Shams University |
Prof. Ashraf El Sayed Abdel Rahman El Ajmi |
|
Member |
Dean of the Faculty of Medicine – Assiut University |
Prof. Alaa Mohamed Ahmed Attia |
|
Member |
Formar Head of the Central Administration of Critical and Emergency Care – Ministry of Health |
Prof. Khaled Gamal Hassan Ali Suleiman El Khatib |
|
Member |
Professor of Critical Care – Kasr Al Ainy - Chairman of the Critical Care Fellowship Board |
Prof. Hatem Hamed Hamed Al Atrosh |
|
Member |
Professor of Critical Care - Faculty of Medicine – Alexandria University |
Prof. Mohamed Mostafa Abdel Salam Megahed |
|
Member |
Assistant Professor in the Department of Critical Care - Faculty of Medicine-Kasr Al Ainy – Cairo University |
Prof. Mohamed Hosni Abdallah |
|
Member |
Assistant Professor of Critical Care – Faculty of Medicine-Minia University |
Prof.Mohamed Omar Abdel Aziz Mohamed |
|
Member |
Assistant Scientific Consultant – Damanhour Teaching Hospital |
Dr. Ayman Abdel Hamid Mahmoud El Tayyar |
|
Member |
Assistant Consultant - Liver Institute |
Dr. Iman Ibrahim El Desouki Mahmoud Ghoneimi |
|
Member |
Supervisor of Emergency and Critical Care – Healthcare Authority |
Dr. Mohamed Mahmoud Helmy Mohamed Badr |
|
Member |
Master’s in Health Economics – Unified Procurement Authority |
Dr.Rymonda Rafaat Rizk Shenouda |
|
Member |
Vice President of Beni Suef University for Environmental Affairs and Community Service |
Dr. Sameh Kamal Abdel Rahman Othman Al Maraghy |
|
Member |
Brigadier Doctor – Head of the Anesthesia and Critical Care Department – Medical Complex - Armed Forces |
Brig. Dr. Magdy Fathy Mohamed Lotfy Abdel Maksoud |
|
Member |
PhD in Critical Care – Colonel Doctor - Armed Forces |
Col. Dr. Yehia Abdel Tawab Mohamed Maki |
|
Member |
Consultant of Critical Care – Ministry of Interior |
Lt. Col. Dr. Ahmed Adel Mahmoud Abdel Hamid Mareekb |
|
Contribution |
Affiliation, Area of expertise / Primary location [work] |
Name |
|
Clinical expert management and crisis management expert |
Adviser to the Minister of Health for Emergency and Urgent Care, Professor of Intensive Care, Faculty of Medicine, Ain Shams University, and Consultant of Internal Medicine and Cardiology |
Prof. Sherif Wadih Nashed |
|
Clinical expert
|
Assistant Professor of Anesthesia and Critical Care Medicine. ,Faculty of Medicine, Cairo University |
Dr. Amr Kamal |
|
management and crisis management expert |
Head of Central Administration of Emergency & Critical Care - Ministry of Health & Population |
Dr. Mohammed Adel El-Sedfy |
|
Clinical expert |
MD cardiology Consultant of cardiology national heart institute Director of teaching hospital and institute |
Dr. Ahmed Farghaly Ali
|
|
Clinical expert |
Head of ICU Matarea teaching hospital MD degree critical care Ain Shams university |
Dr.Hend Abdel Sabour Mansour |
|
Clinical expert |
Consultant of Intensive Care Head of Icu department, Nasr city Insurance Hospital |
Dr. Mohamed Nada
|
|
Clinical expert |
Head of Icu dep.shoubra general hospital Master degree in Intensive Care Ain Shams university *Egyptian fellowship of Intensive Care |
Dr. Marwa Mhmoud Abdelsamia |
|
Clinical expert
|
Egyptian fellowship of Intensive Care Head of ICU dep .dar Elsalam oncology hospital (Hermel ) Master degree in Intensive Care Ain shams university Master degree in hospital administration faculty of commerce Ain shams university |
Dr. Doaa Ali Ismail
|
|
Clinical expert
|
Critical care medicine Consultant, MD Intensive care units administration manager - Central Administration of emergency and critical care- Ministry of Health & Population |
Dr. Mohammed Salah Youssef |
|
Clinical expert
|
Emergency Medicine Consultant Head of the Emergency Department - Central Administration of Emergency & Critical Care - Ministry of Health & Population |
Dr. Omar Nasr
|
|
Clinical expert
|
MD Community Medicine and Public health Director of poison and burn care administration -Central Administration of emergency and critical care- Ministry of Health & Population |
Dr. Mohamed Ali SeifEldin
|
|
Clinical expert
|
Emergency medicine Consultant Former General Director of Emergency Management-Central Administration of emergency and critical care- Ministry of Health & Population |
Dr. Diaaelden Abdelmawla Salama Ali
|
|
Clinical expert
|
Cardiology consultant Egyptian fellowship of Cardiology Egyptian fellowship of hospital management |
Dr. Eriny Kamal Atalla
|
|
Clinical expert
|
Consultant of critical care. Egyptian fellowship in critical care. Leadership in medicine, Harvard medical School. Head of emergency and critical care administration, Directorate of health affairs, Menoufia governorate. |
Dr.Mahmoud Ali Abdelfattah Seria.
|
|
Clinical expert ,management and crisis management expert |
General Director of Emergency Management-Central Administration of emergency and critical care- Ministry of Health & Population Master emergency medicine disaster medicine and management Diplome |
Dr.Hossam Eldin Safwat Mohammed Eladly |
|
Editor, Clinical expert
|
Anaesthesia and Intensive Care specialist - Master of Anaesthesia and Intensive Care -Clinical scholar at Clinical Scholar Research Training Programme (CSRT) -Egypt at Harvard medical School |
Dr. Reham Nashaat Nor ElDeen |
|
Editor, Clinical expert ,management and crisis management expert |
Curative & Critical Care Sector Representative , Crisis Management center, Ministry of Health & Population Disaster Medicine Management Diploma |
Mysara ahmed Abd-Elrazeik , B.Pharm |
All gratitude is due to God Almighty for blessing this work, until it Has reached its end.
The Committee thanks Egyptian Health Council, the ministry of health and population, members of critical care, emergency and crisis management Task Force and the Central Administration of emergency and critical care Central Administration of emergency and critical care for their efforts and participation in developing the clinical guide.
The members of the committee acknowledge the limitations of these guidelines. As a result of the vast amount of medical and healthcare management information to consider, constraints to evaluate the published and rapidly available new evidence, human fallibility and fast progress among others, the reader has to use his own judgment on how best apply our suggestions and recommendations. Therefore, neither the Egyptian health council nor the authors of this document assume responsibility for any injury to individuals as a result of the use of this guide.
This work is not related to any pharmaceutical company. The members of the guideline’s adaptation group and their institute and universities volunteered their participation.
- Abbreviations
AAS: Acute Aortic Syndrome
AD: aortic dissection
AF: Atrial fibrillation
AKI: acute kidney injury
APACHE: Acute Physiology and Chronic Health Evaluation.
AS: Acute stroke.
BiPAP: Bilevel Positive airway pressure.
CCRT: Critical Care Response Team.
CCU: coronary care unit
CPAP: Continuous positive airway pressure.
CPR: Cardiopulmonary resuscitation
CT: computed tomography
DIC: Disseminated intravascular coagulation
DKA: Diabetic ketoacidosis
DNR: Do not resuscitate.
HG: Hyperemesis Gravidarum
HRS: Hepatorenal Syndrome
ICU: intensive care unit
IMCU: Intermediate Care Unit
MEWS: Modified Early Weaning Score.
MODS: multi-organ dysfunction syndrome
MRI: Magnetic Resonance Imaging
NOM: Non-Operative Management
NSTEMI: Non-ST-elevation myocardial infarction
ROSC: Return of spontaneous circulation
RRS: Rapid Response System
RRT: Rapid Response Team
SAPS: Simplified Acute Physiology Score.
SE: Status Epilepticus
SIRS: systemic inflammatory response syndrome
STEMI: ST Elevation Myocardial Infarction.
TAVI: Transcatheter Aortic Valve Implantation.
TBSA: Total body surface area
TOD: target organ damage
UA: Unstable angina
WHO: World Health Organization
- Glossary
Acute aortic syndrome (AAS): - encompasses 3 life-threatening conditions: acute aortic dissection (AAD), intramural hematoma (IMH), and penetrating aortic ulcer (PAU). AAD involves a tear in the aortic wall, creating a false lumen.
Acute coronary syndrome: - group of diseases in which blood flow to the heart is decreases. Some examples include ST-elevation myocardial infarction
Acute Liver Failure: rapid and severe liver injury, impaired liver synthetic function (coagulopathy with INR ≥1.5), and the development of hepatic encephalopathy (any degree of altered mental status) in individuals without pre-existing cirrhosis.
Acute respiratory failure: the inability of the respiratory system to meet the oxygenation, ventilation, or metabolic requirements of the patient.
acute variceal bleeding: gastrointestinal bleeding due to a rupture of collateral portosystemic vascular channels (varices, especially gastrointestinal) usually formed in response to portal hypertension.
Adrenal crisis: Acute manifestation of adrenal insufficiency with symptoms including hypotension, hypovolemic shock, fever, and/or hypoglycemia.
Arrhythmias: an abnormal rhythm of the heart. The only normal rhythm of the heart is a normal sinus rhythm.
Atrial fibrillation - A heart condition that causes an irregular heartbeat, often faster than the normal heart rate.
BiLevel positive airway pressure (BiLevel):- a noninvasive form of mechanical ventilation delivered through nasal or full-face masks with inspiration and exhalation pressures above atmospheric levels that has gained broad clinical support.
Cardiac tamponade: abnormal amounts of fluid accumulate in the pericardial sac compressing the heart and leading to a decrease in cardiac output and shock
Cardiogenic shock: - severe impairment of myocardial performance that results in diminished cardiac output, end‐organ hypoperfusion, and hypoxia.
Cardiovascular disease: - Disease of the heart and/or blood vessels.
Coma: brain failure with unarousable unresponsiveness to any external stimulation that may occur from a process/defect originating in the central nervous system or may reflect a systemic metabolic process.
Continuous positive airway pressure: - type of positive airway pressure that is used to deliver a set pressure to the airways that is maintained throughout the respiratory cycle, during both inspiration and expiration.
Critical Care Response Team: - a multidisciplinary team of clinical personnel constituted and equipped with the relevant competence to bring critical care to the patient's bedside, thus preventing the patient's status from degenerating into cardiac arrest.
Dehydration: A condition that occurs when the body loses too much water and other fluids that it needs to work normally.
Diabetes mellitus: a condition arising when the pancreas does not produce enough insulin or the body cannot effectively use insulin.
Diabetic ketoacidosis: a serious life-threatening complication of diabetes characterized by hyperglycemia (high blood glucose levels), ketosis (high levels of ketone bodies in the blood or urine), and metabolic acidosis (high anion gap).
distributive shock: abnormal distribution of blood flow in the smallest blood vessels results in inadequate blood supply to the body tissues, resulting in ischemia and organ dysfunction.
Eclampsia: complication of severe preeclampsia, is commonly defined as new onset of grand mal seizure activity and/or unexplained coma during pregnancy or postpartum in a woman with signs or symptoms of preeclampsia.
Esophageal perforation: known as Boerhaave syndrome, is a rupture of the esophageal wall with or without a transmural communication between the upper gastrointestinal tract and the mediastinum.
HELLP Syndrome: rare but life-threatening complication of pregnancy that is characterized by Hemolysis (breakdown of red blood cells), Elevated Liver enzyme levels, and a Low Platelet count. HELLP develops late in pregnancy, or sometimes after birth.
Hemodynamically unstable: - abnormal or unstable blood pressure that results in improper circulation and organs of the body do not receive adequate blood flow. Hemodynamic instability is characterized by chest pain, confusion, hypotension (i.e., low blood pressure), abnormal heart rate, loss of consciousness, restlessness, shortness of breath, cold hands, arms, legs, or feet, etc.
Hyperemesis Gravidarum: severe, persistent nausea and vomiting during pregnancy that can lead to dehydration, electrolyte imbalance, and weight loss.
Hyperglycemic syndromes: a clinical conditions that arises from a complication of diabetes mellitus.
Hyperosmolar hyperglycemic state: a metabolic complication of diabetes mellitus characterized by severe hyperglycemia, extreme dehydration, hyperosmolar plasma, and altered consciousness. It most often occurs in type 2 diabetes, often in the setting of physiologic stress.
Hypertension: - Raised blood pressure.
hypertensive crisis: severe increase in blood pressure (systolic ≥180 mm Hg and/or diastolic ≥110 mm Hg).
Hypertensive Emergency: Severely elevated blood pressure (BP) – often SBP >180 mmHg or DBP >120 mmHg, though the absolute level is less critical than the presence of organ damage – accompanied by evidence of acute, ongoing target organ damage (TOD).
Hypertensive Urgency: Severely elevated blood pressure (BP) – often SBP >180 mmHg or DBP >120 mmHg, but without evidence of acute ongoing target organ damage. These patients usually do not require ICU admission and can be managed with gradual BP reduction using oral medications, often on an outpatient or short-stay basis.
Ischemic stroke: - A stroke that happens when a blood clot blocks an artery that is carrying blood to the brain.
Life-threatening gastrointestinal bleeding: acute haemorrhage originating from the gastrointestinal tract that leads to significant hemodynamic compromise can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus.
life-threatening hemoptysis : a life-threatening event including significant airway obstruction, significant abnormal gas exchange, or hemodynamic instability. It is expectoration of a large amount of blood and/or a rapid rate of bleeding approximately 150 mL of blood expectorated in a 24-hour period (easily quantifiable by patients as roughly a half cup of blood in 24 hours) or bleeding at a rate ≥100 mL/hour. Or small amounts of blood in patients with underlying cardiorespiratory disease may be enough to endanger life, particularly if thrombus obstructs a major airway or there is very little residual functional lung tissue.
Lower Gastrointestinal Bleeding (LGIB): Bleeding that occurs distal to the ligament of Treitz, often from the colon, rectum, or small intestine.
Magnetic resonance imaging (MRI):- A non-invasive imaging technique that allows for detailed examination of the brain
Massive Transfusion Protocol (MTP): A standardized protocol for rapid blood product replacement in cases of major hemorrhage.
Myxedema coma: severe hypothyroidism leading to decreased mental status, hypothermia, and other symptoms related to slowing of function in multiple organs.
Pneumothorax: a collection of air outside the lung but within the pleural cavity. This can cause all or part of the lung to collapse.
Sepsis: life-threatening organ dysfunction caused by a dysregulated host response to infection.
Septic shock: a subset of sepsis and subclass of distributive shock in which particularly profound circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than with sepsis alone with a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and serum lactate level greater than 2 mmol/L (>18 mg/dL) in the absence of hypovolemia.
Sever Hyperkalemia: a serum or plasma potassium level above the upper limits of normal, usually greater than 5.0 mEq/L to 5.5 mEq/L that may cause life-threatening cardiac arrhythmias, muscle weakness, or paralysis.
severe acute pancreatitis: - acute inflammatory attack of the pancreas of sudden onset with persistent organ failure, that is, organ failure >48 h.
Tension pneumothorax: a life-threatening emergency wherein a large air collection in the pleural space compromises respiration and cardiac function.
Thyroid storm: a rare and life-threatening severe thyrotoxicosis
Transcatheter aortic valve implantation (TAVI):- the implantation of the aortic valve of the heart through the blood vessels without actual removal of the native valve (as opposed to the aortic valve replacement by open heart surgery, surgical aortic valve replacement, AVR).
Upper Gastrointestinal Bleeding (UGIB): Bleeding originating above the ligament of Treitz, commonly from the esophagus, stomach, or duodenum.- Introduction
In countries like Egypt, where critical care resources like ICU beds are limited, it's crucial to prioritize patients who will benefit most from intensive care. Early identification and treatment of critically ill patients can often prevent the need for ICU admission and improve outcomes. Currently, there's no single, universally accepted guide for when patients need critical care.
