Prevention and Management of Overweight and Obesity in Children and Adolescents
| Site: | EHC | Egyptian Health Council |
| Course: | Pediatrics Guidelines |
| Book: | Prevention and Management of Overweight and Obesity in Children and Adolescents |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:02 AM |
Description
"last update: 26 August 2025" Download Guideline
- Executive Summary
Childhood obesity is one of the most serious public health challenges of the 21st century. The prevalence has increased at an alarming rate, affecting many low- and middle-income countries particularly in urban settings.
The increasing prevalence of childhood obesity has led to the emergence of multiple serious obesity-related comorbidities that not only threaten the health of those affected but also promise to place a large strain on the health care system.
For children less than 5 years of age, overweight is weight-for-height greater than 2 standard deviations above WHO Child Growth Standards median; and obesity is weight-for-height greater than 3 standard deviations above the WHO Child Growth Standards median. Children and adolescents aged between 5–19 years, overweight is BMI-for-age greater than 1 standard deviation above the WHO Growth Reference median; and obesity is greater than 2 standard deviations above the WHO Growth Reference median is widely accepted that increase in obesity results from an imbalance between energy intake and expenditure, with an increase in positive energy balance being closely associated with the lifestyle adopted and the dietary intake preferences
Childhood obesity is associated with a higher chance of obesity, premature death and disability in adulthood. But in addition to increased future risks, obese children experience breathing difficulties, increased risk of fractures, hypertension, early markers of cardiovascular disease, insulin resistance and psychological effects.
This guideline focuses on prevention and management of pediatric obesity and complications.
Guideline development process and methods
After reviewing all the inclusion and exclusion criteria and quality appraisal results, the GDG/ GAG recommended using the following source original clinical practice guidelines (CPGs):
1. WHO: Assessing and managing children at primary health care facilities to prevent overweight and obesity in the context of the double burden of malnutrition, 2017,
2. The Clinical Practice Guidelines For The Management Of Overweight And Obesity In Adults, Adolescents And Children In Australia, 2013.
3. Clinical practice guideline for the diagnosis and treatment of pediatric obesity: recommendations from the Committee on Pediatric Obesity of the Korean Society of Pediatric Gastroenterology Hepatology and Nutrition. Korean J Pediatr. 2019 Jan;62(1):3-21.
We conducted Adolopment for these guidelines: (Adoption, Adaptation, and Development)
- Adoption for most of the guideline recommendations.
- Development of Good Practice Statements
Recommendations and Good Practice Statements (GPS)
This version of the CPG includes recommendations and good practice statements on the following four sub-sections:
A. Diagnosis of pediatric obesity and complications
The guideline covers infants, children and adolescents less than 17 years.
This guideline emphasis on early detection of overweight and obesity & identification of infants, children and adolescents at high risk of developing overweight and obesity.
B. Management of overweight and obesity.
This section includes recommendations and good practice statements on proper management of overweight and obesity in the targeted population.
C. Prevention of overweight, obesity and future complications.
We can summarize the guidelines’ recommendations for Prevention and Management of Overweight and Obesity in Children and Adolescents in the following:
· We recommend the following methods for early prevention of overweight and obesity in children and adolescent:
Exclusive breastfeeding is recommended up to 6 months.
Avoid excessive weight gain and/or increased weight-to- length ratio from the very first months of life.
Solid foods and beverages other than breast milk or infant formulas should be introduced no earlier than 4 months and no later than 6 months.
Protein intake should be limited to less than 15% of the daily energy intake.
Reduction of lipid intake to percentages indicated for adults is not recommended
Sweetened drinks should be avoided.
(Strong recommendation).
· In overweight and obese infants, children and adolescents without co-morbidities, we recommend that the healthcare provider diagnose the cause using history taking through asking about:
1-Developmental history including
➡️ Age.
➡️ Type of delivery, birth weight and length, gestational age at birth, maternal gestational diabetes.
➡️ Infant feeding, including duration of breastfeeding and /or formula.
➡️ Growth and development (e.g. age at which the child walked, talked).
2- Physical and mental health including
➡️ Weight history including previous weight management interventions, previous and current eating behaviours, recent weight gain.
➡️ Physical conditions associated with overweight (e.g. joint problems).
➡️ Physical disability affecting mobility.
➡️ Mental health (e.g. depression, anxiety, low self-esteem, eating disorder) and social experience (e.g. isolation, bullying).
➡️ Family history of obesity, type 2 diabetes, gestational diabetes, hypertension, dyslipidaemia, cardiovascular disease, sleep apnoea, polycystic ovary syndrome, bariatric surgery, eating disorders.
➡️ Medications that may contribute to weight gain (e.g. glucocorticoids, psychoactive agents).
➡️ Sleeping routine and presence of snoring.
➡️ Menstrual history for girls.
3- Health behaviours including
➡️ Dietary intake (especially high intake of sugar-containing drinks and high-energy foods, and low intake of fruit and vegetables).
➡️ Previous and current dietary behaviours—for example, recurrent episodes of dieting, signs of pathological hyperphagia (such as eating large portions very quickly, being difficult to distract from food) and signs of disordered eating (such as binge eating).
➡️ Dietary patterns—for example, eating breakfast and regular meals, snacking, eating prepared foods outside the home (eating out, take-away).
➡️ Levels of physical activity and sedentary activity (e.g. hours spent in screen-based activities per day) (e.g. time spent being active, active transport, time spent outside, participation in structured exercise).
➡️ Family body-image behaviours (e.g. body perceptions, body checking and avoidant behaviours, body-related thoughts and beliefs, distress associated with body weight or shape, family talk and modelling related to body weight and shape)
4- Comorbidities including
➡️ Is the person on medications associated with weight gain?
➡️ Is fitness level sufficient for moderate-intensity activity?
➡️ Is mobility impaired (e.g. due to obesity or comorbidities)?
➡️ Is activity impeded by disability?
➡️ Is lifestyle change impeded by disability?
➡️ Has the person experienced life stressors (e.g. abuse, trauma, grief)?
➡️ Is the person experiencing symptoms of depression?
➡️ Is the person experiencing or at risk of an eating disorder?
(Strong recommendation).
· In overweight and obese infants, children and adolescent's without co-morbidities, wwe suggest that the healthcare provider diagnose the cause, using general and focused examination for appropriate determination of etiology through :
I- Anthropometric parameters: Weight, length/height, Waist and hip circumference are useful surrogates in estimating visceral fat.
➡️ Children <24 months of age diagnosed as overweight if their weight for length is above the 95th percentile on the WHO Growth Charts.
➡️ Children and adolescents >2 years of age diagnosed with overweight when the BMI is above the 85th but less than the 95th percentile for age and sex, and obesity when the BMI is above the 95th percentile.
➡️ A waist- to-height ratio of ≥ 0.5 may be useful in predicting cardiovascular risk and is easy to calculate.
II- Obesity focused clinical signs: Clinical assessment aims to identify possible causes for overweight or obesity, and indicators of comorbidities
1- Cutaneous examination:
➡️ Acanthosis nigricans (velvety, light brown-to-black markings usually on the neck, under the arms or in the groin.
➡️ Intertrigo.
➡️ Hirsutism/acne from androgen excess: A sensitive examination of the status of excess hair in females.
➡️ Striae when associated with obesity are lighter and narrower. But if darker and wider in child with short stature with hypertension, screen for Cushing’s.
2- Pubertal or tanner staging
3- Skeletal problems :
➡️ If knee or hip pain exclude slipped capital femoral epiphysis.
➡️ Pes planus (flat feet),
➡️ Genu valgum (knock knee).
