Urinary Tract Infection
| Site: | EHC | Egyptian Health Council |
| Course: | Urology Surgery Guidelines |
| Book: | Urinary Tract Infection |
| Printed by: | Guest user |
| Date: | Saturday, 27 June 2026, 5:16 PM |
Description
"last update:
7 Sep 2025" Download Guideline
- Acknowledgement
Steering Panel (in alphabetical order)
1. Prof. Mohamed Sherif Mourad, Ain Shams University (Chair of Panel)
2. Prof. Mohamed Ahmed Shalaby, Assiut University
3. Prof. Mohamed Rafik El Halaby, Ain Shams University
4. Prof. Ahmed Aly Morsy, Cairo University
5. Prof. Hassan Abo Elenein, Mansoura University
6. Prof. Hisham Hammouda, Assiut University
7. Prof. AbdelNasser El Gamasy, Tanta University
8. Prof. Ahmed El Baz, Tudor Bilhartz Institute
9. Prof. Hamada Nassar, Damanhour Institute
10. Prof. Mohamed Wageih, Kobry El kobba Military Hospital
Guidelines Development Group of urological infection committee
1) Prof. Mostafa Khalil, professor of urology (Benha University) (Chair)
2) Prof. Tarek R Eleithy, professor of urology (Theodor Bilharz Research institute) Prof. Shabieb Ahmed, professor of urology (Benha University)
3) Prof. Rabea Gomaa, professor of urology (Benha University)
4) Ass,Prof. Hossam Elawady, assistant professor of urology (Ain shams university) Ass,Prof. Hussein Shaher, assistant professor of urology (Benha University)
5) Ass.Prof. Mohamed Abuelnaga, assistant professor of urology (Ain shams university) Ass,Prof. Amany Kasem. assistant professor of microbiology (Benha University)
6) Dr. Kareem Nouh, lecturer of urology (Benha University)
- Executive Summary
These guidelines provide essential summarized updated information for diagnosis, treatment and prevention of urinary tract Infections with emphasizing on judicious use of antimicrobials based on culture and sensitivity to reduce bacterial resistance which is a serious issue especially with malpractice and misuse of antibiotics in Egypt. Moreover, the recommendations included in these guidelines are not representing absolute mandates but provisional protocols respecting environmental and socioeconomic conditions of Egypt, considering our religious and traditional background
1. Diagnosis of ABU is made by urine culture, either properly collected clean-catch specimen or a catheterized specimen is acceptable. (Strong)
2. Do not to treat ABU in the following condition. (Strong)
· Women without risk factors.
· Patients with regulated diabetes mellitus.
· Post-menopausal women.
· Elderly institutionalized patients.
· Patients with spinal cord injury, dysfunctional and/or reconstructed lower urinary tracts, and indwelling catheter
· Patients with renal transplant. Patients with arthroplasty surgeries.
· Patients with recurrent urinary tract infections.
3. Treat ABU prior urologic procedure breaching the mucosa and in pregnancy. (Strong)
4. Diagnosis of uncomplicated cystitis in women who have no risk factors for complicated urinary tract infections by a focused history of lower urinary tract symptoms. (Strong)
5. Uses of urine cultures in the following situations: (Strong)
a. suspected acute pyelonephritis.
b. symptoms that do not resolve or recur within four weeks after the completion of treatment.
c. women who present with atypical symptoms. Pregnant women.
6. Women with uncomplicated cystitis should be treated by antimicrobial therapy with or without symptomatic treatment. (Strong)
Recommendations for Recurrent UTIs
7. Diagnosis of each UTI episode clinically and is supported by symptoms of dysuria, frequency, urgency, hematuria, back pain, costovertebral tenderness and the absence of vaginal discharge or irritation. (Strong)
8. Complicated cases of UTI may also be ruled out on history and physical examination. Uroflowmetry and determining post void residual are suggested tests in postmenopausal women to exclude complicated cases of UTI. (Conditional)
9. Culture and sensitivity analysis when symptomatic and in 2 weeks from sensitivity-adjusted treatment to confirm UTI guide further treatment and exclude persistence. (Strong)
10. Further investigations e.g. (pelviabdominal US, PUT, CT abdomen and pelvis with or without contrast or cystoscopy) are not routinely recommended except in atypical cases. (Strong)
11. management and follow-up
Behavioral modifications are suggested e.g. reduced fluid intake, habitual and post-coital delayed urination, wiping from front to back after defecation, douching and wearing occlusive underwear. (good practice statement)
12. Non antimicrobial measures: Hormonal replacement: Use vaginal estrogen cream in post- menopausal women to prevent recurrent UTIs. (good practice statement)
13. Immunoactive prophylaxis: Use OM-89(Uro-vaxom) as an immunoprophylaxis in females with recurrent UTIs. (Strong)
14. Prophylaxis with cranberry: Do not use cranberry as a prophylaxis against recurrent UTIs. (Conditional)
Recommendations for uncomplicated pyelonephritis
15. Detailed history taking and urinalysis including the assessment of white and red blood cells and nitrite, for routine diagnosis. (Strong)
16. perform urine culture and antimicrobial susceptibility testing in patients with pyelonephritis. (Strong)
17. Imaging of the urinary tract (US) to exclude urgent urological disorders.Strong
18. treat patients who will be managed as outpatients by single-drug oral therapy with a fluoroquinolone or cephalosporines. (Strong)
19. Patients requiring hospitalization should be treated initially with an intravenous antimicrobial regimen e.g. a fluoroquinolone, an aminoglycoside (with or without ampicillin), or an extended- spectrum cephalosporin. (Strong)
20. Carbapenem is used only in patients with early culture results indicating the presence of multi-drug resistance organisms. (Strong)
Recommendations for complicated UTI
21. Urinalysis is recommended including the assessment of white and red blood cells and nitrite, for routine diagnosis. (Strong)
22. Performing urine culture and antimicrobial susceptibility testing is also recommended in patients with complicated UTI. (Strong)
23. Imaging of the urinary tract with US to exclude urgent urological disorders is recommended. Additional investigations, such as an unenhanced helical computed tomography (CT) is recommended if the patient remains febrile after 72 hours of treatment. (Strong)
24. For diagnosis of complicating factors in pregnant women, US, or magnetic resonance imaging (MRI) is recommended to avoid radiation risk to the foetus. (Strong)
25. It is recommended to properly manage the urological abnormality or the underlying complicating factor. (Strong)
26. Renal abscess: IT can rupture into the urinary tract or penetrate through the renal capsule to become a perinephric abscess. Use of IV combined antibiotics and careful observation of a small abscess less than 3 cm or even 5 cm in a clinically stable patient. Percutaneous drainage if greater than 5 cm in diameter or open surgical drainage if percutaneous drainage failed. (Strong)
27. Perinephric abscess: Broad spectrum antimicrobial agents are to be started immediately upon diagnosis of perinephric abscess. For larger collections or those not responsive to initial antibiotic therapy, intervention by percutaneous drainage techniques, by US or CT is recommended. Surgical drainage, or nephrectomy if the kidney is nonfunctioning or severely infected. (Strong)
28. Emphysematous pyelonephritis: Most patients are septic, and fluid resuscitation and broad-spectrum antimicrobial therapy is nedded . If the kidney is functioning, medical therapy can be considered. If a kidney is obstructed, catheter drainage is considered. If the affected kidney is nonfunctioning and not obstructed, nephrectomy should be performed because medical treatment alone is usually lethal. Nephrectomy is recommended for patients who do not improve after a few days of therapy. (Strong)
29. Xanthogranulomatous pyelonephritis (XGP): This is characterized by a chronic purulent, fatty inflammation of the renal parenchyma, the pelvis, and the hilar tissue. The primary obstacle to the correct treatment ofXGP is incorrect diagnosis. broad-spectrum antimicrobial therapy is recommended to stabilize the patient preoperatively, and, occasionally, long-term antimicrobial therapy will eradicate the infection and restore renal function. Because the renal abnormality may be diagnosed preoperatively as a renal tumor and/ or is diffuse, nephrectomy is usually performed. If localized XGP is diagnosed preoperatively or at exploration, it is amenable to partial nephrectomy. (Strong)
