THE MANAGEMENT OF ACUTE MYOCARDIAL INFARCTION IN PATIENTS PRESENTING WITH ST-SEGMENT ELEVATION (STEMI)
| Site: | EHC | Egyptian Health Council |
| Course: | Cardiology Guidelines |
| Book: | THE MANAGEMENT OF ACUTE MYOCARDIAL INFARCTION IN PATIENTS PRESENTING WITH ST-SEGMENT ELEVATION (STEMI) |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:51 AM |
Description
"last update:
16 Sept 2025" Download Guideline
Table of contents
- - Executive summary
- - RECOMMENDATIONS
- - ACKNOWLEDGEMENTS
- - ACRONYMS AND ABBREVIATIONS
- - GLOSSARY
- - INTRODUCTION
- - SCOPE AND OBJECTIVES
- - TARGET AUDIENCE
- - Methods
- - CLINICAL AND QUALITY INDICATORS FOR MONITORING
- - Gap of evidence and future research
- - Implementation of the guidelines
- - Figures
- - ANNEXES
- - REFERENCES
- Executive summary
|
· We recommend that the diagnosis and management of STEMI should be based on the implementation of “regional networks” between hospitals (‘hub’ and ‘spoke’ model) linked by an efficient ambulance service. · We recommend that each regional network (cluster of hub and spokes) should share a written protocol of referral and consultation |
|
Strong recommendation |
|
· We recommend that a national call center for the ambulance should be established and well publicized to make it easily remembered and used by patients. |
|
Strong recommendation |
|
· We recommend that patients with chest pain and/or suspected STEMI should dial the EMS call center number without delays. We do not recommend self transfer (patients to use vehicles other than the EMS to reach hospitals in order to seek medical advice). |
|
Strong recommendation |
|
We recommend that all ambulance vehicles should be equipped with ECG machines and defibrillators. |
|
Strong recommendation |
|
We recommend that all ambulance personnel should be trained to recognize the symptoms of STEMI, administer aspirin, administer oxygen when appropriate, relieve pain and provide basic life support including using the defibrillator if indicated. |
|
Strong recommendation |
|
We recommend that all ambulance personnel should be trained to record an ECG and either interpret or transmit it, so that it can be reviewed by hospital-based cardiologist to establish or reject a STEMI diagnosis. |
|
Strong recommendation |
|
We recommend that once ECG diagnosis is confirmed, primary PCI team in the Cath lab of the Hub should be alerted of an imminent patient arrival |
|
Strong recommendation |
|
We recommend that all patients with confirmed or suspected STEMI should receive 300 mg of chewable aspirin as soon as possible if patients were not receiving ASA before or if no contraindication. |
|
Strong recommendation |
|
We recommend that the ambulance should transfer the clinically stable patient from the field to the nearest PCI capable hospital, bypassing non- PCI capable hospitals. |
|
Strong recommendation |
|
We recommend that if the patient during transfer becomes unstable or deteriorate clinically, he should be redirected to the nearest hospital with ER |
|
Strong recommendation |
|
We recommend that an ambulance transferring patients from the field to the hospital can be equipped with a trained paramedic while an ambulance transferring patient in-between hospitals should include an accompanying doctor on board. |
|
Strong recommendation |
|
We recommend that all EMS should have a written protocol stating the updated management protocols and should establish a formal relationship with a PCI center to enable prompt patient transfer |
|
Strong recommendation |
|
We recommend that the time of EMS response, arrival to the patient, arrival to the designated hospital and the time of first ECG should be recorded and regularly audited aiming at improving performance quality metrics |
|
Strong recommendation |
|
We recommend that reperfusion of the infarct related artery should be offered to all patients with STEMI presenting within the first 12 hours following chest pain onset. |
|
Strong recommendation |
|
We recommend that reperfusion of the infarct related artery should be offered to all patients with STEMI presenting within the 12-48 hours following chest pain onset. |
|
Strong recommendation |
|
We recommend that primary PCI should be used as a default reperfusion strategy for suspected STEMI patients provided that time delay would not exceed 120 minutes. |
|
Strong recommendation |
|
We recommend that patients should bypass non-PCI-capable centers and instead be transferred to the nearest Primary PCI Centre with the goal of achieving a maximum FMC-to device time of ≤ 120 minutes (ideal FMC-to-device time ≤ 90 minutes in urban settings). |
|
Strong recommendation |
|
We recommend that in areas where the transfer of patients to the nearest hub will exceed 120 minutes, patients should be offered fibrinolytic therapy with immediate transfer afterwards to the hub for cardiac catheterization within 2-24 hours post fibrinolysis. This pathway is the Pharmacoinvasive pathway. |
|
Strong recommendation |
|
We recommend that public awareness campaigns should be organized to reduce “patient delay” and should include the following messages: · Importance to know common symptoms of STEMI and to recognize it as early as possible · Importance to react rapidly by calling the emergency services (123: ambulance service or 16474: critical cases services). |
|
Strong recommendation |
|
We recommend the following measures and policies to help minimize “system delays”: · It is mandatory to do a pre-hospital ECG and diagnose a STEMI in less than 10 minutes from the patient presentation. · EMS personell should send the pre-hospital ECG to a hospital-based consultant to confirm or reject the diagnosis of STEMI. · Once the diagnosis of STEMI is confirmed in the pre-hospital setting, immediate activation of the catheterization laboratory should be initiated, the patient should be directed to the nearest hub (Hospital with 24/7 primary PCI service). · In the hub, the system should allow the EMS personell to bypass the emergency department and bring the patient straight to the catheterization laboratory. · For patients presenting in a non-capable PCI center, door-in to door-out time, defined as the duration between arrival of the patient at the hospital to discharge of the patient in an ambulance en route to the PCI center, should not exceed 30 minutes. · Patients who will receive fibrinolytic therapy should receive it in less than 10 minutes from diagnosis and should be transferred to a primary PCI capable center routinely within 2-24 hours after thrombolytic therapy · A written protocol in PCI non-capable hospitals should determine the reperfusion strategy of this hospital whether direct transfer to PCI capable hospital or transfer after fibrinolytic therapy. The written protocol should establish a formal relationship with a PCI center to enable prompt patient transfer. · All hospitals and EMS taking care of patients presenting with STEMI should adopt the time targets summarized in Table #. We recommend that management delays should be recorded and audited regularly and policies should be established to regularly improve them. |
|
Strong recommendation |
|
We recommend that appropriate and urgent management of STEMI starts from the moment of first medical contact (FMC) |
|
Strong recommendation |
|
We recommend that correct diagnosis of STEMI is usually based on symptoms consistent with myocardial ischaemia (i.e., persistent chest pain) and 12-lead electrocardiogram (ECG). |
|
Strong recommendation |
|
We recommend considering the typical characters of chest pain as retrosternal compression or heaviness with radiation to the left arm, neck, or lower jaw. |
|
Strong recommendation |
|
We recommend that atypical and less-typical symptoms such as shortness of breath, nausea/vomiting, fatigue, palpitations, or syncope should be considered the presenting symptoms in some patients (e.g. in elderly and females). |
|
Strong recommendation |
|
We do not recommend using reduction in chest pain after nitroglycerin (glyceryl trinitrate) administration as a diagnostic maneuver |
|
Moderate recommendation |
|
We recommend that patients with ongoing ischemic discomfort should receive sublingual nitroglycerin (0.4 mg) or isosorbide dinitrates (5 mg) every 5 minutes for a total of 3 doses, after which an assessment should be made about the need for intravenous nitroglycerin. |
|
Strong recommendation |
|
We recommend that intravenous nitroglycerin is used for relief of ongoing ischemic discomfort, control of hypertension or management of pulmonary congestion. |
|
Strong recommendation |
|
We recommend that morphine sulfate (2 to 4 mg IV with increments of 2 to 8 mg repeated at 5-to-15-minute intervals) may be considered for severe pain refractory to nitrates and other anti-ischemic therapies with the goal of relieving pain and reducing anxiety. |
|
Moderate recommendation |
|
We Recommend that oral beta-blockers should be administered promptly to those patients without a contraindication irrespective of concomitant fibrinolytic therapy or performance of primary PCI. |
|
Strong recommendation |
|
We recommend IV beta-blockers promptly to STEMI patients without contraindications, especially if a tachy- arrhythmia or hypertension is present. |
|
Moderate recommendation |
|
We recommend against routine use of supplemental oxygen in patients with STEMI who have an arterial oxygen saturation ≥90 % with no signs of respiratory distress. |
|
Moderate recommendation |
|
We recommend that patients with oxygen saturation <90% or respiratory distress should be treated with oxygen as needed. |
|
Strong recommendation |
|
We recommend that non-steroidal anti-inflammatory drugs (NSAIDs), except aspirin, should be avoided to relieve chest pain, or any other indication, in the acute phases of STEMI management. |
|
Moderate recommendation |
|
We recommend 12-lead ECG recording and prompt interpretation in less than 10 min at the site of first medical contact (FMC). |
|
Strong recommendation |
|
We recommend an ECG monitoring with defibrillator capacity as soon as possible in all patients with suspected or confirmed STEMI |
|
Strong recommendation |
|
We recommend that, in the proper clinical context, ST-segment elevation (measured at the J-point) is considered suggestive of acute coronary artery occlusion when it is present in at least two contiguous leads with ST-segment elevation ≥2.5 mm in men < 40 years, ≥2 mm in men > 40 years, or ≥1.5 mm in women in leads V2–V3 and/or ≥1 mm in the other leads [in the absence of left ventricular hypertrophy or LBBB]. |
|
Strong recommendation |
|
We recommend in patients with inferior STEMI, to record right precordial leads (V3R and V4R) seeking ST segment elevation, to identify concomitant right ventricular (RV) infarction |
|
Moderate recommendation |
|
We recommend that the presence of a Q-wave on the ECG should not necessarily change the reperfusion strategy decision. |
|
Strong recommendation |
|
We recommend that patients with a clinical suspicion of ongoing myocardial ischaemia and LBBB should be managed in a way similar to STEMI patients, regardless of whether the LBBB is previously known. |
|
Strong recommendation |
|
We recommend routine blood sampling for serum markers as soon as possible in the acute phase but this should not delay reperfusion treatment. Biomarkers can be of importance in clinical diagnosis and prognosis. We recommend hsTn if available. |
|
Strong recommendation |
|
We recommend quick history taking, assessing vital signs, identifying significant co-morbidities, securing an IV line and doing an ECG within 10 minutes from ER arrival, getting the cath lab ready in <30 min, achieving door to balloon time of <60 min and overall FMC-to-device time of ≤ 90 minutes |
|
Strong Recommendation |
|
We recommend giving the patient as soon as possible, if not previously given and if not contraindicated, 4 chewable aspirin tablets (300 mg). |
|
Strong Recommendation |
|
We recommend giving the patient, once diagnosed, Ticagrelor 180 mg (oral or via NGT) (or Clopidogrel 600 mg if Ticagrelor is not available or contraindicated). Ticagrelor contra-indications are history of intra-cerebral hemorrhage or moderate-severe hepatic failure. |
|
Strong Recommendation |
|
We do not recommend routine glycoprotein IIb/IIIa inhibitors or fibrinolytics before arrival at the catheter laboratory to people with acute STEMI for whom primary PCI is planned. |
|
Moderate Recommendation |
|
We recommend giving patients with persistent cardiac chest pain or discomfort sublingual Nitrates if SBP >140 mmHg and if RV infarct can be excluded. |
|
Conditional recommendation |
|
We recommend, If SBP <90 mmHg and patient is not in acute pulmonary edema, to administer a 300 mL fluid challenge. |
|
Conditional recommendation |
|
We recommend, if chest pain is still present, to administer morphine in increments of 2-4 mg. |
|
Conditional recommendation |
|
We recommend radial access over femoral access if performed by an experienced radial operator. |
|
Conditional Recommendation |
|
We recommend use of UFH for procedural anticoagulation |
|
Strong Recommendation |
|
We recommend that Enoxaparin can be used as an alternative option to UFH |
|
Conditional Recommendation |
|
We recommend against using fondaparinux during primary PCI |
|
Strong Recommendation |
|
We recommend Primary PCI of the IRA using DES |
|
Strong Recommendation |
|
We recommend CABG should be considered in patients with ongoing ischemia and large areas of jeopardized myocardium if PCI of the IRA cannot be performed |
|
Conditional recommendation |
|
We recommend PCI of non-IRA lesions before hospital discharge, in hemodynamically stable patients with STEMI and multivessel disease. |
|
Conditional Recommendation |
|
We recommend PCI to culprit vessel only rather than complete revascularization during the index procedure in patients with STEMI and cardiogenic shock. |
|
Conditional Recommendation |
|
We recommend Re-do coronary angiography (with possible PCI) in patients with symptoms or signs of recurrent or remaining ischemia after primary PCI. |
|
Strong Recommendation |
|
We recommend against the routine use of I.V. GPI for primary PCI except as bailout for patients with heavy thrombus burden. |
|
Conditional Recommendation |
|
We recommend Against the routine use of IC GPI for primary PCI |
|
Strong Recommendation |
|
We recommend against the routine use of IC fibrinolysis |
|
Weak Recommendation |
|
We recommend against the routine use of IC adenosine to prevent no-reflow. |
|
Weak Recommendation |
|
We recommend against the routine use of thrombus aspiration except as bailout for patients with heavy thrombus burden. |
|
Strong Recommendation |
|
We recommend against the routine use of deferred stenting. |
|
Strong recommendation |
|
We recommend fibrinolytic therapy within 12 h of symptom onset if primary PCI cannot be performed within 120 min from STEMI diagnosis and there are no contraindications. |
|
Strong recommendation |
|
We recommend Primary PCI rather than fibrinolysis in patients with heart failure/shock. |
|
Strong recommendation |
|
We recommend, when fibrinolysis is the reperfusion strategy, to initiate this treatment as soon as possible after STEMI diagnosis. Door to needle time should not exceed 10 minutes. |
|
Strong recommendation |
|
We recommend to use single-bolus weight adjusted tenecteplase tissue plasminogen activator (TNK-tPA) if available as it is preferred over streptokinase. |
|
Conditional recommendation |
|
We recommend that late presenters (particularly >3 h) should be considered for transfer to primary PCI because the efficacy and clinical benefit of fibrinolysis decrease as the time from symptom onset increases. |
|
Conditional recommendation |
|
We recommend that Clopidogrel (rather than ticagrelor) plus aspirin is preferred when fibrinolysis is the used strategy for reperfusion. |
|
Strong recommendation |
|
We recommend that parenteral anticoagulation in patients treated with lytics is used until revascularization or for the duration of hospital stay up to 8 days. |
|
Strong recommendation |
|
We recommend that the anticoagulant to be is Enoxaparin I.V. loading bolus followed by S.C. maintenance (preferred over UFH). |
|
Strong recommendation |
|
We recommend that the anticoagulant can also be UFH given as a weight-adjusted I.V. bolus followed by infusion. |
|
Strong recommendation |
|
We recommend that the anticoagulant can also be Fondaparinux I.V. bolus followed by S.C. dose 24 h later in patients treated with streptokinase. |
|
Conditional recommendation |
|
We recommend transfer to a PCI-capable center angiography and PCI of the IRA following successful fibrinolysis in all patients within 2-24 hours after fibrinolysis. |
|
Strong recommendation |
|
We recommend rescue PCI immediately when fibrinolysis has failed (<50% ST-segment resolution at 60–90 min) or at any time in the presence of hemodynamic or electrical instability, or worsening ischaemia. |
|
Strong recommendation |
|
We recommend emergency angiography and PCI in the case of recurrent ischaemia or evidence of reocclusion after initial successful fibrinolysis. |
|
Strong recommendation |
|
We recommend that same day repatriation can be considered provided that the patient 1. Has undergone a successful uncomplicated primary PCI 2. Is without ongoing myocardial ischemia 3. Is without arrhythmias 4. Is hemodynamically stable not requiring vasoactive or mechanical support 5. Does not need early revascularization to infarct-related or other arteries 6. Is transferred while monitored via ambulance and accompanied by a physician |
|
Conditional recommendation |
|
We recommend that all STEMI patients with successful reperfusion therapy and an uncomplicated clinical course to be kept monitored by ECG in the CCU/ICU for a minimum of 24 hours, after which they can be transferred to a monitored intermediate care unit for an additional 24-48 hours. |
|
Strong recommendation |
|
We recommend that early hospital discharge within 24-72 hours can be considered provided that the patient 1. Has undergone a successful uncomplicated primary PCI 2. Without ongoing ischemia, arrhythmias or hemodynamic instability 3. Does not need early revascularization to the infarct-related or other arteries 4. Is scheduled for early rehabilitation and adequate follow-up |
|
Conditional recommendation |
|
We recommend short and long-term risk assessment as soon as the patient is admitted to CCU/ICU, through 1. Clinical evaluation for signs of ongoing ischemia or hemodynamic instability 2. Clinical evaluation, cardiac enzymes and echocardiography for assessment of extent of myocardial damage and state of LV and RV functions, exclude mechanical complications and LV thrombus 3. Clinical and laboratory assessment of dyslipidemia, dysglycemia, hypertension, renal dysfunction or peripheral vascular disease 4. Clinical, invasive coronary angiography or noninvasive imaging (stress echo, CMR, SPECT, or PET) to assess residual ischemia and myocardial viability in non-reperfused patients. |