➡️ Bowed tibias.
4- Cardiac: measure blood pressure (with appropriate cuff size)
5- Respiratory examination: if in doubt refer
6- Abdominal examination- exclude hepatomegaly.
(Weak (conditional) recommendation).
· In overweight and obese infants, children and adolescents without co-morbidities, we suggest the following laboratory tests to assess the case:
➡️ Complete blood count.
➡️ Lipid profile.
➡️ 25 hydroxy vitamin D level.
➡️ Iron profile
(Good practice statement).
· We recommend that the healthcare provider should refer overweight and obese infants, children and adolescents if upon examination there are red flags suggestive of endocrine, genetic, neurologic manifestations or evidence of co-morbidities.
(Strong recommendation).
· In children and adolescent obesity without comorbidities we recommend diet intervention for management as follow :
➡️ Regular meals including breakfast and snacks.
➡️ Healthy high nutritive value food.
➡️ Eat meals as family.
➡️ Provide a calculator for daily caloric, macro and micronutrients needs depending on weight and age (difficult to interpret).
➡️ We can use my plate as alternative easier method. (5 meals per day, 3 hours apart, each meal is balanced containing one portion protein, carbohydrate, vegetables and fruits each).
(Strong recommendation).
· For children and adolescents who are overweight or obese, we recommend lifestyle change including reduced energy intake and sedentary behavior, increased physical activity and measures to support behavioral change.
(Strong recommendation).
➡️ Focus lifestyle programs on parents, carers and families.
➡️ Encourage moderate and physical activities.
➡️ Increase daily activities (walking to school).
➡️ Be involved in sport team.
➡️ Parents should be active with the child (playing, walking).
➡️ Be role model by being active themselves.
➡️ Avoid being controlling or restricting to the child’s food intake.
➡️ Avoid using food as rewards.
➡️ Comfort the child with attention instead of food.
➡️ Decrease time –screen based activities.
➡️ Separate eating from watching tv or computer.
(Weak (conditional) recommendation).
Physical activity :
➡️ Active moderate to vigorous activity for at least 20 min/day to 60 min/day, 5 days/week.
➡️ Programmed exercise targeting decreasing body fat.
➡️ Increasing daily physical activities.
(Strong recommendation).
Behavioral changes :
➡️ Recommend family based approach to adapt healthier habits and decrease parental obesogenic lifestyle pattern.
➡️ Decrease sedentary time : nonacademic screen time, digital activities 1-2 hr/d.
➡️ Adequate sleep pattern.
➡️ Setting realistic goals for change.
➡️ Development of public health interventions to control overweight and obesity in children with lower socioeconomic status.
(Strong recommendation).
· We suggest against drug treatment as it is not generally recommended for children younger than 12 years.
In children aged ≥ 12 years, treatment with orlistat is recommended only if physical comorbidities (such as orthopedic problems or sleep apnea) or severe psychological comorbidities are present.
Treatment should be started in a specialist pediatric setting, by multidisciplinary teams with experience of prescribing in this age group
Orlistat acts by inhibiting pancreatic lipase and increasing fecal losses of triglyceride
(Weak (conditional) recommendation).
· For post-pubertal adolescents with a BMI > 40 kg/m2 (or > 35 kg/m2 with obesity-related complications), we suggest laparoscopic adjustable gastric banding via specialist bariatric/pediatric teams may be considered if other interventions have been unsuccessful in producing weight loss.
Bariatric surgery should only be undertaken by a highly specialized surgical team within the framework of a multidisciplinary approach.
(Weak (conditional) recommendation).
To detect TTT success, we recommend :
1- BMI 85-94 (overweight):
Weight maintenance until BMI < 85 (for all age group 2-18 years).
2- BMI 95-98 (obesity):
2-5 -years: maintain weight until BMI <85 or weight loss not more than 0.5 kg/month(assess that adequate energy diet is obtained)
6-18 years: weight loss not more than 0.9 kg/month
3- BMI >/ 99(severe obesity):
2-5 years: gradual weight loss not more than 0.5 kg/month.
6-18 years: gradual loss of weight not more than 0.9 kg/month
(Strong recommendation).
Guideline Registration
PREPARE (Practice guideline REgistration for transPAREncy), WHO Collaborating Center for Guideline Implementation and Knowledge Translation, EBM Center, University of Lanzhou, Lanzhou, China. Registration Number: ((submitted and in process)). Link: http://www.guidelines-registry.org/- Recommendations
|
Table 3. Recommendations |
|
|
|||
|
A. prevention of overweight and obesity in children and adolescent |
|||||
|
N |
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
A1 |
What are preventative methods for early prevention of overweight and obesity in children and adolescent by pediatricians, primary health care professionals, in outpatient clinics and primary health care facilities |
WHO 2017 |
A1 • Exclusive breastfeeding is recommended for up to 6 months. • Avoid excessive weight gain and/or increased weight-to- length ratio from the very first months of life. • Solid foods and beverages other than breast milk or infant formulas should be introduced no earlier than 4 months and no later than 6 months • Protein intake should be limited to less than 15% of the daily energy intake. • Reduction of lipid intake to percentages indicated for adults is not recommended. • Sweetened drinks should be avoided. |
Moderate |
Strong
|
|
Table 4. Recommendations |
|
|
|||
|
B. Diagnosis of overweight and obesity in children and adolescent. |
|||||
|
N |
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
B1 |
In overweight and obese infants, children and adolescents without co-morbidities, how can the healthcare provider diagnose the cause using history taking appropriate determination of the etiology? |
Australian 2013 |
B1. 1-Developmental history: ➡️ Age. ➡️ Type of delivery, birth weight and length, gestational age at birth, maternal gestational diabetes. ➡️ Infant feeding, including duration of breastfeeding and /or formula. ➡️ Growth and development (e.g. age at which the child walked, talked). 2-Physical and mental health. ➡️ Weight history including previous weight management interventions, previous and current eating behaviours, recent weight gain. ➡️ Physical conditions associated with overweight (e.g. joint problems). ➡️ Physical disability affecting mobility. ➡️ Mental health (e.g. depression, anxiety, low self-esteem, eating disorder) and social experience (e.g. isolation, bullying). ➡️ Family history of obesity, type 2 diabetes, gestational diabetes, hypertension, dyslipidaemia, cardiovascular disease, sleep apnoea, polycystic ovary syndrome, bariatric surgery, eating disorders. ➡️ Medications that may contribute to weight gain (e.g. glucocorticoid, psychoactive agents). ➡️ Sleeping routine and presence of snoring. ➡️ Menstrual history for girls. 3- Health behaviours ➡️ Dietary intake (especially high intake of sugar-containing drinks and high-energy foods, and low intake of fruit and vegetables). ➡️ Previous and current dietary behaviours—for example, recurrent episodes of dieting, signs of pathological hyperphagia (such as eating large portions very quickly, being difficult to distract from food) and signs of disordered eating (such as binge eating). ➡️ Dietary patterns, for example, eating breakfast and regular meals, snacking, eating prepared foods outside the home (eating out, take-away). ➡️ Levels of physical activity and sedentary activity (e.g. hours spent in screen-based activities per day) (e.g. time spent being active, active transport, time spent outside, participation in structured exercise). ➡️ Family body-image behaviours (e.g. body perceptions, body checking and avoidant behaviours, body-related thoughts and beliefs, distress associated with body weight or shape, family talk and modelling related to body weight and shape). 4- Comorbidities ➡️ Is the person on medications associated with weight gain?. ➡️ Is fitness level sufficient for moderate-intensity activity?. ➡️ Is mobility impaired (e.g. due to obesity or comorbidities)?. ➡️ Is activity impeded by disability?. ➡️ Is lifestyle change impeded by disability?. ➡️ Has the person experienced life stressors (e.g. abuse, trauma, grief)?. ➡️ Is the person experiencing symptoms of depression?. ➡️ Is the person experiencing or at risk of an eating disorder? |
Moderate |
Strong |
|
B2 |
In overweight and obese infants, children and adolescent's without co-morbidities, how the healthcare provider diagnose the cause, using general and focused examination for appropriate determination of etiology
|
Korean 2019
Australian 2013 |
B2 I- Anthropometric parameters: Weight, length/height, Waist and hip circumference are useful surrogates in estimating visceral fat. • Children <24 months of age diagnosed as overweight if their weight for length is above the 95th percentile on the WHO Growth Charts • Children and adolescents >2 years of age diagnosed with overweight when the BMI is above the 85th but less than the 95th percentile for age and sex, and obesity when the BMI is above the 95th percentile. • A waist- to-height ratio of ≥ 0.5 may be useful in predicting cardiovascular risk and is easy to calculate.