Generally, patients with single-organ failure may be managed in intermediate or high-dependency care units. However, those experiencing respiratory failure or more than two-organ failure typically require ICU admission. While "track and trigger" systems have been introduced in intermidate care unite to identify and treat sick patients promptly, there's no definitive proof yet that they successfully prevent deterioration. Therefore, the decision to admit a patient to critical care still largely depends on a clinician's judgment, along with an assessment of the patient's immediate physiological state and long-term health.
New guidelines have been developed to address these challenges, focusing on several key areas:
➡️Key Aspects of the Guidelines
· General Conditions and Transfer: These guidelines emphasize the importance of quickly transferring critically ill patients to available ICU beds. If an ICU isn't available at the current hospital, national or regional referral systems should be used.
· ICU Admission and Triage Policies: The guidelines stress the need for fair and transparent triage decisions, taking into account clinical needs, patient demographics, ICU capacity, and available resources. They also highlight the importance of balancing planned post-operative admissions with emergency cases and having a flexible system for immediate life-threatening conditions.
· Intermediate Care Units (IMCUs): The guidelines recommend establishing IMCUs. These units would act as a bridge between general wards and ICUs, aiming to improve patient safety, reduce the number of patients readmitted to the ICU, and make better use of critical care beds.
· Rapid Response Systems (RRS): The guidelines advocate for developing and implementing RRS. These systems help identify, assess, and triage deteriorating patients on general wards early on, using vital sign-based triggers and a dedicated Rapid Response Team (RRT).
· Admission and Discharge Criteria Checklists: Detailed checklists are provided for ICU admission, based on specific diagnoses and physiological parameters. These cover a wide range of conditions affecting various organ systems, including cardiovascular, pulmonary, neurological, gastrointestinal, endocrine, obstetric, trauma, renal, and other critical emergencies like sepsis and environmental injuries.
· Mass Casualty Incidents, Pandemics, and Epidemics: The guidelines include preparedness plans for ICUs to manage large-scale disasters, covering aspects like increasing capacity, allocating resources, and coordinating responses.
· ICU Discharge: A structured, comprehensive assessment is outlined for patient discharge, focusing on the patient's physiological stability, the resolution of acute conditions, and the ability of the receiving unit to ensure a safe transition of care.
The guidelines are built upon a foundation of evidence-based practices, drawing from national and international guidelines, Due to the lack of in-depth clinical evidence on the subject and the overlap of intensive care services with most medical specialties, writing this guide required overlap with many clinical guides for those specialties, including revised research papers, and Textbooks. The methodology for developing these guidelines involved a rigorous process, including a comprehensive search for relevant literature and the appraisal of retrieved guidelines.
The committee completed the review and revision of to review current guidelines for the admission, discharge, and triage related to the clinical guide and to provide a framework for practice and to make recommendations for change.
In order to reach the highest levels of assurance while writing the guide, it was adopted to review the diseases most exposed to intensive care doctors during their work. The methodology included a thorough search for relevant literature and a critical evaluation of existing guidelines. In 2024, the Central Administration for Emergency and Critical Care of the Egyptian Ministry of Health and Population formed a task force. This task force, composed of its members and doctors from major Egyptian hospitals across critical medical specialties, reviewed and revised current admission, discharge, and triage guidelines. Their goal was to create a practical framework and recommend changes, ensuring standardization in diagnosis and care possibilities across hospitals. They specifically focused on diseases most commonly encountered by intensive care doctors to ensure the guide's practical relevance and highest level of assurance.
- Scope & Purpose
This document serves as a national guideline, aiming to standardize and improve critical care delivery. It addresses the diverse needs of critically ill patients, the optimal utilization of limited ICU resources, and the importance of a structured approach to critical care management.
also to reducing malpractice, variation in practice, and healthcare costs.
- TARGET AUDIENCE
The guideline is intended for:Clinicians who are involved in the care and treatment of patients in emergency department and ICU and any OTHER departments need to referral critical ill pateints including intensive care ,emergency medicine, neurology, Pediatricians ,Family doctors and internal medicine doctors and High nurses.
- Methods
We adopted WHO proposed seven distinct steps for development of clinical guidelines to ensure a thorough and rigorous process
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Due to the lack of in-depth clinical evidence on the subject and the overlap of intensive care services with most medical specialties, writing this guide required overlap with many clinical guides for those specialties, including revised research papers, and Textbooks.
inclusion/exclusion criteria followed in the search and retrieval of guidelines to be adapted :
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author not on behalf of an organization in order to be valid and comprehensive, a guideline ideally requires multidisciplinary input.
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations.
The following characteristics of the retrieved guidelines were summarized in a table:
• Developing organisation/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least two members. the panel decided a cut-off point or rank the guidelines (any guideline scoring above 50% on the rigour dimension was retained). These guidelines were adapted mainly from Society of Critical Care Medicine ICU Admission, Discharge, and Triage Guidelines update in 2016, with partial incorporation of insights from reputable sources to enhance its comprehensiveness and applicability [1]
Evidence assessment:
According to WHO handbook for Guidelines we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed information on GRADE is available on the following sites:
■ GRADE working group: https://www.gradeworkinggroup.org/
■ GRADE online training modules: http://cebgrade.mcmaster.ca/
Table 1 Quality of evidence in GRADE
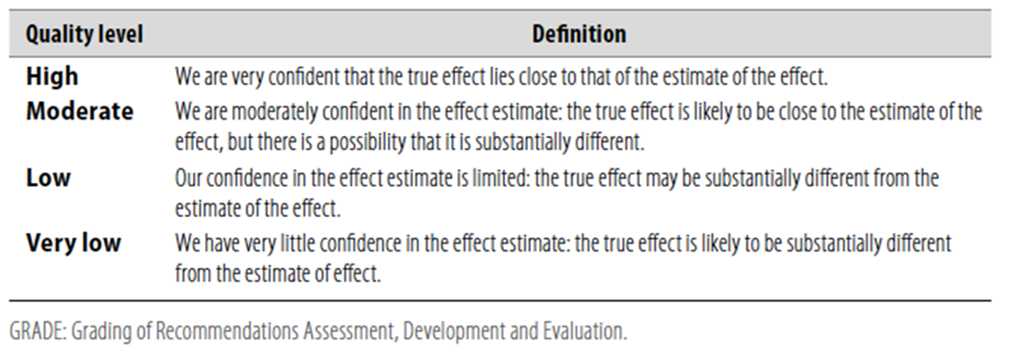
Table 2 Significance of the four levels of evidence
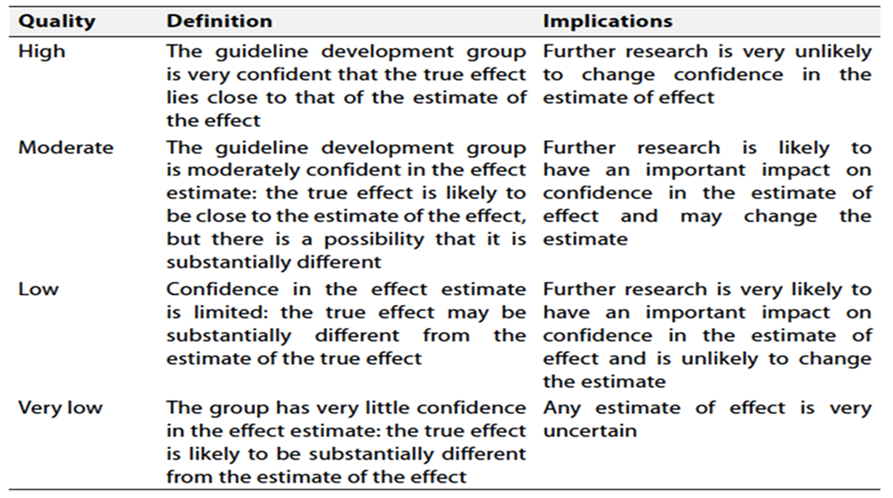
Table 3 Factors that determine How to upgrade or downgrade the quality of evidence.
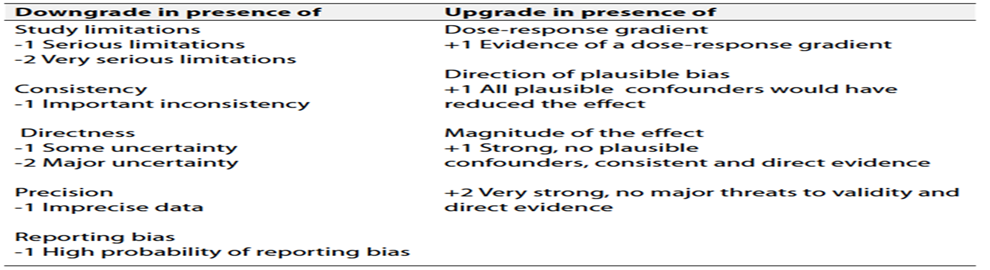
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.- Clinical indictor for Monitoring and evaluating the impact of the guideline
The following are two performance measures or indicators for implementing this adapted guideline:
1- mortality rate of patients
Numerator : mortality rate of patients discharge from ICU as per guideline recommendations
Denominator : Total number of patients discharge from ICU
Data Source: Hospital or clinic patient records.
- Research needs
· Improving accuracy of severity scoring tools (APACHE, SAPS, and Mortality Prediction Model) and nursing productivity models
· Utilizing telemedicine to monitor discharged patients and “capture” red flags to increase timeliness of intervention and prevent readmission to critical care.
· Utilizing telemedicine to assist with monitoring critical care patients who were triaged to a nontraditional critical care unit because of lack of critical care bed availability.
- Updating of the guideline
These guidelines will be updated whenever there is new evidence.
- References
1. Nates JL, Nunnally M, Kleinpell R, et al. ICU Admission, Discharge, and Triage Guidelines: A Framework to Enhance Clinical Operations, Development of Institutional Policies, and Further Research. Crit Care Med. 2016;44(8):1553-1602. doi:10.1097/CCM.0000000000001856
2. Cardoso LT, Grion CM, Matsuo T, et al. Impact of delayed admission to intensive care units on mortality of critically ill patients: a systematic review and meta-analysis. Intensive Care Med. 2011;37(10):1551-1559. doi: 10.1007/s00134-011-2305-9
3. Chalfin DB, Trzeciak S, Likourezos A, Baumann BM, Dellinger RP; DELAY-ED Study Group. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35(6):1477-1483. doi: 10.1097/01.CCM.0000266587.74546.5A
4. Chalfin DB, Trzeciak S, Likourezos A, Baumann BM, Dellinger RP; DELAY-ED study group. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35(6):1477-1483. doi:10.1097/01.CCM.0000266585.74905.5A
5. Fan E, MacDonald RD, Adhikari NK, et al. Outcomes of interfacility critical care adult patient transport: a systematic review. Crit Care. 2006;10(1):R6. doi:10.1186/cc3924.
6. Kohl BA, Fortino-Mullen M, Praestgaard A, Hanson CW, Dimartino J, Ochroch EA. The effect of ICU telemedicine on mortality and length of stay. J Telemed Telecare. 2012;18(5):282-286. doi:10.1258/jtt.2012.120208
7. Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. Lancet. 2010;376(9749):1339-1346. doi:10.1016/S0140-6736(10)60446-1
8. Zimmerman JE, Kramer AA, McNair DS, Malila FM. Intensive care unit length of stay: benchmarking based on Acute Physiology and Chronic Health Evaluation (APACHE) IV. Crit Care Med. 2006;34(10):2517-2529. doi: 10.1097/01.CCM.0000239318.50102.D9
9. Wunsch H, Angus DC, Harrison DA, et al. Variation in critical care services across North America and Western Europe. Crit Care Med. 2008;36(10):2787-e9. doi:10.1097/CCM.0b013e318186aec8
10. Truog RD, Mitchell C, Daley GQ. The toughest triage — allocating ventilators in a pandemic. N Engl J Med. 2020;382(21):1973-1975. doi: 10.1056/NEJMp2005689
11. Christian MD, Sprung CL, King MA, et al. Triage: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest. 2014;146(4 Suppl):e61S-74S. doi:10.1378/chest.14-0736
12. Vincent JL, Rubenfeld GD. Does intermediate care improve patient outcomes or reduce costs?. Crit Care. 2015;19(1):89. Published 2015 Mar 2. doi:10.1186/s13054-015-0813-0
13. Beaussier M, Guidet B, Aegerter P, et al. Profiles of the patients admitted to intermediate care units in France: Admission criteria appropriateness and potential outcome benefits (UNISURC project part 2). J Crit Care. 2025;88:155078. doi:10.1016/j.jcrc.2025.155078
14. Wang L, Qing J, Zhang X, et al. Effects of the intermediate care unit on the oldest-old general surgical patients: a retrospective, pre- and postintervention study. Aging Clin Exp Res. 2021;33(6):1557-1566. doi:10.1007/s40520-020-01662-5
15. López-Jardón P, Martínez-Fernández MC, García-Fernández R, Martín-Vázquez C, Verdeal-Dacal R. Utility of Intermediate Care Units: A Systematic Review Study. Healthcare (Basel). 2024;12(3):296. Published 2024 Jan 24. doi:10.3390/healthcare12030296
16. Smith GB, Redfern OC, Pimentel MA, et al. The National Early Warning Score 2 (NEWS2). Clin Med (Lond). 2019;19(3):260. doi:10.7861/clinmedicine.19-3-260
17. Mezzaroba AL, Tanita MT, Festti J, Carrilho CM, Cardoso LT, Grion CM. Evaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital. Avaliação de 5 anos de atuação de um time de resposta rápida liderado por médico intensivista em hospital universitário. Rev Bras Ter Intensiva. 2016;28(3):278-284. doi:10.5935/0103-507X.20160045
18. Hatlem T, Jones C, Woodard EK. Reducing mortality and avoiding preventable ICU utilization: analysis of a successful rapid response program using APR DRGs [published correction appears in J Healthc Qual. 2022 Nov-Dec 01;44(6):373. doi: 10.1097/JHQ.0000000000000368.]. J Healthc Qual. 2011;33(5):7-16. doi:10.1111/j.1945-1474.2011.00084.x
19. Boniatti MM. Advances in performance, more benefits... the perspectives of rapid response teams. Avanços na atuação, mais benefícios... as perspectivas dos times de resposta rápida. Rev Bras Ter Intensiva. 2016;28(3):217-219. doi:10.5935/0103-507X.20160048
20. Cross G, Bilgrami I, Eastwood G, et al. The epidemiology of sepsis during rapid response team reviews in a teaching hospital. Anaesth Intensive Care. 2015;43(2):193-198. doi:10.1177/0310057X1504300208
21. Park SH, Kang J, Kim TJ, Lee HY, Cho HJ, Lee SM. Current status of the rapid response system and early warning score: a survey-based analysis. Acute Crit Care. 2022;37(4):687-689. doi:10.4266/acc.2022.01144
22. Robertson M, Lim AKH, Bloom A, et al. Epidemiology and Prognostic Significance of Rapid Response System Activation in Patients Undergoing Liver Transplantation. J Clin Med. 2021;10(23):5680. Published 2021 Dec 1. doi:10.3390/jcm10235680
23. Winters BD, Weaver SJ, Pfoh ER, Yang T, Pham JC, Dy SM. Rapid-response systems as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 Pt 2):417-425. doi:10.7326/0003-4819-158-5-201303051-00009
24. Beitler JR, Link N, Bails DB, Hurdle K, Chong DH. Reduction in hospital-wide mortality after implementation of a rapid response team: a long-term cohort study. Crit Care. 2011;15(6):R269. doi:10.1186/cc10547
25. Schneider AG, Calzavacca P, Mercer I, Hart G, Jones D, Bellomo R. The epidemiology and outcome of medical emergency team call patients treated with non-invasive ventilation. Resuscitation. 2011;82(9):1218-1223. doi:10.1016/j.resuscitation.2011.04.009
26. Lyons PG, Edelson DP, Churpek MM. Rapid response systems. Resuscitation. 2018;128:191-197. doi:10.1016/j.resuscitation.2018.05.013
27. Mahmoodpoor A, Sanaie S, Saghaleini SH, et al. Prognostic value of National Early Warning Score and Modified Early Warning Score on intensive care unit readmission and mortality: A prospective observational study. Front Med (Lausanne). 2022;9:938005. Published 2022 Aug 4. doi:10.3389/fmed.2022.938005
28. Mellinghoff J, O'Shea P, Dawson D, Ball J, Rhodes A, Grounds M. Delayed discharges revisited: impact of a liaison post on patients' transition from ICU to ward care. Crit Care. 2012;16(Suppl 1):P513. doi:10.1186/cc11120
29. Baker-McClearn D, Carmel S. Impact of critical care outreach services on the delivery and organization of hospital care. J Health Serv Res Policy. 2008;13(3):152-157. doi:10.1258/jhsrp.2008.008003
30. Garcea G, Thomasset S, McClelland L, Leslie A, Berry DP. Impact of a critical care outreach team on critical care readmissions and mortality. Acta Anaesthesiol Scand. 2004;48(9):1096-1100. doi:10.1111/j.1399-6576.2004.00509.x
31. Barfod C, Lauritzen MM, Danker JK, et al. Abnormal vital signs are strong predictors for intensive care unit admission and in-hospital mortality in adults triaged in the emergency department - a prospective cohort study. Scand J Trauma Resusc Emerg Med. 2012;20:28. Published 2012 Apr 10. doi:10.1186/1757-7241-20-28
32. Guidelines for intensive care unit admission, discharge, and triage. Task Force of the American College of Critical Care Medicine, Society of Critical Care Medicine. Crit Care Med. 1999;27(3):633-638.