Recommendations for catheter-associated UTI
30. Routine urinary culture only in symptomatic patients, take the sample from the catheter using an aseptic technique, if the catheter has been removed obtain a midstream urine sample. (Strong)
31. Don’t use pyuria as indicator for catheter associated UTI, the longer the catheter in place, the most likely bacteria will be found. After one month nearly all patients have bacteriuria. (Strong)
32. Don’t use the presence or absence of odorous or cloudy urine alone to differentiate CA-UTI from CA- asymptomatic bacteriuria. (Strong)
33. Give oral antibiotics as a first line if the person can take oral medications, and the severity of their condition does not require intravenous antibiotics. (Strong)
34. Choice of intravenous antibiotics (if vomiting, unable to take oral antibiotics or severely unwell). Antibiotics may be combined if susceptibility of sepsis is a concern. (Strong)
35. Don’t treat CA-UTI asymptomatic bacteriuria in general except prior to traumatic urinary tract intervention and pregnant woman as of increased risk of pyelonephritis and preterm labor. (Strong)
Recommendations for urosepsis
36. Perform the quick SOFA score to identify patients with potential sepsis. (Strong)
37. Take a urine culture and two sets of blood cultures before starting antimicrobial treatment. (Strong)
38. We suggest Using biomarkers for diagnosis; however, urosepsis cannot be diagnosed from biomarkers alone. Procalcitonin monitoring may be useful in patients likely to develop sepsis and to differentiate from a severe inflammatory status not due to bacterial infection, Serum lactate is a marker of organ dysfunction and is associated with mortality in sepsis. (Conditional)
39. urosepsis treatment requires a combination of appropriate antimicrobial therapy, source control (obstruction of the urinary tract) and adequate life-support care. (Strong)
40. urologists collaborate with intensive care and infectious disease specialists for the best management of the patient is suggested. (good practice statement)
Recommendations for urethritis
41. Detailed history taking and urine analysis (first voided urine) and leukocyte esterase testing is diagnostic of urethritis. (Strong)
42. We suggest Gram or methylene-blue stain of urethral secretions, to diagnose gonococcal urethritis. (Conditional)
43. It is strongly recommended to instruct Patients to abstain from sexual intercourse for seven days after therapy. (Strong)
44. Gonococcal urethritis : Nucleic acid amplification tests are suggested (NAAT) especially in cases of urethritis with negative Gram stain test as it is more sensitive and specific in diagnosis of chlamydial and gonococcal infections.Urethral swab culture is suggested before initiation of treatment, in patients with a positive NAAT for gonorrhea to assess the antimicrobial resistance profile of the infective strain. (Conditional)
45. Urethral swab culture for N. gonorrhoeae and C. trachomatis is suggested in treatment failure or persistence of symptoms more than 4 weeks of treatment. (Conditional)
46. It is recommended to assess all sexual partners at risk. Empirical treatment is strongly recommended following diagnosis especially in severe cases.Combination treatment using two antimicrobials with different mechanisms of action is strongly recommended.It is strongly recommended to start with Ceftriaxone 1 g intramuscularly or intravenously with azithromycin 1 g single oral dose as first line treatment. (Strong)
47. Non-gonococcal urethritis: Oral doxycycline 100 mg twice daily for seven days as first-line treatment is strongly recommended. (Strong)
48. It is also suggested, single dose oral azithromycin 500 mg day one and 250 mg days two to four. Fluoroquinolones, such as ofloxacin or levofloxacin is considered as second-line treatment only in selected cases. (Conditional)
49. Oral metronidazole or tinidazole 2 g single dose as first-line treatment for urethritis caused by T. vaginalis. (Strong)
Recommendations for Acute Bacterial Prostatitis
50. Detailed history taking and mid-stream urine analysis, testing for nitrite and leukocytes is strongly recommended. (Strong)
51. Mid-stream urine culture and sensitivity for proper antimicrobial treatment is suggested and Transrectal ultrasound is considered if prostatic abscess is highly suggested. (Conditional)
52. Empirical high doses bactericidal antimicrobials, such as broad- spectrum penicillin, a third-generation cephalosporin or fluoroquinolones are recommended.It is recommended to continue oral treatment after improvement of general condition for two to four weeks.In case of prostatic abscess, both surgical drainage or conservative treatment according to abscess size and general condition is recommended. (Strong)
Recommendations for Chronic Bacterial Prostatitis CBP
53. Detailed history taking including (sexual activities, marital status and age of marriage) is recommended. (Strong)
54. The Meares and Stamey 2- or 4-glass test is strongly recommended in patients with CBP. (Strong)
55. Prostatic biopsy is not recommended to avoid sepsis. (Strong)
56. Transrectal ultrasound is suggested in selected cases to rule out chronic prostatic abscess and prostatic calcification. (good practice statement)
57. Semen culture is suggested as a part of evaluation of chronic bacterial prostatitis. (good practice statement)
58. PSA testing is not recommended for patients with CBP as it has no clinical or practical significance. (Strong)
59. Fluoroquinolone is strongly recommended as a first-line treatment for 4-6 weeks Doxycycline is recommended for Mycoplasma infection 100 mg BID for 10 days. (Strong)
60. Metronidazole is suggested in patients with Trichomonas vaginalis for 14 days. (conditional)
Recommendations for acute infective epididymitis
61. Obtain detailed history, symptoms analysis and also obtain first voided urine and a mid-stream urine for pathogen identification by culture and nucleic acid amplification test. (Strong)
62. Prescribe a single antibiotic or a combination of two antibiotics active against Chlamydia trachomatis and Enterobacteriaceae in young sexually active men. in older men without sexual risk factors only Enterobacteriaceae should be considered. (Strong)
63. Give single dose ceftriaxone 500 mg intramuscularly in addition to a course of an antibiotic active against Chlamydia trachomatis if gonorrheal infection is suspected. (Strong)
Recommendations for Fournier’s gangrene
64. Start treatment for Fournier’s gangrene with broad-spectrum antibiotics on presentation, with subsequent refinements according to culture and clinical response. (Strong)
65. Commence repeated surgical debridement for Fournier’s gangrene within 24 hours of presentation. (Strong)
66. We consider performing primary or secondary wound closure for scrotal defects ≤ 50%, with the use of flaps or skin grafts for defects involving > 50% of the scrotum or with extension outside the scrotum. (good practice statement)
Recommendations for antimicrobial prophylaxis in different urologic procedures
67. We consider it before urodynamic study and cystography. (Conditional)
68. We consider it before urethral catheterization and removal. (good practice statement)
69. We consider it before Shock-Wave Lithotripsy. (Conditional)
70. We consider it before Simple Cystoscopy. (Conditional)
71. We recommend it before TRUS guided prostatic biopsy, Transurethral Resection of the Prostate and bladder tumors, ureteroscopy, percutaneous renal Surgery and open or laparoscopic surgery. (Strong)
Recommendations for urinary Schistosomiasis
72. Urine analysis for diagnosis should be collected between 9 AM and 3 PM. to assess the egg count. (Strong)
73. Serologic tests: (Strong)
o It is strongly recommended when the diagnosis of urinary schistosomiasis is suspected, and urine is negative for eggs
o FAST-ELISA followed by Western blot analysis.
