the Management of Achalasia
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | جراحه عامه |
| كتاب: | the Management of Achalasia |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:03 AM |
الوصف
"last update:
7 Sep 2025" Download Guideline
- Executive Summary
Achalasia is a primary motor disorder of the oesophagus characterised by absence of peristalsis and insufficient lower oesophageal sphincter relaxation. With new advances and developments in achalasia management, there is an increasing demand for comprehensive evidence-based guidelines to assist clinicians in achalasia patient care.
These guidelines describe the management of achalasia including diagnosis and treatment.
Our recommendations are:
- In patients who are initially suspected of having GERD but do not respond to acid-suppressive therapy, we suggest evaluation for achalasia, (Conditional recommendation).
- We recommend using High Resolution Manometry (HRM) over conventional line tracing for the diagnosis of achalasia, (Strong recommendation).
- We suggest using a barium esophagogram to diagnose achalasia if manometry is unavailable, although it is less sensitive than oesophageal manometry. The working group suggests using Timed Barium Esophagogram (TBE), if available, over standard barium esophagogram, (Conditional recommendation).
- We recommend performing endoscopy in all patients with symptoms suggestive of achalasia to exclude other diseases, (Strong recommendation).
- We recommend against making the diagnosis of achalasia solely based on endoscopy, (Good practice statement).
- We suggest that classifying achalasia subtypes by the Chicago Classification may help inform prognosis and treatment choice, (Conditional recommendation).
- We recommend against the use of calcium blockers, phosphodiesterase inhibitors or nitrates for the treatment of achalasia, (Good practice statement).
- We recommend against medical therapy or Botulinum toxin injection as definitive treatment of achalasia. (Strong recommendation).
· We recommend botulinum toxin injection as first-line therapy for patients with achalasia that are unfit for definitive therapies compared with other less-effective pharmacological therapies, (Good practice statement).
- We suggest that POEM, PD or LHM result in comparable symptomatic improvement in patients with early achalasia, (Conditional recommendation).
- We recommend POEM or laparoscopic Heller myotomy for management of patients with achalasia types I and II, and the treatment option should be based on shared decision-making between the patient and provider, (Strong recommendation).
- We recommend tailored POEM or LHM for type III achalasia as a more efficacious alternative disruptive therapy at the LES compared to PD, (Strong recommendation).
- We suggest that patients undergoing POEM are counselled regarding the increased risk of post procedural reflux compared with pneumatic dilation and laparoscopic Heller myotomy. The choice is based on patient preferences and physician expertise, (Conditional recommendation).
- We recommend myotomy with fundoplication in controlling distal esophageal acid exposure, (Strong recommendation).
- We suggest either Dor or Toupet fundoplication to control esophageal acid exposure in patients with achalasia undergoing surgical myotomy, (Conditional recommendation).
- We recommend against stent placement for management of long-term dysphagia in patients with achalasia, (Strong recommendation).
- We recommend against obtaining routine gastrograffin esophagogram after dilatation. This test should be reserved for patients with a clinical suspicion for perforation after dilation, (Strong recommendation).
- We suggest that Eckardt Score (ES) or HRM alone not be used to define treatment failure in evaluating continued or recurrent symptoms after definitive therapy for achalasia, (Conditional recommendation).
- Patients with recurrent or persistent dysphagia after initial treatment should undergo repeat evaluation with TBE and upper endoscopy with or without oesophageal manometry, (Good practice statement).
- Post procedural management of reflux options include objective testing for esophageal acid exposure, long-term acid suppressive therapy, and surveillance upper endoscopy, (Conditional recommendation).
- We suggest treating recurrent or persistent dysphagia after LHM with PD, POEM or redo surgery, (Conditional recommendation).
- We suggest that PD is appropriate for patients with achalasia post-initial surgical myotomy or POEM in need of retreatment, (Conditional recommendation).
- We suggest that POEM is an option in patients with achalasia who have previously undergone PD or LHM, (Conditional recommendation).
- We suggest that Heller myotomy be considered before esophagectomy in patients who have failed PD and POEM and there is evidence of incomplete myotomy, (Conditional Recommendation).
- We suggest esophagectomy or cardioplasty in surgically-fit patients with megaesophagus, (Good practice statement).
- We suggest against routine endoscopic surveillance for esophageal carcinoma in patients with achalasia, (Conditional recommendation).
- Recommendations
Section I. Diagnosis of Achalasia:
- In patients who are initially suspected of having GERD but do not respond to acid-suppressive therapy, we suggest evaluation for achalasia, (Conditional recommendation, low certainty evidence, (1)).