33. K Ehikhametalor, L-A Fisher, C Bruce, et al. Guidelines for Intensive Care Unit Admission, Discharge and Triage. West Indian Med J. 2019;68(2):46-54 doi:10.7727/wimj.2018.197
34. Lemeshow S, Le Gall JR. Modeling the severity of illness of ICU patients. A systems update. JAMA. 1994;272(13):1049-1055
35. Soares J, Leung C, Campbell V, Van Der Vegt A, Malycha J, Andersen C. Intensive care unit admission criteria: a scoping review. J Intensive Care Soc. 2024;25(3):296-307. Published 2024 Apr 15. doi:10.1177/17511437241246901
36. Sadaka F, EthmaneAbouElMaali C, Cytron MA, Fowler K, Javaux VM, O'Brien J. Predicting Mortality of Patients With Sepsis: A Comparison of APACHE II and APACHE III Scoring Systems. J Clin Med Res. 2017;9(11):907-910. doi:10.14740/jocmr3083w
37. Wilfong EM, Lovly CM, Gillaspie EA, et al. Severity of illness scores at presentation predict ICU admission and mortality in COVID-19. J Emerg Crit Care Med. 2021;5:7. doi:10.21037/jeccm-20-92 (100)
38. Keegan MT, Gajic O, Afessa B. Severity of illness scoring systems in the intensive care unit. Crit Care Med. 2011;39(1):163-169. doi:10.1097/CCM.0b013e3181f96f81
39. Tang WM, Tong CK, Yu WC, Tong KL, Buckley TA. Outcome of adult critically ill patients mechanically ventilated on general medical wards. Hong Kong Med J. 2012;18(4):284-290.
40. Lott JP, Iwashyna TJ, Christie JD, Asch DA, Kramer AA, Kahn JM. Critical illness outcomes in specialty versus general intensive care units. Am J Respir Crit Care Med. 2009;179(8):676-683. doi:10.1164/rccm.200808-1281OC
41. Sasser SM, Hunt RC, Faul M, et al. Guidelines for field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2011. MMWR Recomm Rep. 2012;61(RR-1):1-20.
42. Collet JP, Thiele H, Barbato E, et al; ESC Scientific Document Group. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3898-4019. doi: 10.1093/eurheartj/ehad191
43. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119-177. doi:10.1093/eurheartj/ehx393
44. Asano T, Koeda Y, Nasu T, et al. Impact of High Care Unit Management on In-Hospital Mortality in Patients with ST-Elevation Myocardial Infarction. Int Heart J. 2025;66(2):226-233. doi:10.1536/ihj.24-720
45. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines [published correction appears in Circulation. 2013 Dec 24;128(25):e481]. Circulation. 2013;127(4):e362-e425. doi:10.1161/CIR.0b013e3182742cf6
46. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization [published correction appears in Eur Heart J. 2019 Oct 1;40(37):3096. doi: 10.1093/eurheartj/ehz507.]. Eur Heart J. 2019;40(2):87-165. doi:10.1093/eurheartj/ehy394 (4)
47. Anderson JL, Morrow DA. Acute Myocardial Infarction. N Engl J Med. 2017;376(21):2053-2064. doi:10.1056/NEJMra1606915
48. McDonagh TA, Metra M, Adamo M, et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure [published correction appears in Eur Heart J. 2024 Jan 1;45(1):53. doi: 10.1093/eurheartj/ehad613.]. Eur Heart J. 2023;44(37):3627-3639. doi:10.1093/eurheartj/ehad195 (4.1, 54, 64)
49. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in Circulation. 2022 May 3;145(18):e1033. doi: 10.1161/CIR.0000000000001073.] [published correction appears in Circulation. 2022 Sep 27;146(13):e185. doi: 10.1161/CIR.0000000000001097.] [published correction appears in Circulation. 2023 Apr 4;147(14):e674. doi: 10.1161/CIR.0000000000001142.]. Circulation. 2022;145(18):e895-e1032. doi:10.1161/CIR.0000000000001063
50. van Diepen S, Katz JN, Albert NM, et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2017;136(16):e232-e268. doi:10.1161/CIR.0000000000000525
51. Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999;341(9):625-634. doi:10.1056/NEJM199908263410901
52. Thiele H, Zeymer U, Neumann FJ, et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med. 2012;367(14):1287-1296. doi:10.1056/NEJMoa1208410
53. Vahdatpour C, Collins D, Goldberg S. Cardiogenic Shock. J Am Heart Assoc. 2019;8(8):e011991. doi:10.1161/JAHA.119.011991
54. Tehrani BN, Truesdell AG, Sherwood MW, et al. Standardized Team-Based Care for Cardiogenic Shock [published correction appears in J Am Coll Cardiol. 2019 Jul 23;74(3):481. doi: 10.1016/j.jacc.2019.06.010.]. J Am Coll Cardiol. 2019;73(13):1659-1669. doi:10.1016/j.jacc.2018.12.084
55. Zeppenfeld K, Tfelt-Hansen J, de Riva M, et al; ESC Scientific Document Group. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022;43(40):3997-4126. doi: 10.1093/eurheartj/ehac262
56. Hindricks G, Potpara T, Dagres N, et al; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373-498. doi: 10.1093/eurheartj/ehaa612
57. Brugada J, Katritsis DG, Arbelo E, et al; ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020;41(5):655-720. doi: 10.1093/eurheartj/ehz467
58. Glikson M, Nielsen JC, Kronborg MB, et al; ESC Scientific Document Group. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021;42(35):3427-3520. doi: 10.1093/eurheartj/ehab364
59. elker GM, Teerlink JR. Diagnosis and Management of Acute Heart Failure. In: Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF, Braunwald E, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Elsevier; 2022:chap 26.
60. Adams KF Jr, Fonarow GC, Emerman CL, et al; ADHERE Scientific Advisory Committee and Investigators. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005;149(2):209-216. doi: 10.1016/j.ahj.2004.08.005
61. Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J Hypertens. 2023;41(12):2159-2241. doi: 10.1097/HJH.0000000000003480
62. Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018 Jun;71(6):1269-1324. doi: 10.1161/HYP.0000000000000066. Epub 2017 Nov 13. Erratum in: Hypertension. 2018 Jun;71(6):e136-e139. doi: 10.1161/HYP.0000000000000075. Erratum in: Hypertension. 2018 Sep;72(3):e33. doi: 10.1161/HYP.0000000000000080. PMID: 29133354.
63. nger T, Borghi C, Charchar F, et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension. 2020;75(6):1334-1357. doi: 10.1161/HYPERTENSIONAHA.120.15026
64. Watson K, Broscious N, Devabhakthuni S, Noel ZR. Management of Hypertensive Crises: A Review for Practitioners. Cardiol Clin. 2024;42(1):71-81. doi: 10.1016/j.ccl.2023.07.008
65. Marik PE, Varon J. Hypertensive crises: challenges and management. Chest. 2007;131(6):1949-1962. doi: 10.1378/chest.06-2490
66. Panchal AR, Bartos JA, Cabañas JG, et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S366-S468. doi: 10.1161/CIR.0000000000000916
67. Nolan JP, Sandroni C, Böttiger BW, et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-resuscitation care. Resuscitation. 2021;161:220-256. doi: 10.1016/j.resuscitation.2021.02.012
68. Nielsen N, Wetterslev J, Cronberg T, et al; TTM Trial Investigators. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369(23):2197-2206. doi: 10.1056/NEJMoa1310519 (8)
69. Dankiewicz J, Cronberg T, Lilja G, et al; TTM2 Trial Investigators. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N Engl J Med. 2021;384(24):2283-2294. doi: 10.1056/NEJMoa2100591
70. Adler Y, Charron P, Imazio M, et al; ESC Scientific Document Group. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36(42):2921-2964. doi: 10.1093/eurheartj/ehv318
71. Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003;349(7):684-690. doi: 10.1056/NEJMra022643
72. Ariyarajah V, Spodick DH. Cardiac tamponade revisited: a critical review of decision-making in the emergency room. Am J Emerg Med. 2007;25(2):218-224. doi: 10.1016/j.ajem.2006.07.009
73. Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;146(24):e334-e482. doi: 10.1161/CIR.0000000000001106 (Also published in J Am Coll Cardiol. 2022;80(24):e223–e393).
74. Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC Guidelines on the diagnosis and management of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014;35(41):2873-2926. doi: 10.1093/eurheartj/ehu281
75. Pape LA. Acute Aortic Syndromes. Circulation. 2021;144(15):1253-1270. doi: 10.1161/CIRCULATIONAHA.121.054319
76. CA, Clough RE. Management of acute aortic dissection. Lancet. 2015;385(9970):800-811. doi: 10.1016/S0140-6736(14)61005-9
77. Evangelista A, Isselbacher EM, Bossone E, et al; IRAD Investigators. Insights From the International Registry of Acute Aortic Dissection: Toward Standardized Reporting. Circulation. 2018;137(17):1837-1848. doi: 10.1161/CIRCULATIONAHA.117.031244
78. Cahill TJ, Jewell PD, Ponnuthurai FA, et al. Management of acute aortic dissection in critical care. J Intensive Care Soc. 2023;24(4):409-418. doi: 10.1177/17511437231162219
79. Laine L, Barkun AN, Saltzman JR, et al. ACG Clinical Guideline: Upper Gastrointestinal and Ulcer Bleeding. Am J Gastroenterol. 2021;116(5):899-917. doi: 10.14309/ajg.0000000000001245
80. Gralnek IM, Stanley AJ, Morris AJ, et al. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2021. Endoscopy. 2021;53(3):300-329. doi: 10.1055/a-1369-5274
81. Oakland K, Chadwick G, East JE, et al; British Society of Gastroenterology. Diagnosis and management of acute lower gastrointestinal bleeding: guidelines from the British Society of Gastroenterology. Gut. 2019;68(5):776-789. doi: 10.1136/gutjnl-2018-317807
82. Strate LL, Gralnek IM. ACG Clinical Guideline: Management of Patients With Acute Lower Gastrointestinal Bleeding. Am J Gastroenterol. 2016;111(4):459-474. doi: 10.1038/ajg.2016.41
83. de Franchis R, Bosch J, Garcia-Tsao G, et al; Baveno VII Faculty. Baveno VII - Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959-974. doi: 10.1016/j.jhep.2021.12.022
84. Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2017;65(1):310-335. doi: 10.1002/hep.28906
85. Stanley AJ, Laine L. Management of acute upper gastrointestinal bleeding. BMJ. 2019;364:l536. doi: 10.1136/bmj.l536
86. Al Duhailib Z, Dionne JC, Alhazzani W. Management of severe upper gastrointestinal bleeding in the ICU. Curr Opin Crit Care. 2020;26(2):212-218. doi: 10.1097/MCC.0000000000000699
87. Oakland K, et al. External validation of the Oakland score for acute lower gastrointestinal bleeding. Gut. 2020;69(9):1586-1591. doi: 10.1136/gutjnl-2019-319942
88. uropean Association for the Study of the Liver. EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure. J Hepatol. 2017;66(5):1047-1081. doi: 10.1016/j.jhep.2016.12.005
89. Lee WM, Larson AM, Stravitz RT; Acute Liver Failure Study Group. AASLD position paper: the management of acute liver failure: update 2011. Hepatology. 2012;55(3):965-967. doi: 10.1002/hep.25503
90. Olson JC, Kamath PS, et al; Society of Critical Care Medicine (SCCM). Guidelines for the Management of Adult Acute and Acute-on-Chronic Liver Failure in the ICU (Part II). Crit Care Med. 2023;51(8):1088-1104. doi: 10.1097/CCM.0000000000005990
91. Stravitz RT, Lee WM. Acute liver failure. Lancet. 2019;394(10201):869-881. doi: 10.1016/S0140-6736(19)31894-X (12)
92. Bernal W, Wendon J. Acute liver failure. N Engl J Med. 2013;369(26):2525-2534. doi: 10.1056/NEJMra1208937 (12)
93. Bernal W, Davison S, Auzinger G. Management of acute liver failure in intensive care. BJA Educ. 2021;21(5):186-192. doi: 10.1016/j.bjae.2021.01.004
94. Vege SS, Yadav D, Chari ST, et al. American College of Gastroenterology Guideline: Management of Acute Pancreatitis. Am J Gastroenterol. 2024;119(3):397-420. doi: 10.14309/ajg.0000000000002735 (13)
95. Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013 Jul-Aug;13(4 Suppl 2):e1-15. doi: 10.1016/j.pan.2013.07.063. PMID: 24054878.