|
Strong recommendation |
|
We recommend the continuation of chronic anticoagulation regimen during admission. |
|
Strong recommendation |
|
We recommend Primary PCI rather than fibrinolytic therapy regardless of the anticipated time delay. |
|
Strong recommendation |
|
We recommend Radial over femoral approach during PPCI. |
|
Strong recommendation |
|
We recommend the use of additional parenteral anticoagulation while in the Cath lab during primary PCI, regardless of the timing of the last dose of oral anticoagulants. |
|
Strong recommendation |
|
We recommend giving the usual 300 mg loading dose of oral aspirin. |
|
Strong recommendation |
|
We recommend using clopidogrel (600 mg loading dose) rather than ticagrelor or prasugrel. |
|
Strong recommendation |
|
We recommend prescribing triple antithrombotic therapy for the first week after primary PCI and up to one month in high thrombotic risk and low bleeding risk, after which we recommend discontinuing aspirin and continue on oral anticoagulants and clopidogrel for one year. Then, we recommend keeping the patient on oral anticoagulants only thereafter. |
|
Strong recommendation |
|
We recommend the assessment of bleeding risk in all patients. |
|
Strong recommendation |
|
We recommend the use of Novel oral anticoagulants over warfarin for patients with non-valvular atrial fibrillation. |
|
Strong recommendation |
|
We recommend that in case of warfarin, the dose intensity should be carefully monitored with a target international normalized ratio (INR) in the lower part of the recommended target range. When non-vitamin K antagonist oral anticoagulants are used, the lowest effective tested dose for stroke prevention should be applied. |
|
Strong recommendation |
|
We recommend against the use of GP IIB/IIIA inhibitors. |
|
Strong recommendation |
|
We recommend adding proton pump inhibitor for gastric protection. |
|
Strong recommendation |
|
We recommend to maintain a high index of suspicion for diagnosing STEMI in elderly patients who present with atypical complaints. |
|
Strong recommendation |
|
We recommend Primary PCI or thrombolytic therapy (according to the standard indications) with no upper age limit. |
|
Strong recommendation |
|
We recommend radial access over femoral access to reduce bleeding risk. |
|
Strong recommendation |
|
We recommend against giving a loading dose of clopidogrel when thrombolytic therapy is indicated. |
|
Strong recommendation |
|
We recommend adding proton pump inhibitor for gastric protection. |
|
Strong recommendation |
|
We recommend to maintain a high index of suspicion for diagnosing STEMI in patients with diabetes who present with atypical complaints. |
|
Strong recommendation |
|
We recommend that selection of reperfusion therapy (primary PCI or fibrinolytics) is like patients without diabetes. |
|
Strong recommendation |
|
We recommend the use of the more potent oral P2Y12 receptor inhibitors (prasugrel or ticagrelor) over clopidogrel. |
|
Strong recommendation |
|
We recommend the evaluation of glycemic status in all STEMI patients with and without a known history of diabetes or hyperglycemia, and to monitor it frequently in diabetic patients and patients with hyperglycemia. |
|
Strong recommendation |
|
We recommend management of hyperglycemia and maintain a blood glucose concentration ≤200 mg/dl but absolutely avoid hypoglycemia (defined as glucose levels ≤70 mg/dl). |
|
Moderate recommendation |
|
We recommend the assessment of the renal insufficiency risk and to measure eGFR in patients on metformin and/or sodium-glucose co-transporter-2 (SGLT2) inhibitors. |
|
Strong recommendation |
|
We recommend to maintain a high index of suspicion for diagnosing STEMI in patients with renal dysfunction who present with atypical complaints. |
|
Strong recommendation |
|
We recommend measuring eGFR as soon as possible in patients with suspected renal dysfunction as elderly, diabetics, and heart failure. |
|
Strong recommendation |
|
We recommend adjusting dose of antithrombotic drugs according to renal function. |
|
Strong recommendation |
|
We recommend adequate hydration during and after primary PCI and limiting the dose of contrast agents, preferentially low-osmolality contrast agents to reduce the risk of contrast-induced nephropathy. |
|
Strong recommendation |
|
We recommend adding proton pump inhibitor for gastric protection |
|
Strong recommendation |
|
We recommend immediate assessment of non-reperfused patients for evidence of electrical or hemodynamic instability or evidence of ongoing ischemia. This evidence would make them candidates for primary PCI even beyond the time window of reperfusion. |
|
Strong recommendation |
|
We recommend doing echocardiography as soon as possible for these patients to detect complications or any indication for invasive intervention. |
|
Strong recommendation |
|
We recommend noninvasive tests to detect evidence of residual ischemia or myocardial viability that indicate further invasive assessment with or without revascularization. |
|
Strong recommendation |
|
We recommend medical therapy including DAPT and secondary prevention therapies for stable patients who were not reperfused. |
|
Strong recommendation |
|
We recommend that in patients in whom PCI is finally performed, ticagrelor is preferred, while in patients who do not undergo PCI, either ticagrelor or clopidogrel can be used. |
|
Strong recommendation |
|
We recommend anticoagulation, preferably with fondaparinux, until coronary revascularization is done or hospital discharge. |
|
Strong recommendation |
|
We recommend against routine reperfusion of the infarct related artery in stable patients beyond the first 48 hour of symptom onset. |
|
Strong recommendation |
|
We recommend the initiation of ACE inhibitor (or if not tolerated, ARB) therapy as soon as possible in all hemodynamically stable patients with evidence of LVEF ≤ 40% and/or heart failure to reduce the risk of hospitalization and death. |
|
Strong recommendation |
|
We recommend the initiation of Beta-blocker therapy in patients with LVEF ≤ 40% and/or heart failure after stabilization, to reduce the risk of death, recurrent MI, and hospitalization for heart failure |
|
Strong recommendation |
|
We recommend the initiation of an MRA therapy in patients with heart failure and LVEF ≤ 40% with no severe renal failure or hyperkalemia to reduce the risk of cardiovascular hospitalization and death. |
|
Strong recommendation |
|
We recommend the use of Loop diuretics in patients with acute heart failure with symptoms/signs of fluid overload to improve symptoms. |
|
Strong recommendation |
|
We recommend the use of IV nitrates in patients with symptomatic heart failure with SBP >90 mmHg to improve symptoms and reduce congestion. |
|
Strong recommendation |
|
We suggest the use of Intravenous nitrates or sodium nitroprusside in patients with heart failure and elevated SBP to control blood pressure and improve symptoms. |
|
Moderate recommendation |
|
We recommend Oxygen therapy in patients with pulmonary oedema with SaO2 < 90% to maintain a saturation > 95%. |
|
Strong recommendation |
|
We suggest non-invasive positive pressure ventilation (continuous positive airway pressure, biphasic positive airway pressure) in patients with respiratory distress (respiratory rate >25 breaths/min, SaO2 <90%) without hypotension. |
|
Moderate recommendation |
|
We recommend patient intubation in patients with respiratory failure or exhaustion, leading to hypoxemia, hypercapnia, or acidosis, and if non-invasive ventilation is not tolerated. |
|
Strong recommendation |
|
We recommend the use of opiates to relieve dyspnea and anxiety in patients with pulmonary oedema and severe dyspnea. Respiration should be monitored. |
|
Weak recommendation |
|
We recommend the use of IV inotropic agents and/or vasopressors in patients with severe heart failure with hypotension (systolic BP < 90 mmHg) refractory to standard medical treatment. |
|
Weak recommendation |
|
We recommend that SGLT2 inhibitors may be considered in the setting of acute STEMI especially in diabetic patients and if complicated with heart failure after stabilization. |
|
Weak recommendation |
|
We recommend that ARNI, in place of ACE inhibitors or ARBS, may be considered in the setting of acute STEMI especially if complicated with heart failure after stabilization. |
|
Weak recommendation |
|
We recommend immediate primary PCI to infarct related artery if coronary anatomy is suitable. |
|
Strong recommendation |
|
We recommend primary PCI to infarct related artery only as the default strategy. |
|
Strong recommendation |
|
We recommend fibrinolysis if a primary PCI strategy is not available within 120 min from STEMI diagnosis and mechanical complications have been ruled out. |
|
Moderate recommendation |
|
We recommend emergency CABG if coronary anatomy is not suitable for PCI, or if PCI has failed , or in case of mechanical complication. |
|
Strong recommendation |
|
We recommend continuous invasive blood pressure monitoring with an arterial line. |
|
Strong recommendation |
|
We recommend hemodynamic assessment with pulmonary artery catheter for confirming diagnosis or guiding therapy. |
|
Weak recommendation |
|
We recommend immediate echocardiography to assess ventricular and valvular functions, loading conditions, and to detect mechanical complications. |
|
Strong recommendation |
|
We recommend that mechanical complications to be treated as early as possible after discussion by the Heart Team. |
|
Strong recommendation |
|
We recommend Oxygen/mechanical respiratory support according to blood gases. |
|
Strong recommendation |
|
We recommend the use of intra-aortic balloon pumping in patients with mechanical complications. |
|
Moderate recommendation |
|
We recommend against the routine use of intra-aortic balloon pumping. |
|
Strong recommendation |
|
We recommend Ultrafiltration in patients with refractory congestion who failed to respond to diuretics. |
|
Weak recommendation |
|
We recommend the use of Inotropic/vasopressor agents for hemodynamic stabilization. |
|
Weak recommendation |
|
We recommend the short-term use of mechanical circulatory support e.g. ECLS or ECMO in patients in refractory shock. |
|
Weak recommendation |
|
We recommend the use of intravenous beta-blockers for rate control if there are no clinical signs of acute heart failure or hypotension. |
|
Strong recommendation |
|
We recommend the use of intravenous amiodarone for rate control, in case of concomitant acute heart failure but no hypotension. |
|
Strong recommendation |
|
We recommend that the use of intravenous digitalis for rate control, might be considered, in case of concomitant acute heart failure and hypotension. |
|
Conditional recommendation |
|
We recommend immediate electrical cardioversion when adequate rate control cannot be achieved promptly with pharmacological agents and ongoing ischemia, severe hemodynamic compromise, or heart failure. |
|
Strong recommendation |
|
We recommend the use of intravenous amiodarone to promote electrical cardioversion and/or decrease risk for early recurrence of AF after electrical cardioversion. |
|
Strong recommendation |
|
We recommend long term anticoagulation depending on CHA₂DS₂-VASc score and taking concomitant antithrombotic therapy into account |
|
Conditional recommendation |
|
We recommend against the prophylactic treatment with antiarrhythmic drugs to prevent AF in STEMI patients. |
|
Strong recommendation |
|
We recommend the use of intravenous beta-blocker treatment in STEMI patients with polymorphic VT and/or VF unless contraindicated. |
|
Strong recommendation |
|
We recommend prompt and complete revascularization to treat myocardial ischemia that may be present in patients with recurrent VT and/or VF. |
|
Strong recommendation |
|
We recommend the use of intravenous amiodarone in treatment of recurrent polymorphic VT. |
|
Strong recommendation |
|
We suggest the use of intravenous amiodarone for recurrent VT with hemodynamic intolerance despite repetitive electrical cardioversion. |
|
Conditional recommendation |
|
We recommend correction of electrolyte imbalances (especially hypokalemia and hypomagnesemia) in patients with VT and/or VF. |
|
Strong recommendation |
|
We suggest transvenous catheter pace termination and/or overdrive pacing if VT cannot be controlled by repetitive electrical cardioversion. |
|
Conditional recommendation |
|
We suggest radiofrequency catheter ablation followed by ICD implantation in patients with recurrent VT, VF, or electrical storm despite complete revascularization and optimal medical therapy. |
|
Conditional recommendation |
|
We suggest intravenous lidocaine if beta-blockers, amiodarone, and overdrive stimulation are not effective/applicable in patients with recurrent VT with hemodynamic influence despite repetitive electrical cardioversion. |
|
Weak recommendation |
|
We recommend against the use of antiarrhythmic drugs in asymptomatic and hemodynamically irrelevant ventricular arrhythmias. |
|
Strong recommendation |
|
We recommend in cases of sinus bradycardia with hemodynamic instability or high degree AV block without stable escape rhythm the use of intravenous positive chronotropic medication (epinephrine, vasopressin, and/or atropine). |
|
Strong recommendation |
|
We recommend in cases of sinus bradycardia with hemodynamic instability or high degree AV block without stable escape rhythm the use of temporary pacing in cases of failure to respond to positive chronotropic medication. |
|
Strong recommendation |
|
We recommend in cases of sinus bradycardia with hemodynamic instability or high degree AV block without stable escape rhythm urgent angiography with a view to revascularization if the patient has not received previous reperfusion therapy. |
|
Strong recommendation |
|
We recommend urgent primary PCI strategy in patients with resuscitated cardiac arrest and an ECG consistent with STEMI. If PCI is not available, fibrinolytic therapy can be used with caution if there is no contraindication. |
|
Strong recommendation |
|
We recommend urgent coronary angiography (within 2 h) in survivors of cardiac arrest, including unresponsive survivors, when there is a high index of suspicion of ongoing STEMI that includes: · Presence of chest pain before arrest. · Clear history of established CAD. · Abnormal or uncertain ECG results. |
|
Conditional recommendation |
|
We recommend urgent echocardiography to exclude non-coronary causes (cerebrovascular event, respiratory failure, non-cardiogenic shock, pulmonary embolism, and intoxication). |
|
Strong recommendation |
|
We recommend urgent coronary angiography, with possible PCI, if suspected cardiac cause provided there is no evidence of poor neurological outcome that includes: · Unwitnessed cardiac arrest. · Late arrival of a pre-hospital team without basic life support (>10 min). · An initial non-shockable rhythm. · More than 20 min of advanced life support without return to spontaneous circulation. |
|
Conditional recommendation |
|
We recommend our hospitals to provide therapeutic hypothermia to unconscious patients after out of hospital cardiac arrest, aiming for a constant temperature between 32 and 36 C for at least 24 h. |
|
Conditional recommendation |
|
We recommend the indefinite use of aspirin in the dosage range of 75–162 mg/day for patients without contraindications after myocardial infarction. |
|
||
|
Strong recommendation |
|
||
|
We recommend the use clopidogrel (75 mg daily) in case of aspirin contraindication or intolerance as a single long-term therapy. |
|
||
|
Conditional recommendation |
|
||
|
We recommend that dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor (preferably ticagrelor) to be prescribed for up to 12 months in patients following acute myocardial infarction, irrespective of stent implantation unless there are contraindications such as excessive risk of bleeding. |
|
||
|
Strong recommendation |
|
||
|
We recommend oral beta blockers to patients with heart failure and/or LVEF ≤40% unless contraindicated. |
|
||
|
Strong recommendation |
|
||
|
We recommend routine oral beta blockers to be considered to all patients without contraindications. |
|
||
|
Conditional recommendation |
|
||
|
We recommend an LDL-C goal of <55 mg/dl and a reduction of at least 50% of the baseline LDL-C. |
|||
|
Strong recommendation |
|||
|
We recommend starting high-intensity statin therapy as early as possible, unless contraindicated, and maintain it for life. |
|||
|
Strong recommendation |
|||
|
We recommend, in patients with LDL-C not at goal despite a maximally tolerated statin dose, combination with Ezetimibe and/or protein convertase subtilisin/kexin type 9 reducing drugs (PCSK9i or Inclisiran). |
|||
|
Conditional recommendation |
|||
|
We recommend, for patients with statin intolerance, a reduced dose of statin therapy and/or ezetimibe. |
|||
|
Strong recommendation |
|||
|
We recommend Bempedoic acid in patients with statin intolerance, either alone or in combination with ezetimibe, as it has new evidence for safety and efficacy |
|||
|
Weak recommendation |
|||
|
We recommend that ACE inhibitors should be used starting from the first 24 h of STEMI in patients with evidence of heart failure, LV systolic dysfunction, diabetes, or an anterior infarct. |
|
||
|
Strong recommendation |
|
||
|
We recommend that a n ARB, preferably valsartan, can be an alternative to ACE inhibitors in patients with heart failure and/or LV systolic dysfunction, particularly those who are intolerant of ACE inhibitors. |
|
||
|
Strong recommendation |
|
||
|
We recommend routine ACEI/ARBS to be considered to all patients without contraindications. |
|
||
|
Conditional recommendation |
|
||
|
We recommend that MRAs should be used in patients with an LVEF ≤40% and heart failure or diabetes, who are already receiving an ACE inhibitor and a beta blocker, provided there is no renal failure or hyperkalemia. |
|
||
|
Strong recommendation |
|
||
|
We recommend, in cases of hypertension, tachycardia or angina, that non-dihydropyridine CCBs may be used if ß blockers are contraindicated particularly in the presence of obstructive airway disease. |
|
||
|
Conditional recommendation |
|
||
|
We do not recommend the routine use of oral nitrates in STEMI which was of no benefit in a randomized controlled trial. |
|
||
|
Conditional recommendation |
|
||
|
We recommend that SGLT2 inhibitors should be considered after STEMI especially if complicated with heart failure. |
|
||
|
Weak recommendation |
|
||
|
We recommend that ARNI, in place of ACE inhibitors or ARBS, should be considered after STEMI especially if complicated with heart failure. |
|
||
|
Weak recommendation |
|
||
|
We recommend that smoking should be discontinued by patients with a history of myocardial infarction. |
|
Strong recommendation |
|
We recommend that regular aerobic physical activity should be considered after myocardial infarction. |
|
Strong recommendation |
|