II- Obesity focused clinical signs: Clinical assessment aims to identify possible causes for overweight or obesity, and indicators of comorbidities 1- Cutaneous examination: ➡️ Acanthosis nigricans (velvety, light brown-to-black markings usually on the neck, under the arms or in the groin. ➡️ Intertrigo. ➡️ Hirsutism/acne from androgen excess: a sensitive examination of the status of excess hair in females. ➡️ Striae when associated with obesity are lighter and narrower. But if darker and wider in child with short stature with hypertension, screen for Cushing’s. 2- Pubertal or tanner staging. 3- Skeletal problems: ➡️ If knee or hip pain, exclude slipped capital femoral epiphysis, ➡️ Pes planus (flat feet). ➡️ Genu valgum (knock knee). ➡️ Bowed tibias 4- Cardiac: measure blood pressure (with appropriate cuff size) 5- Respiratory examination: if in doubt refer 6- Abdominal examination- exclude hepatomegaly.
|
Low
Low |
Weak (conditional)
Weak (conditional) |
|
B3 |
In overweight and obese infants, children and adolescents without co-morbidities, what are the basic laboratory tests requested by the health care provider to assess the case. |
|
B3 · Complete blood count
|
|
Good Practice Statement |
|
B4 |
When and to whom should the healthcare provider refer to overweight and obese infants, children and adolescents without co-morbidities?
|
Australian 2013 |
B4 The healthcare provider should refer overweight and obese infants, children and adolescents if upon examination there are red flags suggestive of endocrine, genetic, neurologic manifestations or evidence of co-morbidities |
Moderate |
Strong |
|
Table 5. Recommendations |
|
|
|||
|
C. Management of overweight and obesity in children and adolescent |
|||||
|
N |
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
C1 |
Role of diet intervention for management of children and adolescent obesity without comorbidities by pediatricians, primary health care professionals, in outpatient clinics and primary health care facilities |
Australian guidelines (2013) |
C1. • Regular meals including breakfast and snacks • Healthy high nutritive value food • Eat meals as family • Provide a calculator for daily caloric, macro and micronutrients need depending on weight and age (difficult to interpret). • We can use my plate as an easier alternative method. (5 meals per day, 3 hours apart, each meal is balanced containing one portion of protein, carbohydrate, vegetables and fruits each). |
Moderate |
Strong |
|
C2 |
Role of lifestyle modification for management of children and adolescent obesity without comorbidities by pediatricians, primary health care professionals, in outpatient clinics and primary health care facilities
|
Australian (2013)
Korean 2019
Korean 2019 |
For children and adolescents who are overweight or obese, recommend lifestyle change including reduced energy intake and sedentary behavior, increased physical activity and measures to support behavioral change. Focus lifestyle programs on parents, carers and families.
• Encourage moderate and physical activities • Increase daily activities (walking to school) • Be involved in sport team • Parents should be active with the child (playing, walking) • Be role model by being active themselves • Avoid controlling or restricting to the child’s food intake • Avoid using food as rewards • Comfort the child with attention instead of food • Decrease time –screen-based activities • Separate eating from watching tv or computer
Physical activity 1. Active moderate to vigorous activity for at least 20 min/day to 60 min/day, 5 days/week 2. Programmed exercise targeting decreasing body fat 3. Increasing daily physical activities
Behavioral changes 1. Recommend family-based approach to adapt healthier habits and decrease parental obesogenic lifestyle pattern 2. Decrease sedentary time, nonacademic screen time, digital activities 1-2 hr/d 3. Adequate sleep pattern 4. Setting realistic goals for change 5. Development of public health interventions to control overweight and obesity in children with lower socioeconomic status |
Moderate
Low
High
High
|
Strong
Weak (conditional)
Strong
Strong |
|
C3 |
What is the pharmacological role in management of children and adolescent obesity
|
Australian (2013) |
C3
|
Low |
Weak (conditional) |
|
C4 |
What is the role of bariatric Surgical procedure referral in adolescent obesity ?
|
Australian (2013)
Korean 2019 |
C4 • For post-pubertal adolescents with a BMI > 40 kg/m2(or > 35 kg/m2 with obesity-related complications), laparoscopic adjustable gastric banding via specialist bariatric/pediatric teams may be considered if other interventions have been unsuccessful in producing weight loss. • Bariatric surgery should only be undertaken by a highly specialized surgical team within the framework of a multidisciplinary approach.
Aim (how to detect TTT success) 1.BMI 85-94 (overweight): Weight maintenance until BMI < 85 (for all age group 2-18 years). 2.BMI 95-98 (obesity) • 2-5 -years: maintain weight until BMI <85 or weight loss not more than 0.5 kg/month (assess that adequate energy diet is obtained) • 6-18years: weight loss not more than 0.9 kg/month 3. BMI >/ 99(severe obesity): • 2-5 years: gradual weight loss not more than 0.5 kg/month. • 6-18 years: gradual loss of weight not more than 0.9 kg/month |
Low
Moderate |
Weak (conditional)
Strong |
Evidence to recommendations: Considerations
The GDG/ GAG was guided by the results of the AGREE II appraisals of the eligible CPGs and thoroughly reviewed the recommendations of the original source WHO CPGs in consideration of local contextual factors related to the national Egyptian health system like burden of the disease, equity, acceptability, feasibility, and other relevant factors. The GDG decided through an informal consensus process to adopt most recommendations. both ETD and changing strength of recommendation were not done in this guideline.
Also, GDG/ GAG develops a good practice statement to improve acceptability and feasibility.
- Acknowledgements
· The GDG/ GAG acknowledge EPG for its help in completing this project.
· We acknowledge WHO, the Australian guidelines and the Committee of Pediatric Obesity of The Korean Society of Pediatric Gastroenterology Hepatology and Nutrition for accepting our requests for permission to adapt their guidelines (the source original guidelines) for their cooperation in providing the permission for adapting our guidelines.
· Finally, we wish the best for all our patients and their families who inspired us. It is for them this work is being finalized.
Funding
· This work is not related to any pharmaceutical or industrial company. The members of the GDG/ GAG and their institutes and universities volunteered their participation and contributions.