96. Crockett SD, Wani S, Gardner TB, Falck-Ytter Y, Barkun AN; American Gastroenterological Association Institute Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis. Gastroenterology. 2018;154(4):1096-1101. doi: 10.1053/j.gastro.2018.01.032(13)
97. Leppäniemi A, Tolonen M, Tarasconi A, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019;14:27. doi: 10.1186/s13017-019-0247-0(13)
98. Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. Lancet. 2020;396(10252):726-734. doi: 10.1016/S0140-6736(20)31310-6 (13)
99. Forsmark CE, Vege SS, Wilcox CM. Acute Pancreatitis. N Engl J Med. 2016;375(20):1972-1981. doi: 10.1056/NEJMra1505202 (13)
100. De Waele E, Malbrain MLNG, Spapen HD. How to deal with severe acute pancreatitis in the critically ill. Curr Opin Crit Care. 2019;25(2):180-186. doi: 10.1097/MCC.0000000000000583
101. Greenberg JA, Hsu J, Bawazeer M, et al. Clinical practice guideline: management of acute pancreatitis. Can J Surg. 2016;59(2):128-140. doi: 10.1503/cjs.015015
102. Chirica M, Kelly MD, Siboni S, et al. Esophageal emergencies: WSES guidelines. World J Emerg Surg. 2019;14:26. Published 2019 May 31. doi:10.1186/s13017-019-0245-2
103. Kaman L, Iqbal J, Kundil B, Kochhar R. Management of Esophageal Perforation in Adults. Gastroenterology Res. 2010;3(6):235-244. doi:10.4021/gr263w
104. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181-1247. doi:10.1007/s00134-021-06506-y
105. Brinster CJ, Singhal S, Lee L, Marshall MB, Kaiser LR, Kucharczuk JC. Evolving options in the management of esophageal perforation. Ann Thorac Surg. 2004;77(4):1475-1483. doi:10.1016/j.athoracsur.2003.08.037
106. Eroglu A, Turkyilmaz A, Aydin Y, Yekeler E, Karaoglanoglu N. Current management of esophageal perforation: 20 years experience. Dis Esophagus. 2009;22(4):374-380. doi:10.1111/j.1442-2050.2008.00918.x
107. De Palma A, Cantatore MG, Di Gennaro F, et al. Multidisciplinary Approach in the Treatment of Descending Necrotizing Mediastinitis: Twenty-Year Single-Center Experience. Antibiotics (Basel). 2022;11(5):664. Published 2022 May 16. doi:10.3390/antibiotics11050664
108. Guarino A, Ashkenazi S, Gendrel D, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr. 2014;59(1):132-152. doi:10.1097/MPG.0000000000000375
109. Hooper L, Bunn D, Jimoh FO, Fairweather-Tait SJ. Water-loss dehydration and aging. Mech Ageing Dev. 2014;136-137:50-58. doi:10.1016/j.mad.2013.11.009
110. Shane AL, Mody RK, Crump JA, et al. 2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea. Clin Infect Dis. 2017;65(12):e45-e80. doi:10.1093/cid/cix669
111. Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335-1343. doi:10.2337/dc09-9032 (
112. Dhatariya KK; Joint British Diabetes Societies for Inpatient Care. The management of diabetic ketoacidosis in adults-An updated guideline from the Joint British Diabetes Society for Inpatient Care. Diabet Med. 2022;39(6):e14788. doi:10.1111/dme.14788 (
113. Mustafa OG, Haq M, Dashora U, Castro E, Dhatariya KK; Joint British Diabetes Societies (JBDS) for Inpatient Care Group. Management of Hyperosmolar Hyperglycaemic State (HHS) in Adults: An updated guideline from the Joint British Diabetes Societies (JBDS) for Inpatient Care Group. Diabet Med. 2023;40(3):e15005. doi:10.1111/dme.15005
114. Umpierrez G, Korytkowski M. Diabetic emergencies - ketoacidosis, hyperglycaemic hyperosmolar state and hypoglycaemia. Nat Rev Endocrinol. 2016;12(4):222-232. doi:10.1038/nrendo.2016.15 (16, 63)
115. Pasquel FJ, Umpierrez GE. Hyperosmolar hyperglycemic state: a historic review of the clinical presentation, diagnosis, and treatment. Diabetes Care. 2014;37(11):3124-3131. doi:10.2337/dc14-0984 (16, 63)
116. Dhatariya KK, Glaser NS, Codner E, Umpierrez GE. Diabetic ketoacidosis. Nat Rev Dis Primers. 2020;6(1):40. Published 2020 May 14. doi:10.1038/s41572-020-0165-1
117. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis [published correction appears in Thyroid. 2017 Nov;27(11):1462. doi: 10.1089/thy.2016.0229.correx.]. Thyroid. 2016;26(10):1343-1421. doi:10.1089/thy.2016.0229
118. Satoh T, Isozaki O, Suzuki A, et al. 2016 Guidelines for the management of thyroid storm from The Japan Thyroid Association and Japan Endocrine Society (First edition). Endocr J. 2016;63(12):1025-1064. doi:10.1507/endocrj.EJ16-0336
119. Akamizu T, Satoh T, Isozaki O, et al. Diagnostic criteria, clinical features, and incidence of thyroid storm based on nationwide surveys [published correction appears in Thyroid. 2012 Sep;22(9):979]. Thyroid. 2012;22(7):661-679. doi:10.1089/thy.2011.0334
120. Chiha M, Samarasinghe S, Kabaker AS. Thyroid storm: an updated review. J Intensive Care Med. 2015;30(3):131-140. doi:10.1177/0885066613498053
121. Carroll R, Matfin G. Endocrine and metabolic emergencies: thyroid storm. Ther Adv Endocrinol Metab. 2010;1(3):139-145. doi:10.1177/2042018810382481
122. Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the treatment of hypothyroidism: prepared by the american thyroid association task force on thyroid hormone replacement. Thyroid. 2014;24(12):1670-1751. doi:10.1089/thy.2014.0028
123. Wall CR. Myxedema coma: diagnosis and treatment. Am Fam Physician. 2000;62(11):2485-2490. (18)
124. Mathew V, Misgar RA, Ghosh S, et al. Myxedema coma: a new look into an old crisis. J Thyroid Res. 2011;2011:493462. doi:10.4061/2011/493462 (
125. Wiersinga WM. Myxedema and Coma (Severe Hypothyroidism). In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Updated 2023 Jan 11. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279007/ (18, 42)
126. Dutta P, Bhansali A, Masoodi SR, Bhadada S, Sharma N, Rajput R. Predictors of outcome in myxoedema coma: a study from a tertiary care centre. Crit Care. 2008;12(1):R1. doi:10.1186/cc6211 (18)
127. Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. doi:10.1210/jc.2015-1710
128. Rushworth RL, Torpy DJ, Falhammar H. Adrenal Crisis. N Engl J Med. 2019;381(9):852-861. doi:10.1056/NEJMra1807486
129. Annane D, Pastores SM, Arlt W, et al. Critical illness-related corticosteroid insufficiency (CIRCI): a narrative review from a Multispecialty Task Force of the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM). Intensive Care Med. 2017;43(12):1781-1792. doi:10.1007/s00134-017-4914-x
130. Hahner S, Ross RJ, Arlt W, et al. Adrenal insufficiency. Nat Rev Dis Primers. 2021;7(1):19. Published 2021 Mar 11. doi:10.1038/s41572-021-00252-7 (19)
131. Puar TH, Stikkelbroeck NM, Smans LC, Zelissen PM, Hermus AR. Adrenal Crisis: Still a Deadly Event in the 21st Century. Am J Med. 2016;129(3):339.e1-339.e3399. doi:10.1016/j.amjmed.2015.08.021
132. American Diabetes Association Professional Practice Committee . 16. Diabetes Care in the Hospital: Standards of Care in Diabetes-2025. Diabetes Care. 2025;48(Supplement_1):S321-S334. doi:10.2337/dc25-S016 (20)
133. Perez-Guzman MC, Duggan E, Gibanica S, et al. Continuous Glucose Monitoring in the Operating Room and Cardiac Intensive Care Unit. Diabetes Care. 2021;44(3):e50-e52. doi:10.2337/dc20-2386 (20)
134. Okabayashi T, Shima Y, Sumiyoshi T, et al. Intensive versus intermediate glucose control in surgical intensive care unit patients. Diabetes Care. 2014;37(6):1516-1524. doi:10.2337/dc13-1771 (20)
135. Cryer PE, Axelrod L, Grossman AB, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009;94(3):709-728. doi:10.1210/jc.2008-1410 (20)
136. Cryer PE. Hypoglycemia, functional brain failure, and brain death. J Clin Invest. 2007;117(4):868-870. doi:10.1172/JCI31669 (20, 64)
137. Umpierrez G, Korytkowski M. Diabetic emergencies - ketoacidosis, hyperglycaemic hyperosmolar state and hypoglycaemia. Nat Rev Endocrinol. 2016;12(4):222-232. doi:10.1038/nrendo.2016.15 (20)
138. Iqbal A, Heller S. Managing hypoglycaemia. Best Pract Res Clin Endocrinol Metab. 2016;30(3):413-430. doi:10.1016/j.beem.2016.06.004 (20)
139. Zeeman GG. Obstetric critical care: a blueprint for improved outcomes. Crit Care Med. 2006;34(9 Suppl):S208-S214. doi:10.1097/01.CCM.0000231884.99763.69(22,21,23, 24)
140. Pollock W, Rose L, Dennis CL. Pregnant and postpartum admissions to the intensive care unit: a systematic review. Intensive Care Med. 2010;36(9):1465-1474. doi:10.1007/s00134-010-1951-0 (22,21,23, 24)
141. Pandya ST, Mangalampally K. Critical care in obstetrics. Indian J Anaesth. 2018;62(9):724-733. doi:10.4103/ija.IJA_577_18
142. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet Gynecol. 2020;135(6):e237-e260. doi:10.1097/AOG.0000000000003891
143. Lam MTC, Dierking E. Intensive Care Unit issues in eclampsia and HELLP syndrome. Int J Crit Illn Inj Sci. 2017;7(3):136-141. doi:10.4103/IJCIIS.IJCIIS_33_17 (21)
144. Hypertension in pregnancy: diagnosis and management. London: National Institute for Health and Care Excellence (NICE); 2019 Jun 25. (NICE Guideline, No. 133.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK546004/
145. Brown MA, Magee LA, Kenny LC, et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice. Hypertension. 2018;72(1):24-43. doi:10.1161/HYPERTENSIONAHA.117.10803 (21)
146. Tranquilli AL, Dekker G, Magee L, et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens. 2014;4(2):97-104. doi:10.1016/j.preghy.2014.02.001 (21)
147. Haram K, Svendsen E, Abildgaard U. The HELLP syndrome: clinical issues and management. A Review. BMC Pregnancy Childbirth. 2009;9:8. Published 2009 Feb 26. doi:10.1186/1471-2393-9-8
148. Gabbe SG, Niebyl JR, Simpson JL, et al. Obstetrics: Normal and Problem Pregnancies. 7th ed. Elsevier; 2021:chap 31
149. Singh S, McGlennan A, England A, Simons R. A validation study of the CEMACH recommended modified early obstetric warning system (MEOWS) [published correction appears in Anaesthesia. 2012 Apr;67(4):453]. Anaesthesia. 2012;67(1):12-18. doi:10.1111/j.1365-2044.2011.06896.x
150. Committee on Obstetric Practice. Committee Opinion No. 692: Emergent Therapy for Acute-Onset, Severe Hypertension During Pregnancy and the Postpartum Period. Obstet Gynecol. 2017;129(4):e90-e95. doi:10.1097/AOG.0000000000002019 (22)
151. Duan R, Xu X, Wang X, Yu H. Perinatal outcome in women with bacterial sepsis: A cross-sectional study from West China. Medicine (Baltimore). 2019;98(44):e17751. doi:10.1097/MD.0000000000017751 (22)
152. Escobar MF, Nassar AH, Theron G, et al. FIGO recommendations on the management of postpartum hemorrhage 2022. Int J Gynaecol Obstet. 2022;157 Suppl 1(Suppl 1):3-50. doi:10.1002/ijgo.14116 (22)
153. El-Abd H, Mashhour K, Mwafy A. Clinical characteristics and outcomes of obstetric patients requiring ICU admission. Crit Care. 2011;15(Suppl 1):P513. doi:10.1186/cc9933 (22)
154. Codsi E, Rose CH, Blauwet LA. Subsequent Pregnancy Outcomes in Patients With Peripartum Cardiomyopathy. Obstet Gynecol. 2018;131(2):322-327. doi:10.1097/AOG.0000000000002439 (23)
155. Nelson-Piercy C, Dean C, Shehmar M, et al. The Management of Nausea and Vomiting in Pregnancy and Hyperemesis Gravidarum (Green-top Guideline No. 69). BJOG. 2024;131(7):e1-e30. doi:10.1111/1471-0528.17739
156. Echt DS, Liebson PR, Mitchell LB, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med. 1991;324(12):781-788. doi:10.1056/NEJM199103213241201
157. Fiorentini M, Nedu B, Dapoto F, Brunelli E, Pilu G, Youssef A. When time is brain: a systematic review about Wernicke encephalopathy as a dramatic consequence of thiamin deficiency in hyperemesis gravidarum. J Matern Fetal Neonatal Med. 2023;36(2):2223678. doi:10.1080/14767058.2023.2223678 (23)
158. Escobar MF, Nassar AH, Theron G, et al. FIGO recommendations on the management of postpartum hemorrhage 2022. Int J Gynaecol Obstet. 2022;157 Suppl 1(Suppl 1):3-50. doi:10.1002/ijgo.14116 (24)
159. Prevention and Management of Postpartum Haemorrhage: Green-top Guideline No. 52. BJOG. 2017;124(5):e106-e149. doi:10.1111/1471-0528.14178(24)
160. Gabbe SG, Niebyl JR, Simpson JL, et al. Obstetrics: Normal and Problem Pregnancies. 7th ed. Elsevier; 2021:chap 18 (24)
161. Rossaint R, Afshari A, Bouillon B, et al. The European guideline on management of major bleeding and coagulopathy following trauma: sixth edition. Crit Care. 2023;27(1):80. Published 2023 Mar 1. doi:10.1186/s13054-023-04327-7 (24)
162. Günaydın B. Management of Postpartum Haemorrhage. Turk J Anaesthesiol Reanim. 2022;50(6):396-402. doi:10.5152/TJAR.2022.21438 (24)
163. Green L, Knight M, Seeney FM, et al. The epidemiology and outcomes of women with postpartum haemorrhage requiring massive transfusion with eight or more units of red cells: a national cross-sectional study. BJOG. 2016;123(13):2164-2170. doi:10.1111/1471-0528.13831 (24)
164. Pollock W, Rose L, Dennis CL. Pregnant and postpartum admissions to the intensive care unit: a systematic review. Intensive Care Med. 2010;36(9):1465-1474. doi:10.1007/s00134-010-1951-0
165. American College of Surgeons Committee on Trauma. ATLS® Advanced Trauma Life Support® Student Course Manual. 10th ed. Chicago, IL: American College of Surgeons; 2018. (25, 26,27, 30,38, 62)
166. Carney N, Totten AM, O'Reilly C, et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery. 2017;80(1):6-15. doi:10.1227/NEU.0000000000001432 (25,27)
167. Hawryluk GWJ, Rubiano AM, Totten AM, et al. Guidelines for the Management of Severe Traumatic Brain Injury: 2020 Update of the Decompressive Craniectomy Recommendations. Neurosurgery. 2020;87(3):427-434. doi:10.1093/neuros/nyaa278 (25)
168. Yuan Q, Wu X, Sun Y, et al. Impact of intracranial pressure monitoring on mortality in patients with traumatic brain injury: a systematic review and meta-analysis. J Neurosurg. 2015;122(3):574-587. doi:10.3171/2014.10.JNS1460 (25, 45, 62)
169. Meyfroidt G, Bouzat P, Casaer MP, et al. Management of moderate to severe traumatic brain injury: an update for the intensivist [published correction appears in Intensive Care Med. 2022 Jul;48(7):989-991. doi: 10.1007/s00134-022-06759-1.]. Intensive Care Med. 2022;48(6):649-666. doi:10.1007/s00134-022-06702-4 (25)
170. Berlowitz DJ, Wadsworth B, Ross J. Respiratory problems and management in people with spinal cord injury. Breathe (Sheff). 2016;12(4):328-340. doi:10.1183/20734735.012616
171. Picetti E, Demetriades AK, Catena F, et al. Early management of adult traumatic spinal cord injury in patients with polytrauma: a consensus and clinical recommendations jointly developed by the World Society of Emergency Surgery (WSES) & the European Association of Neurosurgical Societies (EANS). World J Emerg Surg. 2024;19(1):4. Published 2024 Jan 18. doi:10.1186/s13017-023-00525-4