We recommend a healthy Mediterranean diet that controls blood pressure and BMI in the healthy range and avoiding alcohol. |
|
Strong recommendation |
|
We recommend that all patients after STEMI should be involved in a structured cardiac rehabilitation program. It includes exercise training, detecting and controlling risk factors, psychological counselling, guiding the patient to adopt healthy life style and be compliant to cardio protective medications. |
|
Strong recommendation |
|
We recommend that the patient should be counseled as to when to return back to work, sports, recreation and sexual activity while self monitoring biomedical indices. |
|
Strong recommendation |
- RECOMMENDATIONS
|
I. STEMI SYSTEMS OF CARE AND REPERFUSION ALGORITHMS4.5 |
|
A. STEMI REGIONAL NETWORKS |
|
· We recommend that the diagnosis and management of STEMI should be based on the implementation of “regional networks” between hospitals (‘hub’ and ‘spoke’ model) linked by an efficient ambulance service. · We recommend that each regional network (cluster of hub and spokes) should share a written protocol of referral and consultation |
|
Strong recommendation; moderate certainty evidence |
|
Implementation remarks · STEMI networks aim at providing timely and efficient care, reduce reperfusion delay, improve reperfusion rates, and apply protocols for updated STEMI care and thus improve prognosis of STEMI patients. · Every geographic area with one million inhabitants should be served by at least one or two hubs and 10-15 spokes. · The hub should be equipped with a cardiac catheterization facility and able to offer primary PCI around the clock (24 hours a day, 7days a week; 24/7). · The hub should act as a referral center to several smaller hospitals which are non-PCI capable facilities (spokes). · Patients arriving at spokes should be transferred via an ambulance to the hub while patients first seen by an ambulance should be transferred directly to the assigned hub bypassing the spokes. · Patients presenting to a non-PCI-capable hospital, and awaiting transportation for primary or rescue PCI, are attended in an appropriately monitored area. |
|
· We recommend that a national call center for the ambulance should be established and well publicized to make it easily remembered and used by patients. |
|
Strong recommendation, moderate certainty evidence |
|
· We recommend that patients with chest pain and/or suspected STEMI should dial the EMS call center number without delays. We do not recommend patients to use vehicles other than the EMS to reach hospitals in order to seek medical advice. |
|
Strong recommendation, moderate certainty evidence |
|
Implementation remarks · In Egypt, this number is 123 (ambulance service) or 16474 (critical care services). |
|
We recommend that all ambulance vehicles should be equipped with ECG machines and defibrillators. |
|
Strong recommendation, low certainty evidence |
|
We recommend that all ambulance personnel should be trained to recognize the symptoms of STEMI, administer aspirin, administer oxygen when appropriate, relieve pain and provide basic life support including using the defibrillator if indicated. |
|
Strong recommendation, low certainty evidence |
|
We recommend that all ambulance personnel should be trained to record an ECG and either interpret or transmit it, so that it can be reviewed by hospital-based cardiologist to establish or reject a STEMI diagnosis. |
|
Strong recommendation, low certainty evidence |
|
We recommend that once ECG diagnosis is confirmed, primary PCI team in the Cath lab of the Hub should be alerted of an imminent patient arrival |
|
Strong recommendation, low certainty evidence |
|
We recommend that all patients with confirmed or suspected STEMI should receive 300 mg of chewable aspirin as soon as possible if no contraindication. |
|
Strong recommendation, strong certainty evidence |
|
We recommend that the ambulance should transfer the clinically stable patient from the field to the nearest PCI capable hospital, bypassing non- PCI capable hospitals. |
|
Strong recommendation, low certainty evidence |
|
We recommend that if the patient during transfer becomes unstable or deteriorate clinically, he should be redirected to the nearest hospital with ER |
|
Strong recommendation, low certainty evidence |
|
We recommend that an ambulance transferring patients from the field to the hospital be equipped with a trained paramedic while an ambulance transferring patient in-between hospitals should include an accompanying doctor on board. |
|
Strong recommendation, low certainty evidence |
|
We recommend that all EMS should have a written protocol stating the updated management protocols and should establish a formal relationship with a PCI center to enable prompt patient transfer |
|
Strong recommendation, low certainty evidence |
|
We recommend that the time of EMS response, arrival to the patient, arrival to the designated hospital and the time of first ECG should be recorded and regularly audited aiming at improving performance quality metrics |
|
Strong recommendation, low certainty evidence |
|
Implementation remarks · The ambulance should be equipped by an ECG machine to do pre-hospital ECG that can be interpreted by a hospital-based consultant, directing the patient to the nearest primary PCI capable hospital. · The ambulance should be equipped by a defibrillator to revert fatal cardiac arrhythmias if such complication happens. |
|
A. REPERFUSION ALGORITHMS |
|
We recommend that reperfusion of the infarct related artery should be offered to all patients with STEMI presenting within the first 12 hours following chest pain onset. |
|
Strong recommendation, strong certainty evidence |
|
We recommend that reperfusion of the infarct related artery should be offered to all patients with STEMI presenting within the 12-48 hours following chest pain onset. |
|
Strong recommendation, moderate certainty evidence |
|
We recommend that primary PCI should be used as a default reperfusion strategy for suspected STEMI patients if time delay would not exceed 120 minutes. |
|
Strong recommendation, strong certainty evidence |
|
We recommend that patients should bypass non-PCI-capable centers and instead be transported to the nearest Primary PCI Centre with the goal of achieving a maximum FMC-to device time of ≤ 120 minutes (ideal FMC-to-device time ≤ 90 minutes in urban settings). |
|
Strong recommendation, moderate certainty evidence |
|
We recommend that in areas where the transfer of patients to the nearest hub will exceed 120 minutes, patients should be offered fibrinolytic therapy with immediate transfer afterwards to the hub for cardiac catheterization within 2-24 hours post fibrinolysis. This pathway is the Pharmacoinvasive pathway. |
|
Strong recommendation, strong certainty evidence |
Evidence and rationale:
Primary PCI is the preferred reperfusion strategy in patients with STEMI within 12h of symptom onset, provided it can be performed expeditiously (i.e. 120min from STEMI diagnosis) by an experienced team. An experienced team includes not only interventional cardiologists but also skilled support staff. Lower mortality rates among patients undergoing primary PCI are observed in centers with a high volume of PCI procedures.6 Real-life data confirm that primary PCI is performed faster and results in lower mortality if performed in high-volume centres.7 Randomized clinical trials in high volume, experienced centers have repeatedly shown that, if delay to treatment is similar, primary PCI is superior to fibrinolysis in reducing mortality, reinfarction, or stroke.8.9 However, in some circumstances, primary PCI is not an immediate option and fibrinolysis could be initiated expeditiously. The extent to which the PCl-related time delay diminishes the advantages of PCI over fibrinolysis has been widely debated. Because no specifically designed study has addressed this issue; The recent Strategic Reperfusion Early After Myocardial infarction (STREAM) trial randomized early STEMI presenters without the possibility of immediate PCI to immediate fibrinolysis (followed by routine early angiography) or transfer to primary PCl.10 The median PCl-related delay in this trial was 78min, and there were no differences in clinical outcomes. This Task Force recognizes the lack of contemporaneous data to set the limit to choose PCI over fibrinolysis. For simplicity, an absolute time from STEMI diagnosis to PCl-mediated reperfusion [I.e. wire crossing of the infarct-related artery (IRA)] rather than a relative PCl-related delay over fibrinolysis has been chosen. This limit is set to 120min.
Given the maximum limit of 10 min from STEMI diagnosis to bolus of fibrinolytics, the 120min absolute time would correspond to a PCl-related delay in the range of 110-120 min, being in the range of the times identified in old studies and registries as the limit delay to choose PCI.11-13
There is general agreement that a primary PCI strategy should also be followed for patients with symptoms lasting >12h in the presence of: (1) ECG evidence of ongoing ischemia; (2) ongoing or recurrent pain and dynamic ECG changes; and (3) ongoing or recurrent pain, symptoms. and signs of heart failure, shock, or malignant arrhythmias. However, there is no consensus as to whether PCI is also beneficial in patients presenting >12h from symptom onset in the absence of clinical and/or electrocardiographic evidence of ongoing ischemia. In asymptomatic patients without persistent symptoms 12-48 h after symptom onset, a small (n = 347) randomized study showed improved myocardial salvage and 4 year survival in patients treated with primary PCI compared with conservative treatment alone.14,15 However, in stable patients with persistent occlusion of the IRA 3-28 days after Ml, the large (n = 2166) Occluded Artery Trial {OAT) revealed no clinical benefit from routine coronary intervention with medical management, beyond that from medical management alone.16,17 A meta-analysis of trials testing whether late recanalization of an occluded IRAis beneficial showed no benefit of reperfusion.18 Therefore, routine PCI of an occluded IRA in asymptomatic patients >48 h after onset of symptoms is not indicated. These patients should be managed like all patients with chronic total occlusion, in which revascularization should be considered in the presence of symptoms or objective evidence of viability/ischemia in the territory of the occluded artery.19
If the reperfusion strategy is fibrinolysis, the goal is to inject the bolus of fibrinolytics within 10min from STEMI diagnosis. This time is selected based on the median time from randomization to bolus recorded in the STREAM trial which was 9 min.10 In previous ESC STEMI guidelines20, the target time was 30 min, but this was calculated from FMC (as opposed to STEMI diagnosis). STEMI diagnosis should occur within 10 min from FMC.
Figures 5 and 6 summarize target times for patients presenting in the pre hospital setting or in a non-PCI center.
To shorten the time to treatment. Fibrinolysis should be administered in the pre-hospital setting if possible.10,21,22 Patients should be transferred to a PCl-capable facility as soon as possible after the bolus of lytics administration.
Rescue PCI is indicated in the case of failed fibrinolysis (i.e. ST-segment resolution < 50% within 60-90 min of fibrinolytic administration), or in the presence of hemodynamic or electrical instability, worsening ischemia, or persistent chest pain,121124 while a routine early PCI strategy is indicated after successful fibrinolysis (preferably 2-24 h after fibrinolysis).23,24
Patients with a clinical presentation compatible with AMI and a non-interpretable ST-segment on the ECG, such as those with bundle branch block or ventricular pacing,25-27 should undergo a primary PCI strategy.
|
We recommend that public awareness campaigns should be organized to reduce “patient delay” and should include the following messages: · Importance to know common symptoms of STEMI and to recognize it as early as possible · Importance to react rapidly by calling the emergency services (123: ambulance service or 16474: critical cases services). |
|
Strong recommendation, low-certainty evidence |
|
We recommend the following measures and policies to help minimize “system delays”: · It is mandatory to do a pre-hospital ECG and diagnose a STEMI in less than 10 minutes from the patient presentation. · EMS personell should send the pre-hospital ECG to a hospital-based consultant to confirm or reject the diagnosis of STEMI. · Once the diagnosis of STEMI is confirmed in the pre-hospital setting, immediate activation of the catheterization laboratory should be initiated, the patient should be directed to the nearest hub (Hospital with 24/7 primary PCI service). · In the hub, the system should allow the EMS personell to bypass the emergency department and bring the patient straight to the catheterization laboratory. · For patients presenting in a non-capable PCI center, door-in to door-out time, defined as the duration between arrival of the patient at the hospital to discharge of the patient in an ambulance en route to the PCI center, should not exceed 30 minutes. · Patients who will receive fibrinolytic therapy should receive it in less than 10 minutes from diagnosis and should be transferred to a primary PCI capable center routinely within 2-24 hours after thrombolytic therapy · A written protocol in PCI non-capable hospitals should determine the reperfusion strategy of this hospital whether direct transfer to PCI capable hospital or transfer after fibrinolytic therapy. The written protocol should establish a formal relationship with a PCI center to enable prompt patient transfer. · All hospitals and EMS taking care of patients presenting with STEMI should adopt the time targets summarized in Table #. We recommend that management delays should be recorded and audited regularly and policies should be established to regularly improve them. |
|
Strong recommendation, low-certainty evidence |
|
Implementation remarks · The most important concept in the management of STEMI is the time urgency by which the patients are treated. · Management of delays are important indicators of quality of care in STEMI. Delay is a major cause of increased morbidity and mortality. · Delays are either due to late patient presentation or delays in the system of care during diagnosis and treatment. · Patient delay or late presentation to seek medical advice is a major problem in the management of STEMI. |
|
II. STEMI DIAGNOSIS |
|
A. CHEST PAIN ANALYSIS AND MANAGEMENT |
|
We recommend that appropriate and urgent management of STEMI starts from the moment of first medical contact (FMC) |
|
Strong recommendation, strong-quality evidence |
|
We recommend that correct diagnosis of STEMI is usually based on symptoms consistent with myocardial ischaemia (i.e., persistent chest pain) and 12-lead electrocardiogram (ECG). |
|
Strong recommendation, strong-quality evidence |
|
We recommend considering the typical characters of chest pain as retrosternal compression or heaviness with radiation to the left arm, neck, or lower jaw. |
|
Strong recommendation, weak-quality evidence |
|
We recommend that atypical and less-typical symptoms such as shortness of breath, nausea/vomiting, fatigue, palpitations, or syncope should be considered the presenting symptoms in some patients (e.g. in elderly and females). |
|
Strong recommendation, weak-quality evidence |
|
We do not recommend using reduction in chest pain after nitroglycerin (glyceryl trinitrate) administration as a diagnostic maneuver |
|
Moderate recommendation, weak-quality evidence |
|
We recommend that patients with ongoing ischemic discomfort should receive sublingual nitroglycerin (0.4 mg) or isosorbide dinitrates (5 mg) every 5 minutes for a total of 3 doses, after which an assessment should be made about the need for intravenous nitroglycerin. |
|
Strong recommendation, High-quality evidence |
|
We recommend that intravenous nitroglycerin is used for relief of ongoing ischemic discomfort, control of hypertension or management of pulmonary congestion. |
|
Strong recommendation, high-quality evidence |
|
We recommend that morphine sulfate (2 to 4 mg IV with increments of 2 to 8 mg repeated at 5-to-15-minute intervals) may be considered for severe pain refractory to nitrates and other anti-ischemic therapies with the goal of relieving pain and reducing anxiety. |
|
Moderate recommendation, moderate-quality evidence |
|
We Recommend that oral beta-blockers should be administered promptly to those patients without a contraindication irrespective of concomitant fibrinolytic therapy or performance of primary PCI. |
|
Strong recommendation, high-quality evidence |
|
We recommend IV beta-blockers promptly to STEMI patients without contraindications, especially if a tachy- arrhythmia or hypertension is present. |
|
Moderate recommendation, high-quality evidence |
|
We recommend against routine use of supplemental oxygen in patients with STEMI who have an arterial oxygen saturation ≥90 % with no signs of respiratory distress. |
|
Moderate recommendation, Low-quality evidence |
|
We recommend that patients with oxygen saturation <90% or respiratory distress should be treated with oxygen as needed. |
|
Strong recommendation, moderate-quality evidence |
|
We recommend that non-steroidal anti-inflammatory drugs (NSAIDs), except aspirin, should be avoided to relieve chest pain, or any other indication, in the acute phases of STEMI management. |
|
Moderate recommendation, moderate-quality evidence |
|
Implementation remarks • Relief of pain is of paramount importance, not only for comfort reasons but because the pain is associated with sympathetic activation, which causes vasoconstriction and increases the workload of the heart. • Control of cardiac pain is typically accomplished with a combination of nitrates, opiate analgesic agents, oxygen, and beta-adrenergic blockers. · In patients with STEMI, nitrates can reduce the symptoms of chest discomfort and HF as well as treat hypertension. However, nitrates can occasionally produce profound hypotension in patients with right ventricular infarction, aortic stenosis, or who recently used sildenafil. · Intravenous opioids (e.g., morphine) are the analgesics most used. However, morphine use is associated with a slower uptake, delayed onset of action, and reducing effects of oral antiplatelet agents (i.e., clopidogrel, ticagrelor, and prasugrel), which may lead to early treatment failure in susceptible individuals. · During the first few hours after the onset of STEMI, beta blocking agents may diminish myocardial oxygen demand by reducing heart rate, systemic arterial pressure, and myocardial contractility. · Routine use of supplemental oxygen in STEMI patients is of unclear benefit. |
Evidence and rationale:
Management-including diagnosis and treatment-of STEMI starts from the point of first medical contact (FMC). It is recommended that a regional reperfusion strategy should be established to maximize efficiency.