- Abbreviations
|
Adolopment |
Adoption-Adaptation-Development |
||
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation Instrument |
||
|
BMI |
Body mass index |
||
|
CPG |
Clinical Practice Guideline |
||
|
DHS |
Demographic and Health Survey |
||
|
EDHS |
Egypt Demographic and Health Survey |
||
|
EMR |
Eastern Mediterranean region |
||
|
ENGC |
Egyptian National Guidelines Committee |
||
|
EPG |
Egyptian Pediatrics Clinical Practice Guidelines Committee |
||
|
EPG CPG |
EPG Clinical Practice Guideline |
||
|
ERG |
External Review Group |
||
|
GAG |
Guideline Adaptation Group |
||
|
GDG |
Guideline Development Group |
||
|
GL |
Guideline |
||
|
GPS |
Good Practice Statement |
||
|
GRADE |
Grading of Recommendations Assessment, Development and Evaluation |
||
|
OPC |
Outpatient clinic |
||
|
PICO |
population, intervention, comparison, and outcomes |
||
|
Patient population, intervention, professionals, outcomes, and healthcare context |
||
|
RCT |
Randomized controlled study |
||
|
RIGHT |
A Reporting Tool for Practice Guidelines in Health Care |
||
|
WHO |
World health organization |
- Glossary
1. Acceptability
Is the extent to which the users are likely to adopt a recommendation, based on internal qualities such as clarity, comprehensiveness, and logical reasoning and on external factors such as the burden imposed on the process and system of care, patient and providers attitudes and beliefs, and patients needs, expectations, and preferences.
2. Adaptation (of guidelines)
Is the systematic approach to considering the use and/or modification of (a) guidelines(s) produced in one cultural and organizational setting for application in different context? Adaptation can be used as an alternative to de novo guideline development or for customizing (an) existing guideline(s) to suit the local context.
3. Adoption (of a guideline)
Is the acceptance of a guideline as a whole after the assessment of its quality, currency, and content. When health care providers (or other users of recommendations) adopt a guideline, they feel committed to change their practices in accordance with the recommendations of the guideline.
4. Admission
Admission, for the purpose of this guideline, refers to a child being registered and entering inpatient care as a patient. This is distinguished from the term “enrolment”, which is used for outpatient care.
5. Applicability
Is the extent to which the users are able to put a recommendation into practice, based on internal qualities such as a clearly defined eligible patient population that matches the population to which the intervention is targeted in the local setting and external factors such as the availability of the necessary knowledge, skills, provider time, staff, equipment, and other resources.
Applicability is sometimes taken as a synonym for feasibility:
Feasibility of the acquisition of necessary skills and knowledge
Feasibility of the necessary increase in provider time, staff, equipment, and so on.
6. Culture
Culture represents the norms and values of a specific group, community, or population.
7. Diffusion
Is a passive means of transferring knowledge; it is not directed towards a target audience (e.g. publication of articles in medical journals).
8. Dissemination
Is more active than diffusion in that it targets a specific audience and involve tailoring the information for that audience (e.g. of dissemination strategies include targeted mailings, presentations, and press conferences.
9. Evidence-based principles
Evidence-Based Medicine (EBM) has been defined as ― the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of EBM means integrating individual clinical expertise with the best available external clinical evidence from systematic research.
10. Evidence tables
Are summaries of the most salient information from studies identified in the systematic review. The elements of evidence tables are dependent on the types of information in studies related to a particular topic but might include information such as the article reference, the study type (e.g. RCT or Cohort), the number of patients and their characteristics, and the intervention, comparison arms, outcome measures, and effect sizes.
11. Guideline or Clinical Practice Guideline (CPG)
Systematically developed statements about specific health problems, intended to assist practitioners and patients in making decisions about appropriate health care.
12. Guideline consistency
Agreement between the evidence and the recommendations, based on the:
Comprehensiveness of the study search and selection process,
Coherence between the results of the studies and their interpretation by the guideline authors, and
Transparency between interpretation and recommendations.
13. Guideline content
In the ‘ADAPTE Manual and Resource Toolkit for Guideline Adaptation’ document, guideline content refers to the recommendations in the source guidelines.
14. Guideline currency
A CPG may be considered up to date ―when (no) new information on interventions, outcomes, and performance justifies updating (it).
15. Guideline quality
By quality of clinical practice guidelines, we mean the confidence that the potential biases of guideline developmentaddressed adequately and that the recommendations are both internally and externally valid, and are feasible for practice. This process involves taking into account the benefits, harms and costs of the recommendations, as well as the practical issues attached to them. Therefore, the assessment (of quality) includes judgments about the methods used for developing the guidelines, the content of the final recommendations, and the factors linked to their uptake.
16. Guideline topic
In the ADAPTE Manual and Resource Toolkit for Guideline Adaptation' document, the topic refers to the theme of the guideline, as described in the guideline title, for a targeted population (disease and patients) and intervention. The purpose, the audience, and the setting intended for the guideline, although not necessarily explicitly stated in the title, are also part of the topic. A guideline on a given topic may contain more than one health question.
17. Health question or clinical question or key question
Is a precisely described health issue (e.g. clinical, professional practice or public health) relating to the topic of the guideline? Guideline may include one or more questions.
18. Implementation
Implementation includes methods to promote the uptake of research findings into routine healthcare in both clinical and policy contexts and hence to improve the quality and effectiveness of healthcare. It includes the study of influences on healthcare professional and organizational behavior.
19. Intra-class correlations
Intra-class correlations provide a measurement of the extent to which two or more raters agree when rating the same set of things. It is a reliability index and is typically a ratio of the variance of interest over the sum of the variance of interest plus error.
20. Recommendation
Any statement that promote or advocate a particular course of action in clinical care.
21. Stakeholder
A stakeholder is an individual, group and/or organization with a stake in your decision to implement a guideline. Stakeholders include individuals or groups who will be directly or indirectly affected by the implementation of a guideline.
22. Source guideline
In the ADAPTE Manual and Resource Toolkit for Guideline Adaptation' document, source guideline refer to those guidelines selected to undergo assessments of quality, currency, content, consistency, and acceptability/applicability and upon which an adapted guideline may be based.
- Introduction
Childhood obesity is one of the most serious public health challenges of the 21st century. The prevalence has increased at an alarming rate, affecting many low- and middle-income countries particularly in urban settings. In 2020, 144 million children were affected by stunting and 47 million children were wasted while 38.3 million children were overweight or obese (1).
Since 1980, the prevalence of obesity has doubled in more than 70 countries and has continuously increased in most other countries. High BMI accounted for 4.0 million deaths globally, nearly 40% of which occurred in people who were not obese. More than two thirds of deaths related to high BMI were due to cardiovascular disease (2).
According to UNICEF report about childhood obesity in Egypt 2015, 39.6 % of males aged 5-9 years were overweight and 15.1% were obese, while 37.9% of females in the same age group were overweight and 11% were obese. In those aged 10-14 years, 34.4 % of males were overweight and 9.9% were obese while the percentage in females of the same age group was 35.4% and 8.5% respectively. In adolescents aged 15-19 years old the percentages of overweight and obese males were 29.4% and 4.9% respectively while 35.9% of females in the same age group were overweight and 8.7% were obese (3). Shafie et al. (4) in 2020, reported a 12.2 and 9.6 % prevalence of overweight and obesity among Egyptian primary school children, respectively.
The increasing prevalence of childhood obesity has led to the emergence of multiple serious obesity-related comorbidities that not only threaten the health of those affected but also promise to place a large strain on the health care system. In addition, obesity in childhood tracks strongly into adulthood, particularly in those with severe obesity and/or a strong family history of obesity (4,5).
Owing to the increasing rates of childhood obesity, the global life expectancy in the United States will, for the first time in recent history, decline, and the American Heart Association has reclassified obesity as a ‘major, modifiable risk factor’ for coronary heart disease (5,6).