- We recommend using High Resolution Manometry (HRM) over conventional line tracing for the diagnosis of achalasia, (Strong recommendation, moderate certainty evidence, (3)).
- We suggest using a barium esophagogram to diagnose achalasia if manometry is unavailable, although it is less sensitive than oesophageal manometry. The working group suggests using Timed Barium Esophagogram (TBE), if available, over standard barium esophagogram, (Conditional recommendation, moderate certainty evidence, (3)).
- We recommend performing endoscopy in all patients with symptoms suggestive of achalasia to exclude other diseases, (Strong recommendation, low certainty evidence, (3)).
- We recommend against making the diagnosis of achalasia solely based on endoscopy, (Good practice statement).
- We suggest that classifying achalasia subtypes by the Chicago Classification may help inform prognosis and treatment choice, (Conditional recommendation, low certainty evidence, (1)).
Section II. Medical Treatment of Achalasia:
- We recommend against the use of calcium blockers, phosphodiesterase inhibitors or nitrates for the treatment of achalasia, (Good practice statement).
- We recommend against medical therapy or Botulinum toxin injection as definitive treatment of achalasia. (Strong recommendation, moderate certainty evidence, (2)).
· We recommend botulinum toxin injection as first-line therapy for patients with achalasia that are unfit for definitive therapies compared with other less-effective pharmacological therapies, (Good practice statement).
Section III. Endoscopic Treatment of Achalasia:
- We suggest that POEM, PD or LHM result in comparable symptomatic improvement in patients with early achalasia, (Conditional recommendation, moderate certainty evidence, (1)).
- We recommend POEM or laparoscopic Heller myotomy for management of patients with achalasia types I and II, and the treatment option should be based on shared decision-making between the patient and provider, (Strong recommendation, moderate certainty evidence, (2)).
- We recommend tailored POEM or LHM for type III achalasia as a more efficacious alternative disruptive therapy at the LES compared to PD, (Strong recommendation, moderate certainty evidence, (1)).
- We suggest that patients undergoing POEM are counselled regarding the increased risk of post procedural reflux compared with pneumatic dilation and laparoscopic Heller myotomy. The choice is based on patient preferences and physician expertise, (Conditional recommendation, moderate certainty evidence, (1)).
Section IV. Surgical Treatment of Achalasia:
- We recommend myotomy with fundoplication in controlling distal esophageal acid exposure, (Strong recommendation, moderate certainty evidence, (1)).
- We suggest either Dor or Toupet fundoplication to control esophageal acid exposure in patients with achalasia undergoing surgical myotomy, (Conditional recommendation, moderate certainty evidence, (1)).
- We recommend against stent placement for management of long-term dysphagia in patients with achalasia, (Strong recommendation, moderate certainty evidence, (1)).
Section V. Post-Therapy Assessment:
- We recommend against obtaining routine gastrograffin esophagogram after dilatation. This test should be reserved for patients with a clinical suspicion for perforation after dilation, (Strong recommendation, low certainty evidence, (1)).
- We suggest that Eckardt Score (ES) or HRM alone not be used to define treatment failure in evaluating continued or recurrent symptoms after definitive therapy for achalasia, (Conditional recommendation, low certainty evidence, (1)).
- Patients with recurrent or persistent dysphagia after initial treatment should undergo repeat evaluation with TBE and upper endoscopy with or without oesophageal manometry, (Good practice statement).
- Post procedural management of reflux options include objective testing for esophageal acid exposure, long-term acid suppressive therapy, and surveillance upper endoscopy, (Conditional recommendation, low certainty evidence, (3)).
Section VI. Post-Failed Initial Therapies or Megaesophagus:
- We suggest treating recurrent or persistent dysphagia after LHM with PD, POEM or redo surgery, (Conditional recommendation, low certainty evidence, (3)).
- We suggest that PD is appropriate for patients with achalasia post-initial surgical myotomy or POEM in need of retreatment, (Conditional recommendation, low certainty evidence, (3)).
- We suggest that POEM is an option in patients with achalasia who have previously undergone PD or LHM, (Conditional recommendation, low certainty evidence, (1)).
- We suggest that Heller myotomy be considered before esophagectomy in patients who have failed PD and POEM and there is evidence of incomplete myotomy, (Conditional Recommendation, low certainty evidence, (1)).
- We suggest esophagectomy or cardioplasty in surgically fit patients with megaesophagus, (Good practice statement).
Section VII. Cancer Surveillance:
- We suggest against routine endoscopic surveillance for esophageal carcinoma in patients with achalasia, (Conditional recommendation, low certainty evidence, (1)).