A working diagnosis of STEMI must first be made. This is usually based on symptoms consistent with myocardial ischemia (i.e., persistent chest pain) and signs [I.e. 12-lead electrocardiogram (ECG)]. Important dues are a history of CAD and radiation of pain to the neck. lower jaw, or left arm. Some patients present with less-typical symptoms such as shortness of breath, nausea/vomiting. fatigue, palpitations, or syncope.1 A reduction in chest pain after nitroglycerin (glyceryl trinitrate) administration can be misleading and is not recommended as a diagnostic maneuver.2 In cases of symptom relief after nitroglycerin administration, another 12-lead ECG must be obtained. A complete normalization of the ST-segment elevation after nitroglycerin administration, along with complete relief of symptoms, is suggestive of coronary spasm, with or without associated Ml. In these cases, an early coronary angiography (within 24 h) is recommended. In cases of recurrent episodes of ST-segment elevation or chest pain, immediate angiography is required.
• Relief of pain is of paramount importance, not only for comfort reasons but because the pain is associated with sympathetic activation, which causes vasoconstriction and increases the workload of the heart.
• Control of cardiac pain is typically accomplished with a combination of nitrates, opiate analgesic agents, oxygen, and beta-adrenergic blockers.
· In patients with STEMI, nitrates can reduce the symptoms of chest discomfort and HF as well as treat hypertension. However, nitrates can occasionally produce profound hypotension in patients with right ventricular infarction, aortic stenosis, or who recently used sildenafil.
· Intravenous opioids (e.g. morphine) are the analgesics most used. However, morphine use is associated with a slower uptake, delayed onset of action, and reducing effects of oral antiplatelet agents (i.e. clopidogrel, ticagrelor, and prasugrel), which may lead to early treatment failure in susceptible individuals.
· During the first few hours after the onset of STEMI, beta blocking agents may diminish myocardial oxygen demand by reducing heart rate, systemic arterial pressure, and myocardial contractility.
· Routine use of supplemental oxygen in STEMI patients is of unclear benefit.28-30
|
I. ECG INTERPRETATION |
|
We recommend 12-lead ECG recording and prompt interpretation in less than 10 min at the site of first medical contact (FMC). |
|
Strong recommendation, Moderate-quality evidence |
|
We recommend an ECG monitoring with defibrillator capacity as soon as possible in all patients with suspected or confirmed STEMI |
|
Strong recommendation, Moderate -quality evidence |
|
We recommend that, in the proper clinical context, ST-segment elevation (measured at the J-point) is considered suggestive of acute coronary artery occlusion when it is present in at least two contiguous leads with ST-segment elevation ≥2.5 mm in men < 40 years, ≥2 mm in men > 40 years, or ≥1.5 mm in women in leads V2–V3 and/or ≥1 mm in the other leads [in the absence of left ventricular hypertrophy or LBBB]. |
|
Strong recommendation, moderate-quality evidence |
|
We recommend in patients with inferior STEMI, to record right precordial leads (V3R and V4R) seeking ST segment elevation, to identify concomitant right ventricular (RV) infarction |
|
Moderate recommendation, weak-quality evidence |
|
We recommend that the presence of a Q-wave on the ECG should not necessarily change the reperfusion strategy decision. |
|
Strong recommendation, moderate-quality evidence |
|
We recommend that patients with a clinical suspicion of ongoing myocardial ischaemia and LBBB should be managed in a way similar to STEMI patients, regardless of whether the LBBB is previously known. |
|
Strong recommendation, moderate-quality evidence |
It is recommended to initiate ECG monitoring as soon as possible in all patients with suspected STEMI to detect life threatening arrhythmias and allow prompt defibrillation if indicated. When a STEMI is suspected, a 12-lead ECG must be acquired and interpreted as soon as possible at the time of FMC to facilitate early STEMI diagnosis and triage.31
In patients with a clinical suspicion of myocardial ischemia and STsegment elevation, reperfusion therapy needs to be initiated as soon as possible.32 If the ECG is equivocal or does not show evidence to support the clinical suspicion of Ml, ECGs should be repeated and,
when possible, compared with previous recordings. If interpretation of pre-hospital ECG is not possible on-site, field transmission of the ECG is recommended.33
In the proper clinical context, ST-segment elevation (measured at the J-point) is considered suggestive of ongoing coronary artery acute occlusion in the following cases: when it is present in at least two contiguous leads with ST-segment elevation ≥2.5 mm in men < 40 years, ≥2 mm in men > 40 years, or ≥1.5 mm in women in leads V2–V3 and/or ≥1 mm in the other leads [in the absence of left ventricular hypertrophy or LBBB].34
In patients with inferior Ml, it is recommended to record right precordial leads (V3R and V4R) seeking ST-segment elevation, to identify concomitant right ventricular (RV) infarction.35
Likewise, ST-segment depression in leads V1-V3 suggests myocardial ischemia, especially when the terminal T-wave is positive (ST-segment elevation equivalent), and confirmation by concomitant ST-segment elevation ≥ 0.5 mm recorded in leads V7, V9 should be considered as a means to identify posterior Ml.34
The presence of a Q-wave on the ECG should not necessarily change the reperfusion strategy decision.
The ECG diagnosis may be more difficult in some cases, which nevertheless deserve prompt management and triage. Among these:
Bundle branch block. In the presence of LBBB, the ECG diagnosis of AMI is difficult but often possible if marked ST-segment abnormalities are present. Somewhat complex algorithms have been offered to assist the diagnosis, but they do not provide diagnostic certainty.36
The presence of concordant ST-segment elevation (i.e. in leads with positive QRS deflections) appears to be one of the best indicators of ongoing Ml with an occluded infarct artery.37
Patients with a clinical suspicion of ongoing myocardial ischemia and LBBB should be managed in a way like STEMI patients, regardless of whether the LBBB is previously known. It is important to remark that the presence of a (presumed) new LBBB does not predict an Ml per se.38
Patients with Ml and right bundle branch block (RBBB) have a poor prognosis.55 It may be difficult to detect transmural ischemia in patients with chest pain and RBBB.
Therefore, a primary PCI strategy (emergent coronary angiography and PCI if indicated) should be considered when persistent ischemic symptoms occur in the presence of RBBB.
Ventricular pacing.
Pacemaker rhythm may also prevent interpretation of ST-segment changes and may require urgent angiography to confirm diagnosis and initiate therapy. Reprogramming the pacemaker-allowing an evaluation of ECG changes during intrinsic heart rhythm--may be considered in patients who are not dependent on ventricular pacing, without delaying invasive investigation.39.40
Non-diagnostic ECG.
Some patients with an acute coronary occlusion may have an initial ECG without ST-segment elevation, sometimes because they are seen very early after symptom onset (in which case, one should look for hyper-acute T-waves, which may pre cede ST-segment elevation). It is important to repeat the ECG or monitor for dynamic ST-segment changes. In addition, there is a concern that some patients with acute occlusion of a coronary artery and ongoing Ml, such as those with an occluded circumflex coronary artery,41,42 acute occlusion of a vein graft. or left main disease, may present without ST-segment elevation, and be denied reperfusion therapy, resulting in a larger infarction and worse outcomes. Extending the standard 12-lead ECG with V V9 leads may identify some of these patients. In any case, suspicion of ongoing myocardial ischemia is an indication for a primary PCI strategy even in patients without diagnostic ST-segment elevation.43-46
Isolated posterior Ml.
In AMI of the inferior and basal portion of the heart, often corresponding to the left circumflex territory, isolated ST-segment depression ≥ 0.5 mm in leads V1-V3 represents the dominant finding. These should be managed as a STEMI. The use of additional posterior chest wall leads [elevation V7-V9 ≥ 0.5mm (≥ 1mm in men, 40years old)] is recommended to detect ST segment elevation consistent with inferior and basal Ml.
Left main coronary obstruction.
The presence of ST depression 1mm in six or more surface leads (inferolateral ST depression), coupled with ST-segment elevation in aVR and/or V1, suggests multivessel ischemia or left main coronary artery obstruction, particularly if the patient presents with hemodynamic compromise.47
|
C. CARDIAC ENZYMES |
|
We recommend routine blood sampling for serum markers mainly troponins as soon as possible in the acute phase but this should not delay reperfusion treatment. Biomarkers can be of importance in clinical diagnosis and prognosis. We recommend hsTn if available. |
|
Strong recommendation, Low-quality evidence |
Evidence and rational:
Blood sampling for serum markers is routinely carried out in the acute phase. This is indicated but should not delay the reperfusion strategy/treatment.
If in doubt regarding the possibility of acute evolving Ml, emergency imaging aids the provision of timely reperfusion therapy to these patients. If echocardiography is not available or if doubts persist after echo, a primary PCI strategy is indicated (including immediate transfer to a PCI center if the patient is being treated in a non-PCI center).
Some non-AMI conditions can present with symptoms and ECG findings similar to STEMI. An emergency coronary angiography is therefore indicated in these cases.
|
IV. MANAGEMENT IN PCI CAPABLE HOSPITAL/ PRIMARY PCI and ADJUNCTIVE THERAPY (preferred prehospital diagnosis to overcome the delay in the ER) |
|
A. IN ER (OR IN THE CAH LAB IN CASE ER IS BYPASSED) |
|
We recommend quick history taking, assessing vital signs, identifying significant co-morbidities, securing an IV line and doing an ECG within 10 minutes from ER arrival, getting the Cath lab ready in <30 min, achieving door to balloon time of <60 min and overall FMC-to-device time of ≤ 90 minutes |
|
Strong Recommendation, Low-Quality Evidence |
|
We recommend giving the patient as soon as possible, if not previously given and if not contraindicated, 4 chewable aspirin tablets (300 mg). |
|
Strong Recommendation, moderate-Quality Evidence |
|
We recommend giving the patient, once diagnosed, Ticagrelor 180 mg (oral or via NGT) (or Clopidogrel 600 mg if Ticagrelor is not available or contraindicated). Ticagrelor contra-indications are history of intra-cerebral hemorrhage or moderate-severe hepatic failure. |
|
Strong Recommendation, high-Quality Evidence |
|
We do not recommend routine glycoprotein IIb/IIIa inhibitors or fibrinolytics before arrival at the catheter laboratory to people with acute STEMI for whom primary PCI is planned. |
|
moderate Recommendation, weak-Quality Evidence |
|
We recommend giving patients with persistent cardiac chest pain or discomfort sublingual Nitrates if SBP >140 mmHg and if RV infarct can be excluded. |
|
Conditional recommendation, weak evidence |
|
We recommend, If SBP <90 mmHg and patient is not in acute pulmonary edema, to administer a 300 mL fluid challenge. |
|
Conditional recommendation, weak evidence |
|
We recommend, if chest pain is still present, to administer morphine in increments of 2-4 mg. |
|
Conditional recommendation, weak evidence |
B. IN CATH LAB DURING PRIMARY PCI |
|
We recommend radial access over femoral access if performed by an experienced radial operator. |
|
(Conditional Recommendation, strong-Quality Evidence). |
|
We recommend use of UFH for procedural anticoagulation |
|
(Strong Recommendation, Low-Quality Evidence). |
|
We recommend that Enoxaparin can be used as an alternative option to UFH |
|
(Conditional Recommendation, Moderate-Quality Evidence). |
|
We recommend against using fondaparinux during primary PCI |
|
(Strong Recommendation, Moderate-Quality Evidence). |
|
We recommend Primary PCI of the IRA using DES |
|
(Strong Recommendation, high-Quality Evidence). |
|
We recommend CABG in patients with ongoing ischemia and large areas of jeopardized myocardium if PCI of the IRA cannot be performed |
|
(Conditional recommendation, low quality evidence) |
|
We recommend PCI of non-IRA lesions before hospital discharge, in hemodynamically stable patients with STEMI and multivessel disease. |
|
(Conditional Recommendation, high-Quality Evidence) |
|
We recommend PCI to culprit vessel only rather than complete revascularization during the index procedure in patients with STEMI and cardiogenic shock. |
|
(Conditional Recommendation, high-Quality Evidence). |
|
We recommend Re-do coronary angiography (with possible PCI) in patients with symptoms or signs of recurrent or remaining ischemia after primary PCI. |
|
(Strong Recommendation; Low-Quality Evidence). |
|
We recommend against the routine use of I.V. GPI for primary PCI except as bailout for patients with heavy thrombus burden. |
|
(Conditional Recommendation, High- Quality Evidence). |
|
We recommend Against the routine use of IC GPI for primary PCI |
|
(Strong Recommendation, High-Quality Evidence). |
|
We recommend against the routine use of IC fibrinolysis |
|
(Weak Recommendation; Low-Quality Evidence). |
|
We recommend against the routine use of IC adenosine to prevent no-reflow. |
|
(Weak Recommendation, Low-Quality Evidence). |
|
We recommend against the routine use of thrombus aspiration except as bailout for patients with heavy thrombus burden. |
|
(Strong Recommendation, High-Quality Evidence). |
|
We recommend against the routine use of deferred stenting. |
|
(Strong recommendation, moderate- Quality Evidence) |
|
IV. MANAGEMENT IN PCI NON-CAPABLE HOSPITAL; Transfer Vs FIBRINOLYSIS AND PHARMACOINVASIVE STRATEGY |
|
We recommend fibrinolytic therapy within 12 h of symptom onset if primary PCI cannot be performed within 120 min from STEMI diagnosis and there are no contraindications. |
|
(Strong recommendation-high certainty evidence) (3,4,5) |
|
We recommend Primary PCI rather than fibrinolysis in patients with heart failure/shock. |
|
(Strong recommendation-high certainty evidence) (18,22) |
|
We recommend, when fibrinolysis is the reperfusion strategy, to initiate this treatment as soon as possible after STEMI diagnosis. Door to needle time should not exceed 10 minutes. |
|
(Strong recommendation-high certainty evidence) (6,7,8,9) |
|
We recommend to use single-bolus weight adjusted tenecteplase tissue plasminogen activator (TNK-tPA) if available as it is preferred over streptokinase. |
|
(Conditional recommendation-moderate certainty evidence) (10) |
|
We recommend that late presenters (particularly >3 h) should be considered for transfer to primary PCI because the efficacy and clinical benefit of fibrinolysis decrease as the time from symptom onset increases. |
|
(Conditional recommendation-moderate certainty evidence) (3,4,5) |
|
We recommend that Clopidogrel (rather than ticagrelor) plus aspirin is preferred when fibrinolysis is the used strategy for reperfusion. |
|
(Strong recommendation-high certainty evidence) (11,12) |
|
We recommend that parenteral anticoagulation in patients treated with lytics is used until revascularization or for the duration of hospital stay up to 8 days. |
|
(Strong recommendation-high certainty evidence) (13,14,15) |
|
We recommend that the anticoagulant to be is Enoxaparin I.V. loading bolus followed by S.C. maintenance (preferred over UFH). |
|
(Strong recommendation-high certainty evidence) |
|
We recommend that the anticoagulant can also be UFH given as a weight-adjusted I.V. bolus followed by infusion. |
|
(Strong recommendation-moderate certainty evidence) |
|
We recommend that the anticoagulant can also be Fondaparinux I.V. bolus followed by S.C. dose 24 h later in patients treated with streptokinase. |
|
(Conditional recommendation-moderate certainty evidence) (16,17) |
|
We recommend transfer to a PCI-capable center angiography and PCI of the IRA following successful fibrinolysis in all patients within 2-24 hours after fibrinolysis. |
|
(Strong recommendation-high certainty evidence) (5,18,19,20,21) (24,25,26) |
|
We recommend rescue PCI immediately when fibrinolysis has failed (<50% ST-segment resolution at 60–90 min) or at any time in the presence of hemodynamic or electrical instability, or worsening ischaemia. |
|
(Strong recommendation-high certainty evidence) (5,18,23) |
|
We recommend emergency angiography and PCI in the case of recurrent ischaemia or evidence of reocclusion after initial successful fibrinolysis. |
|
(Strong recommendation-moderate certainty evidence) (18,22) |
|
The largest absolute benefit is seen among patients at highest risk, including the elderly, and when treatment is offered <2 h after symptom onset. (1,2) |
|
V. STEMI MANAGEMENT IN CCU AFTER REPERFUSION |
|
We recommend that same day repatriation can be considered provided that the patient 1. Has undergone a successful uncomplicated primary PCI 2. Is without ongoing myocardial ischemia 3. Is without arrhythmias 4. Is hemodynamically stable not requiring vasoactive or mechanical support 5. Does not need early revascularization to infarct-related or other arteries 6. Is transferred while monitored via ambulance and accompanied by a physician |
|
Conditional recommendation with low level of evidence |
|
We recommend that all STEMI patients with successful reperfusion therapy and an uncomplicated clinical course to be kept monitored by ECG in the CCU/ICU for a minimum of 24 hours, after which they can be transferred to a monitored intermediate care unit for an additional 24-48 hours. |
|
Strong recommendation with low level of evidence |
|
We recommend that early hospital discharge within 24-72 hours can be considered provided that the patient 1. Has undergone a successful uncomplicated primary PCI 2. Without ongoing ischemia, arrhythmias or hemodynamic instability 3. Does not need early revascularization to the infarct-related or other arteries 4. Is scheduled for early rehabilitation and adequate follow-up |
|
Conditional recommendation with low level of evidence |
|
We recommend short and long-term risk assessment as soon as the patient is admitted to CCU/ICU, through 1. Clinical evaluation for signs of ongoing ischemia or hemodynamic instability 2. Clinical evaluation, cardiac enzymes and echocardiography for assessment of extent of myocardial damage and state of LV and RV functions, exclude mechanical complications and LV thrombus 3. Clinical and laboratory assessment of dyslipidemia, dysglycemia, hypertension, renal dysfunction or peripheral vascular disease 4. Clinical, invasive coronary angiography or noninvasive imaging (stress echo, CMR, SPECT, or PET) to assess residual ischemia and myocardial viability in non-reperfused patients. |
|
Strong recommendation with low level of evidence |
|
· All hospitals taking care of patients with STEMI should have CCU/ICU equipped with monitors, defibrillators, mechanical ventilators and staff capable of managing ischemic heart disease and its complications. · The policy of same day transfer of patients with STEMI from Primary PCI-capable hospitals back to referring non-PCI capable hospitals (repatriation) helps keeping CCU beds available for new cases of primary PCI and helps keeping bonds with the patients and their nearby local hospitals. |
|
V. HIGH RISK STEMI PATIENTS AND COMPLICATIONS |
|
A. STEMI PATIENTS ON ORAL ANTICOAGULANTS |
|
We recommend the continuation of chronic anticoagulation regimen during admission. |
|
Strong recommendation, weak-quality evidence |
|
We recommend Primary PCI rather than fibrinolytic therapy regardless of the anticipated time delay. |
|
Strong recommendation, weak-quality evidence |
|
We recommend Radial over femoral approach during PPCI. |
|
Strong recommendation, weak-quality evidence |
|
We recommend the use of additional parenteral anticoagulation while in the cath lab during primary PCI, regardless of the timing of the last dose of oral anticoagulants. |
|
Strong recommendation, weak-quality evidence |
|
We recommend giving the usual 300 mg loading dose of oral aspirin. |
|
Strong recommendation, weak-quality evidence |
|
We recommend using clopidogrel (600 mg loading dose) rather than ticagrelor or prasugrel. |
|
Strong recommendation, weak-quality evidence |
|
We recommend prescribing triple antithrombotic therapy for the first week after primary PCI and up to one month in high thrombotic risk and low bleeding risk, after which we recommend discontinuing aspirin and continue on oral anticoagulants and clopidogrel for one year. Then, we recommend keeping the patient on oral anticoagulants only thereafter. |
|
Strong recommendation, weak-quality evidence |
|
We recommend the assessment of bleeding risk in all patients. |
|
Strong recommendation, weak-quality evidence |
|
We recommend the use of Novel oral anticoagulants over warfarin for patients with non-valvular atrial fibrillation. |
|
Strong recommendation, weak-quality evidence |
|
We recommend that in case of warfarin, the dose intensity should be carefully monitored with a target international normalized ratio (INR) in the lower part of the recommended target range. When non-vitamin K antagonist oral anticoagulants are used, the lowest effective tested dose for stroke prevention should be applied. |
|
Strong recommendation, weak-quality evidence |
|
We recommend against the use of GP IIB/IIIA inhibitors. |
|
Strong recommendation, weak-quality evidence |
|
We recommend adding proton pump inhibitor for gastric protection. |
|
Strong recommendation, Moderate-quality evidence |
Evidence and rationale:
Many patients presenting with STEMI are previously on oral anticoagulation or require long-term anticoagulation afterwards. The addition of DAPT to oral anticoagulation increases the risk of bleeding complications two- to three-fold compared to anticoagulation alone, based on data from RE-LY Trial.48 Given that oral anticoagulation is a relative contraindication for fibrinolysis, when these patients present with a STEMI, they should be triaged for primary PCI strategy regardless of the anticipated time to PCI-mediated reperfusion. Patients should receive additional parenteral anticoagulation, regardless of the timing of the last dose of oral anticoagulant. GP IIb/IIIa inhibitors should be avoided. Loading of aspirin should be done as in all STEMI patients, and clopidogrel is the P2Y12 inhibitor of choice (600 mg loading dose) before or at the latest at the time of PCI. Prasugrel and ticagrelor are not recommended. Ideally, a chronic anticoagulation regimen should not be stopped during admission. Gastric protection with a proton pump inhibitor (PPI) is recommended.