Overweight and obesity are defined by WHO as abnormal or excessive fat accumulation that may impair health (6,7). WHO definitions for being overweight and obesity are based on both weight and length/height estimates, i.e. weight-for-length/height and body mass index (BMI) but not mid-upper arm circumference (1).
For children less than 5 years of age, overweight is weight-for-height greater than 2 standard deviations above WHO Child Growth Standards median; and obesity is weight-for-height greater than 3 standard deviations above the WHO Child Growth Standards median. Children and adolescents aged between 5–19 years, overweight is BMI-for-age greater than 1 standard deviation above the WHO Growth Reference median; and obesity is greater than 2 standard deviations above the WHO Growth Reference median is widely accepted that increase in obesity results from an imbalance between energy intake and expenditure, with an increase in positive energy balance being closely associated with the lifestyle adopted and the dietary intake preferences
The genetic factor accounts for less than 5% of cases of childhood obesity. Therefore, while genetics can play a role in the development of obesity, it is not the cause of the dramatic increase in childhood obesity (8).
Childhood obesity can profoundly affect children’s physical health, social, and emotional wellbeing, and self-esteem. It is also associated with poor academic performance and a lower quality of life experienced by the child (9).
Childhood obesity is associated with a higher chance of obesity, premature death and disability in adulthood. But in addition to increased future risks, obese children experience breathing difficulties, increased risk of fractures, hypertension, early markers of cardiovascular disease, insulin resistance and psychological effects (1).
Prevention and treatment of pediatric obesity and complications are key strategic goals, in order to reduce morbidity, mortality, and expected costs for the care of obese adults (10).
Given the multifactorial nature of obesity, preventive interventions should be designed to modify the environmental and social determinants. Health and non-health professionals should be involved in implementing healthy food education and promoting physical activity. To be effective, actions must be multicomponent, multilevel, building agreements, and alliances among many stakeholders, including families, community organizations such as nurseries, schools, sport institutions, health care providers, and teachers (11,12).
The main stay of management is behavior modification that should involve the whole family. (9,13) Pharmacological therapy can only be applied after the failure of the multidisciplinary lifestyle intervention. Bariatric surgery is the ultimate solution in adolescents with morbid obesity and resistant to all other treatments, especially when serious complications are present (10).
This guideline was implemented in order to decrease the prevalence, to manage overweight and obesity and to prevent the future complications related to obesity among Egyptian children to raise a healthy generation.
Purpose and Scope
These guidelines have been developed to standardize the delivery of services and to implement the guidance on the prevention, diagnosis and management of Overweight and Obesity in Children and Adolescents.
It provides guidance to primary health care providers, pediatricians and specially trained nurses.
The guidelines aimed to:
1. Early detection of overweight and obesity in infants, children and adolescents.
- Identification of infants, children and adolescents at high risk of developing overweight and obesity.
- Proper diagnosis of overweight and obesity in the targeted population.
This version of the guideline includes recommendations and good practice statements for
· Management of overweight and obesity in the targeted population.
· Prevention of overweight and obesity in the targeted population.
- Methods
Methods of search:
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation. Keywords used for search are: overweight, obesity, children overweight & adolescents overweight.
Inclusion / exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on methodology of development including the systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated 2013 and later or the last 5 years)
• Selecting peer-reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author
The following three categories of databases and websites were searched:
1. CPG databases and libraries (e.g., GIN, ECRI, SIGN, DynaMed, BIGG-REC PAHO)
2. Bibliographic databases (e.g., PubMed, Google Scholar)
3. Specialized professional societies (related to the pediatric subspecialty)
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least two members. The panel decided a cut-off point or rank the guidelines (any guideline scoring above 60% on the rigor dimension was retained)
After reviewing all the previous criteria the GDG/ GAG recommended using 3 guidelines:
- WHO: Assessing and managing children at primary health care facilities to prevent overweight and obesity in the context of the double burden of malnutrition, 2017,
- The Clinical Practice Guidelines For The Management Of Overweight And Obesity In Adults, Adolescents And Children In Australia, 2013.
- Clinical practice guideline for the diagnosis and treatment of pediatric obesity: recommendations from the Committee on Pediatric Obesity of the Korean Society of Pediatric Gastroenterology Hepatology and Nutrition. Korean J Pediatr. 2019 Jan;62(1):3-21.
We did Adolopment for these guidelines: (Adoption, Adaptation, and Development)
- Adoption for most of the guideline recommendations.
- Development of Good Practice Statement
Contributors to the guideline development process:
Guideline Development Group (GDG)/ Guideline Adaptation Group (GAG):
The GDG/ GAG included two subgroups; the clinicians/ healthcare providers subgroup and the guideline methodologists’ subgroup.
Clinicians Subgroups
The clinicians’ subgroup or clinical panel for this guideline included experts with a range of knowledge, technical skills and diverse perspectives in the field of infant and young child feeding.
The main functions of the clinical panel were adolopment of prevention and management of overweight and obesity in children and adolescents Guidelines, determining the scope of the guideline and guideline, reviewing the evidence, and formulating evidence-informed recommendations in case of changing strength of recommendations.
Guideline Methodologists Subgroup
There were 3 guideline methodologists with expertise in guidelines development, adaptation, GRADE and translation of evidence into recommendations. Methodologists provided orientation and overview of evidence-informed guideline development processes using the GRADE approach, guideline adaptation using the Adapted ADAPTE, provided AGREE II assessment of the source guidelines in collaboration with the clinician’s subgroup, generation of the EtD frameworks whenever applicable.
External Review Group:
The External Review Group for this guideline comprises 2 clinical national experts who have interest and expertise in as well as eminent international reviewers in prevention and management of overweight and obesity in children and adolescents.
They were identified by Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) as people who can provide valuable insights during the guideline development process.
The External Review Group was asked to comment on (peer review) the final guideline to identify any criticism on the content and to comment on clarity and applicability as well as issues relating to implementation, dissemination, ethics, regulations, or monitoring, but not to change the recommendations formulated by the GDG/ GAG. The members of the External Review Group were required to submit declarations of interest before the peer review process.
Guideline Development/ Adaptation Group meetings:
GDG/ GAG meetings were organized virtually (weekly/bimonthly). Due to the extensive scope of the guideline, EPG was responsible for overseeing the adolopment process. the timetable and objectives of each meeting. GDG/ GAG meetings were also attended by members of the methodologists. Working rules for each contributor type were outlined by the chair at the start of each meeting, covering aspects such as vocal rights, voting, and evidence to decision and recommendation formulating processes.
Declarations of interests:
Prospective members of the GDG/ GAG were asked to fill in and sign the standard WHO declaration of interest and confidentiality undertaking forms. All guideline members and methodologists were also asked to fill in and sign the standard WHO declaration-of-interests.
Members of the external review group will be asked to fill in and sign the standard WHO declaration-of-interests form before the peer review process.
Evidence for the guideline:
We used the GRADE system (Grading of Recommendations, Assessment, Development and Evaluation) for assigning the quality of evidence and strength of recommendations that includes the following definitions [15]. Informed by the evidence required for the GRADE Evidence to Decision (EtD) framework(s) was(were) done while considering changing strength of recommendations according to availability of some resources in the recommendations (both ETD and changing strength of recommendation were not done in this guideline).