172. uest JD, Kelly-Hedrick M, Williamson T, et al. Development of a Systems Medicine Approach to Spinal Cord Injury. J Neurotrauma. 2023;40(17-18):1849-1877. doi:10.1089/neu.2023.0024
173. Bin-Alamer O, Bhenderu LS, Stuebe C, et al. Penetrating spinal cord injury: a systematic review and meta-analysis of clinical features and treatment outcomes. Spinal Cord. 2022;60(10):845-853. doi:10.1038/s41393-022-00813-x
174. Cadotte DW, Fehlings MG. Spinal cord injury: a systematic review of current treatment options. Clin Orthop Relat Res. 2011;469(3):732-741. doi:10.1007/s11999-010-1674-0
175. Smyth L, Bendinelli C, Lee N, et al. WSES guidelines on blunt and penetrating bowel injury: diagnosis, investigations, and treatment. World J Emerg Surg. 2022;17(1):13. Published 2022 Mar 4. doi:10.1186/s13017-022-00418-y (26,27,30)
176. Meisner M, Adina H, Schmidt J. Correlation of procalcitonin and C-reactive protein to inflammation, complications, and outcome during the intensive care unit course of multiple-trauma patients. Crit Care. 2006;10(1):R1. doi:10.1186/cc3910 (26,27,30)
177. van der Wilden GM, Velmahos GC, Emhoff T, et al. Successful nonoperative management of the most severe blunt liver injuries: a multicenter study of the research consortium of new England centers for trauma. Arch Surg. 2012;147(5):423-428. doi:10.1001/archsurg.2012.147 (26,27,30
178. Rossaint R, Afshari A, Bouillon B, et al. The European guideline on management of major bleeding and coagulopathy following trauma: sixth edition. Crit Care. 2023;27(1):80. Published 2023 Mar 1. doi:10.1186/s13054-023-04327-7(26,27,30)
179. Appelbaum RD, Farrell MS, Hoth JJ, et al. Handoffs and transitions of care in the intensive care unit: an American Association for the Surgery of Trauma Critical Care Committee clinical consensus document. Trauma Surg Acute Care Open. 2025;10(1):e001677. Published 2025 Feb 17. doi:10.1136/tsaco-2024-001677 (26,27)
180. Stassen NA, Bhullar I, Cheng JD, et al. Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S294-S300. doi:10.1097/TA.0b013e3182702afc (26,30)
181. Coccolini F, Coimbra R, Ordonez C, et al. Liver trauma: WSES 2020 guidelines. World J Emerg Surg. 2020;15(1):24. Published 2020 Mar 30. doi:10.1186/s13017-020-00302-7 (26)
182. Coccolini F, Moore EE, Kluger Y, et al. Kidney and uro-trauma: WSES-AAST guidelines. World J Emerg Surg. 2019;14:54. Published 2019 Dec 2. doi:10.1186/s13017-019-0274-x (26, 30)
183. Spahn DR, Bouillon B, Cerny V, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit Care. 2019;23(1):98. Published 2019 Mar 27. doi:10.1186/s13054-019-2347-3 (27,30)
184. Pape, H.-C., Peitzman, A. B., Rotondo, M. F., Giannoudis, P. V., & European Society for Trauma and Emergency Surgery, issuing body. (2017). Damage control management in the polytrauma patient (H.-C. Pape, A. B. Peitzman, M. F. Rotondo, & P. V. Giannoudis, Eds.; Second edition.). Springer.(27)
185. MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354(4):366-378. doi:10.1056/NEJMsa052049 (27, 30)
186. Shere-Wolfe RF, Galvagno SM Jr, Grissom TE. Critical care considerations in the management of the trauma patient following initial resuscitation. Scand J Trauma Resusc Emerg Med. 2012;20:68. Published 2012 Sep 18. doi:10.1186/1757-7241-20-68 (27)
187. Atiyeh B, Gunn SW, Dibo S. Primary triage of mass burn casualties with associated severe traumatic injuries. Ann Burns Fire Disasters. 2013;26(1):48-52. (28,99)
188. Hughes A, Almeland SK, Leclerc T, et al. Recommendations for burns care in mass casualty incidents: WHO Emergency Medical Teams Technical Working Group on Burns (WHO TWGB) 2017-2020. Burns. 2021;47(2):349-370. doi:10.1016/j.burns.2020.07.001 (28,99)
189. Shere-Wolfe RF, Galvagno SM Jr, Grissom TE. Critical care considerations in the management of the trauma patient following initial resuscitation. Scand J Trauma Resusc Emerg Med. 2012;20:68. Published 2012 Sep 18. doi:10.1186/1757-7241-20-68 (28,99)
190. Jeschke MG, van Baar ME, Choudhry MA, Chung KK, Gibran NS, Logsetty S. Burn injury. Nat Rev Dis Primers. 2020;6(1):11. Published 2020 Feb 13. doi:10.1038/s41572-020-0145-5 (28)
191. Erickson MJ, Enkhbaatar P, Lee JO. Inhalation Injury. Semin Plast Surg. 2024;38(2):93-96. Published 2024 Apr 4. doi:10.1055/s-0044-1782646 (28)
192. Pham TN, Cancio LC, Gibran NS; American Burn Association. American Burn Association practice guidelines burn shock resuscitation. J Burn Care Res. 2008;29(1):257-266. doi:10.1097/BCR.0b013e31815f3876 (28)
193. Pereira R, Buglevski M, Perdigoto R, et al. Intra-abdominal hypertension and abdominal compartment syndrome in the critically ill liver cirrhotic patient-prevalence and clinical outcomes. A multicentric retrospective cohort study in intensive care. PLoS One. 2021;16(5):e0251498. Published 2021 May 13. doi:10.1371/journal.pone.0251498 (29, 62)
194. Kawasaki Y, Kamidani R, Okada H, et al. Midline fasciotomy for severe acute pancreatitis with abdominal compartment syndrome: Case report. Ann Med Surg (Lond). 2022;79:104081. Published 2022 Jun 28. doi:10.1016/j.amsu.2022.104081 (29, 62)
195. Akrivos VS, Koutalos A, Stefanou N, Koskiniotis A, Arnaoutoglou C. Crush injury and crush syndrome: a comprehensive review. EFORT Open Rev. 2025;10(6):424-430. Published 2025 Jun 2. doi:10.1530/EOR-2025-0055
196. Wall CJ, Lynch J, Harris IA, et al. Clinical practice guidelines for the management of acute limb compartment syndrome following trauma. ANZ J Surg. 2010;80(3):151-156. doi:10.1111/j.1445-2197.2010.05213.x (29)
197. Oğuz, İ., & Şen, I. A. (2024). Analysis of patients with crush syndrome with and without intensive care requirement in the 2023 Kahramanmaraş’s earthquake: A Single-Center experience from Türkiye. Journal of Critical Care, 81,154707. https://doi.org/10.1016/j.jcrc.2024.154707 (29)
198. Abu-Zidan FM, Jawas A, Idris K, Cevik AA. Surgical and critical care management of earthquake musculoskeletal injuries and crush syndrome: A collective review. Turk J Emerg Med. 2024;24(2):67-79. Published 2024 Apr 4. doi:10.4103/tjem.tjem_11_24
199. Bielka K, Kuchyn I, Horoshko V. Intensive care units during the Ukraine war: challenges and opportunities. Intensive Care Med. 2023;49(8):1011-1014. doi:10.1007/s00134-023-07117-5 (30)
200. Cannon JW, Khan MA, Raja AS, et al. Damage control resuscitation in patients with severe traumatic hemorrhage: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2017;82(3):605-617. doi:10.1097/TA.0000000000001333 (30)
201. Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):775-787. doi:10.1001/jama.2016.0289)
202. ProCESS Investigators, Yealy DM, Kellum JA, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370(18):1683-1693. doi:10.1056/NEJMoa1401602
203. Levy MM, Evans LE, Rhodes A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Med. 2018;44(6):925-928. doi:10.1007/s00134-018-5085-0
204. Angus DC, van der Poll T. Severe sepsis and septic shock [published correction appears in N Engl J Med. 2013 Nov 21;369(21):2069]. N Engl J Med. 2013;369(9):840-851. doi:10.1056/NEJMra1208623
205. Luks AM, Auerbach PS, Freer L, et al. Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Acute Altitude Illness: 2019 Update. Wilderness Environ Med. 2019;30(4S):S3-S18. doi:10.1016/j.wem.2019.04.006 (32)
206. Lott C, Truhlář A, Alfonzo A, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances [published correction appears in Resuscitation. 2021 Oct;167:91-92. doi: 10.1016/j.resuscitation.2021.08.012.]. Resuscitation. 2021;161:152-219. doi:10.1016/j.resuscitation.2021.02.011 (32)
207. Hackett PH, Roach RC. High-altitude illness. N Engl J Med. 2001;345(2):107-114. doi:10.1056/NEJM200107123450206 (32)
208. Stream JO, Grissom CK. Update on high-altitude pulmonary edema: pathogenesis, prevention, and treatment. Wilderness Environ Med. 2008;19(4):293-303. doi:10.1580/07-WEME-REV-173.1 (32)
209. Moon RE. Hyperbaric treatment of air or gas embolism: current recommendations. Undersea Hyperb Med. 2019;46(5):673-683.(32)
210. Vann RD, Butler FK, Mitchell SJ, Moon RE. Decompression illness. Lancet. 2011;377(9760):153-164. doi:10.1016/S0140-6736(10)61085-9 (32)
211. Schmidt AC, Sempsrott JR, Hawkins SC, Arastu AS, Cushing TA, Auerbach PS. Wilderness Medical Society Clinical Practice Guidelines for the Treatment and Prevention of Drowning: 2019 Update. Wilderness Environ Med. 2019;30(4S):S70-S86. doi:10.1016/j.wem.2019.06.007 (32)
212. Matsumoto H, Takeba J, Umakoshi K, et al. Successful treatment for disseminated intravascular coagulation (DIC) corresponding to phenotype changes in a heat stroke patient. J Intensive Care. 2019;7:2. Published 2019 Jan 15. doi:10.1186/s40560-019-0359-3 (32)
213. Zilberberg MD, Epstein SK. Acute lung injury in the medical ICU: comorbid conditions, age, etiology, and hospital outcome. Am J Respir Crit Care Med. 1998;157(4 Pt 1):1159-1164. doi:10.1164/ajrccm.157.4.9704088 (32)
214. Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301-1308. doi:10.1056/NEJM200005043421801 (32)
215. Lang HJ, Amito J, Dünser MW, Giera R, Towey R. Intensive-care management of snakebite victims in rural sub-Saharan Africa: An experience from Uganda. South Afr J Crit Care. 2020;36(1):10.7196/SAJCC.2020.v36i1.404. Published 2020 Jul 30. doi:10.7196/SAJCC.2020.v36i1.404 (33)
216. Al Abri S, Al Rumhi M, Al Mahruqi G, Shakir AS. Scorpion Sting Management at Tertiary and Secondary Care Emergency Departments. Oman Med J. 2019;34(1):9-13. doi:10.5001/omj.2019.02 (33)
217. Bosnak M, Levent Yilmaz H, Ece A, et al. Severe scorpion envenomation in children: Management in pediatric intensive care unit. Hum Exp Toxicol. 2009;28(11):721-728. doi:10.1177/0960327109350667 (33)
218. Reis MB, Arantes EC. Immunosuppressive therapies in scorpion envenomation: new perspectives for treatment. Front Toxicol. 2024;6:1503055. Published 2024 Nov 19. doi:10.3389/ftox.2024.1503055 (33)
219. Godoy DA, Badenes R, Seifi S, Salehi S, Seifi A. Neurological and Systemic Manifestations of Severe Scorpion Envenomation. Cureus. 2021;13(4):e14715. Published 2021 Apr 27. doi:10.7759/cureus.14715 (33)
220. Baseer KA, Naser MAA. Predictors for Mortality in Children with Scorpion Envenomation Admitted to Pediatric Intensive Care Unit, Qena Governorate, Egypt. Am J Trop Med Hyg. 2019;101(4):941-945. doi:10.4269/ajtmh.19-0319 (33)
221. Boyer LV, Theodorou AA, Berg RA, et al. Antivenom for critically ill children with neurotoxicity from scorpion stings. N Engl J Med. 2009;360(20):2090-2098. doi:10.1056/NEJMoa0808455 (33)
222. Sarker, S. K., Salim, M., Hossain, M. M., & Mandal, B. K. (2022). Snake Envenomation in the Intensive Care Unit of a Tertiary Care Hospital, Dhaka, Bangladesh: A Prospective Cohort Study. Journal of Current and Advance Medical Research, 9(1), 48–55. https://doi.org/10.3329/jcamr.v9i1.59745 (33)
223. Carvalho J, Moinho R, Macao P, Oliveira G. When snakebites complicate: a paediatric case with shock and compartment syndrome. BMJ Case Rep. 2021;14(2):e240206. Published 2021 Feb 9. doi:10.1136/bcr-2020-240206 (33)
224. Matthay MA, Thompson BT, Ware LB. The Berlin definition of acute respiratory distress syndrome: should patients receiving high-flow nasal oxygen be included?. Lancet Respir Med. 2021;9(8):933-936. doi:10.1016/S2213-2600(21)00105-3 (35,61)
225. ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669 (35,61)
226. Liapikou A, Ferrer M, Polverino E, et al. Severe community-acquired pneumonia: validation of the Infectious Diseases Society of America/American Thoracic Society guidelines to predict an intensive care unit admission. Clin Infect Dis. 2009;48(4):377-385. doi:10.1086/596307 (35, 61)
227. Phua J, Ngerng WJ, Lim TK. The impact of a delay in intensive care unit admission for community-acquired pneumonia. Eur Respir J. 2010;36(4):826-833. doi:10.1183/09031936.00154209 (35, 61)
228. Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301-1308. doi:10.1056/NEJM200005043421801 ) 35, 61)
229. Anesi GL, Liu VX, Chowdhury M, et al. Association of ICU Admission and Outcomes in Sepsis and Acute Respiratory Failure. Am J Respir Crit Care Med. 2022;205(5):520-528. doi:10.1164/rccm.202106-1350OC (35, 61)
230. Zirpe KG, Tiwari AM, Gurav SK, et al. Timing of Invasive Mechanical Ventilation and Mortality among Patients with Severe COVID-19-associated Acute Respiratory Distress Syndrome. Indian J Crit Care Med. 2021;25(5):493-498. doi:10.5005/jp-journals-10071-23816 (35, 61)
231. McDonough G, Khaing P, Treacy T, McGrath C, Yoo EJ. The Use of High-Flow Nasal Oxygen in the ICU as a First-Line Therapy for Acute Hypoxemic Respiratory Failure Secondary to Coronavirus Disease 2019. Crit Care Explor. 2020;2(10):e0257. Published 2020 Oct 16. doi:10.1097/CCE.0000000000000257 (35)
232. Camporota, L., Meadows, C., Ledot, S., Scott, I., Harvey, C., Garcia, M., & Vuylsteke, A. (2021). Consensus on the referral and admission of patients with severe respiratory failure to the NHS ECMO service. The Lancet Respiratory Medicine, 9(2), e16-e17. (35)
233. Hendrickson KW, Peltan ID, Brown SM. The Epidemiology of Acute Respiratory Distress Syndrome Before and After Coronavirus Disease 2019. Crit Care Clin. 2021;37(4):703-716. doi:10.1016/j.ccc.2021.05.001 (35)
234. Zhao L, Su F, Zhang N, et al. The impact of the new acute respiratory distress syndrome (ARDS) criteria on Berlin criteria ARDS patients: a multicenter cohort study [published correction appears in BMC Med. 2024 Nov 9;22(1):515. doi: 10.1186/s12916-024-03750-z.]. BMC Med. 2023;21(1):456. Published 2023 Nov 23. doi:10.1186/s12916-023-03144-7 (35)
235. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543-603. doi:10.1093/eurheartj/ehz405 (36)
236. Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association [published correction appears in Circulation. 2012 Aug 14;126(7):e104] [published correction appears in Circulation. 2012 Mar 20;125(11):e495]. Circulation. 2011;123(16):1788-1830. doi:10.1161/CIR.0b013e318214914f (36)
237. Meyer G, Vicaut E, Danays T, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-1411. doi:10.1056/NEJMoa1302097 (36)