In general, continuation of oral anticoagulation in patients with an indication for DAPT should be evaluated carefully and continued only if compelling evidence exists.49
Ischemic and bleeding risks should be taken into consideration. For most patients, triple therapy (in the form of oral anticoagulation, aspirin, and clopidogrel) should be considered for 6 months. Then, oral anticoagulation plus aspirin or clopidogrel should be considered for an additional 6 months. After 1 year, it is indicated to maintain only oral anticoagulation. In cases of very high bleeding risk, triple therapy can be reduced to 1 month after STEMI, continuing on dual therapy (oral anticoagulation plus aspirin or clopidogrel) up to 1 year, and thereafter only anticoagulation.50
The dose intensity of oral anticoagulation should be carefully monitored with a target international normalized ratio in the lower part of the recommended target range. When non-vitamin K antagonist oral anticoagulants are used, the lowest effective tested dose for stroke prevention should be applied. In general, dose reduction below the approved dose is not recommended. The Open-Label, Randomized, Controlled, Multicenter Study Exploring Two Treatment Strategies of Rivaroxaban and a Dose-Adjusted Oral Vitamin K Antagonist Treatment Strategy in Subjects with Atrial Fibrillation who Undergo Percutaneous Coronary Intervention (PIONEER AF-PCI) study randomized 2124 patients with non-valvular AF, who had undergone PCI with stenting (∼12% STEMI patients), to receive low-dose rivaroxaban [15 mg o.d. (once a day)] plus a P2Y12 inhibitor (93% clopidogrel) and no aspirin for 12 months, very-low-dose rivaroxaban (2.5 mg b.i.d.) plus DAPT (95% clopidogrel) for 1, 6, or 12 months, or standard therapy with a dose-adjusted vitamin K antagonist plus DAPT (96% clopidogrel) for 1, 6, or 12 months. The primary safety endpoint (TIMI clinically significant bleeding) was lower in the two groups receiving rivaroxaban. No difference in major bleeding or transfusion was observed across groups. However, this study was underpowered for assessing differences in ischemic events such as stent thrombosis or stroke rates. Therefore, uncertainty remains regarding the comparative performance of three tested antithrombotic regimens in patients at high stroke and/or stent thrombosis risk.51
|
A. STEMI ELDERLY PATIENTS (ABOVE 70 YEARS) |
|
We recommend to maintain a high index of suspicion for diagnosing STEMI in elderly patients who present with atypical complaints. |
|
Strong recommendation, weak-quality evidence |
|
We recommend Primary PCI or thrombolytic therapy (according to the standard indications) with no upper age limit. |
|
Strong recommendation, weak-quality evidence |
|
We recommend radial access over femoral access to reduce bleeding risk. |
|
Strong recommendation, weak-quality evidence |
|
We recommend against giving a loading dose of clopidogrel when thrombolytic therapy is indicated. |
|
Strong recommendation, weak-quality evidence |
|
We recommend adding proton pump inhibitor for gastric protection. |
|
Strong recommendation, moderate-quality evidence |
Evidence and rationale:
It is key to maintain a high index of suspicion for MI in elderly patients who present with atypical complaints, based on the data from the GRACE study.52 In addition, the elderly have more comorbidities and are less likely to receive reperfusion therapy compared with younger patients, based on the data from both the ACACIA registry and the Vital Heart Response registry.53,54 Elderly patients are also at particular risk of bleeding and other complications from acute therapies because bleeding risk increases with age, renal function tends to decrease, and the prevalence of comorbidities is high, based on observational studies that shown frequent excess dosing of antithrombotic therapies in elderly patients.55 There is no upper age limit with respect to reperfusion, especially with primary PCI, based on the data from TRIANA trial.56
|
B. STEMI DIABETIC PATIENTS |
|
We recommend to maintain a high index of suspicion for diagnosing STEMI in patients with diabetes who present with atypical complaints. |
|
Strong recommendation, Low-quality evidence |
|
We recommend that selection of reperfusion therapy (primary PCI or fibrinolytics) is like patients without diabetes. |
|
Strong recommendation, Low-quality evidence |
|
We recommend the use of the more potent oral P2Y12 receptor inhibitors (prasugrel or ticagrelor) over clopidogrel. |
|
Strong recommendation, Low-quality evidence |
|
We recommend the evaluation of glycemic status in all STEMI patients with and without a known history of diabetes or hyperglycemia, and to monitor it frequently in diabetic patients and patients with hyperglycemia. |
|
Strong recommendation, Low-quality evidence |
|
We recommend management of hyperglycemia and maintain a blood glucose concentration ≤200 mg/dl but absolutely avoid hypoglycemia (defined as glucose levels ≤70 mg/dl). |
|
Moderate recommendation, weak-quality evidence |
|
We recommend the assessment of the renal insufficiency risk and to measure eGFR in patients on metformin and/or sodium-glucose co-transporter-2 (SGLT2) inhibitors. |
|
Strong recommendation, Low-quality evidence |
Patients with diabetes are known to present with atypical chest pain more frequently than patients without diabetes and consequently may receive delayed initiation of treatment.57
Although patients with diabetes are at higher risk of death and complications (including repeat revascularization after PCI), selection of antithrombotic therapies and reperfusion therapy is the same as in patients without diabetes. Regarding the use of antiplatelet drugs, the more potent oral P2Y12 receptor inhibitors (prasugrel or ticagrelor) have consistently shown increased relative benefits with higher absolute risk reductions in patients with diabetes compared with clopidogrel.58
On admission, it is recommended to evaluate glycemic status in all STEMI patients with and without a known history of diabetes or hyperglycemia, and to monitor it frequently in diabetic patients and patients with hyperglycemia. In critically ill patients, there is a high risk of hypoglycemia-related events when using intensive insulin therapy.59
In the absence of robust data to guide the optimal glucose management (e.g., treatment thresholds and glucose targets) in STEMI patients, a close but not too strict glucose control seems the best approach. In the acute phase, it is reasonable to manage hyperglycemia (i.e., maintain a blood glucose concentration ≤11.0 mmol/L or 200 mg/dL) but absolutely avoid hypoglycemia.60
|
C. STEMI PATIENTS WITH RENAL DYSFUNCTION |
|
We recommend to maintain a high index of suspicion for diagnosing STEMI in patients with renal dysfunction who present with atypical complaints. |
|
Strong recommendation, weak-quality evidence |
|
We recommend measuring eGFR as soon as possible in patients with suspected renal dysfunction as elderly, diabetics, and heart failure. |
|
Strong recommendation, weak-quality evidence |
|
We recommend adjusting dose of antithrombotic drugs according to renal function. |
|
Strong recommendation, weak-quality evidence |
|
We recommend adequate hydration during and after primary PCI and limiting the dose of contrast agents, preferentially low-osmolality contrast agents to reduce the risk of contrast-induced nephropathy. |
|
Strong recommendation, weak-quality evidence |
|
We recommend adding proton pump inhibitor for gastric protection |
|
Strong recommendation, weak-quality evidence |
Renal dysfunction is present in approximately 30–40% of patients with ACS and is associated with a worse prognosis and increased risk of in-hospital complications.61
Owing to differences in presentation (less frequent presentation with chest pain and fewer typical ECG signs) diagnosis may be delayed. Although decisions on reperfusion in patients with STEMI have to be made before any assessment of renal function is available, it is important to estimate the GFR as soon as possible. The type and dose of antithrombotic agent and the amount of contrast agent should be considered based on renal function.61
Ensuring proper hydration during and after primary PCI and limiting the dose of contrast agents, preferentially low-osmolality contrast agents, are important steps in minimizing the risk of contrast-induced nephropathy.62
|
D. NON-REPERFUSED STEMI PATIENTS |
|
We recommend immediate assessment of non-reperfused patients for evidence of electrical or hemodynamic instability or evidence of ongoing ischemia. This evidence would make them candidates for primary PCI even beyond the time window of reperfusion. |
|
Strong recommendation, weak-quality evidence |
|
We recommend doing echocardiography as soon as possible for these patients to detect complications or any indication for invasive intervention. |
|
Strong recommendation, weak-quality evidence |
|
We recommend noninvasive tests to detect evidence of residual ischemia or myocardial viability that indicate further invasive assessment with or without revascularization. |
|
Strong recommendation, weak-quality evidence |
|
We recommend medical therapy including DAPT and secondary prevention therapies for stable patients who were not reperfused. |
|
Strong recommendation, weak-quality evidence |
|
We recommend that in patients in whom PCI is finally performed, ticagrelor is preferred, while in patients who do not undergo PCI, either ticagrelor or clopidogrel can be used. |
|
Strong recommendation, weak-quality evidence |
|
We recommend anticoagulation, preferably with fondaparinux, until coronary revascularization is done or hospital discharge. |
|
Strong recommendation, weak-quality evidence |
|
We recommend against routine reperfusion of the infarct related artery in stable patients beyond the first 48 hour of symptom onset. |
|
Strong recommendation, weak-quality evidence |
A primary PCI strategy is indicated in the presence of signs or symptoms suggestive of ongoing myocardial ischemia, heart failure, hemodynamic instability, or life-threatening arrhythmias in patients fail to receive reperfusion therapy within the recommended time (first 12 h),63 and should be considered in stable asymptomatic patients between 12–48 h after symptom onset.64,65
After that time, either a non-invasive test for the presence of residual myocardial ischemia/viability to decide a late invasive strategy or elective coronary angiography should be considered. However, routine PCI is not indicated in totally occluded IRA beyond the first 48 h from symptom onset due to the increased risk of late complications.66
Early echocardiography with LVEF assessment is indicated in all patients. Medical therapy should include DAPT, anticoagulation, and secondary prevention therapies. In patients in whom PCI is finally performed, ticagrelor or prasugrel are preferred,67 while in patients who do not undergo PCI, clopidogrel is indicated.68
Anticoagulation, preferably with fondaparinux, is indicated until coronary revascularization is done or hospital discharge.69
|
F. STEMI COMPLICATED BY ACUTE HEART FAILURE: |
|
We recommend the initiation of ACE inhibitor (or if not tolerated, ARB) therapy as soon as possible in all hemodynamically stable patients with evidence of LVEF ≤ 40% and/or heart failure to reduce the risk of hospitalization and death. |
|
Strong recommendation, High quality evidence |
|
We recommend the initiation of Beta-blocker therapy in patients with LVEF ≤ 40% and/or heart failure after stabilization, to reduce the risk of death, recurrent MI, and hospitalization for heart failure |
|
Strong recommendation, High-quality evidence |
|
We recommend the initiation of an MRA therapy in patients with heart failure and LVEF ≤ 40% with no severe renal failure or hyperkalemia to reduce the risk of cardiovascular hospitalization and death. |
|
(Strong recommendation, Moderate-quality evidence) |
|
We recommend the use of Loop diuretics in patients with acute heart failure with symptoms/signs of fluid overload to improve symptoms. |
|
(Strong recommendation, Low-quality evidence) |
|
We recommend the use of IV nitrates in patients with symptomatic heart failure with SBP >90 mmHg to improve symptoms and reduce congestion. |
|
(Strong recommendation, Low-quality evidence) |
|
We suggest the use of Intravenous nitrates or sodium nitroprusside in patients with heart failure and elevated SBP to control blood pressure and improve symptoms. |
|
(Moderate recommendation, Low-quality evidence) |
|
We recommend Oxygen therapy in patients with pulmonary oedema with SaO2 < 90% to maintain a saturation > 95%. |
|
(Strong recommendation, Low-quality evidence) |
|
We suggest non-invasive positive pressure ventilation (continuous positive airway pressure, biphasic positive airway pressure) in patients with respiratory distress (respiratory rate >25 breaths/min, SaO2 <90%) without hypotension. |
|
(Moderate recommendation, Moderate-quality evidence) |
|
We recommend patient intubation in patients with respiratory failure or exhaustion, leading to hypoxemia, hypercapnia, or acidosis, and if non-invasive ventilation is not tolerated. |
|
(Strong recommendation, Low-quality evidence) |
|
We recommend the use of opiates to relieve dyspnea and anxiety in patients with pulmonary oedema and severe dyspnea. Respiration should be monitored. |
|
(Weak recommendation, Moderate-quality evidence) |
|
We recommend the use of IV inotropic agents and/or vasopressors in patients with severe heart failure with hypotension (systolic BP < 90 mmHg) refractory to standard medical treatment. |
|
(Weak recommendation, Low-quality evidence) |
|
We recommend that SGLT2 inhibitors may be considered in the setting of acute STEMI especially in diabetic patients and if complicated with heart failure after stabilization. |
|
(Weak recommendation, weak-quality evidence) |
|
We recommend that ARNI, in place of ACE inhibitors or ARBS, may be considered in the setting of acute STEMI especially if complicated with heart failure after stabilization. |
|
(Weak recommendation, weak-quality evidence) |
Severely symptomatic patients with pulmonary congestion may also need i.v. morphine to reduce dyspnea and anxiety, but routine use is not recommended due to concerns about its safety, as it may induce nausea and hypopnea.70
Non-invasive positive pressure ventilation (continuous positive airway pressure, biphasic positive airway pressure) or high-flow nasal cannula is effective in treating pulmonary oedema and should be considered in patients with respiratory distress (respiratory rate >25 breaths/min, SaO2 <90%) and started soon.71
In patients with heart failure and adequate blood pressure (SBP >90 mmHg), but a severe reduction in cardiac output resulting in compromised vital organ perfusion not responding to standard therapy, treatment with dobutamine or levosimendan may be considered. However, the clinical evidence of levosimendan in cardiogenic shock is limited.72
Considering the residual risk on contemporary medical treatment, as well as the growing evidence and mechanisms of action of SGLT2 inhibitors, it is enticing to consider their potential to improve outcomes in acute MI if initiated early in the course of presentation. Prior trials of patients with T2DM, HF, or nephropathy predominantly focused on stable outpatients and excluded patients with recent acute cardiovascular events. A STEMI with a high degree of myocardial injury that confers high risk for negative ventricular remodeling may be particularly inviting to early SGLT2 inhibitor therapy based on timing of initiation. Variation in hemodynamic stability, dynamic changes in cardiac output, intracardiac filling pressures, degree of left ventricular dysfunction, peripheral organ perfusion, renal function, and timing of concomitant therapy including coronary revascularization may also affect the relative efficacy and safety of SGLT2 inhibition. Factoring these considerations, similar to the timing of initiation of angiotensin-converting enzyme inhibitor and beta-blocker, the most appropriate timing for SGLT2 inhibition is presumably upon establishment of hemodynamic stability.73 In T2DM AMI patients, the use of SGLT2-I was associated with a lower risk of adverse cardiovascular outcomes during index hospitalization and long-term follow-up.74
For patients with acute anterior STEMI undergoing primary PCI, early initiation of ARNI provided significant clinical benefits.75
In PARADISE-MI trial, Sacubitril–valsartan was not associated with a significantly lower incidence of death from cardiovascular causes or incident heart failure than ramipril among patients with acute myocardial infarction.76
|
G. STEMI COMPLICATED BY CARDIOGENIC SHOCK |
|
We recommend immediate primary PCI to infarct related artery if coronary anatomy is suitable. |
|
Strong recommendation, Moderate-quality evidence |
|
We recommend primary PCI to infarct related artery only as the default strategy. |
|
Strong recommendation, Moderate-quality evidence |
|
We recommend fibrinolysis if a primary PCI strategy is not available within 120 min from STEMI diagnosis and mechanical complications have been ruled out. |
|
Moderate recommendation, Low-quality evidence |
|
We recommend emergency CABG if coronary anatomy is not suitable for PCI, or if PCI has failed , or in case of mechanical complication. |
|
Strong recommendation, Moderate-quality evidence |
|
We recommend continuous invasive blood pressure monitoring with an arterial line. |
|
Strong recommendation, Low-quality evidence |
|
We recommend hemodynamic assessment with pulmonary artery catheter for confirming diagnosis or guiding therapy. |
|
Weak recommendation, Moderate-quality evidence |
|
We recommend immediate echocardiography to assess ventricular and valvular functions, loading conditions, and to detect mechanical complications. |
|
Strong recommendation, Low-quality evidence |
|
We recommend that mechanical complications to be treated as early as possible after discussion by the Heart Team. |
|
Strong recommendation, Low-quality evidence |
|
We recommend Oxygen/mechanical respiratory support according to blood gases. |
|
Strong recommendation, Low-quality evidence |
|
We recommend the use of intra-aortic balloon pumping in patients with mechanical complications. |
|
Moderate recommendation, Low-quality evidence |
|
We recommend against the routine use of intra-aortic balloon pumping. |
|
Strong recommendation, Moderate-quality evidence |
|
We recommend Ultrafiltration in patients with refractory congestion who failed to respond to diuretics. |
|
Weak recommendation, Moderate-quality evidence |
|
We recommend the use of Inotropic/vasopressor agents for hemodynamic stabilization. |
|