Research Needs:
· Comparison between esophagectomy with gastric pull-up and laparoscopic cardioplasty for advanced achalasia or megaesophagus
· Comparison between POEM and LHM for the treatment of achalasia
· Comparison between laparoscopic cardioplasty for achalasia with and without Toupet antireflux procedure
· Should the result of HRM influence the choice of treatment modality for achalasia?
- Acknowledgement
We would like to acknowledge the Guideline General Surgery, (GGS) committee for developing this guideline.
Chair of GGS: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University.
Moderator of GGS: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University.
Members of GGS (Alphabetically):
Abel-Motey Hussein Aly, Professor of Surgery, Cairo University.
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University.
Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University.
Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University.
Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University.
Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University.
Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
|
AGRREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
ES |
Eckardt Score |
|
GERD |
Gastro-Esophageal Reflux Disease |
|
GGS |
Guidelines General Surgery (committee) |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation |
|
HRM |
High Resolution Manometry |
|
LES |
Lower Esophageal Sphincter |
|
LHM |
Laparoscopic Heller’s Myotomy |
|
PD |
Pneumatic Dilatation |
|
POEM |
Per-Oral Endoscopic Myotomy |
|
TBE |
Timed Barium Esophagogram |
- Introduction
Achalasia is a primary esophageal motor disorder of unknown etiology characterized by degeneration of the myenteric plexus, which results in impaired relaxation of the esophagogastric junction (EGJ), along with the loss of organized peristalsis in the esophageal body. The criterion standard for diagnosing achalasia is higher solution esophageal manometry showing incomplete relaxation of the EGJ coupled with the absence of organized peristalsis. Three achalasia subtypes have been defined based on high-resolution manometry findings in the esophageal body, (1).
Other treatment options include botulinum toxin injection, pneumatic dilation, and Heller myotomy. Esophageal motor abnormalities in achalasia lead to symptoms of dysphagia for solids and liquids without oropharyngeal transfer difficulties in roughly 90% of patients, regurgitation in 75%, weight loss in 60%, chest pain in 50%, and heartburn in 40%, (2).
Treatment of patients with achalasia has evolved in recent years with the introduction of peroral endoscopic myotomy, (2).
- Scope and Purpose