238. Konstantinides SV, Torbicki A, Agnelli G, et al. 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism [published correction appears in Eur Heart J. 2015 Oct 14;36(39):2666. doi: 10.1093/eurheartj/ehv131.] [published correction appears in Eur Heart J. 2015 Oct 14;36(39):2642. doi: 10.1093/eurheartj/ehu479.]. Eur Heart J. 2014;35(43):3033-3069k. doi:10.1093/eurheartj/ehu283 (36)
239. Charya AV, Holden VK, Pickering EM. Management of life-threatening hemoptysis in the ICU. J Thorac Dis. 2021;13(8):5139-5158. doi:10.21037/jtd-19-3991 (37)
240. O'Gurek D, Choi HYJ. Hemoptysis: Evaluation and Management. Am Fam Physician. 2022;105(2):144-151. (37)
241. Atchinson PRA, Hatton CJ, Roginski MA, Backer ED, Long B, Lentz SA. The emergency department evaluation and management of massive hemoptysis. Am J Emerg Med. 2021;50:148-155. doi:10.1016/j.ajem.2021.07.041 (37)
242. Ong TH, Eng P. Massive hemoptysis requiring intensive care. Intensive Care Med. 2003;29(2):317-320. doi:10.1007/s00134-002-1553-6 (37)
243. Lordan JL, Gascoigne A, Corris PA. The pulmonary physician in critical care * Illustrative case 7: Assessment and management of massive haemoptysis. Thorax. 2003;58(9):814-819. doi:10.1136/thorax.58.9.814 (37)
244. Gagnon S, Quigley N, Dutau H, Delage A, Fortin M. Approach to Hemoptysis in the Modern Era. Can Respir J. 2017;2017:1565030. doi:10.1155/2017/1565030 (37)
245. Roberts DJ, Leigh-Smith S, Faris PD, et al. Clinical Presentation of Patients With Tension Pneumothorax: A Systematic Review. Ann Surg. 2015;261(6):1068-1078. doi:10.1097/SLA.0000000000001073 (38)
246. Roberts DJ, Leigh-Smith S, Faris PD, et al. Clinical Presentation of Patients With Tension Pneumothorax: A Systematic Review. Ann Surg. 2015;261(6):1068-1078. doi:10.1097/SLA.0000000000001073 (38)
247. Leigh-Smith S, Harris T. Tension pneumothorax--time for a re-think?. Emerg Med J. 2005;22(1):8-16. doi:10.1136/emj.2003.010421 (38)
248. Thachuthara-George J. Pneumothorax in patients with respiratory failure in ICU. J Thorac Dis. 2021;13(8):5195-5204. doi:10.21037/jtd-19-3752 (38)
249. Zarogoulidis P, Kioumis I, Pitsiou G, et al. Pneumothorax: from definition to diagnosis and treatment. J Thorac Dis. 2014;6(Suppl 4):S372-S376. doi:10.3978/j.issn.2072-1439.2014.09.2 (38)
250. de Lassence A, Timsit JF, Tafflet M, et al. Pneumothorax in the intensive care unit: incidence, risk factors, and outcome. Anesthesiology. 2006;104(1):5-13. doi:10.1097/00000542-200601000-00003 (38)
251. Ball CG, Kirkpatrick AW, Feliciano DV. The occult pneumothorax: what have we learned?. Can J Surg. 2009;52(5):E173-E179. (38)
252. Hooper C, Lee YC, Maskell N; BTS Pleural Guideline Group. Investigation of a unilateral pleural effusion in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65 Suppl 2:ii4-ii17. doi:10.1136/thx.2010.136978 (39)
253. Bateman M, Alkhatib A, John T, Parikh M, Kheir F. Pleural Effusion Outcomes in Intensive Care: Analysis of a Large Clinical Database. J Intensive Care Med. 2020;35(1):48-54. doi:10.1177/0885066619872449 (39)
254. Feller-Kopman DJ, Reddy CB, DeCamp MM, et al. Management of Malignant Pleural Effusions. An Official ATS/STS/STR Clinical Practice Guideline. Am J Respir Crit Care Med. 2018;198(7):839-849. doi:10.1164/rccm.201807-1415ST (39)
255. Maslove DM, Chen BT, Wang H, Kuschner WG. The diagnosis and management of pleural effusions in the ICU. J Intensive Care Med. 2013;28(1):24-36. doi:10.1177/0885066611403264 (39)
256. Walden AP, Jones QC, Matsa R, Wise MP. Pleural effusions on the intensive care unit; hidden morbidity with therapeutic potential. Respirology. 2013;18(2):246-254. doi:10.1111/j.1440-1843.2012.02279.x (39)
257. Bediwy AS, Al-Biltagi M, Saeed NK, Bediwy HA, Elbeltagi R. Pleural effusion in critically ill patients and intensive care setting. World J Clin Cases. 2023;11(5):989-999. doi:10.12998/wjcc.v11.i5.989 (39)
258. Azoulay E. Pleural effusions in the intensive care unit. Curr Opin Pulm Med. 2003;9(4):291-297. doi:10.1097/00063198-200307000-00008 (39)
259. Janmeja, A.K.; Mohapatra, P. R.; Saini, M. S.; Khurana, A.. REEXPANSION PULMONARY EDEMA- A CASE REPORT. Lung India 24(2):p 72-74, Apr–Jun 2007. | DOI: 10.4103/0970-2113.44217 (39)
260. Mattison LE, Coppage L, Alderman DF, Herlong JO, Sahn SA. Pleural effusions in the medical ICU: prevalence, causes, and clinical implications. Chest. 1997;111(4):1018-1023. doi:10.1378/chest.111.4.1018 (39)
261. Jany B, Welte T. Pleural Effusion in Adults-Etiology, Diagnosis, and Treatment. Dtsch Arztebl Int. 2019;116(21):377-386. doi:10.3238/arztebl.2019.0377 (39)
262. Rochwerg B, Brochard L, Elliott MW, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017;50(2):1602426. Published 2017 Aug 31. doi:10.1183/13993003.02426-2016 (40,41,54,61)
263. Osadnik CR, Tee VS, Carson-Chahhoud KV, Picot J, Wedzicha JA, Smith BJ. Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;7(7):CD004104. Published 2017 Jul 13. (40, 61)
264. Talbot T, Roe T, Dushianthan A. Management of Acute Life-Threatening Asthma Exacerbations in the Intensive Care Unit. Applied Sciences. 2024; 14(2):693. https://doi.org/10.3390/app14020693 (40)
265. Gayen S, Dachert S, Lashari BH, et al. Critical Care Management of Severe Asthma Exacerbations. J Clin Med. 2024;13(3):859. Published 2024 Feb 1. doi:10.3390/jcm13030859 (40)
266. Watson AJR, Roe T, Arscott O, Thomas C, Ward J, Beecham R, Browning D, Saeed K, Dushianthan A. Characteristics, Management, and Outcomes of Acute Life-Threatening Asthma in Adult Intensive Care. Clinics and Practice. 2024; 14(5):1886-1897. https://doi.org/10.3390/clinpract14050149 (40)
267. Agusti A, Vogelmeier CF. GOLD 2024: a brief overview of key changes. J Bras Pneumol. 2023;49(6):e20230369. Published 2023 Dec 22. doi:10.36416/1806-3756/e20230369 (40)
268. Papiris S, Kotanidou A, Malagari K, Roussos C. Clinical review: severe asthma. Crit Care. 2002;6(1):30-44. doi:10.1186/cc1451
269. Talbot T, Roe T, Dushianthan A. Management of Acute Life-Threatening Asthma Exacerbations in the Intensive Care Unit. Applied Sciences. 2024; 14(2):693. https://doi.org/10.3390/app14020693
270. Laksono, Sidhi1,2; Angkasa, Irwan Surya3. Dyspnea in Emergency Settings: Up-to-date Diagnosing and Management in the Emergency Department. Current Medical Issues 22(1):p 37-44, Jan–Mar 2024. | DOI: 10.4103/cmi.cmi_117_23 (41)
271. DeVos E, Jacobson L. Approach to Adult Patients with Acute Dyspnea. Emerg Med Clin North Am. 2016;34(1):129-149. doi:10.1016/j.emc.2015.08.008 (41)
272. Smith GB, Prytherch DR, Meredith P, Schmidt PE, Featherstone PI. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation. 2013;84(4):465-470. doi:10.1016/j.resuscitation.2012.12.016
273. Duyu M, Karakaya Altun Z, Yildiz S. Nontraumatic coma in the pediatric intensive care unit: etiology, clinical characteristics and outcome. Turk J Med Sci. 2021;51(1):214-223. Published 2021 Feb 26. doi:10.3906/sag-2004-330 (42)
274. Nolan JP, Sandroni C, Böttiger BW, et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med. 2021;47(4):369-421. doi:10.1007/s00134-021-06368-4 (42)
275. Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335-1343. doi:10.2337/dc09-9032 (42)
276. Horsting MW, Franken MD, Meulenbelt J, van Klei WA, de Lange DW. The etiology and outcome of non-traumatic coma in critical care: a systematic review. BMC Anesthesiol. 2015;15:65. Published 2015 Apr 29. doi:10.1186/s12871-015-0041-9 (42)
277. Wijdicks EF, Bamlet WR, Maramattom BV, Manno EM, McClelland RL. Validation of a new coma scale: The FOUR score. Ann Neurol. 2005;58(4):585-593. doi:10.1002/ana.20611 (42)
278. Sandroni C, Cronberg T, Sekhon M. Brain injury after cardiac arrest: pathophysiology, treatment, and prognosis. Intensive Care Med. 2021;47(12):1393-1414. doi:10.1007/s00134-021-06548-2 (42)
279. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association [published correction appears in Stroke. 2019 Dec;50(12):e440-e441. doi: 10.1161/STR.0000000000000215.]. Stroke. 2019;50(12):e344-e418. doi:10.1161/STR.0000000000000211 (43, 44,45)
280. Hemphill JC 3rd, Greenberg SM, Anderson CS, et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2015;46(7):2032-2060. doi:10.1161/STR.0000000000000069 (43, 44,45)
281. Connolly ES Jr, Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012;43(6):1711-1737. doi:10.1161/STR.0b013e3182587839 (43, 44,45)
282. Omar WM, Khader IRA, Hani SB, ALBashtawy M. The Glasgow Coma Scale and Full Outline of Unresponsiveness score evaluation to predict patient outcomes with neurological illnesses in intensive care units in West Bank: a prospective cross-sectional study. Acute Crit Care. 2024;39(3):408-419. doi:10.4266/acc.2024.00570 (43)
283. Musick S, Alberico A. Neurologic Assessment of the Neurocritical Care Patient. Front Neurol. 2021;12:588989. Published 2021 Mar 22. doi:10.3389/fneur.2021.588989 (43)
284. Kramer AH, Zygun DA. Do neurocritical care units save lives? Measuring the impact of specialized ICUs. Neurocrit Care. 2011;14(3):329-333. doi:10.1007/s12028-011-9530-y
285. Steiner T, Purrucker JC, Aguiar de Sousa D, et al. European Stroke Organisation (ESO) and European Association of Neurosurgical Societies (EANS) guideline on stroke due to spontaneous intracerebral haemorrhage. Eur Stroke J. Published online May 22, 2025. doi:10.1177/23969873251340815 (44)
286. Berge E, Whiteley W, Audebert H, et al. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur Stroke J. 2021;6(1):I-LXII. doi:10.1177/2396987321989865 (44)
287. Sandset EC, Anderson CS, Bath PM, et al. European Stroke Organisation (ESO) guidelines on blood pressure management in acute ischaemic stroke and intracerebral haemorrhage. Eur Stroke J. 2021;6(2):XLVIII-LXXXIX. doi:10.1177/23969873211012133
288. An SJ, Kim TJ, Yoon BW. Epidemiology, Risk Factors, and Clinical Features of Intracerebral Hemorrhage: An Update. J Stroke. 2017;19(1):3-10. doi:10.5853/jos.2016.00864 (44,45)
289. Stroke Unit Trialists' Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database Syst Rev. 2013;2013(9):CD000197. Published 2013 Sep 11. doi:10.1002/14651858.CD000197.pub3 (44, 45)
290. Moughal S, Trippier S, Al-Mousa A, et al. Strokectomy for malignant middle cerebral artery infarction: experience and meta-analysis of current evidence. J Neurol. 2022;269(1):149-158. doi:10.1007/s00415-020-10358-9
291. Cook AM, Morgan Jones G, Hawryluk GWJ, et al. Guidelines for the Acute Treatment of Cerebral Edema in Neurocritical Care Patients. Neurocrit Care. 2020;32(3):647-666. doi:10.1007/s12028-020-00959-7 (45,46)
292. Latifi AN, Gopal V, Raissi S. Focal Neurological Deficit Secondary to Severe Hyponatraemia Mimicking Stroke. Eur J Case Rep Intern Med. 2019;6(10):001244. Published 2019 Oct 11. doi:10.12890/2019_001244 (45)
293. Deshpande HH, Jagiasi BG, Thorat SS. Approach to focal neurological deficit. In: Deshpande HH, Jagiasi BG, Thorat SS, eds. Manual of Neurocritical Care. Jaypee Brothers Medical Publishers; 2023:130. (45)
294. van Doorn PA, Van den Bergh PYK, Hadden RDM, et al. European Academy of Neurology/Peripheral Nerve Society Guideline on diagnosis and treatment of Guillain-Barré syndrome. Eur J Neurol. 2023;30(12):3646-3674. doi:10.1111/ene.16073
295. Wiendl H, Abicht A, Chan A, et al. Guideline for the management of myasthenic syndromes [published correction appears in Ther Adv Neurol Disord. 2024 Apr 30;17:17562864241246400. doi: 10.1177/17562864241246400.]. Ther Adv Neurol Disord. 2023;16:17562864231213240. Published 2023 Dec 26. doi:10.1177/17562864231213240
296. Wendell LC, Levine JM. Myasthenic crisis. Neurohospitalist. 2011;1(1):16-22. doi:10.1177/1941875210382918 (50)
297. Bellanti R, Rinaldi S. Guillain-Barré syndrome: a comprehensive review. Eur J Neurol. 2024;31(8):e16365. doi:10.1111/ene.16365 (50)
298. Pritchard J. Guillain-Barré syndrome. Clin Med (Lond). 2010;10(4):399-401. doi:10.7861/clinmedicine.10-4-399 (50)
299. Walgaard C, Lingsma HF, Ruts L, et al. Prediction of respiratory insufficiency in Guillain-Barré syndrome. Ann Neurol. 2010;67(6):781-787. doi:10.1002/ana.21976 (50)
300. Leonhard SE, Mandarakas MR, Gondim FAA, et al. Diagnosis and management of Guillain-Barré syndrome in ten steps. Nat Rev Neurol. 2019;15(11):671-683. doi:10.1038/s41582-019-0250-9 (50)
301. Costa Oliveira, D., Xavier Pires, S., Santos, A. (2023). The Approach to a Patient with a Myasthenic Crisis in an Intensive Care Unit. In: Pérez-Torres, D., Martínez-Martínez, M., Schaller, S.J. (eds) Best 2022 Clinical Cases in Intensive Care Medicine. Lessons from the ICU. Springer, Cham. https://doi.org/10.1007/978-3-031-36398-6_60 (50)
302. Sanders DB, Wolfe GI, Benatar M, et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology. 2016;87(4):419-425. doi:10.1212/WNL.0000000000002790 (50)
303. Hughes RA, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barré syndrome. Cochrane Database Syst Rev. 2014;2014(9):CD002063. Published 2014 Sep 19. doi:10.1002/14651858.CD002063.pub6 (50)
304. Narayanaswami P, Sanders DB, Wolfe G, et al. International Consensus Guidance for Management of Myasthenia Gravis: 2020 Update. Neurology. 2021;96(3):114-122. doi:10.1212/WNL.0000000000011124 (50)
305. van de Beek D, Cabellos C, Dzupova O, et al. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clin Microbiol Infect. 2016;22 Suppl 3:S37-S62. doi:10.1016/j.cmi.2016.01.007 (46)
306. El-Hajj VG, Pettersson I, Gharios M, et al. Detection and Management of Elevated Intracranial Pressure in the Treatment of Acute Community-Acquired Bacterial Meningitis: A Systematic Review. Neurocrit Care. 2024;41(1):228-243. doi:10.1007/s12028-023-01937-5
307. Glimåker M, Johansson B, Grindborg Ö, Bottai M, Lindquist L, Sjölin J. Adult bacterial meningitis: earlier treatment and improved outcome following guideline revision promoting prompt lumbar puncture. Clin Infect Dis. 2015;60(8):1162-1169. doi:10.1093/cid/civ011
308. Moller K, Skinhoj P. Guidelines for managing acute bacterial meningitis. BMJ. 2000;320(7245):1290. doi:10.1136/bmj.320.7245.1290
309. Sonneville R, de Montmollin E, Contou D, et al.
Clinical features, etiologies, and outcomes in adult patients with
meningoencephalitis requiring intensive care (EURECA): an international prospective
multicenter cohort study [published correction appears in Intensive Care Med.