Weak recommendation, Low-quality evidence |
|
We recommend the short-term use of mechanical circulatory support e.g. ECLS or ECMO in patients in refractory shock. |
|
Weak recommendation, Low-quality evidence |
In STEMI patients presenting with cardiogenic shock in which PCI-mediated reperfusion is estimated to occur >120 min, immediate fibrinolysis and transfer to a PCI center should be considered. Cardiogenic shock characterization and management do not necessarily need invasive hemodynamic monitoring, but ventricular and valve function should be urgently evaluated by transthoracic echocardiography and associated mechanical complications ruled out.77,78
Treatments include immediate reperfusion, with primary PCI whenever possible.79
Invasive monitoring with an arterial line is recommended.72
Diuretic therapy is recommended when adequate perfusion is attained. Intravenous inotropic agents or vasopressors are usually required to maintain an SBP >90 mmHg, and to increase cardiac output and improve vital organ perfusion. Dobutamine is the initial therapy for patients with predominant low cardiac output, whereas norepinephrine may be safer and more effective than dopamine in patients with cardiogenic shock and severe hypotension.80
IABP counterpulsation does not improve outcomes in patients with STEMI and cardiogenic shock without mechanical complications,81 nor does it significantly limit infarct size in those with potentially large anterior MIs.82
Therefore, routine IABP counterpulsation cannot be recommended, but may be considered for hemodynamic support in selected patients (i.e., severe mitral insufficiency or ventricular septal defect). A small exploratory trial studying the Impella CP percutaneous circulatory support device did not find any benefit compared with IABP in AMI complicated by cardiogenic shock.83
Mechanical LV assist devices (LVADs), including percutaneous short-term mechanical circulatory support devices (i.e., intra-cardiac axial flow pumps and arterial-venous extracorporeal membrane oxygenation), have been used in patients not responding to standard therapy, including inotropes, fluids, and IABP, but evidence regarding their benefits is limited.84
Therefore, short-term mechanical circulatory support may be considered as a rescue therapy in order to stabilize the patients and preserve organ perfusion (oxygenation) as a bridge to recovery of myocardial function, cardiac transplantation, or even LV assist device destination therapy on an individual basis.85,86
|
H. STEMI COMPLICATED BY ATRIAL FIBRILLATION |
|
We recommend the use of intravenous beta-blockers for rate control if there are no clinical signs of acute heart failure or hypotension. |
|
Strong recommendation, low-quality evidence |
|
We recommend the use of intravenous amiodarone for rate control, in case of concomitant acute heart failure but no hypotension. |
|
Strong recommendation, low-quality evidence |
|
We recommend that the use of intravenous digitalis for rate control, might be considered, in case of concomitant acute heart failure and hypotension. |
|
Conditional recommendation, moderate-quality evidence |
|
We recommend immediate electrical cardioversion when adequate rate control cannot be achieved promptly with pharmacological agents and ongoing ischemia, severe hemodynamic compromise, or heart failure. |
|
Strong recommendation, low-quality evidence |
|
We recommend the use of intravenous amiodarone to promote electrical cardioversion and/or decrease risk for early recurrence of AF after electrical cardioversion. |
|
Strong recommendation, low-quality evidence |
|
We recommend long term anticoagulation depending on CHA₂DS₂-VASc score and taking concomitant antithrombotic therapy into account |
|
Conditional recommendation, low-quality evidence |
|
We recommend against the prophylactic treatment with antiarrhythmic drugs to prevent AF in STEMI patients. |
|
Strong recommendation, moderate-quality evidence |
The most frequent supraventricular arrhythmia is AF, with up to 21% of STEMI patients affected.87
Electrical cardioversion should be considered but early recurrence of AF is frequent after successful cardioversion. Acute rhythm control with antiarrhythmic drugs is limited to the use of amiodarone.88
Adequate rate control can be accomplished by administration of beta-blockers.89
Patients with AF and risk factors for thromboembolism should be adequately treated with chronic oral anticoagulation.88
I. STEMI COMPLICATED BY VENTRICULAR TACHYCARDIA / FIBRILLATION |
|
We recommend the use of intravenous beta-blocker treatment in STEMI patients with polymorphic VT and/or VF unless contraindicated. |
|
Strong recommendation, Moderate-quality evidence |
|
We recommend prompt and complete revascularization to treat myocardial ischemia that may be present in patients with recurrent VT and/or VF. |
|
Strong recommendation, Low-quality evidence |
|
We recommend the use of intravenous amiodarone in treatment of recurrent polymorphic VT. |
|
Strong recommendation, Low-quality evidence |
|
We suggest the use of intravenous amiodarone for recurrent VT with hemodynamic intolerance despite repetitive electrical cardioversion. |
|
Conditional recommendation, Low-quality evidence |
|
We recommend correction of electrolyte imbalances (especially hypokalemia and hypomagnesemia) in patients with VT and/or VF. |
|
Strong recommendation, Low-quality evidence |
|
We suggest transvenous catheter pace termination and/or overdrive pacing if VT cannot be controlled by repetitive electrical cardioversion. |
|
Conditional recommendation, Low-quality evidence |
|
We suggest radiofrequency catheter ablation followed by ICD implantation in patients with recurrent VT, VF, or electrical storm despite complete revascularization and optimal medical therapy. |
|
Conditional recommendation, Low-quality evidence |
|
We suggest intravenous lidocaine if beta-blockers, amiodarone, and overdrive stimulation are not effective/applicable in patients with recurrent VT with hemodynamic influence despite repetitive electrical cardioversion. |
|
Weak recommendation, Low-quality evidence |
|
We recommend against the use of antiarrhythmic drugs in asymptomatic and hemodynamically irrelevant ventricular arrhythmias. |
|
Strong recommendation, Low-quality evidence |
The incidence of VT and VF has declined over recent decades, most probably due to the uptake of reperfusion strategies and the early use of beta-blockers.90 However, 6–8% of patients still develop hemodynamically significant VT or VF during this phase.91
Beta-blockers are recommended if no contraindications exist.92 If there is no sufficient control, i.v. administration of amiodarone is recommended.93 In case of contraindications to amiodarone, i.v. lidocaine may be considered, although no studies comparing superiority of either drug in STEMI patients are available. VT or VF may occur at the time of restoration of coronary blood flow (reperfusion arrhythmias). No specific antiarrhythmic drug therapy is necessary due to the benign long-term course.94
|
J. STEMI COMPLICATED BY SINUS BRADYCARDIA OR HIGH DEGREE AV BLOCK |
|
We recommend in cases of sinus bradycardia with hemodynamic instability or high degree AV block without stable escape rhythm the use of intravenous positive chronotropic medication (epinephrine, vasopressin, and/or atropine). |
|
Strong recommendation, Low-quality evidence |
|
We recommend in cases of sinus bradycardia with hemodynamic instability or high degree AV block without stable escape rhythm the use of temporary pacing in cases of failure to respond to positive chronotropic medication. |
|
Strong recommendation, Low-quality evidence |
|
We recommend in cases of sinus bradycardia with hemodynamic instability or high degree AV block without stable escape rhythm urgent angiography with a view to revascularization if the patient has not received previous reperfusion therapy. |
|
Strong recommendation, Low-quality evidence |
Evidence and rationale:
Sinus bradycardia is common in the first hours of STEMI, especially in inferior MI. In some cases, opioids are responsible.95 It often requires no treatment. If accompanied by severe hypotension, sinus bradycardia should be treated with i.v. atropine. Second-degree type I (Mobitz I or Wenckebach) AV block is usually associated with inferior wall MI and seldom causes adverse hemodynamic effects. If so, atropine should be used first; if it fails, pacing should be instituted. Agents that slow AV conduction (such as beta-blockers, digitalis, verapamil, or amiodarone) should be used with caution. Second-degree type II (Mobitz II) AV block and complete AV block may be indications for pacing. A transvenous pacing electrode should be inserted in the presence of advanced AV block with a low escape rhythm, and considered if bifascicular or trifascicular block develops.96
|
K. STEMI COMPLICATED BY OUT-OF-HOSPITAL CARDIAC ARREST |
|
We recommend urgent primary PCI strategy in patients with resuscitated cardiac arrest and an ECG consistent with STEMI. If PCI is not available, fibrinolytic therapy can be used with caution if there is no contraindication. |
|
Strong recommendation, Low-quality evidence |
|
We recommend urgent coronary angiography (within 2 h) in survivors of cardiac arrest, including unresponsive survivors, when there is a high index of suspicion of ongoing STEMI that includes: · Presence of chest pain before arrest. · Clear history of established CAD. · Abnormal or uncertain ECG results. |
|
Conditional recommendation, Low-quality evidence |
|
We recommend urgent echocardiography to exclude non-coronary causes (cerebrovascular event, respiratory failure, non-cardiogenic shock, pulmonary embolism, and intoxication). |
|
Strong recommendation, Low-quality evidence |
|
We recommend urgent coronary angiography, with possible PCI, if suspected cardiac cause provided there is no evidence of poor neurological outcome that includes: · Unwitnessed cardiac arrest. · Late arrival of a pre-hospital team without basic life support (>10 min). · An initial non-shockable rhythm. · More than 20 min of advanced life support without return to spontaneous circulation. |
|
(Conditional recommendation, Low-quality evidence) |
|
We recommend our hospitals to provide therapeutic hypothermia to unconscious patients after out of hospital cardiac arrest, aiming for a constant temperature between 32 and 36 C for at least 24 h. |
|
(Conditional recommendation, Low-quality evidence) |
|
Societal recommentdations to improve the outcome of out of hospital cardiac arrest · Encourage private and governmental non-medical institutes to provide training in basic life support of at least 20% of their staff. · Mass training of high school and university students for basic life support. · Spread of automated defibrillator in the public places as a second step after training on BLS. |
Evidence and rationale:
Many deaths occur very early after STEMI onset due to ventricular fibrillation (VF). As this arrhythmia frequently occurs at an early stage, these deaths usually happen out of hospital.97 In patients following cardiac arrest and ST-segment elevation on the ECG, primary PCI is the strategy of choice.98
Given the high prevalence of coronary occlusions and the potential difficulties in interpreting the ECG in patients after cardiac arrest, urgent angiography (within 2 h)2 should be considered in survivors of cardiac arrest, including unresponsive survivors, when there is a high index of suspicion of ongoing infarction (such as the presence of chest pain before arrest, a history of established CAD, and abnormal or uncertain ECG results).99
However, in patients without ST-segment elevation, a quick evaluation at the emergency department or intensive cardiac care unit (ICCU) to exclude non-coronary causes (cerebrovascular event, respiratory failure, non-cardiogenic shock, pulmonary embolism, and intoxication), and to perform urgent echocardiography, is reasonable. The decision to perform urgent coronary angiography and PCI if indicated should also take into account factors associated with poor neurological outcome. Unfavorable pre-hospital settings indicating a remote likelihood for neurological recovery [i.e., unwitnessed cardiac arrest, late arrival of a pre-hospital team without lay basic life support (>10 min), presence of an initial non-shockable rhythm, or more than 20 min of advanced life support without return to spontaneous circulation] should be taken strongly into consideration to argue against an invasive coronary strategy.100
Unconscious patients admitted to critical care units after out-of-hospital cardiac arrest are at high risk for death, and neurologic deficits are common among those who survive.101
Prevention and improved treatment of out-of-hospital cardiac arrest is crucial to reduce the mortality related to CAD.102
VI. SECONDARY PREVENTION AFTER STEMI
|
A. Pharmacotherapy: |
|
||
|
1. Anti-platelet therapy |
|
||
|
We recommend the indefinite use of aspirin in the dosage range of 75–162 mg/day for patients without contraindications after myocardial infarction. |
|
||
|
(Strong recommendation, high certainty evidence). |
|
||
|
We recommend the use clopidogrel (75 mg daily) in case of aspirin contraindication or intolerance as a single long-term therapy. |
|
||
|
(Conditional recommendation, high certainty evidence). |
|
||
|
We recommend that dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor (preferably ticagrelor) to be prescribed for up to 12 months in patients following acute myocardial infarction, irrespective of stent implantation unless there are contraindications such as excessive risk of bleeding. |
|
||
|
(Strong recommendation, high certainty evidence). |
|
||
|
2. ß-blockers: |
|
||
|
We recommend oral beta blockers to patients with heart failure and/or LVEF ≤40% unless contraindicated. |
|
||
|
(Strong recommendation, high certainty evidence). |
|
||
|
We recommend routine oral beta blockers to be considered to all patients without contraindications. |
|
||
|
(Conditional recommendation, moderate certainty evidence). |
|
||
|
3. Lipid Lowering Therapies: |
|||
|
We recommend an LDL-C goal of <55 mg/dl and a reduction of at least 50% of the baseline LDL-C. |
|||
|
(Strong recommendation, moderate-certainty evidence). |
|||
|
We recommend starting high-intensity statin therapy as early as possible, unless contraindicated, and maintain it for life. |
|||
|
(Strong recommendation, high-certainty evidence). |
|||
|
We recommend, in patients with LDL-C not at goal despite a maximally tolerated statin dose, combination with Ezetimibe and/or protein convertase subtilisin/kexin type 9 reducing drugs (PCSK9i or Inclisiran). |
|||
|
(Conditional recommendation, high-certainty evidence). |
|||
|
We recommend, for patients with statin intolerance, a reduced dose of statin therapy and/or ezetimibe. |
|||
|
(Strong recommendation, high-certainty evidence). |
|||
|
We recommend Bempedoic acid in patients with statin intolerance, either alone or in combination with ezetimibe, as it has new evidence for safety and efficacy |
|||
|
(Weak recommendation, moderate-certainty evidence). |
|||
|
4. Renin-angiotensin-aldosterone blockers: |
|
||
|
We recommend that ACE inhibitors should be used starting from the first 24 h of STEMI in patients with evidence of heart failure, LV systolic dysfunction, diabetes, or an anterior infarct. |
|
||
|
(Strong recommendation, high certainty evidence). |
|
||
|
We recommend that a n ARB, preferably valsartan, can be an alternative to ACE inhibitors in patients with heart failure and/or LV systolic dysfunction, particularly those who are intolerant of ACE inhibitors. |
|
||
|
(Strong recommendation, moderate certainty evidence). |
|
||
|
We recommend routine ACEI/ARBS to be considered to all patients without contraindications. |
|
||
|
(Conditional recommendation, moderate certainty evidence). |
|
||
|
5. Mineralocorticoid/aldosterone receptor antagonists: |
|
||
|
We recommend that MRAs should be used in patients with an LVEF ≤40% and heart failure or diabetes, who are already receiving an ACE inhibitor and a beta blocker, provided there is no renal failure or hyperkalemia. |
|
||
|
(Strong recommendation, moderate certainty evidence). |
|
||
|
6. Calcium antagonists: |
|
||
|
We recommend, in cases of hypertension, tachycardia or angina, that non-dihydropyridine CCBs may be used if ß blockers are contraindicated particularly in the presence of obstructive airway disease. |
|
||
|
(Conditional recommendation, moderate certainty evidence). |
|
||
|
7. Nitrates: |
|
||
|
We do not recommend the routine use of oral nitrates in STEMI which was of no benefit in a randomized controlled trial. |
|
||
|
(Conditional recommendation, moderate certainty evidence). |
|
||
|
8. SGLT2 inhibitors |
|
||
|
We recommend that SGLT2 inhibitors should be considered after STEMI especially if complicated with heart failure. |
|
||
|
(Weak recommendation, weak quality evidence) |
|
||
|
9. ARNI |
|
||
|
We recommend that ARNI, in place of ACE inhibitors or ARBS, should be considered after STEMI especially if complicated with heart failure. |
|
||
|
(Weak recommendation, weak quality evidence) |
|
||
|
B. LIFESTYLE MODIFICATIONS: |
|
We recommend that smoking should be discontinued by patients with a history of myocardial infarction. |
|
(Strong recommendation, high certainty evidence). |
|
We recommend that regular aerobic physical activity should be considered after myocardial infarction. |
|
(Strong recommendation, high certainty evidence). |
|
We recommend a healthy Mediterranean diet that controls blood pressure and BMI in the healthy range and avoiding alcohol. |
|
(Strong recommendation, moderate certainty evidence). |
|
C. CARDIAC REHABILITATION: |
|
We recommend that all patients after STEMI should be involved in a structured cardiac rehabilitation program. It includes exercise training, detecting and controlling risk factors, psychological counselling, guiding the patient to adopt healthy life style and be compliant to cardio protective medications. |
|
(Strong recommendation, high certainty evidence). |
|
We recommend that the patient should be counseled as to when to return back to work, sports, recreation and sexual activity while self monitoring biomedical indices. |
|
(Strong recommendation, moderate certainty evidence). |
Evidence and rationale:
Patients remain at high risk of recurrent ischemic events following a myocardial infarction. The goal of secondary prevention strategies is to reduce the risk of recurrent adverse cardiovascular events including left ventricular (LV) dysfunction and heart failure while reducing symptom burden including angina and exercise-induced ischemia and extending life expectancy.