The scope of this guideline is set recommendations for the diagnosis and treatment of achalasia. The main purpose of these guidelines is to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the good surgical practice to our patients, and finally to be cost effective.
- Target Audience
The principle targeted candidates are the practicing surgeons, however endoscopists and radiologists and all specialists involved in the treatment of achalasia are also included.
- Methods
A comprehensive search for guidelines was undertaken to identify the relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2020 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GGS decided to adapt the ACG Clinical Guidelines: Diagnosis and Management of Achalasia 2020; ASGE Guideline on the Management of Achalasia 2020; and Europian Guidelines on Achalasia: United European Gastroenterology and European Society of Neurogastroenterology and Motility recommendations 2020, (1 - 3).
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
GRADE working group: https://www.gradeworkinggroup.org/
GRADE online training modules: http://cebgrade.mcmaster.ca/
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’ or ‘Low’ (table 1& 2).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
these are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Clinical Indicators for Monitoring
1) Upper endoscopy.
2) Esophageal manometry study.
3) Barium Studies
- Updating of the Guideline
The GGS committee for guidelines development is responsible for the continuous evaluation of evidence available about achalasia. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1: Quality and Significance of the Four Levels of Evidence in
GRADE
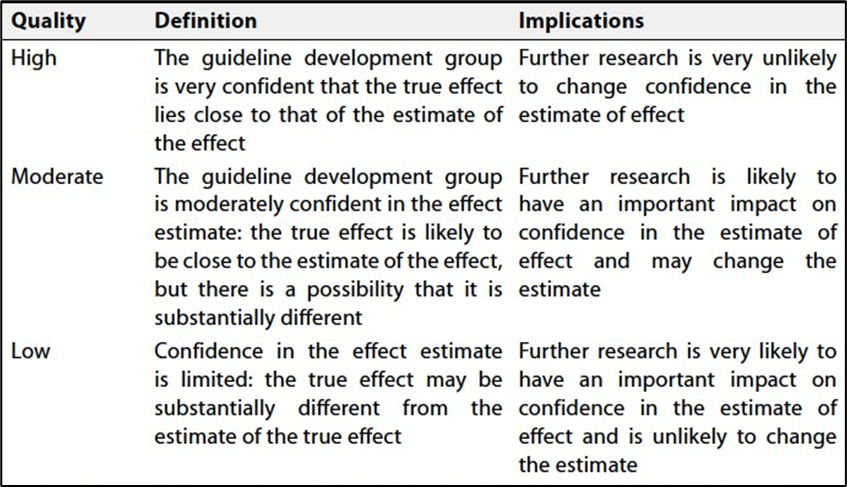
Table 2: Factors that
Determine How to Upgrade or Downgrade the Quality of Evidence
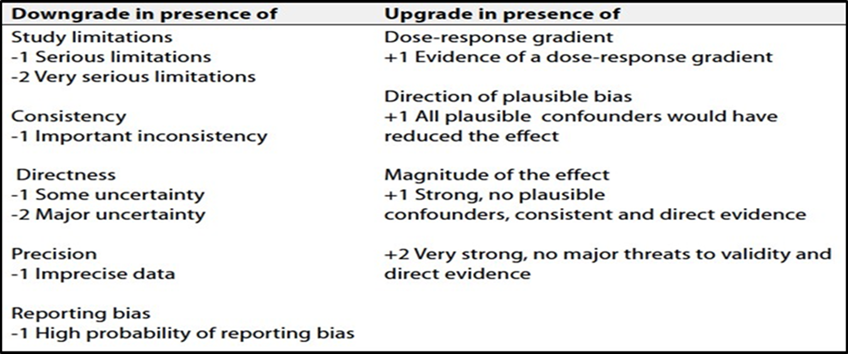
Table 3: Eckardt score: clinical scoring for achalasia4
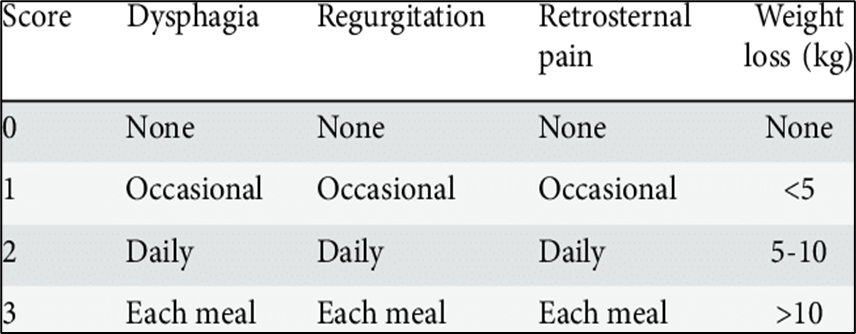
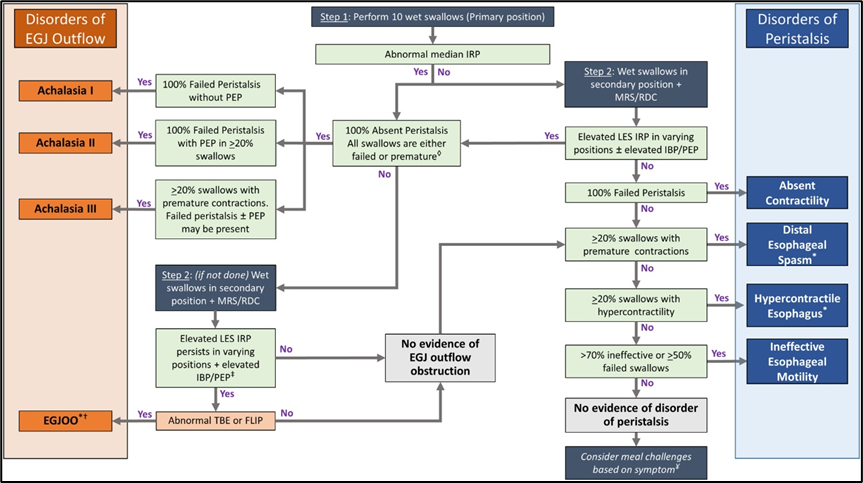
Figure 1: Chicago Classification for Achalasia version 4.0©5
- References
- ACG Clinical Guidelines: Diagnosis and Management of Achalasia. Am J Gastroenterol 2020; Vol. 115: 1393–1411.
- ASGE Guideline on the Management of Achalasia. Gastrointestinal Endoscopy 2020; Vol. 91(2): 213-227e6
- Europian Guidelines on Achalasia: United European Gastroenterology and European Society of Neurogastroenterology and Motility recommendations. United European Gastroenterology Journal 2020; Vol. 8(1): 13–33
- Treatment of achalasia in the era of high-resolution manometry - Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/figure/Eckardt-score-clinical-scoring-for-achalasia_tbl1_279532358
- Esophageal motility disorders on high-resolution manometry: Chicago classification version 4.0©. Neurogastroenterol Motil, 2021 Jan;33(1):e14058. doi: 10.1111/nmo.14058