Description of the interpretation of the GRADE four levels of certainty of evidence:
Table 1. Classification of the Quality of Evidence
|
High |
We are very confident that the true effect lies close to that of the estimate of the effect. |
|
Moderate |
We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. |
|
Low |
Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. |
|
Very Low |
We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of the effect. |
GRADE EtD’s contextual factors, criteria and considerations that link to the strength of recommendations:
Criteria and Considerations:
1. Benefits and harms: When a new recommendation is developed, desirable effects (benefits) need to be weighed against undesirable effects (risks/harms), considering any previous recommendation or another alternative. The larger the gap or gradient in favor of the desirable effects over the undesirable effects, the more likely that a strong recommendation will be made.
2. Certainty of the evidence about the effects: The higher the certainty of the scientific evidence base, the more likely that a strong will be made.
3. Values and preferences: If there is no important uncertainty or variability in how much people value the main outcomes, it is likely that a strong recommendation will be made. Uncertainty or variability around these values that could likely lead to different decisions, is more likely to lead to a conditional recommendation.
4. Economic implications: Lower costs (monetary, infrastructure, equipment or human resources) or greater cost-effectiveness are more likely to support a strong recommendation.
5. Equity and human rights: If an intervention will reduce inequities, improve equity or contribute to the realization of human rights, the greater the likelihood of a strong recommendation.
6. Feasibility: The greater the feasibility of an intervention to all stakeholders, the greater the likelihood of a strong recommendation.
7. Acceptability: If a recommendation is widely supported by health workers and program managers and there is widespread acceptance for implementation within the health service, the likelihood of a strong recommendation is greater.
Table 2. Classification of the Strengths of Recommendations
|
Strong |
The desirable effects of an intervention clearly outweigh the undesirable effects (or vice versa), so most patients should receive the recommended course of action. |
|
Conditional |
There is uncertainty about the trade-offs. The clinician and patient need to discuss the patient's values and preferences, and the decision should be individualized. |
Developing good practice statements:
The GDG/ GAG also developed good practice statements for this guideline, which are actionable messages relevant to the guideline questions. The justification for each good practice statement was carefully considered by the GDG/ GAG with an emphasis that they are clearly needed. Good practice statements were developed, guided by the following GRADE criteria:
1- Message is really necessary with regard to actual healthcare practice
2- Have large net positive consequence (relevant outcomes and downstream consequences) (GRADE EtD domains)
3- Collecting and summarizing the evidence is a poor use of time and resources
4- Include awell-documented, clear rationale connecting indirect evidence
5- Are clear and actionable statements.
The GDG/ GAG collectively drafted and finalized good practice statements with relevant justifications and remarks to help with their interpretation, with close support and input from the consultant and guideline methodologists.
We have used the Reporting Items for Practice Guidelines in Healthcare (RIGHT) extension for adapted guidelines (RIGHT-Ad@pt Tool) as a reporting checklist for this guideline adaptation process as recommended by the EQUATOR network.
- Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing prevention and management of overweight and obesity in children and adolescents strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of nutritional care delivery, care gaps and current needs.
3. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
4. Identify barriers to, and facilitators of implementation.
5. Select an implementation framework and its component strategies.
6. Develop a step-by-step implementation plan:
· Select the target populations and evaluate the outcome.
· Identify the local resources to support the implementation.
· Set timelines.
· Distribute the tasks to the members.
· Evaluate the outcomes.
7. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
· Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
· Educational materials: printed or electronic information (software).
· Web-based education: computer-based educational activities.
· A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
· Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
· Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
· Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
· Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
· Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behaviors.
· Mass media campaigns.
3. For Nurses
· Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
· Educational materials: printed.
· A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
· Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
· Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
· Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
· Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
· Administrative policies and procedures.
· Formularies: Drug safety programs, electronic medication administration records.
5.Other activities to assist the implementation of the adapted guideline’s recommendations include:
· International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
· Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
Evidence to Decision Tables: (if any)
Guideline Implementation Tools
Educational materials based on this Adapted CPG for prevention and management of overweight and obesity in children and adolescents have been made available in several forms including:
• Educational materials based on this Adapted CPG are made available in several forms, including
- Booklet with executive summary of guidelines for physicians and primary health care professionals.
Limitations and suggestions for further research needs
Future research recommendations for prevention and management of overweight and obesity in children and adolescents in the Egyptian context could include:
· Epidemiological studies on prevalence of overweight and obesity.
· Further studies on pharmacological & surgical rôle in obesity in children and adolescents.
These recommendations aim to address specific challenges and characteristics of the Egyptian context, potentially leading to more effective prevention and management strategies for overweight and obesity in children and adolescents.
Challenges
· Media promotion for Junk food.
· Pharmacological options limitation of use in pediatrics & limited resources for evidence.
Strengthen the evidence base of the next update of this guideline by generating GRADE summary of finding tables, evidence profiles, and EtD frameworks.
Monitoring and evaluating the impact of the guideline.
The following are three performance measures or indicators for implementing this adapted CPG for prevention and management of overweight and obesity in children and adolescents:
1. Adherence to prevention and management of overweight and obesity in children and adolescent Guidelines
· Numerator: Number of children with overweight and obesity who received treatment as per guideline recommendations.
· Denominator: Total number of children diagnosed with overweight and obesity.
· Data Source: Hospital or clinic patient records.
2. Duration of Hospital Stay
· Numerator: Total number of hospital stay days for children with overweight and obesity.
· Denominator: Total number of children admitted with overweight and obesity.
· Data Source: Hospital admission and discharge records.
3. Rate of Readmission
· Numerator: Number of children readmitted with symptoms of overweight and obesity within a certain period (e.g., 30 days) after discharge.
· Denominator: Total number of children initially admitted with overweight and obesity.
· Data Source: Hospital readmission records.
These key performance indicators are designed to measure the effectiveness and adherence to the guidelines, the efficiency of the treatment in terms of resource utilization (hospital stay), and the success of the treatment in preventing further complications (readmissions).
Updating of the guideline
The EPG prevention and management of overweight and obesity in children and adolescents GAG has decided to conduct the next review of this adapted CPG for updates after five years. This should be carried out in 2029 after checking for updates in the source CPGs, consultation of expert opinion on the changes needed for updating according to the newest evidence and recommendations published in this area and the clinical audit and feedback from implementation efforts in the aforementioned local healthcare settings except if any breakthrough evidence- based recommendations are published before that date. The process will be guided by the Checklist for the Reporting of Updated Guidelines (CheckUp) Tool that is freely provided by the AGREE Enterprise and by the Reporting Items for Practice Guidelines in Healthcare (RIGHT) extension for adapted guidelines RIGHT-Ad@pt Checklist.
- References
1. WHO. Noncommunicable diseases: Childhood overweight and obesity19 October 2020 | Q&A.
2. 2. Afshin A, Forouzanfar M Marissa B Reitsma et al., (2017): Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N Engl J Med 2017;377:13-27. DOI: 10.1056/NEJMoa1614362
3. 3.United Nations Children's Fund, Egypt : Children in Egypt: a statistical digest, UNICEF Egypt, Cairo, Egypt, June 2015
4. 4.El-Shafie AM, Kasemy ZA, Omar ZA, Alkalash SH, Salama AA, Mahrous KS, et al. Prevalence of short stature and malnutrition among Egyptian primary school children and their coexistence with Anemia. Ital J Pediatr. 2020 Jun 29;46(1):91
5. 5.Seema Kumar, and Aaron S. Kelly: Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment, Mayo Clin Proc. 2017;92(2):251-265
6. 6.Luc F. Van Gaal, Ilse L. Mertens & Christophe E. De Block: Mechanisms linking obesity with cardiovascular disease, NATURE|Vol 444|14 December 2006.