The strategies encompass pharmacology (antiplatelets, ß-blockers, calcium channel blockers, renin angiotensin system blockers and lipid-lowering therapies), lifestyle modifications (smoking cessation, exercise, and diet) and cardiac rehabilitation (patient assessment, physical activity counselling, exercise training, risk factor control, patient education, psycho-social management, and vocational advice).
Aspirin inhibits thromboxane A2 of the cyclooxygenase pathway, preventing collagen−mediated platelet activation and aggregation. The combined use of aspirin and a P2Y12 inhibitor has an additive effect in inhibiting platelet activation, thereby reducing the risk of major adverse cardiovascular events in patients with STEMI.
It has also been shown in clinical trials that third generation P2Y12 inhibitors (ticagrelor and prasugrel) show additional benefit in terms of decreased ischemic events compared to clopidogrel with a slight increase in bleeding. However, the net outcomes are favorable for these drugs. In all the current guidelines, DAPT has typically been recommended for 12 months following myocardial infarction with ticagrelor and prasugrel generally preferred over clopidogrel. ß-blockers, such as carvedilol, bisoprolol, nebivolol and metoprolol improve cardiac output and left ventricular function while reducing peripheral vascular resistance, cardiovascular death, and infarct size.
Much of the evidence regarding beta-blockade in the post-MI setting is from trials set in the pre-reperfusion era. The evidence base for beta-blockers following MI is strongest in those patients with left ventricular ejection fraction (LVEF) ≤40% or heart failure, in whom they are strongly recommended5. In the absence of these co-morbidities, the long-term benefit (and optimal duration of therapy) is less certain. Statins inhibit the formation of atherosclerotic plaques by reducing the levels of LDL C, stabilize the lipid core and reduce inflammation in arterial wall. Therefore, statins are recommended in all patients with STEMI, irrespective of cholesterol concentration at presentation.
A meta-analysis of five RCTs comparing high- and low-intensity statin therapies concluded that the high-intensity statin therapy was more efficacious in risk reduction for cardiovascular death, non-fatal MI and ischemic stroke.
PCSK9i are recommended as a secondary treatment for lowering lipids. PCSK9i enhances the metabolism of LDL-C in the liver by inhibiting the PCSK9 protein. The FOURIER and ODYSSEY outcomes trials demonstrated that the addition of evolocumab or alirocumab to statin therapy in patients with a history of cardiovascular disease achieved a relative risk reduction of approximately 15% for the composite endpoint of cardiovascular death, MI, stroke, and coronary revascularization compared to a placebo administered with statin therapy.
ACEIs and ARBs offer cardio-protection after MI by limiting infarct size and ventricular remodeling. These agents confer survival benefits independent of other therapies used in the long-term management of high-risk STEMI patients.
Based on the results of HOPE and EUROPA trials, ACE inhibitor (ramipril, perindopril) for all STEMI patients with ejection fraction <40%, renal dysfunction, or diabetes regardless of ejection fraction should be given if no contraindication exists. The VALIANT trial results suggest that valsartan may be used as an alternative to an ACE inhibitor (in ACE inhibitor intolerant patients) for the long-term management of patients with left ventricular dysfunction after STEMI. Aldosterone blockade reduces post-MI ventricular remodeling in patients with left ventricular systolic dysfunction and affects several pathophysiological pathways considered to play a role in the prognosis of patients following myocardial infarction.
Aldosterone blockade reduces post-MI ventricular remodeling in patients with left ventricular systolic dysfunction and affects several pathophysiological pathways considered to play a role in the prognosis of patients following myocardial infarction and have been shown to reduce all-cause mortality and readmission for worsening heart failure when commenced following an acute MI in patients who also have LVEF ≤40% and either heart failure or Diabetes.
The EPHESUS trial demonstrated that treatment with eplerenone 3-14 days after an acute MI significantly reduced mortality and the rate of hospitalization for heart failure.
calcium antagonists early in the course of STEMI showed no beneficial effect on death or reinfarction, with a trend of higher mortality for patients treated with nifedipine.
A meta-analysis of 17 trials involving calcium antagonists early in the course of STEMI showed no beneficial effect on death or re-infarction, with a trend of higher mortality for patients treated with nifedipine. Therefore, routine use of calcium antagonists in the acute phase is not indicated.
The routine use of nitrates in STEMI was of no benefit in a randomized controlled trial against placebo and is therefore not recommended.
In the DAPA-HF and EMPERORR reduced trials, treatment with a SGLT2 inhibitor – respectively dapagliflozin and empagliflozin – was associated with a lower risk of CV death or admission for worsening heart failure.
Sacubitril/valsartan was superior to ramipril among high-risk survivors of acute myocardial infarction (MI), according to a new post hoc win-ratio analysis of the PARADISE-MI randomized trial, even though the trial’s primary results showed no difference between the medications in cardiovascular death or incident heart failure.
Key life control interventions include cessation of smoking, optimal blood pressure control, diet advice and weight control, and encouraging physical activity. Detailed recommendations are available from the ESC Guidelines on prevention.
The prognostic benefits of Cardiac rehabilitation extend beyond the first year. At five years, patients attending the Cardiac rehabilitation program had lower total and cardiovascular mortality as well as lower hospitalization rates than non-attenders. The GOSPEL trial, a multi factorial, continued reinforced intervention up to 3 years after rehabilitation following AMI, effectively decrease the risk of nonfatal AMI, and a better prescription of drugs for secondary prevention was seen in the intervention group.103
- ACKNOWLEDGEMENTS
|
Prof. Dr. Magdy Abdelhamid Prof. Dr. Sameh Shaheen Prof. Dr. Ahmed Magdy Prof. Dr. Mohamed Sleem Prof. Dr. Hazem Khamis
Prof. Dr. Karim Said Prof. Dr. Hamza Kabil Prof.
Dr. Reda Bayoumy |
Dr. Mohamed Moustafa
Dr. Tamer El Wasify
Dr. Moustafa Khalifa
Dr. Mohamed Hamza Kabil
We would Like to thank Dr. Amr Youssef for his help in checking the document during the final process of editing.
- ACRONYMS AND ABBREVIATIONS
|
ACE |
Angiotensin Converting Enzyme |
|
ACS |
Acute Coronary Syndrome |
|
AF |
Atrial Fibrillation |
|
AMI |
Acute Myocardial Infarction |
|
ARBS |
Angiotensinogen Receptor Blockers |
|
ARNI |
Angiotensin Receptor/Neprilysin Inhibitor |
|
AV BLOCK |
Atrio Ventricular Block |
|
b.i.d |
Bid In Die (Twice Daily) |
|
BP |
Blood Pressure |
|
C/I |
Contraindicated |
|
CABG |
Coronary Artery Bypass Graft |
|
CAD |
Coronary Artery Disease |
|
CCBs |
Calcium Channel Blockers |
|
CCU/ICU |
Coronary Care Unit/ Intensive Care Unit |
|
CMR |
Cardiac Magnetic Resonance |
|
CSK9i |
Protein Convertase Subtilisin/Kexin Type 9 |
|
D2B |
Door To Balloon |
|
DAPT |
Dual Antiplatelet Therapy |
|
DES |
Drug Eluting Stent |
|
ECG |
Electrocardiogram |
|
ECLS |
Extra Corporeal Life Support |
|
ECMO |
Extra Corporeal Membrane Oxygenator |
|
eGFR |
Estimated Glomerular Filtration Rate |
|
EMS |
Emergency Medical System |
|
ER |
Emergency Room |
|
ESC |
European Society of Cardiology |
|
FMC |
First Medical Contact |
|
GP |
Glycoprotein |
|
GPI |
Glycoprotein Inhibitor |
|
HF |
Heart Failure |
|
hsTn |
High Sensitivity Troponin |
|
I.V. |
Intra Venous |
|
IABP |
Intra-Aortic Balloon Pump |
|
IC |
Intra Coronary |
|
ICCU |
Intensive Coronary Care Unit |
|
ICD |
Internal Cardioverter Defibrillator |
|
IRA |
Infarct Related Artery |
|
LBBB |
Left Bundle Branch Block |
|
LDL-C |
Low Density Lipoprotein Cholesterol |
|
LV |
Left Ventricle |
|
LVADs |
Left Ventricular Assist Devices |
|
LVEF |
Left Ventricular Ejection Fraction |
|
MI |
Myocardial Infarction |
|
MRA |
Mineralocorticoid Receptor Antagonist |
|
PCI |
Percutaneous Coronary Intervention |
|
PET |
Positron Emission Tomography |
|
RCTs |
Randomized Controlled Trials |
|
RV |
Right Ventricular |
|
SaO2 |
Saturation of arterial Oxygen |
|
SBP |
Systolic Blood Pressure |
|
SGLT2 |
Sodium-Glucose Co-Transporter-2 |
|
SPECT |
Single Positron Emission Computed Tomography |
|
STEMI |
ST-Elevation Myocardial Infarction |
|
T2DM |
Type 2 Diabetes Mellitus |
|
TNK-tPA |
Tenecteplase Tissue Plasminogen Activator |
|
UFH |
Unfractionated Heparin |
|
VF |
Ventricular Fibrillation |
|
VT |
Ventricular Tachycardia |
- GLOSSARY
|
TERM |
DEFINITION |
|
First medical contact (FMC) |
Time of EMS arrival at scene (prehospital) or hospital registration (walk-in) |
|
Time of STEMI diagnosis |
Time of performance and interpretation of first ECG diagnostic of STEMI |
|
First device deployment |
Deployment of first PCI device (balloon or first stent) |
|
Door in Door out (DIDO) |
Time between registration of patient at non PCI capable hospital and patient leaving non-PCI capable hospital via EMS |
|
Interfacility transport time |
Time on the road between leaving non-PCI capable hospital and arrival at PCI capable hospital |
|
Primary percutaneous coronary intervention (PPCI) |
Mechanical reperfusion techniques aimed at restoring flow to the culprit vessel in acute STEMI. May include balloon angioplasty, coronary stenting or thrombectomy |
|
Pharmacoinvasive strategy |
A reperfusion strategy utilizing adjunctive PCI following initial pharmacological reperfusion with fibrinolysis. Consists of 1. routine immediate transfer to PCI centres after fibrinolysis, 2. immediate PCI for patients with failed fibrinolysis, and 3. routine angiography +/- PCI within 24 hours after successful fibrinolysis |
|
Facilitated PCI |
A reperfusion strategy where adjuvant therapies such as fibrinolysis or glycoprotein IIb/IIIa inhibitors are administered while in transit to immediate diagnostic angiography with the intent to perform immediate PPCI |
- INTRODUCTION
Acute ST-segment elevation myocardial infarction (STEMI) is the most serious manifestation of coronary artery disease (CAD) with high morbidity and mortality.1 Mortality due to CVD in Egypt is one of the highest compared to other countries in the region and worldwide.2 Outcome of STEMI patients depends on the availability of emergency medical services provided by STEMI networks and on the time delay before which a patient is treated.3
- SCOPE AND OBJECTIVES
The objectives of these guidelines are to provide a practical set of recommendations to the timely diagnosis and up-to-date management of patients presenting with STEMI in Egypt. The goal of these guidelines is to improve survival and quality of life for patients who suffer from STEMI. The guidelines will cover both the early and longer-term (rehabilitation) phases of STEMI.
- TARGET AUDIENCE
The guidelines are directed to Cardiologists, Emergency physicians, Internal medicine physicians, Critical care physicians, Interns, Nurses, administrators and planners dealing with patients presenting with STEMI.
- Methods
Methods of search:
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation. Keywords used for searching are: myocardial infarction, STEMI.
Inclusion / exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on methodology of development including the systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated 2013 and later or the last 5 years)
• Selecting peer-reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author
The following three categories of databases and websites were searched:
CPG databases and libraries (e.g., GIN, ECRI, SIGN, DynaMed, BIGG-REC PAHO)
Bibliographic databases (e.g., PubMed, Google Scholar)
Specialized professional societies (related to the pediatric subspecialty)
All the retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least two members. The panel decided a cut-off point or rank the guidelines (any guideline scoring above 60% on the rigor dimension was retained)
After reviewing all the previous criteria, the GDG/ GAG recommended using 2 guidelines:
2023 ESC Guidelines for the management of acute coronary syndromes - ESC Clinical Practice Guidelines.
2019 Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology Guidelines on the Acute Management of ST-Elevation Myocardial Infarction: Focused Update on Regionalization and Reperfusion
We did Adolopment for these guidelines: (Adoption, Adaptation, and Development)
Adoption for most of the guideline recommendations.
Adaptation for 2 recommendation according to GRADE criteria to be suitable to our Economic implications (Evidence to Decision (EtD) table was done)
Development of Good Practice Statement.
Contributors to the guideline development process:
Guideline Development Group (GDG)/ Guideline Adaptation Group (GAG):
The GDG/ GAG included two subgroups; the clinicians/ healthcare providers subgroup and the guideline methodologists’ subgroup.
Clinicians Subgroups
The clinicians’ subgroup or clinical panel for this guideline included experts with a range of knowledge, technical skills and diverse perspectives in the field of myocardial ischemia
The main functions of the clinical panel were adolopment of STEMI diagnosis and management Guidelines, determining the scope of the guideline and guideline, reviewing the evidence, and formulating evidence-informed recommendations in case of changing strength of recommendations.