o Patients become antibody positive after 4-6 months from infection PCR for antigen detection:Detection of circulating anodic antigen in serum and urine are specific for active infection and quantitative measurements useful for determining infection severity
74. Praziquantel is the recommended oral treatment now,It is currently recommended by the WHO Dose: Two 20-mg/kg oral doses of PZQ are given on the same day, 6 to 8 hours apart (or alternatively, one 40-mg/kg dose) The drug has lower effect against schistosomula than adult worms, so another course should be repeated after several weeks to ensure eradication of infection. (Strong)
75. Cystoscopy is highly recommended if LUTS is persisting after adequate medical treatment or radiological findings of bladder lesions. (Strong)
- Recommendations
Table 4: Recommendations for asymptomatic bacteriuria (ABU)
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
Diagnosis of ABU is made by urine culture, either properly collected clean-catch specimen or a catheterized specimen is acceptable. |
High (3,4) |
Strong |
|
Do not to treat ABU in the following condition. Women without risk factors. Patients with regulated diabetes mellitus. Post-menopausal women. Elderly institutionalized patients. Patients with spinal cord injury, dysfunctional and/or reconstructed lower urinary tracts, and indwelling catheter Patients with renal transplant. Patients with arthroplasty surgeries. Patients with recurrent urinary tract infections. |
High (5,6) |
Strong |
|
Treat ABU prior urologic procedure breaching the mucosa and in pregnancy. |
High (5,6) |
Strong |
Table 5: Recommendations for acute uncomplicated cystitis (AUC)
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
High (7) |
Strong |
|
|
Uses of urine cultures in the following situations: suspected acute pyelonephritis. symptoms that do not resolve or recur within four weeks after the completion of treatment. women who present with atypical symptoms. Pregnant women. |
High (7,8) |
Strong |
|
Women with uncomplicated cystitis should be treated by antimicrobial therapy with or without symptomatic treatment |
High (9) |
Strong |
Table 6: Recommendations for Recurrent UTIs
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
irritation. |
High (8,9) |
Strong |
|
Complicated cases of UTI may also be ruled out on history and physical examination. Uroflowmetry and determining post void residual are suggested tests in postmenopausal women to exclude complicated cases of UTI |
Low (8,9) |
Conditional |
|
Culture and sensitivity analysis when symptomatic and in 2 weeks from sensitivity-adjusted treatment to confirm UTI guide further treatment and exclude persistence. |
High (8,9) |
Strong |
|
Further investigations e.g. (pelviabdominal US, PUT, CT abdomen and pelvis with or without contrast or cystoscopy) are not routinely recommended except in atypical cases |
High (8,9) |
Strong |
|
management and follow-up Behavioral modifications are suggested e.g. reduced fluid intake, habitual and post-coital delayed urination, wiping from front to back after defecation, douching and wearing occlusive underwear. |
Low (8,9) |
good practice statement |
|
Non antimicrobial measures: Hormonal replacement: Use vaginal estrogen cream in post- menopausal women to prevent recurrent UTIs |
Low (8,9) |
good practice statement |
|
Immunoactive prophylaxis: Use OM-89(Uro-vaxom) as an immunoprophylaxis in females with recurrent UTIs. |
High (8,9) |
Strong |
|
Prophylaxis with cranberry: Do not use cranberry as a prophylaxis against recurrent UTIs. |
Moderate (8,9) |
Conditional |
|
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
High (10-12) |
Strong |
|
|
perform urine culture and antimicrobial susceptibility testing in patients with pyelonephritis. |
High (10-12) |
Strong |
|
Imaging of the urinary tract (US) to exclude urgent urological disorders. |
High (10-12) |
Strong |
|
treat patients who will be managed as outpatients by single-drug oral therapy with a fluoroquinolone or cephalosporines. |
High (10-12) |
Strong |
|
Patients requiring hospitalization should be treated initially with an intravenous antimicrobial regimen e.g. a fluoroquinolone, an aminoglycoside (with or without ampicillin), or an extended- spectrum cephalosporin. |
High (10-12) |
Strong |
|
Carbapenem is used only in patients with early culture results indicating the presence of multi-drug resistance organisms. |
High (10-12) |
Strong |
Table 8: Recommendations for complicated UTI
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
Urinalysis is recommended including the assessment of white and red blood cells and nitrite, for routine diagnosis |
High (10) |
Strong |
|
Performing urine culture and antimicrobial susceptibility testing is also recommended in patients with complicated UTI |
High (10,11) |
Strong |
|
Imaging of the urinary tract with US to exclude urgent urological disorders is recommended. Additional investigations, such as an unenhanced helical computed tomography (CT) is recommended if the patient remains febrile after 72 hours of treatment. |
High (10-12) |
Strong |
|
For diagnosis of complicating factors in pregnant women, US, or magnetic resonance imaging (MRI) is recommended to avoid radiation risk to the foetus. |
High (10) |
Strong |
|
It is recommended to properly manage the urological abnormality or the underlying complicating factor. |
High (10) |
Strong |
Table 9: Recommendations for special types of renal infections
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
Renal abscess: IT can rupture into the urinary tract or penetrate through the renal capsule to become a perinephric abscess. Use of IV combined antibiotics and careful observation of a small abscess less than 3 cm or even 5 cm in a clinically stable patient. Percutaneous drainage if greater than 5 cm in diameter or open surgical drainage if percutaneous drainage failed. |
High (13,14) |
Strong |
|
Perinephric abscess: Broad spectrum antimicrobial agents are to be started immediately upon diagnosis of perinephric abscess. For larger collections or those not responsive to initial antibiotic therapy, intervention by percutaneous drainage techniques, by US or CT is recommended . Surgical drainage, or nephrectomy if the kidney is nonfunctioning or severely infected. |
High (15) |
Strong |
|
Emphysematous pyelonephritis: Most patients are septic, and fluid resuscitation and broad-spectrum antimicrobial therapy is nedded . If the kidney is functioning, medical therapy can be considered. If a kidney is obstructed, catheter drainage is considered. If the affected kidney is nonfunctioning and not obstructed, nephrectomy should be performed because medical treatment alone is usually lethal. Nephrectomy is recommended for patients who do not improve after a few days of therapy. |