7. WHO: Obesity and overweight, Key facts, 1 April 2020.
8. 7Krushnapriya Sahoo, Bishnupriya Sahoo, Ashok Kumar Choudhury, Nighat Yasin Sofi, Raman Kumar, and Ajeet Singh Bhadoria. Childhood obesity: causes and consequences. J Family Med Prim Care. 2015 Apr-Jun; 4(2): 187–192doi: 10.4103/2249-4863.154628
9. 8.Anderson PM, Butcher KE. Childhood obesity: Trends and potential causes. Future Child 2006;16:1945.
10.10. Valerio et al. Italian Journal of Pediatrics (2018): Diagnosis, treatment and prevention of pediatric obesity: consensus position statement of the Italian Society for Pediatric Endocrinology and Diabetology and the Italian Society of Pediatrics 44:88 doi.org/10.1186/s13052-018-0525-6
11. 11.Novak NL, Brownell KD. Role of policy and government in the obesity epidemic. Circulation. 2012;126:2345–52.
12. 12. Branca F, Nikogosian H, Lobstein T The Regional Office for Europe of the World Health Organization. The challenge of obesity in the WHO European Region and the strategies for response. Summary., editors. World Health Organization; 2007.
13. 13- August GP, Caprio S, Fennoy I, et al. Prevention and treatment of pediatric obesity: an endocrine society clinical practice guideline based on expert opinion. J Clin Endocrinol Metab. 2008;93:4576–99.
14. Abdel Baky A, Omar TEI, Amer YS; Egyptian Pediatric Clinical Practice Guidelines Committee (EPG). Adapting global evidence-based practice guidelines to the Egyptian healthcare context: the Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) initiative. Bull Natl Res Cent. 2023;47(1):88. https://doi.org/10.1186%2Fs42269-023-01059-0
15. Alshehri A, Almazrou S, Amer Y. Methodological frameworks for adapting global practice guidelines to national context in the Eastern Mediterranean Region. Eastern Mediterranean Health Journal. 2023 Jul 1;29(7). https://www.emro.who.int/emhj-volume-29-2023/volume-29-issue-7/methodological-frameworks-for-adapting-global-practice-guidelines-to-national-context-in-the-eastern-mediterranean-region.html
16. Schünemann H, Brozek J, Guyatt G, Oxman A (editors). GRADE handbook: handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group; 2013 (Online updated version: https://gdt.gradepro.org/app/handbook/handbook.html Accessed 16/8/2024)
17. Klugar M, Lotfi T, Darzi AJ, et al. GRADE Guidance 39: Using GRADE-ADOLOPMENT to adopt, adapt or create contextualized recommendations from source guidelines and evidence syntheses. Journal of Clinical Epidemiology. 2024 Aug 6:111494. https://doi.org/10.1016/j.jclinepi.2024.111494 (in press)
18. Amer YS, Elzalabany MM, Omar TI, Ibrahim AG, Dowidar NL. The ‘Adapted ADAPTE’: an approach to improve utilization of the ADAPTE guideline adaptation resource toolkit in the A lexandria C enter for E vidence‐B ased C linical P ractice G uidelines. Journal of evaluation in clinical practice. 2015 Dec;21(6):1095-106. https://doi.org/10.1111/jep.12479
19. Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. https://doi.org/10.1503%2Fcmaj.090449
20. Agree II (2022) AGREE Enterprise website. Available at: https://www.agreetrust.org/resource-centre/agree-ii/ (Accessed: 16/8/2024).
21. Song Y, Alonso-Coello P, Ballesteros M, et al. A Reporting Tool for Adapted Guidelines in Health Care: The RIGHT-Ad@pt Checklist[J]. Annals of Internal Medicine, 2022, 175(5):710-719. https://doi.org/10.7326/M21-4352 (Official RIGHT Statement Website: http://www.right-statement.org/extensions/13 Accessed 16/8/2024).
- Annexes
Annex Table 1.
Declaration of Conflict of Interests
The members of the guideline development/ adaptation group and the external review group have no academic, financial, or competing interests to declare and none of them were involved in the development of the original source guideline(s).
Any identified potential COI has been reported below.
|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Adaptation Group (Clinical subgroup) |
|||
|
Name |
Affiliation, Area of expertise / Role, Country / Primary location [work] |
Declaration of interests |
|
|
Interest identified |
Management plan & decision |
||
|
Sanaa Youssef Shaaban |
Prof of Pediatrics, Ain shams University |
None |
Not Applicable |
|
Ehab Khairy El khashab |
Professor of Pediatrics, Ain Shams University |
None |
Not Applicable |
|
Enas Raafat |
Professor of child health, National Research Center |
None |
Not Applicable |
|
Gihan Mohamed Bebars |
Professor of Pediatrics. Menia University |
None |
Not Applicable |
|
Hanna Aboulghar |
Professor of Pediatrics, Cairo University |
None |
Not Applicable |
|
Khalil Abd El Khalek |
Professor of Pediatrics, Cairo University |
None |
Not Applicable |
|
Osama M Al-Asheer |
Professor of Pediatrics, Assuit University |
None |
Not Applicable |
|
Sameh Tawfik |
Professor of Pediatrics, AFCM |
None |
Not Applicable |
|
Shereen Abdelghaffar |
Professor of Pediatrics Cairo University |
None |
Not Applicable |
|
Omnia Omar |
Assistant Professor of Pediatrics, Alexandria University |
None |
Not Applicable |
|
Yasmin Gamal El Gendy |
Assistant Professor of Pediatrics and Clinical Nutrition, Ain Shams University, AFCM |
None |
Not Applicable |
|
Christine George |
Lecturer of Pediatrics, Cairo University |
None |
Not Applicable |
|
Guideline Adaptation Group (Methodology Subgroup) |
|||
|
Prof. Ashraf Abdel Baky |
Professor of Pediatrics Ain Shams University, Egypt Founder and Chair of EPG |
None |
Not Applicable |
|
Dr. Yasser Sami Amer |
1. Pediatrics Department and Clinical Practice Guidelines and Quality Research Unit, Quality Management Department, King Saud University Medical City, Riyadh, Saudi Arabia; 2. Research Chair for Evidence-Based Health Care and Knowledge Translation, King Saud University, Riyadh, Saudi Arabia; 3. Chair, Adaptation Working Group, Guidelines International Network (GIN), Perth, Scotland 4. Department of Internal Medicine, Ribeirão Preto Medical School, University of São Paulo (FMRP-USP), Ribeirão Preto, São Paulo, Brazil. |
None |
Not Applicable |
|
Lecturer of Pediatrics, Faculty of Medicine, Modern University for Technology and Information (MTI), Egypt |
None |
Not Applicable |
|
|
External Review Group |
|||
|
Prof. Mona Salem |
Ain shams university |
None |
Not Applicable |
|
Prof. Gehan Foad |
National nutrition institute |
None |
Not Applicable |
|
External Reviewer for methodology |
|||
|
Prof. Iván D. Flórez |
Department of Pediatrics, University of Antioquia, Medellín, Colombia, Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Canada, Leader, AGREE Collaboration (Appraisal of Guidelines for Research & Evaluation) Director, Cochrane Colombia |
None |
Not Applicable |
|
Prof. Airton Tetelbom Stein
|
Professor Titular de Saúde Coletiva, Fundação Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), Porto Alegre, Brazil Professor Adjunto, Universidade Luterana do Brasil (Ulbra), Canoas, Brazil Coordenador de Diretrizes Clínicas, Grupo Hospitalar Conceição, Porto Alegre, Brazil 4. Member, Board of Trustees, Guidelines International Network (G-I-N) |
None |
Not Applicable |
Web annexes
The following annexes can be added as a package of standalone supplementary documents.