2025 Feb;51(2):454-455. doi: 10.1007/s00134-025-07792-6.]. Intensive
Care Med. 2023;49(5):517-529. doi:10.1007/s00134-023-07032-9
(46)
310. Valdoleiros SR, Torrão C, Freitas LS, Mano D, Gonçalves C, Teixeira C. Nosocomial meningitis in intensive care: a 10-year retrospective study and literature review. Acute Crit Care. 2022;37(1):61-70. doi:10.4266/acc.2021.01151 (46)
311. Jaubert P, Charpentier J, Benghanem S, et al. Meningitis in critically ill patients admitted to intensive care unit for severe community-acquired pneumococcal pneumonia. Ann Intensive Care. 2023;13(1):129. Published 2023 Dec 18. doi:10.1186/s13613-023-01211-z (46)
312. Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis. 2004;39(9):1267-1284. doi:10.1086/425368 (45)
313. Tunkel AR, Hasbun R, Bhimraj A, et al. 2017 Infectious Diseases Society of America's Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin Infect Dis. 2017;64(6):e34-e65. doi:10.1093/cid/ciw861 (46)
314. Guillem L, Hernández-Pérez G, Berbel D, Pelegrín I, Falip M, Cabellos C. Seizure prophylaxis in pneumococcal meningitis, cohort study. Epilepsia Open. 2024;9(6):2319-2330. doi:10.1002/epi4.13054 (46)
315. van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M. Clinical features and prognostic factors in adults with bacterial meningitis [published correction appears in N Engl J Med. 2005 Mar 3;352(9):950]. N Engl J Med. 2004;351(18):1849-1859. doi:10.1056/NEJMoa040845 (46)
316. de Gans J, van de Beek D; European Dexamethasone in Adulthood Bacterial Meningitis Study Investigators. Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347(20):1549-1556. doi:10.1056/NEJMoa021334 (46)
317. Brophy GM, Bell R, Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17(1):3-23. doi:10.1007/s12028-012-9695-z (47)
318. Glauser T, Shinnar S, Gloss D, et al. Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society. Epilepsy Curr. 2016;16(1):48-61. doi:10.5698/1535-7597-16.1.48 (47)
319. Claassen J, Goldstein JN. Emergency Neurological Life Support: Status Epilepticus. Neurocrit Care. 2017;27(Suppl 1):152-158. doi:10.1007/s12028-017-0460-1 (47)
320. Wang X, Yang F, Chen B, Jiang W. Non-convulsive seizures and non-convulsive status epilepticus in neuro-intensive care unit. Acta Neurol Scand. 2022;146(6):752-760. doi:10.1111/ane.13718 (47)
321. Brophy GM, Bell R, Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17(1):3-23. doi:10.1007/s12028-012-9695-z (47)
322. Sutter R, Rüegg S, Kaplan PW. Epidemiology, diagnosis, and management of nonconvulsive status epilepticus: Opening Pandora's box. Neurol Clin Pract. 2012;2(4):275-286. doi:10.1212/CPJ.0b013e318278be75 (47)
323. Claassen, J., Riviello, J.J. & Silbergleit, R. Emergency Neurological Life Support: Status Epilepticus. Neurocrit Care 23 (Suppl 2), 136–142 (2015). https://doi.org/10.1007/s12028-015-0172-3 (47)
324. Laccheo I, Sonmezturk H, Bhatt AB, et al. Non-convulsive status epilepticus and non-convulsive seizures in neurological ICU patients. Neurocrit Care. 2015;22(2):202-211. doi:10.1007/s12028-014-0070-0 (47)
325. LaRoche, S.M., Haider, H.A. (2018). The Management of Nonconvulsive Status Epilepticus in Adults. In: Drislane, F., Kaplan MBBS, P. (eds) Status Epilepticus. Current Clinical Neurology. Springer, Cham. https://doi.org/10.1007/978-3-319-58200-9_24
326. Bermeo-Ovalle A. Pick Your Poison but Pick It Wisely: Choosing a Second-Line Medication for the Management of Status Epilepticus. Epilepsy Curr. 2020;20(5):278-281. Published 2020 Sep 2. doi:10.1177/1535759720949252 (47)
327. Treiman DM, Meyers PD, Walton NY, et al. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. 1998;339(12):792-798. doi:10.1056/NEJM199809173391202 (47)
328. Kapur J, Elm J, Chamberlain JM, et al. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus. N Engl J Med. 2019;381(22):2103-2113. doi:10.1056/NEJMoa1905795 (47)
329. Apfelbaum JL, Silverstein JH, Chung FF, et al. Practice guidelines for postanesthetic care: an updated report by the American Society of Anesthesiologists Task Force on Postanesthetic Care. Anesthesiology. 2013;118(2):291-307.
330. Aldecoa C, Bettelli G, Bilotta F, et al. Update of the European Society of Anaesthesiology and Intensive Care Medicine evidence-based and consensus-based guideline on postoperative delirium in adult patients. Eur J Anaesthesiol. 2024;41(2):81-108. doi:10.1097/EJA.0000000000001876
331. Lavezzo B, Biancofiore G, Luca E, et al. Planning intensive care unit admission after elective major abdominal surgery: good clinical practice document by SIAARTI-SIC-ANIARTI. J Anesth Analg Crit Care. 2025;5(1):20. Published 2025 Apr 14. doi:10.1186/s44158-025-00239-w (48)
332. Ylimartimo AT, Koskela M, Lahtinen S, Kaakinen T, Vakkala M, Liisanantti J. Outcomes in patients requiring intensive care unit (ICU) admission after emergency laparotomy: A retrospective study. Acta Anaesthesiol Scand. 2022;66(8):954-960. doi:10.1111/aas.14103 (48)
333. Ohbe H, Matsui H, Kumazawa R, Yasunaga H. Intensive care unit versus high dependency care unit admission after emergency surgery: a nationwide in-patient registry study. Br J Anaesth. 2022;129(4):527-535. doi:10.1016/j.bja.2022.06.030 (48, 49)
334. Apfelbaum JL, Silverstein JH, Chung FF, et al. Practice guidelines for postanesthetic care: an updated report by the American Society of Anesthesiologists Task Force on Postanesthetic Care. Anesthesiology. 2013;118(2):291-307. doi:10.1097/ALN.0b013e31827773e9 (48)
335. Haller G, Myles PS, Wolfe R, Weeks AM, Stoelwinder J, McNeil J. Validity of unplanned admission to an intensive care unit as a measure of patient safety in surgical patients. Anesthesiology. 2005;103(6):1121-1129. doi:10.1097/00000542-200512000-00004 (48)
336. Gillies MA, Power GS, Harrison DA, et al. Regional variation in critical care provision and outcome after high-risk surgery. Intensive Care Med. 2015;41(10):1809-1816. doi:10.1007/s00134-015-3980-1 (49)
337. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179-c184. doi:10.1159/000339789
338. Gong K, Lee HK, Yu K, Xie X, Li J. A prediction and interpretation framework of acute kidney injury in critical care. J Biomed Inform. 2021;113:103653. doi:10.1016/j.jbi.2020.103653 (51)
339. Chen WY, Cai LH, Zhang ZH, et al. The timing of continuous renal replacement therapy initiation in sepsis-associated acute kidney injury in the intensive care unit: the CRTSAKI Study (Continuous RRT Timing in Sepsis-associated AKI in ICU): study protocol for a multicentre, randomised controlled trial. BMJ Open. 2021;11(2):e040718. Published 2021 Feb 19. doi:10.1136/bmjopen-2020-040718
340. Santos PR, Monteiro DL. Acute kidney injury in an intensive care unit of a general hospital with emergency room specializing in trauma: an observational prospective study. BMC Nephrol. 2015;16:30. Published 2015 Mar 19. doi:10.1186/s12882-015-0026-4 (51)
341. Abd ElHafeez S, Tripepi G, Quinn R, et al. Risk, Predictors, and Outcomes of Acute Kidney Injury in Patients Admitted to Intensive Care Units in Egypt. Sci Rep. 2017;7(1):17163. Published 2017 Dec 7. doi:10.1038/s41598-017-17264-7
342. Hoste EA, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411-1423. doi:10.1007/s00134-015-3934-7
343. Pickkers P, Darmon M, Hoste E, et al. Acute kidney injury in the critically ill: an updated review on pathophysiology and management. Intensive Care Med. 2021;47(8):835-850. doi:10.1007/s00134-021-06454-7
344. Naka T, Bellomo R. Bench-to-bedside review: treating acid-base abnormalities in the intensive care unit--the role of renal replacement therapy. Crit Care. 2004;8(2):108-114. doi:10.1186/cc2821
345. Achanti A, Szerlip HM. Acid-Base Disorders in the Critically Ill Patient. Clin J Am Soc Nephrol. 2023;18(1):102-112. doi:10.2215/CJN.04500422 (52)
346. Chua HR, Schneider A, Bellomo R. Bicarbonate in diabetic ketoacidosis - a systematic review. Ann Intensive Care. 2011;1(1):23. Published 2011 Jul 6. doi:10.1186/2110-5820-1-23 (52)
347. Barletta JF, Muir J, Brown J, Dzierba A. A Systematic Approach to Understanding Acid-Base Disorders in the Critically Ill. Ann Pharmacother. 2024;58(1):65-75. doi:10.1177/10600280231165787
348. Jaber S, Paugam C, Futier E, et al. Sodium bicarbonate therapy for patients with severe metabolic acidaemia in the intensive care unit (BICAR-ICU): a multicentre, open-label, randomised controlled, phase 3 trial [published correction appears in Lancet. 2018 Dec 8;392(10163):2440. doi: 10.1016/S0140-6736(18)33040-X.]. Lancet. 2018;392(10141):31-40. doi:10.1016/S0140-6736(18)31080-8
349. Cerdá J, Tolwani AJ, Warnock DG. Critical care nephrology: management of acid-base disorders with CRRT. Kidney Int. 2012;82(1):9-18. doi:10.1038/ki.2011.243 (51,52)
350. Sithole N, Lalla U, Davids MR, Chothia MY. The frequency of acid-base disorders on admission to the intensive care and its association with in-hospital outcome, Cape Town, South Africa: a retrospective cohort study. Pan Afr Med J. 2022;42:130. Published 2022 Jun 16. doi:10.11604/pamj.2022.42.130.32570
351. Jung B, Rimmele T, Le Goff C, et al. Severe metabolic or mixed acidemia on intensive care unit admission: incidence, prognosis and administration of buffer therapy. A prospective, multiple-center study. Crit Care. 2011;15(5):R238. doi:10.1186/cc10487
352. Montague BT, Ouellette JR, Buller GK. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol. 2008;3(2):324-330. doi:10.2215/CJN.04611007
353. Soar J, Perkins GD, Abbas G, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution. Resuscitation. 2010;81(10):1400-1433. doi:10.1016/j.resuscitation.2010.08.015
354. Goyal A, Spertus JA, Gosch K, et al. Serum potassium levels and mortality in acute myocardial infarction. JAMA. 2012;307(2):157-164. doi:10.1001/jama.2011.1967
355. Dépret F, Peacock WF, Liu KD, Rafique Z, Rossignol P, Legrand M. Management of hyperkalemia in the acutely ill patient. Ann Intensive Care. 2019;9(1):32. Published 2019 Feb 28. doi:10.1186/s13613-019-0509-8
356. Palmer BF, Clegg DJ. Diagnosis and treatment of hyperkalemia. Cleve Clin J Med. 2017;84(12):934-942. doi:10.3949/ccjm.84a.17056
357. Vital FM, Ladeira MT, Atallah AN. Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema. Cochrane Database Syst Rev. 2013;(5):CD005351. Published 2013 May 31. doi:10.1002/14651858.CD005351.pub3 (54)
358. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure [published correction appears in Eur Heart J. 2021 Dec 21;42(48):4901. doi: 10.1093/eurheartj/ehab670.]. Eur Heart J. 2021;42(36):3599-3726. doi:10.1093/eurheartj/ehab368
359. Muaddi L, Ledgerwood C, Sheridan R, Dumont T, Nashar K. Acute Renal Failure and Its Complications, Indications for Emergent Dialysis, and Dialysis Modalities. Crit Care Nurs Q. 2022;45(3):258-265. doi:10.1097/CNQ.0000000000000410
360. Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36(42):2921-2964. doi:10.1093/eurheartj/ehv318
361. Rehman KA, Betancor J, Xu B, et al. Uremic pericarditis, pericardial effusion, and constrictive pericarditis in end-stage renal disease: Insights and pathophysiology. Clin Cardiol. 2017;40(10):839-846. doi:10.1002/clc.22770
362. Baldwin JJ, Edwards JE. Uremic pericarditis as a cause of cardiac tamponade. Circulation. 1976;53(5):896-901. doi:10.1161/01.cir.53.5.896
363. European Association for the Study of the Liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J Hepatol. 2010;53(3):397-417. doi:10.1016/j.jhep.2010.05.004
364. Angeli P, Gines P, Wong F, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. Gut. 2015;64(4):531-537. doi:10.1136/gutjnl-2014-308874
365. Facciorusso A. Hepatorenal Syndrome Type 1: Current Challenges And Future Prospects. Ther Clin Risk Manag. 2019;15:1383-1391. Published 2019 Nov 27. doi:10.2147/TCRM.S205328
366. Mindikoglu AL, Pappas SC. New Developments in Hepatorenal Syndrome [published correction appears in Clin Gastroenterol Hepatol. 2018 Jun;16(6):988. doi: 10.1016/j.cgh.2018.03.038.]. Clin Gastroenterol Hepatol. 2018;16(2):162-177.e1. doi:10.1016/j.cgh.2017.05.041
367. Runyon BA. Management of adult patients with ascites caused by cirrhosis. Hepatology. 1998;27(1):264-272. doi:10.1002/hep.510270139
368. O'Leary JG, Levitsky J, Wong F, Nadim MK, Charlton M, Kim WR. Protecting the Kidney in Liver Transplant Candidates: Practice-Based Recommendations From the American Society of Transplantation Liver and Intestine Community of Practice. Am J Transplant. 2016;16(9):2516-2531. doi:10.1111/ajt.13790
369. Wong F, Pappas SC, Curry MP, et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome. N Engl J Med. 2021;384(9):818-828. doi:10.1056/NEJMoa2008290
370. Ghannoum M, Gosselin S, Hoffman RS, et al. Extracorporeal treatment for ethylene glycol poisoning: systematic review and recommendations from the EXTRIP workgroup. Crit Care. 2023;27(1):56. Published 2023 Feb 10. doi:10.1186/s13054-022-04227-2