High (16) |
Strong |
|
Xanthogranulomatous pyelonephritis (XGP): This is characterized by a chronic purulent, fatty inflammation of the renal parenchyma, the pelvis, and the hilar tissue. The primary obstacle to the correct treatment ofXGP is incorrect diagnosis. broad-spectrum antimicrobial therapy is recommended to stabilize the patient preoperatively, and, occasionally, long-term antimicrobial therapy will eradicate the infection and restore renal function. Because the renal abnormality may be diagnosed preoperatively as a renal tumor and/ or is diffuse, nephrectomy is usually performed. If localized XGP is diagnosed preoperatively or at exploration, it is amenable to partial nephrectomy |
High (17) |
Strong |
Table 10: Recommendations for catheter-associated UTI
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
High (18,19) |
Strong |
|
|
Don’t use pyuria as indicator for catheter associated UTI, the longer the catheter in place, the most likely bacteria will be found. After one month nearly all patients have bacteriuria. |
High (18,19) |
Strong |
|
Don’t use the presence or absence of odorous or cloudy urine alone to differentiate CA-UTI from CA- asymptomatic bacteriuria. |
High (18,19) |
Strong |
|
Give oral antibiotics as a first line if the person can take oral medications, and the severity of their condition does not require intravenous antibiotics. |
High (18,19) |
Strong |
|
Choice of intravenous antibiotics (if vomiting, unable to take oral antibiotics or severely unwell). Antibiotics may be combined if susceptibility of sepsis is a concern. |
High (18,19) |
Strong |
|
Don’t treat CA-UTI asymptomatic bacteriuria in general except prior to traumatic urinary tract intervention and pregnant woman as of increase risk of pyelonephritis and preterm labor. |
High (18,19) |
Strong |
Table 11: Recommendations for urosepsis
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
Perform the quick SOFA score to identify patients with potential sepsis. |
High (21) |
Strong |
|
Take a urine culture and two sets of blood cultures before starting antimicrobial treatment. |
High (20,21) |
Strong |
|
We suggest Using biomarkers for diagnosis; however, urosepsis cannot be diagnosed from biomarkers alone. Procalcitonin monitoring may be useful in patients likely to develop sepsis and to differentiate from a severe inflammatory status not due to bacterial infection, Serum lactate is a marker of organ dysfunction and is associated with mortality in sepsis. |
Moderate (20,21) |
Conditional |
|
High (22) |
Strong |
|
|
urologists collaborate with intensive care and infectious disease specialists for the best management of the patient is suggested. |
Low (22) |
good practice statement |
Table 12: Recommendations for urethritis
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
High (24) |
Strong |
|
|
We suggest Gram or methylene-blue stain of urethral secretions, to diagnose gonococcal urethritis. |
Moderate (24) |
Conditional |
|
It is strongly recommended to instruct Patients to abstain from sexual intercourse for seven days after therapy |
High (24) |
Strong |
|
Nucleic acid amplification tests are suggested (NAAT) especially in cases of urethritis with negative Gram stain test as it is more sensitive and specific in diagnosis of chlamydial and gonococcal infections. Urethral swab culture is suggested before initiation of treatment, in patients with a positive NAAT for gonorrhea to assess the antimicrobial resistance profile of the infective strain. |
Low (24) |
Conditional |
|
Urethral swab culture for N. gonorrhoeae and C. trachomatis is suggested in treatment failure or persistence of symptoms more than 4 weeks of treatment. |
Moderate (24) |
Conditional |
|
It is recommended to assess all sexual partners at risk. Empirical treatment is strongly recommended following diagnosis especially in severe cases. Combination treatment using two antimicrobials with different mechanisms of action is strongly recommended. It is strongly recommended to start with Ceftriaxone 1 g intramuscularly or intravenously with azithromycin 1 g single oral dose as first line treatment |
High (24) |
Strong |
|
Oral doxycycline 100 mg twice daily for seven days as first-line treatment is strongly recommended. |
High (24) |
Strong |
|
It is also suggested, single dose oral azithromycin 500 mg day one and 250 mg days two to four. Fluoroquinolones, such as ofloxacin or levofloxacin is considered as second-line treatment only in selected cases. |
Moderate (24) |
Conditional |
|
Oral metronidazole or tinidazole 2 g single dose as first-line treatment for urethritis caused by T. vaginalis. |
High (24) |
Strong |
Table 13: Recommendations for Acute Bacterial Prostatitis
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
High (25) |
Strong |
|
|
Mid-stream urine culture and sensitivity for proper antimicrobial treatment is suggested and Transrectal ultrasound is considered if prostatic abscess is highly suggested. |
Moderate (26) |
Conditional |
|
Empirical high doses bactericidal antimicrobials, such as broad- spectrum penicillin, a third-generation cephalosporin or fluoroquinolones are recommended. It is recommended to continue oral treatment after improvement of general condition for two to four weeks. In case of prostatic abscess, both surgical drainage or conservative treatment according to abscess size and general condition is recommended |
High (26,27) |
Strong |
Table 14 : Recommendations for Chronic Bacterial Prostatitis CBP
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
High |
Strong |
|
|
The Meares and Stamey 2- or 4-glass test is strongly recommended in patients with CBP. |
High (27,28) |
Strong |
|
Prostatic biopsy is not recommended to avoid sepsis. |
Moderate (27,28) |
Strong |
|
Transrectal ultrasound is suggested in selected cases to rule out chronic prostatic abscess and prostatic calcification. |
Low (27,28) |
good practice statement |
|
Semen culture is suggested as a part of evaluation of chronic bacterial prostatitis. |
Low (28) |
good practice statement |
|
PSA testing is not recommended for patients with CBP as it has no clinical or practical significance. |
Moderate (28) |
Strong |
|
Fluoroquinolone is strongly recommended as a first-line treatment for 4-6 weeks Doxycycline is recommended for Mycoplasma infection 100 mg BID for 10 days |
High (28) |
Strong |
|
Metronidazole is recommended in patients with Trichomonas vaginalis for 14 days |
High (28) |