Keywords: The MeSH terms for "Guideline for the prevention and management of overweight and obesity on PubMed are: overweight, obesity, children overweight & adolescents overweight.
Annex Table 3. Annex Nurses and Parents Educational Guide in Ar
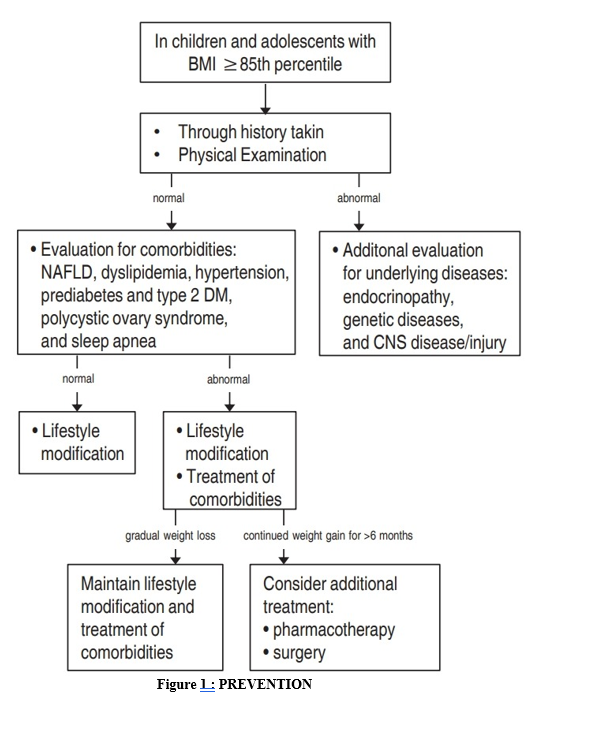
Stepwise assessment and treatment strategies for overweight and obesity children and adolescents. BMI, body mass index; CNS, central nervous system; NAFLD, nonalcoholic fatty liver disease; DM, diabetes mellitus.
Appendix Table 4. The RIGHT-Ad@pt checklist
|
|||||
|
7 sections, 27 topics, and 34 items |
Assessment |
Page(s)* |
Note(s) |
||
|
BASIC INFORMATION |
|||||
|
Title/subtitle |
|||||
|
1 |
Identify the report as an adaptation of practice guideline(s), that is include "guideline adaptation", "adapting", "adapted guideline/recommendation(s)", or similar terminology in the title/subtitle. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
2 |
Describe the topic/focus/scope of the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Cover/first page |
|||||
|
3 |
Report the respective dates of publication and the literature search of the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
4 |
Describe the developer and country/region of the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Executive summary/abstract |
|||||
|
5 |
Provide a summary of the recommendations contained in the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Abbreviations and acronyms |
|||||
|
6 |
Define key terms and provide a list of abbreviations and acronyms (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Contact information of the guideline adaptation group |
|||||
|
7 |
Report the contact information of the developer of the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
SCOPE |
|||||
|
Source guideline(s) |
|||||
|
8 |
Report the name and year of publication of the source guideline(s), provide the citation(s), and whether source authors were contacted. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Brief description of the health problem(s) |
|||||
|
9 |
Provide the basic epidemiological information about the problem (including the associated burden), health systems relevant issues, and note any relevant differences compared to the source guideline(s).
|
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Aim(s) and specific objectives |
|||||
|
10 |
Describe the aim(s) of the adapted guideline and specific objectives, and note any relevant differences compared to the source guideline(s). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Target population(s) |
|||||
|
11 |
Describe the target population(s) and subgroup(s) (if applicable) to which the recommendation(s) is addressed in the adapted guideline, and note any relevant differences compared to the source guideline(s). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
End-users and settings |
|||||
|
12 |
Describe the intended target users of the adapted guideline, and note any relevant differences compared to the source guideline(s). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
13 |
Describe the setting(s) for which the adapted guideline is intended, and note any relevant differences compared to the source guideline(s). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
RIGOR OF DEVELOPMENT |
|||||
|
Guideline adaptation group |
|||||
|
14 |
List all contributors to the guideline adaptation process and describe their selection process and responsibilities. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Adaptation framework/methodology |
|||||
|
15 |
Report which framework or methodology was used in the guideline adaptation process. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Source guideline(s) |
|||||
|
16 |
Describe how the specific source guideline(s) was(were) selected. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Key questions |
|||||
|
17 |
State the key questions of the adapted guideline using a structured format, such as PICO (population, intervention, comparator, and outcome), or another format as appropriate. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
18 |
Describe how the key questions were developed/modified, and/or prioritized. |
☐ Yes ☒ No ☐ Unclear |
|
|
|
|
Source recommendation(s) |
|||||
|
19 |
Describe how the recommendation(s) from the source guideline(s) was(were) assessed with respect to the evidence considered for the different criteria, the judgements and considerations made by the original panel. |
☐ Yes ☒ No ☐ Unclear |
|
|
|
|
Evidence synthesis |
|||||
|
20 |
Indicate whether the adapted recommendation(s) is/are based on existing evidence from the source guideline(s), and/or additional evidence. |
☐ Yes ☒ No ☐ Unclear |
|
|
|
|
21 |
If new research evidence was used, describe how it was identified and assessed. |
☐ Yes ☒ No ☐ Unclear |
NA |
|
|
|
Assessment of the certainty of the body of evidence and strength of recommendation |
|||||
|
22 |
Describe the approach used to assess the certainty/quality of the body/ies of evidence and the strength of recommendations in the adapted guideline and note any differences (if applicable) compared to the source guideline(s). |
☐ Yes ☒ No ☐ Unclear |
NA |
|
|
|
Decision-making processes |
|||||
|
23 |
Describe the processes used by the guideline adaptation group to make decisions, particularly the formulation of recommendations.
|
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
RECOMMENDATIONS |
|||||
|
Recommendations |
|||||
|
24 |
Report recommendations and indicate whether they were adapted, adopted, or de novo. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
25 |
Indicate the direction and strength of the recommendations and the certainty/quality of the supporting evidence and note any differences compared to the source recommendations(s) (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
26 |
Present separate recommendations for important subgroups if the evidence suggests important differences in factors influencing recommendations and note any differences compared to the source recommendations(s) (If applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Rationale/explanation for recommendations |
|||||
|
27 |
Describe the criteria/factors that were considered to formulate the recommendations or note any relevant differences compared to the source guideline(s) (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
EXTERNAL REVIEW AND QUALITY ASSURANCE |
|||||
|
External review |
|||||
|
28 |
Indicate whether the adapted guideline underwent an independent external review. If yes, describe the process. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Organizational approval |
|||||
|
29 |
Indicate whether the adapted guideline obtained organizational approval. If yes, describe the process. |
☒ Yes ☐ No ☐ Unclear |
SNS & NEBMC |
|
|
|
FUNDING, DECLARATION, AND MANAGEMENT OF INTEREST |
|||||
|
Funding source(s) and funder role(s) |
|||||
|
30 |
Report all sources of funding for the adapted guideline and source guideline(s), and the role of the funders. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Declaration and management of interests |
|||||
|
31 |
Report all conflicts of interest of the adapted and the source guideline(s) panels, and how they were evaluated and managed. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
OTHER INFORMATION |
|||||
|
Implementation |
|||||
|
32 |
Describe the potential barriers and strategies for implementing the recommendations (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Update |
|||||
|
33 |
Briefly describe the strategy for updating the adapted guideline (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Limitations and suggestions for further research |
|||||
|
34 |
Describe the challenges of the adaptation process, the limitations of the evidence, and provide suggestions for future research. |
☐ Yes ☒ No ☐ Unclear |
-- |
|
|