371. Woolf AD, Erdman AR, Nelson LS, et al. Tricyclic antidepressant poisoning: an evidence-based consensus guideline for out-of-hospital management. Clin Toxicol (Phila). 2007;45(3):203-233. doi:10.1080/15563650701226192
372. Heard K, Zuckerman M. Approach to the Poisoned Patient. J Educ Teach Emerg Med. 2021;6(1):L1-L4. Published 2021 Jan 15. doi:10.21980/J8264S
373. Boyle JS, Bechtel LK, Holstege CP. Management of the critically poisoned patient. Scand J Trauma Resusc Emerg Med. 2009;17:29. Published 2009 Jun 29. doi:10.1186/1757-7241-17-29
374. Madden MA. Pediatric Toxicology: Emerging Trends. J Pediatr Intensive Care. 2015;4(2):103-110. doi:10.1055/s-0035-1556753
375. St-Onge M, Anseeuw K, Cantrell FL, et al. Experts Consensus Recommendations for the Management of Calcium Channel Blocker Poisoning in Adults. Crit Care Med. 2017;45(3):e306-e315. doi:10.1097/CCM.0000000000002087
376. Chiew AL, Reith D, Pomerleau A, et al. Updated guidelines for the management of paracetamol poisoning in Australia and New Zealand. Med J Aust. 2020;212(4):175-183. doi:10.5694/mja2.50428
377. Kushimoto S, Gando S, Saitoh D, et al. The impact of body temperature abnormalities on the disease severity and outcome in patients with severe sepsis: an analysis from a multicenter, prospective survey of severe sepsis. Crit Care. 2013;17(6):R271. Published 2013 Nov 13. doi:10.1186/cc13106 (60)
378. Laupland KB, Zahar JR, Adrie C, et al. Severe hypothermia increases the risk for intensive care unit-acquired infection. Clin Infect Dis. 2012;54(8):1064-1070. doi:10.1093/cid/cir1033
379. Kushimoto S, Gando S, Saitoh D, et al. The impact of body temperature abnormalities on the disease severity and outcome in patients with severe sepsis: an analysis from a multicenter, prospective survey of severe sepsis. Crit Care. 2013;17(6):R271. Published 2013 Nov 13. doi:10.1186/cc13106
380. Driver J, Fielding A, Mullhi R, Chipp E, Torlinski T. Temperature management of adult burn patients in intensive care: findings from a retrospective cohort study in a tertiary centre in the United Kingdom. Anaesthesiol Intensive Ther. 2022;54(3):226-233. doi:10.5114/ait.2022.119131
381. Launey Y, Nesseler N, Mallédant Y, Seguin P. Clinical review: fever in septic ICU patients--friend or foe?. Crit Care. 2011;15(3):222. doi:10.1186/cc10097
382. Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg Med Clin North Am. 2010;28(1):29-vii. doi:10.1016/j.emc.2009.09.010 (62)
383. Yang J, Liu F, Liang Y, Guo C, Wang J, Chen X. Massive Hemoptysis in Children. Can Respir J. 2020;2020:6414719. Published 2020 Jun 6. doi:10.1155/2020/6414719 (62)
384. Moughal S, Trippier S, Al-Mousa A, et al. Strokectomy for malignant middle cerebral artery infarction: experience and meta-analysis of current evidence. J Neurol. 2022;269(1):149-158. doi:10.1007/s00415-020-10358-9 (62)
385. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clin Infect Dis. 2011;52(4):e56-e93. doi:10.1093/cid/cir073 (63)
386. Omidkhoda N, Abedi F, Ghavami V, et al. The Effect of Heparin and Its Preparations on Disseminated Intravascular Coagulation Mortality and Hospitalization: A Systematic Review. Int J Clin Pract. 2022;2022:2226761. Published 2022 Jul 9. doi:10.1155/2022/2226761 (63)
387. Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review [published correction appears in J Clin Oncol. 2010 Feb 1;28(4):708]. J Clin Oncol. 2008;26(16):2767-2778. doi:10.1200/JCO.2007.15.0177 (51,53, 63)
388. Rosales M, Roncon S, Mariz M, Ferreira AM, Faria F, Santos L. Therapeutic Leukapheresis: Experience of a Single Oncologic Centre. Transfus Med Hemother. 2022;49(4):250-257. Published 2022 Feb 1. doi:10.1159/000520933 (63)
389. Rafat C, Schortgen F, Gaudry S, et al. Use of desmopressin acetate in severe hyponatremia in the intensive care unit. Clin J Am Soc Nephrol. 2014;9(2):229-237. doi:10.2215/CJN.00950113 (63)
390. Lekwijit S, Chan CW, Green LV, Liu VX, Escobar GJ. The Impact of Step-Down Unit Care on Patient Outcomes After ICU Discharge. Crit Care Explor. 2020;2(5):e0114. Published 2020 May 6. doi:10.1097/CCE.0000000000000114
391. Song MJ, Lee YJ. Strategies for successful implementation and permanent maintenance of a rapid response system. Korean J Intern Med. 2021;36(5):1031-1039. doi:10.3904/kjim.2020.693
392. Kansagara D, Fu R, Freeman M, Wolf F, Helfand M. Intensive insulin therapy in hospitalized patients: a systematic review. Ann Intern Med. 2011;154(4):268-282. doi:10.7326/0003-4819-154-4-201102150-00008
393. Cryer PE, Axelrod L, Grossman AB, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009;94(3):709-728. doi:10.1210/jc.2008-1410 (64)
394. Umpierrez G, Korytkowski M. Diabetic emergencies - ketoacidosis, hyperglycaemic hyperosmolar state and hypoglycaemia. Nat Rev Endocrinol. 2016;12(4):222-232. doi:10.1038/nrendo.2016.15 (64)
395. Yao RQ, Ren C, Wu GS, Zhu YB, Xia ZF, Yao YM. Is intensive glucose control bad for critically ill patients? A systematic review and meta-analysis. Int J Biol Sci. 2020;16(9):1658-1675. Published 2020 Mar 12. doi:10.7150/ijbs.43447 (64)
396. Abir M, Choi H, Cooke CR, Wang SC, Davis MM. Effect of a mass casualty incident: clinical outcomes and hospital charges for casualty patients versus concurrent inpatients. Acad Emerg Med. 2012;19(3):280-286. doi:10.1111/j.1553-2712.2011.01278.x
397. Marcozzi DE, Pietrobon R, Lawler JV, et al. Development of a Hospital Medical Surge Preparedness Index using a national hospital survey. Health Serv Outcomes Res Methodol. 2020;20(1):60-83. doi:10.1007/s10742-020-00208-6
398. Ball CG, Kirkpatrick AW, Mulloy RH, Gmora S, Findlay C, Hameed SM. The impact of multiple casualty incidents on clinical outcomes. J Trauma. 2006;61(5):1036-1039. doi:10.1097/01.ta.0000231764.00067.5
399. Abir M, Davis MM, Sankar P, Wong AC, Wang SC. Design of a model to predict surge capacity bottlenecks for burn mass casualties at a large academic medical center. Prehosp Disaster Med. 2013;28(1):23-32. doi:10.1017/S1049023X12001513
400. Lavery GG, Horan E. Clinical review: communication and logistics in the response to the 1998 terrorist bombing in Omagh, Northern Ireland. Crit Care. 2005;9(4):401-408. doi:10.1186/cc350
401. Culley JM, Effken JA. Development and validation of a mass casualty conceptual model. J Nurs Scholarsh. 2010;42(1):66-75. doi:10.1111/j.1547-5069.2009.01320.x
402. Agnoletti V, Russo E, Circelli A, et al. From intensive care to step-down units: Managing patients throughput in response to COVID-19. Int J Qual Health Care. 2021;33(1):mzaa091. doi:10.1093/intqhc/mzaa091
403. Joynt GM, Loo S, Taylor BL, et al. Chapter 3. Coordination and collaboration with interface units. Recommendations and standard operating procedures for intensive care unit and hospital preparations for an influenza epidemic or mass disaster. Intensive Care Med. 2010;36 Suppl 1(Suppl 1):S21-S31. doi:10.1007/s00134-010-1762-3
404. Afriyie-Mensah J, Aboagye ET, Ganu VJ, et al. Clinical and therapeutic outcomes of COVID-19 intensive care units (ICU) patients: a retrospective study in Ghana. Pan Afr Med J. 2021;38:107. Published 2021 Feb 2. doi:10.11604/pamj.2021.38.107.27131
405. Tong A, Baumgart A, Evangelidis N, et al. Core Outcome Measures for Trials in People With Coronavirus Disease 2019: Respiratory Failure, Multiorgan Failure, Shortness of Breath, and Recovery. Crit Care Med. 2021;49(3):503-516. doi:10.1097/CCM.0000000000004817
406. Jöbges S, Vinay R, Luyckx VA, Biller-Andorno N. Recommendations on COVID-19 triage: international comparison and ethical analysis. Bioethics. 2020;34(9):948-959. doi:10.1111/bioe.12805
407. Kucewicz-Czech E, Damps M. Triage during the COVID-19 pandemic. Anaesthesiol Intensive Ther. 2020;52(4):312-315. doi:10.5114/ait.2020.100564
408. Aggour M, Tran Chi C, Fiehler J. Patient prioritization and management during the COVID-19 pandemic. Interv Neuroradiol. 2021;27(1_suppl):19-23. doi:10.1177/15910199211035302
409. Tyrrell CSB, Mytton OT, Gentry SV, et al. Managing intensive care admissions when there are not enough beds during the COVID-19 pandemic: a systematic review. Thorax. 2021;76(3):302-312. doi:10.1136/thoraxjnl-2020-21
410. Brown MJ, Goodwin J. Allocating Medical Resources in the Time of Covid-19. N Engl J Med. 2020;382(22):e79. doi:10.1056/NEJMc2009666
411. Hick JL, Christian MD, Sprung CL; European Society of Intensive Care Medicine's Task Force for intensive care unit triage during an influenza epidemic or mass disaster. Chapter 2. Surge capacity and infrastructure considerations for mass critical care. Recommendations and standard operating procedures for intensive care unit and hospital preparations for an influenza epidemic or mass disaster. Intensive Care Med. 2010;36 Suppl 1:S11-S20. doi:10.1007/s00134-010-1761-4 (99)
412. Rubinson L, Hick JL, Curtis JR, et al. Definitive care for the critically ill during a disaster: medical resources for surge capacity: from a Task Force for Mass Critical Care summit meeting, January 26-27, 2007, Chicago, IL. Chest. 2008;133(5 Suppl):32S-50S. doi:10.1378/chest.07-2691 (99)
413. Khan Z, Hulme J, Sherwood N. An assessment of the validity of SOFA score based triage in H1N1 critically ill patients during an influenza pandemic. Anaesthesia. 2009;64(12):1283-1288. doi:10.1111/j.1365-2044.2009.06135.x
414. AP-HP/Universities/Inserm COVID-19 Research Collaboration. Predictive usefulness of RT-PCR testing in different patterns of Covid-19 symptomatology: analysis of a French cohort of 12,810 outpatients. Sci Rep. 2021;11(1):21233. Published 2021 Oct 27. doi:10.1038/s41598-021-99991-6
415. Oliveira MC, Scharan KO, Thomés BI, et al. Diagnostic accuracy of a set of clinical and radiological criteria for screening of COVID-19 using RT-PCR as the reference standard. BMC Pulm Med. 2023;23(1):81. Published 2023 Mar 9. doi:10.1186/s12890-023-02369-9
416. Hammond NE, Corley A, Fraser JF. The utility of procalcitonin in diagnosis of H1N1 influenza in intensive care patients. Anaesth Intensive Care. 2011;39(2):238-241. doi:10.1177/0310057X1103900213
417. Barfod C, Lauritzen MM, Danker JK, et al. Abnormal vital signs are strong predictors for intensive care unit admission and in-hospital mortality in adults triaged in the emergency department - a prospective cohort study. Scand J Trauma Resusc Emerg Med. 2012;20:28. Published 2012 Apr 10. doi:10.1186/1757-7241-20-28
418. Stelfox HT, Lane D, Boyd JM, et al. A scoping review of patient discharge from intensive care: opportunities and tools to improve care. Chest. 2015;147(2):317-327. doi:10.1378/chest.13-2965
419. Plotnikoff KM, Krewulak KD, Hernández L, et al. Patient discharge from intensive care: an updated scoping review to identify tools and practices to inform high-quality care. Crit Care. 2021;25(1):438. Published 2021 Dec 17. doi:10.1186/s13054-021-03857-2
420. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease [published correction appears in Eur Heart J. 2022 Jun 1;43(21):2022. doi: 10.1093/eurheartj/ehac051.]. Eur Heart J. 2022;43(7):561-632. doi:10.1093/eurheartj/ehab395
421. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in Circulation. 2021 Feb 2;143(5):e228. doi: 10.1161/CIR.0000000000000960.] [published correction appears in Circulation. 2021 Mar 9;143(10):e784. doi: 10.1161/CIR.0000000000000966.]. Circulation. 2021;143(5):e35-e71. doi:10.1161/CIR.0000000000000932
422. Bohula EA, Katz JN, van Diepen S, et al. Demographics, Care Patterns, and Outcomes of Patients Admitted to Cardiac Intensive Care Units: The Critical Care Cardiology Trials Network Prospective North American Multicenter Registry of Cardiac Critical Illness. JAMA Cardiol. 2019;4(9):928-935. doi:10.1001/jamacardio.2019.2467
423. Miller PE, Senman BC, Gage A, et al. Acute Decompensated Valvular Disease in the Intensive Care Unit. JACC Adv. 2024;3(12):101402. Published 2024 Dec 26. doi:10.1016/j.jacadv.2024.101402
424. Akodad M, Schurtz G, Adda J, Leclercq F, Roubille F. Management of valvulopathies with acute severe heart failure and cardiogenic shock. Arch Cardiovasc Dis. 2019;112(12):773-780. doi:10.1016/j.acvd.2019.06.009
425. Duncan CF, Bowcock E, Pathan F, Orde SR. Mitral regurgitation in the critically ill: the devil is in the detail. Ann Intensive Care. 2023;13(1):67. Published 2023 Aug 2. doi:10.1186/s13613-023-01163-4
- Annexes
Modified Early Warning Score Fig.1
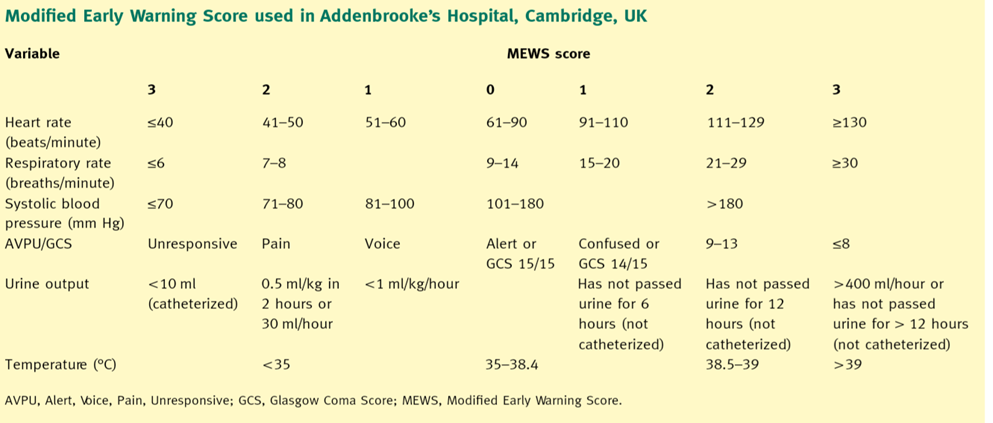
Guide to resource allocation of intensive monitoring and care including levels of monitoring, care, and nursing ratios (table 2):
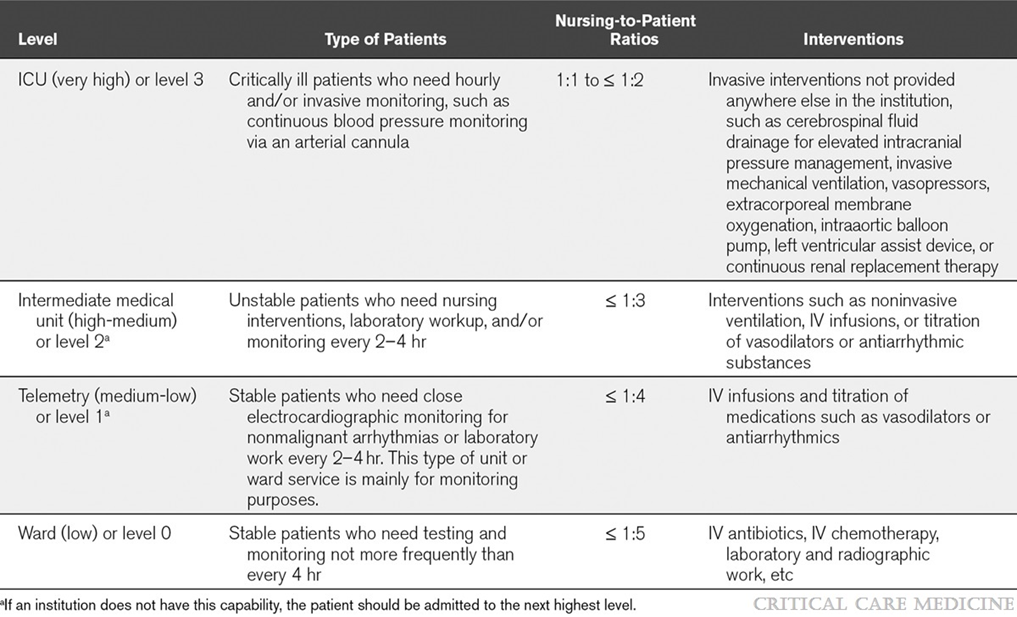
ICU Admission Prioritization framework(table 3)
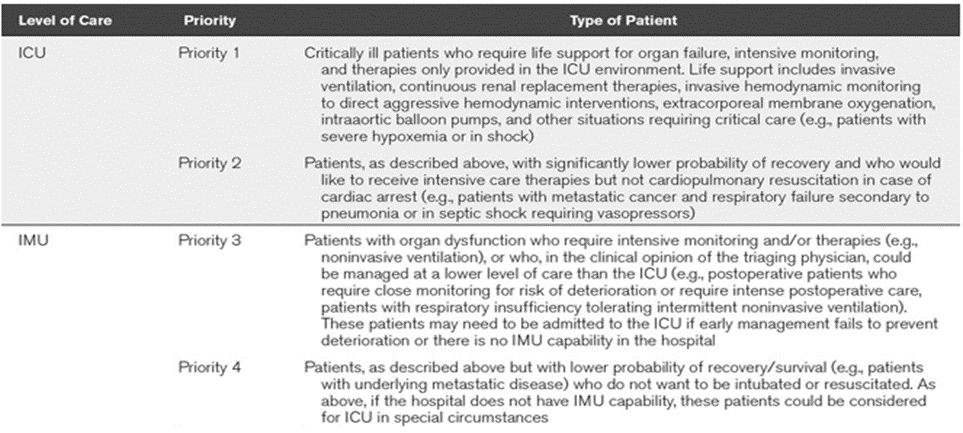
addmsion checklist (table 4, 5)