conditional |
Table 15: Recommendations for acute infective epididymitis
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
High (29) |
Strong |
|
|
Prescribe a single antibiotic or a combination of two antibiotics active against Chlamydia trachomatis and Enterobacteriaceae in young sexually active men. in older men without sexual risk factors only Enterobacteriaceae should be considered. |
High (29) |
Strong |
|
Give single dose ceftriaxone 500 mg intramuscularly in addition to a course of an antibiotic active against Chlamydia trachomatis if gonorrheal infection is suspected. |
High (29) |
Strong |
Table 16: Recommendations for Fournier’s gangrene
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
High (30) |
Strong |
|
|
Commence repeated surgical debridement for Fournier’s gangrene within 24 hours of presentation. |
High (30) |
Strong |
|
We consider performing primary or secondary wound closure for scrotal defects ≤ 50%, with the use of flaps or skin grafts for defects involving > 50% of the scrotum or with extension outside the scrotum. |
Low (30) |
good practice statement |
Table 17: Recommendations for antimicrobial prophylaxis in different urologic procedures:
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
We consider it before urodynamic study and cystography. |
Low (35) |
Conditional |
|
We consider it before urethral catheterization and removal. |
Low(36) |
good practice statement |
|
We consider it before Shock-Wave Lithotripsy. |
Moderate (37) |
Conditional |
|
We consider it before Simple Cystoscopy. |
Moderate (10) |
Conditional |
|
We recommend it before TRUS guided prostatic biopsy, Transurethral Resection of the Prostate and Bladder tumors, ureteroscopy, percutaneous renal Surgery and open or laparoscopic surgery. |
High (39-44) |
Strong |
Table 18: Recommendations for urinary Schistosomiasis
|
Recommendations |
GRADE Level of certainty |
Strength Rating |
|
Urine analysis for diagnosis should be collected between 9 AM and 3 PM. to assess the egg count |
High (48) |
Strong |
|
Serologic tests: It is strongly recommended when the diagnosis of urinary schistosomiasis is suspected, and urine is negative for eggs FAST-ELISA followed by Western blot analysis. Patients become antibody positive after 4-6 months from infection PCR for antigen detection: Detection of circulating anodic antigen in serum and urine are specific for active infection and quantitative measurements useful for determining infection severity |
High (49-50) |
Strong |
|
Praziquantel is the recommended oral treatment now,It is currently recommended by the WHO Dose: Two 20-mg/kg oral doses of PZQ are given on the same day, 6 to 8 hours apart (or alternatively, one 40-mg/kg dose) The drug has lower effect against schistosomula than adult worms, so another course should be repeated after several weeks to ensure eradication of infection |
High (46-40) |
Strong |
|
Cystoscopy is highly recommended if LUTS is persisting after adequate medical treatment or radiological findings of bladder lesions |
High (49) |
Strong |
- Glossary
1. Antibiotic prophylaxis: It is treatment with antimicrobial agent(s) before or shortly after (for limited time) certain surgical procedure to prevent local surgical site
infection or systemic postprocedural infection
2. Complicated UTI : An infection associated with factors that increase the chance of acquiring bacteria and decrease the efficacy of therapy like obstruction and stones
3. Recurrent UTI: Recurrences of uncomplicated and/or complicated UTIs, with a frequency of at least three UTIs/year or two UTIs in the last six months
4. UTI: An inflammatory response of the urothelium to bacterial invasion that is usually associated with bacteriuria and pyuria.
5. Uncomplicated UTI: An infection in a healthy patient with a structurally and functionally normal urinary tract.
6. Urosepsis: Sever form of UTI with a considerable mortality rate
- List of Abbreviations
ABP Acute prostatitis
ABU Asymptomatic bacteriuria
AFP Acid fast bacilli
AUA American urological association
AUC Acute Uncomplicated Cystitis
BPS Best Practice statement
CAA Circulating anodic antigen
CA-uti Catheter associated urinary tract infection
CBP Chronic bacterial prostatitis
CDC The Centers for Disease Control and Prevention
CFU Colony forming unit
CLED Cysteine-lactose- electrolyte- deficient media
CMV Cytomegalovirus
CPPS Chronic pelvic pain syndrome
CT Computed tomography
cUTI Complicated urinary tract infections EAU European association of urology ESBL extended spectrum beta lactamase EQUC Expanded quantitative urine culture
FAST-ELISA Falcon assay screening test – enzyme linked immunosorbent assay
GCS Glasgow coma scale
HPF high power field
LUTS Lower urinary tract symptoms
MDR Multiple drug resistance
MRSA Methicillin Resistant Staph Aureus NAAT nucleic acid amplification tests NG Neisseria gonorrhoeae
NGS next-generation sequencing
NICE National institute for health and care excellence
NIDDK National Institute of Diabetes, Digestive and Kidney Diseases
NIH National Institutes of Health PCR Polymerase chain reaction PMNL polymorphonuclear leukocytes PZQ Praziquentel
SOFA Sequential [Sepsis-related] Organ Failure Assessment
SWL Shock wave lithotripsy
rUTI Recurrent urinary tract infections TMP-SMX Trimethoprim- sulfamethoxazole TRUS Trans rectal ultrasound
TURP Transurethral resection of prostate
UTI Urinary tract infection WGS Whole-genome sequencing WHO World health organization
XGP Xanthogranulomatous pyelonephritis
- Introduction
These guidelines provide essential summarized updated information for diagnosis, treatment and prevention of urinary tract Infections with emphasizing on judicious use of antimicrobials based on culture and sensitivity to reduce bacterial resistance which is a serious issue especially with malpractice and misuse of antibiotics in Egypt. Moreover, the recommendations included in these guidelines are not representing absolute mandates but provisional protocols respecting environmental and socioeconomic conditions of Egypt, considering our religious and traditional background.
- Purpose and scope
These guidelines are crucial for ensuring consistent and evidence-based care, particularly in a field where practices can vary significantly. By aligning local practices with global standards, they not only enhance patient outcomes but also empower healthcare providers with the knowledge to tackle the challenges presented by urological infections effectively. Furthermore, incorporating local expertise ensures that the guidelines are relevant and practical, ultimately fostering a more effective healthcare system in Egypt.
The Urologic Egyptian Guidelines on Urological Infections aim to support clinical practitioners and urologists in comprehensively understanding the incidence, standardized definitions, diagnosis, treatment, and follow-up of urological infections. This document integrates the latest international guidelines with insights from local experts, taking into account the unique healthcare and socioeconomic landscape of Egypt. It also includes perspectives from specialists in urological infections, serving as a thorough and authoritative reference for all clinicians as of the publication date.
- Target audience
The urinary tract infection infection guidelines are mainly intended for practicing urologists , health care providers, nurses, and hygiene control personnel to aid in patient care. They can also benefit health authorities and healthcare institutions by improving their understanding and support of UTI management. Moreover, these guidelines are useful for urologists in training, offering evidence-based insights and clinical recommendations for the treatment of urological infection.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated 2015 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author not on behalf of an organization in order to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in a table:
• Developing organisation/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least two members. the panel decided a cut-off point or rank the guidelines (any guideline scoring above 50% on the rigour dimension was retained).
Databases searched included Cochrane Libraries and European Association of Urology (EAU) guidelines, in the period from January 2022and September 2025. (24)
Adaptation of the Egyptian cultural aspects, the level of urologists’ capabilities and the availability of well equipped hospitals were considered in the methodology of diagnosis and different treatment modalities.
Evidence assessment.
According to WHO handbook for Guidelines we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations (18, 19). GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed information on GRADE is available on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
Table 1 Quality of evidence in GRADE
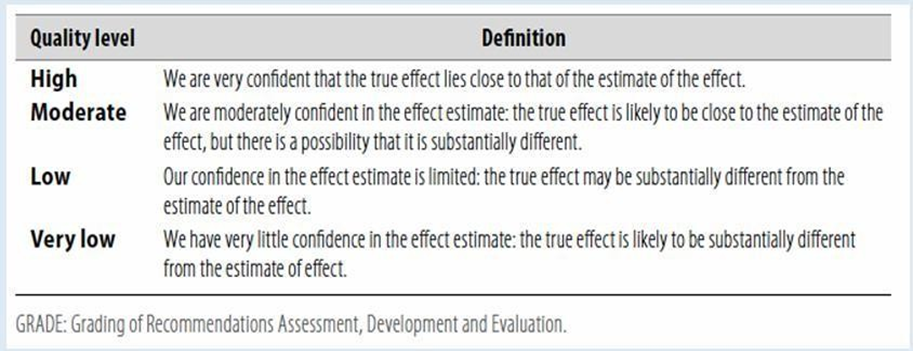
Table 2 Significance of the four levels of evidence
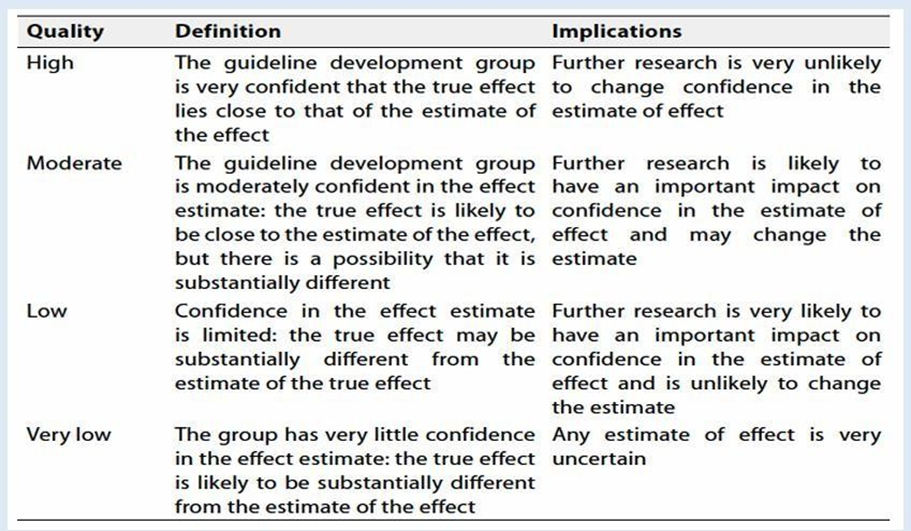
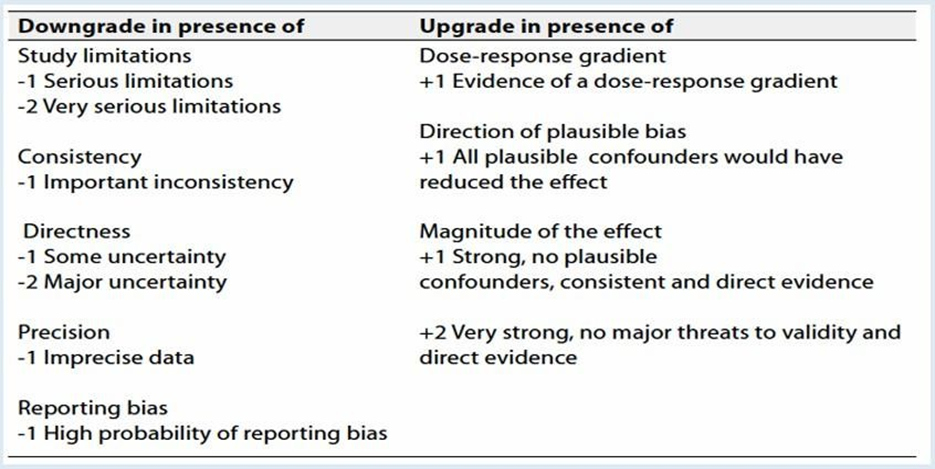
Table 3: Factors that determine How to upgrade or downgrade the quality of evidence
The strength of the recommendation.
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations.
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations.
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations.
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Clinical indicators of monitoring
1. Vital signs with accurate measurements of tperature and pulse.
2. Urine analysis and urine culture and sensitivity
3. Complete blood count
4. Kidney function tests
5. Ultrasound abdomen and pelvis
- Update of Guideline
This guideline will be updated whenever
there is new
evidence
- References
1. Ditkoff EL, Theofanides M, Aisen CM et al, : Assessment of practices in screening and treating women women with bacteriuria. Can J Urol. 2018 oct, 25(5): 9486-9496.
2. Nicolle LE, et al.: Infectious diseases society of American guidelines for the diagnosis for the diagnosis and treatment of asymptomatic bacteriuria in adults. Clin infect Dis, 2005. 40:643.
3. Donald and Amy: Asymtomaticbacteriuria, StatPearls Publishing, January 2020 (internet) .
4. Elzayat MA, Barnett-Vanes A, Dabour MFE, et.al. : Prevalence of undiagnosed asymptomatic bacteriuria and associated risk factors during pregnancy: a cross- sectional study at two tertiary centers in cairo, Egypt. BMJ 2017, 7
5. Hooton TM: The current management strategies for communityacquired urinary tract infection. Infect Dis Clin North Am., 2003, 17:303–22.
6. Foxman B, Barlow R, D’Arcy H et al.: Urinary tract infection: selfreported incidence and associated costs. Ann Epidemiol.,2000, 10:509–15.
7. Fihn SD: Acute uncomplicated urinary tract infection in women. N Engl J Med.,2003, 349:259–66.
8. Abdelkhalik A.M., Agha M.M., Zaki A.M.et al,: Clinical and Lab-assessed antibiotic resistance pattern of uropathogens among women with acute uncomplicated cystitis. The Egyptian journal of hospital medicine October 2018 vol. 73 (11), page 7860-68.
9. Wagenlehner, F.M., et al,: Uncomplicated urinary tract infections. DtschArzteblInt, 2011, 108:415.
10. SchnarrJ, and Smaill F.: Asymptomatic bacteriuria and symptomatic urinary tract infection in pregnancy. Eur J Clin Invest2008,38(suppl 2):50-7.
11. G. Bonkat, R. Bartoletti,F. Bruyèrehttps:European Guidelines-on-urological- infection-large-text.pdf,1-65,2020
12. Shawn Dason, Jeyapandy T. Dason, Anil Kapoor:Canadian Guidelines for the diagnosis and management of recurrent urinary tract infection in women. CUAJVolume5No4,316-322,Oct2011
13. EmanE ., et al. Microbiological Profile of Urinary Tract Infections with special Reference to Antibiotic Susceptibility Pattern of Escherichia coli Isolates. International Journal of Current Microbiology and Applied Sciences ,2319-7706 Volume 7 Number 02 (2018)
14. SulaimanA.,et al., Clinical and Laboratory Profile of Urinary Tract Infections Associated with Extended Spectrum βLactamase Producing Escherichia coli and Klebsiella pneumonia. Annals of Clinical & Laboratory Science, vol. 46, no. 4, 2016
15. Anthony J.etal., Infections of the Urinary Tract. Campbell's urology 11th ed. Philadelphia, chapter12:237-303,2018
16. National institute for health and care excellence Nice Guidelines, 2020
17. Fawkia E. Zahran, Ahmed Ibrahim, Sawsan A. Omer, Sameh A. Elkohafy, Gamil
K. Mohammed, Causative Organisms of Catheter Associated Urinary Tract Infection in Medical Wards and Intensive Care Units, International Journal of Internal Medicine, Vol. 8 No. 3, 2019, pp. 37-41.
18. Cek, M., et al. Healthcare-associated urinary tract infections in hospitalized urological patients--a global perspective: results from the GPIU studies 2003- 2010. World J Urol, 2014.32: 1587.
19. Tandogdu, Z., et al. Antimicrobial resistance in urosepsis: outcomes from the multinational, multicenter global prevalence of infections in urology (GPIU) study 2003-2013. World J Urol, 2016.34: 1193.
20. Singer, M., et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA,2016. 315: 801.
21. Bone, R.C., et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference
Committee.American College of Chest Physicians/Society ofCritical Care Medicine.Chest, 1992.101: 1644.
22. Levy, M.M., et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med, 2003.31: 1250.
23. Jordan SJ, Aaron KJ, Schwebke JR, Van Der Pol BJ, Hook EW 3rd. Defining the Urethritis Syndrome in Men Using Patient Reported Symptoms. Sex Transm Dis. 2018;45(7): e40‐e42.
24. Bonkat G., Bartoletti R., Bruyère F., Cai T. et al. The 2020 European guideline on the management of UrologicalInfections, 2020. 936-74.
25. Street, E.J., et al. The 2016 European guideline on the management of epididymo- orchitis. Int J STDAIDS, 2017. 28: 744.
26. Arnold, A., et al. Preoperative Mechanical Bowel Preparation for Abdominal, Laparoscopic, andVaginal Surgery: A Systematic Review. J Minim Invasive Gynecol, 2015. 22: 737.
27. Çek, M., et al. Acute and Chronic Epididymitis in EAU-EBU Update Series. EurUrolSuppl 2017. 16:124.
28. EAU guidelines for the management of acute infective epididymitis and fourniergangrene 2020 ; Members of the Urinary
Tract Infection (UTI) Working Group of the Guidelines Office of the European Association of Urology G. Bonkat (Co-chair),
R. Pickard (Co-chair), R. Bartoletti, T. Cai, F. Bruyère, S.E. Geerlings, B. Köves, F. Wagenlehner Guidelines Associates: A. Pilatz, B. Pradere, R. Veeratterapillay .
29. ghunam ,WM. Fournier gangrene in Mansura Egypt : A review of 74 cases . J postgrad Med 2008 : 54:106-9
30. Cooper KL, Badalato GM, Rutman MP. Infections of the Urinary Tract. 12 th ed. Campbell-Walsh-Wein Urology .In Partin
.AW, Peters CA, Kavoussi LR Dmochowski RR, Wein AJ editors: Elsevier Saunders: Philadelphia;2020
31. Lightner DJ, Wymer K, Sanchez J, Kavoussi L. Best Practice Statement on Urologic Procedures and Antimicrobial
Prophylaxis. J Urol. 2020 Feb;203(2):351-356
32. Wolf JS Jr, Bennett CJ, Dmochowski RR et al: Best practice policy statement on urologic surgery antimicrobial .prophylaxis. J Urol 2008; 179:1379-1390
33. Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg
.Infect (Larchmt). 2013;14(1):73–156
34. Bratzler DW, Houck PM, Surgical Infection Prevention Guidelines Writers
Workgroup, et al. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. ClinInfec Dis. 2004;38(12):1706–
.1715
35. Bonkat G, Bartoletti RR, Bruyère F, Cai T, Geerlings SE, Köves B, Schubert S, Wagenlehner F, EAU Guidelines on
.urological infections,2019. https://uroweb.org/guideline/urological-infection
36. Foon R, Toozs-Hobson P, Latthe P. Prophylactic antibiotics to reduce the risk of urinary tract infections after urodynamic
)studies. Cochrane Database Syst Rev. 2012;(10
37. Clarke SA, Samuel M, Boddy SA. Are prophylactic antibiotics necessary with clean intermittent catheterization? A .randomized controlled trial. J Pediatr Surg. 2005;40(3):568– 571
38. Honey RJ, Ordon M, Ghiculete D, et al. A prospective study examining the incidence of bacteriuria and urinary tract
.infection after shock wave lithotripsy with targeted antibiotic prophylaxis. J Urol. 2013;189(6):2112–2117
39. Lu Y, Tianyong F, Ping H, et al. Antibiotic prophylaxis for shock wave lithotripsy in patients with sterile urine before
.treatment may be unnecessary: a systematic review and metaanalysis. J Urol. 2012;188(2):441–448
40. Aron M, Rajeev TP and Gupta NP: Antimicrobial prophylaxis for transrectal needle biopsy of the prostate: a randomized controlled study. BJU Int 2000; 85: 682
.41.Dahm, P., et al. Evidence-based Urology. BMJ Books London, 2010: 50
42. Grabe M: Controversies in antimicrobial prophylaxis in urology. Int J Antimicrob Agents 2004; 23: S17
43. Omar M, Selim M, El Sherif E, Abozaid N, Farag E, Garabawey M, Zanaty F. Ciprofloxacin infusion versus third generaton cephalosporin as a surgical prophylaxis for percutaneous nephrolithotomy: a randomized study. Cent European J
Urol. 2019; 72: 57-61
44. Montgomery JS, Johnston WK III and Wolf JS Jr: Wound complications after hand- assisted laparoscopic surgery. J Urol
2005; 174: 2226
Antimicrobial prophylaxis in hip :45.Southwell-Keely JP, Russo RR, March L, Cumming R, Cameron I and Brnabic AJ fracture surgery: a metaanalysis. ClinOrthopRelat Res 2004; (419): 179
46. El-Zahar M I and Abd El-Karim SS. Schistosomiasis: chemoprophylaxis and treatments. Egyptian Pharmaceutical
Journal 2012,1 (11); 1-15
47. Yameny AA.The evolving schistosomiasis agenda 2017-2020 in Egypt : Moving from control toward final elimination.Journal of Bioscience and Applied Research, 20173(2),48-54
48. Jauréguiberry S, Paris L, Caumes E. Acute schistosomiasis, a diagnostic and therapeutic challenge. ClinMicrobiol Infect. 2010;16:225–231.
49. Koraitim M, Ikinger U. Genitourinary bilharziasis. In Ikinger U, Koraitim M, Seitz HK, editors. Schistosomiasis. Berlin:
Ullstein Mosby; 1994
50. EAU guidelines for the management of urogenital schistosomiasis. Bichler KH, Savatovsky I; Members of the Urinary
Tract Infection (UTI) Working Group of the Guidelines Office of the European Association of Urology (EAU):,Naber KG,
Bischop MC, Bjerklund-Johansen TE, Botto H, Cek M, Grabe M, Lobel B, Redorta JP, TenkeP.Eur Urol. 2006 Jun;49(6):998-
1003
51. Al-Sherbiny MM, Osman AM, Hancock K, et al. Application of immunodiagnostic assays: detection of antibodies and circulating antigens in human schistosomiasis and correlation with clinical findings. Am J Trop Med Hyg. 1999;60:960–966
52. Chang AH , Blackburn BG, Hsieh M. Tuberculosis and Parasitic Infections of the Genitourinary Tract. 12 th ed. CampbellWalsh-Wein Urology .In Partin AW, Peters CA, Kavoussi LR Dmochowski RR, Wein AJ editors: Elsevier Saunders: 2020;hiladelphia
53. Gouda I, Mokhtar N, Bilal D, El-Bolkainy T, El-Bolkainy NM. Bilharziasis and bladder cancer: a time trend analysis of 9843 patients. J Egypt NatlCancInst. 2007; 19: 158–62.
54. Freedman LS, Edwards BK, Ries LA, Young JL eds. Cancer Incidence in Four Member Countries (Cyprus, Egypt,Israel, and Jordan) of the Middle East Cancer Consortium (MECC) Comparedwith US SEER. Bethesda, MD: National Cancer Institute, 2006: NIH Pub no. 06–5873.
55. Vandepitte J. et al., (2003):Basic Lab Procedures in Clinical Bacteriology :, part 1 :30 -36
56. https://www.antibioticresearch.org.uk/find-support/urinary-tract-infections-utis/
57. Imam T.M. (2020):Fungal Urinary Tract Infections,Merck Manuals Professional
Edition -1 https://www.merckmanuals.com/professional
58. StopplerM.C. (2019):https://www.medicinenet.com/chlamydia_in_women_overview/article.htm
59. Bebell l. (2019):Antibiotic-resistant urinary tract infections are on the rise- Harvard Health Blog
60. Daryanto B, Janardhana A, Purnomo AF. The Effect of Covid-19 Severity on Lower Urinary Tract Symptoms Manifestations. Med Arch. 2022; 76(2): 127–130.
61. Bardi, T.; Pintado, V.; Gomez-Rojo, M.; Escudero-Sanchez, R.; Azzam Lopez, A.; Diez-Remesal, Y.; Martinez Castro, N.; Ruiz-Garbajosa, P.; Pestaña, D. Nosocomial infections associated to COVID-19 in the intensive care unit: Clinical characteristics and outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 495–502.
62. Karaba, S.M.; Jones, G.; Helsel, T.; Smith, L.L.; Avery, R.; Dzintars, K.; Salinas, A.B.; Keller, S.C.; Townsend, J.L.; Klein, E.; et al. Prevalence of Co-infection at the Time of Hospital Admission in COVID-19 Patients, A Multicenter Study. Open Forum Infect. Dis. 2020, 8, ofaa578.
63. Van Laethem, J.; Wuyts, S.C.M.; Pierreux, J.; Seyler, L.; Verschelden, G.; Depondt, T.; Meuwissen, A.; Lacor, P.; Piérard, D.; Allard, S.D. Presumed Urinary Tract Infection in Patients Admitted with COVID-19: Are We Treating Too Much? Antibiotics 2021, 10, 1493.
64. Cai T, Tascini C, Novelli A, et al. The Management of Urinary Tract Infections during the COVID-19 Pandemic: What Do We Need to Know? .Uro 2022, 2(1), 55-64.
65. Cho, I.; Blaser, M.J. The human microbiome: At the interface of health and disease. Nat. Rev. Genet. 2012, 13, 260–270.
66. . Ackerman AL, Chai TC. The bladder is not sterile: an update on the urinary microbiome. Curr Bladder Dysfunct Rep.2019;14(4):331–341
67. microbiome Thomas-White, K.; Brady, M.; Wolfe, A.J.; Mueller, E.R. The Bladder Is Not Sterile: History and Current Discoveries on the Urinary Microbiome. Curr. Bladder Dysfunct. Rep. 2016, 11, 18–24.
68. Falcou L, Davido B, Even A, et al. Original strategy for prevention of recurrent symptomatic urinary tract infections in patients with neurogenic bladder: bacterial interference, state of the art. ]. Prog Urol. 2018;28(6):307–314
69. Anna Kawalec and Danuta Zwoli ´nska: Emerging Role of Microbiome in the Prevention of Urinary Tract Infections in Children.international journal of molecular science 2022.
70. Miller JM, Binnicker MJ, Campbell S, et al. A guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2018 update by the infectious diseases society of america and the american society for microbiology. Clin Infect Dis. 2018;67(6):e1–e94