Guideline Methodologists Subgroup
There were 7 guideline methodologists with expertise in guidelines development, adaptation, GRADE and translation of evidence into recommendations. Methodologists provided orientation and overview of evidence-informed guideline development processes using the GRADE approach, guideline adaptation using the Adapted ADAPTE, provided AGREE II assessment of the source guidelines in collaboration with the clinician’s subgroup, generation of the EtD frameworks whenever applicable.
External Review Group:
The External Review Group for this guideline comprises 3 clinical national experts who have interest and expertise in as well as eminent international reviewers.
They were identified by Egyptian Society of Cardiology (EgSC) as people who can provide valuable insights during the guideline development process.
The External Review Group was asked to comment on (peer review) the final guideline to identify any criticism on the content and to comment on clarity and applicability as well as issues relating to implementation, dissemination, ethics, regulations, or monitoring, but not to change the recommendations formulated by the GDG/ GAG. The members of the External Review Group were required to submit declarations of interest before the peer review process.
Guideline Development/ Adaptation Group meetings:
GDG/ GAG meetings were organized virtually (weekly/bimonthly). Due to the extensive scope of
the guideline, EPG was responsible for overseeing the adolopment process. the timetable and objectives of each meeting. GDG/ GAG meetings were also attended by members of the methodologists. Working rules for each contributor type were outlined by the chair at the start of each meeting, covering aspects such as vocal rights, voting, and evidence to decision and recommendation formulating processes.
Declarations of interest:
Prospective members of the GDG/ GAG were asked to fill in and sign the standard WHO declaration of interest and confidentiality undertaking forms. All guideline members and methodologists were also asked to fill in and sign the standard WHO declaration-of-interests.
Members of the external review group will be asked to fill in and sign the standard WHO declaration-of-interests form before the peer review process.
Evidence for the guideline:
We used GRADE system (Grading of Recommendations, Assessment, Development, and Evaluations) which is a transparent framework for developing and presenting summaries of evidence and provides a systematic approach for making clinical practice recommendations. It is the most widely adopted tool for grading the quality of evidence and for making recommendations with over 100 organizations worldwide officially endorsing GRADE.
GRADE has four levels of evidence – also known as certainty in evidence or quality of evidence: very low, low, moderate, and high (Table 1). Evidence from randomized controlled trials starts at high quality and, because of residual confounding, evidence that includes observational data starts at low quality.
|
Table 1. GRADE certainty ratings |
|
|
Certainty |
What it means |
|
Very low |
The true effect is probably markedly different from the estimated effect |
|
Low |
The true effect might be markedly different from the estimated effect |
|
Moderate |
The authors believe that the true effect is probably close to the estimated effect |
|
High |
The authors have a lot of confidence that the true effect is similar to the estimated effect. |
In GRADE, recommendations can be strong or weak, in favor or against an intervention. Strong recommendations suggest that all or almost all persons would choose that intervention. Weak recommendations imply that there is likely to be an important variation in the decision that informed people are likely to make. The strength of recommendations is actionable: a weak recommendation indicates that engaging in a shared decision-making process is essential, while a strong recommendation suggests that it is not usually necessary to present both options.
Recommendations are more likely to be weak rather than strong when the certainty in evidence is low, when there is a close balance between desirable and undesirable consequences, when there is substantial variation or uncertainty in patient values and preferences, and when interventions require considerable resources.
- CLINICAL AND QUALITY INDICATORS FOR MONITORING
|
Domain 1: Centre organization |
|
1. The center should be part of a network organization with written protocols for rapid and efficient management |
|
2. Pre-hospital interpretation of ECG for: 1) diagnosis, 2) decision for immediate transfer to a center with catheterization laboratory facilities, and 3) pre-hospital activation of the catheterization laboratory |
|
3. The center should participate in a regular registry or program for quality assessment |
|
4. Routine assessment of relevant times for the reperfusion process in STEMI patients (i.e., times from ‘call to first medical contact’, ‘first medical contact to arrival at PCI center, arrival at PCI center to arterial access) |
|
Domain 2 : Reperfusion/Invasive strategy |
|
5. Proportion of patients with STEMI reperfused among those eligible (onset of symptoms to diagnosis <12 h). |
|
6. Proportion of patients with STEMI who receive timely reperfusion. Timely is defined as: 1) For patients presenting at primary PCI hospitals: <60 min from initial STEMI diagnosis to infarct-related artery wire crossing 2) For patients diagnosed either in a non-PCI hospital or in the out-of-hospital setting and then transferred to a PCI capable center: <90 min from initial STEMI diagnosis to infarct-related artery wire crossing 3) For patients treated with fibrinolysis, initiation of fibrinolysis within 10 minutes after STEMI diagnosis |
|
7. Use of radial access in case of invasive Strategy |
|
8. The time between the initial STEMI diagnosis and arterial access (absolute value) for primary PCI. |
|
Domain 3: In-hospital risk assessment |
|
9. The proportion of patients who have an assessment of LVEF before hospital discharge (LVEF should be assessed and the numerical value recorded for all patients). |
|
10. LDL-Cholesterol assessment should be performed during hospitalization |
|
11. Ischemic and hemorrhagic risk assessment should be performed using a validated risk score. |
|
Domain 4: Anti-thrombotic treatment during hospitalization |
|
12. Proportion of patients with “adequate P2Y12 inhibition” defined as: (number of patients discharged with prasugrel, ticagrelor, or clopidogrel)/(patients eligible). Eligible is defined as follows: 13. For ticagrelor: AMI patients without previous hemorrhagic stroke, high bleeding risk, fibrinolysis or oral anticoagulation. 14. For prasugrel: PCI-treated AMI patients without previous hemorrhagic or ischaemic stroke, high bleeding risk (patients ≥75 years and/or <60 kg body weight is also considered as high bleeding risk features), fibrinolysis or oral anticoagulation. 15. For clopidogrel: no indication for prasugrel or ticagrelor and no high bleeding risk. |
|
16. Patients discharged on dual antiplatelet Therapy |
|
17. Mention the duration of the dual antiplatelet therapy in the discharge letter |
|
Domain 5 : Secondary prevention discharge treatments |
|
18. Proportion of patients discharged from hospital on high intensity statins (defined as atorvastatin ≥40 mg or rosuvastatin ≥20 mg) unless contraindicated |
|
19. Proportion of patients with LVEF <40% who are discharged from hospital on ACEI (or ARBs if intolerant of ACEI). |
|
20. Proportion of patients with LVEF <40% who are discharged from hospital on betablockers |
|
Domain 6: Patient satisfaction |
|
21. Feedback regarding the patient’s experience systematically collected in an organized way from all patients. It should include the following points: · Recommendation to attend an educational program (rehabilitation, smoking cessation, weight control and diet counselling). · Explanations provided by doctors and nurses (about the coronary disease, the benefit/risk of the discharge treatment, and medical follow-up). · Discharge information regarding what to do in case of recurrence of symptoms and timing of visit. · Pain control. |
|
22. Systematic assessment of health-related quality of life in all patients using a validated instrument. |
|
23. The discharge letter should be sent to the Patient |
|
Domain 7: Outcomes |
|
24. Risk adjusted 30-day mortality rate |
- Gap of evidence and future research
Major advances in the management of patients with STEMI have occurred over the last decade yet lack of evidence still prevails in some areas of STEMI spectrum. The following is a list of selected topics that need to be addressed in future research.
(1) Definition and epidemiology
Further research into the underlying characteristics, pathophysiology, and diagnosis of STEMI patients without traditional risk factors.
(2) Diagnosis
Role of AI in facilitating correct diagnosis of STEMI.
(3) Pharmacotherapy of STEMI
i. Pragmatic studies on rapid sequencing of disease-modifying drugs for prevention of STEMI.
ii. Specific therapies for coronary ectasia or slow flow coronary artery disease.
iii. Further evidence from prospective RCTs for the treatment of specific STEMI patients, those with ectasia and slow flow.
(4) Devices and interventions
ii. More research on intervention in delayed patients’ presentation.
iii. RCTs on microvascular coronary artery disease.
(5) Self-management
The role of remote monitoring via smart phone applications in STEMI patients.
- Implementation of the guidelines
1- Health education about common risk factors, symptoms, and preventive measures of STEMI through social media and television national campaigns.
2-Strict regulatory measures for food industries about nutritional food content, especially salt and fat content.
3- Health insurance coverage of STEMI GDMT including novel agents e.g., SGLT2-i.
4- Government and parliament actions for legalization and regulation of STEMI treatment drugs support programs.
5-Scientefic meeting and webinars directed for GP and internal medicine physicians to increase awareness about STEMI diagnosis.
Update of the guidelines
This guideline will be updated when there is new evidence.
- Figures
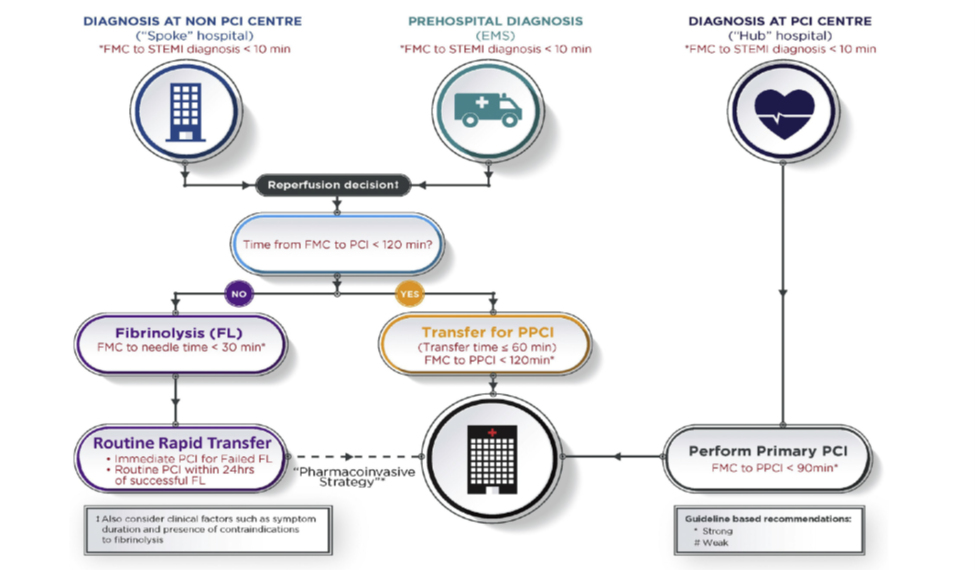
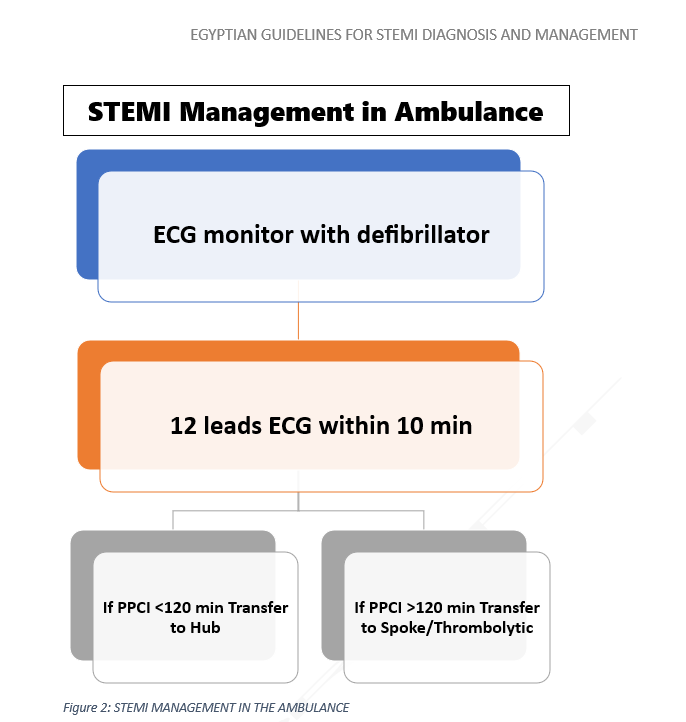
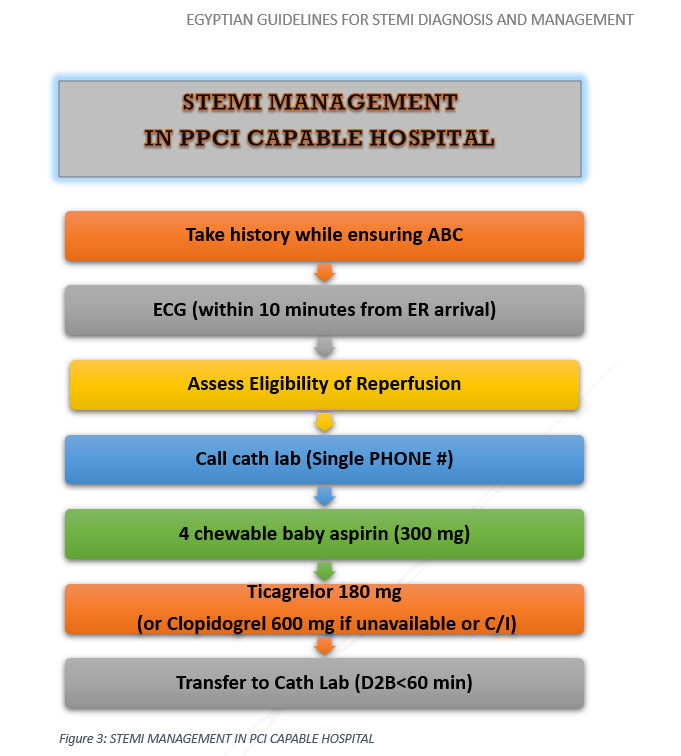
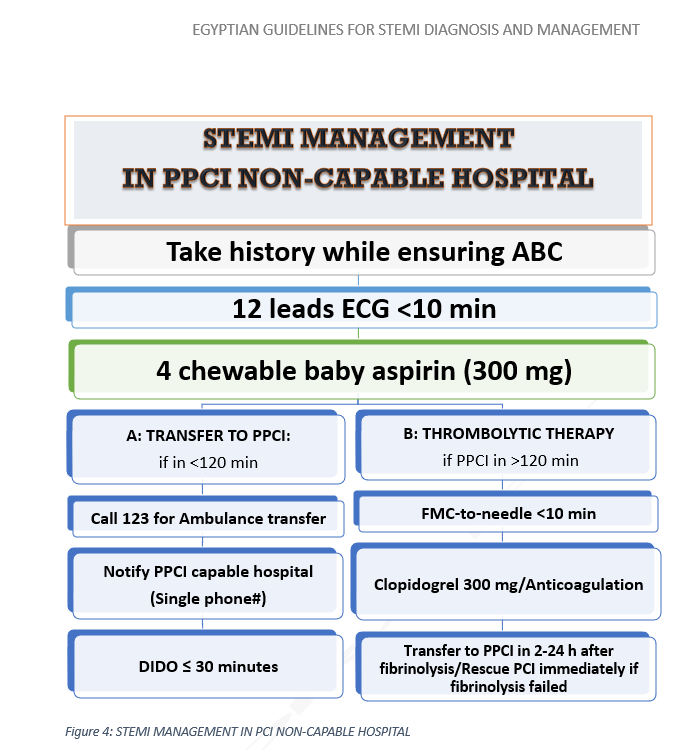
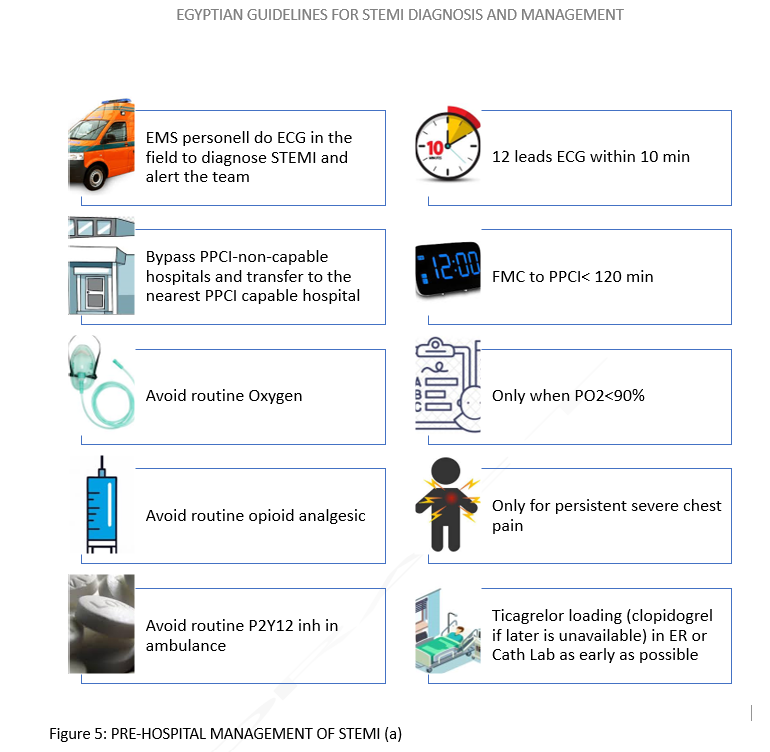
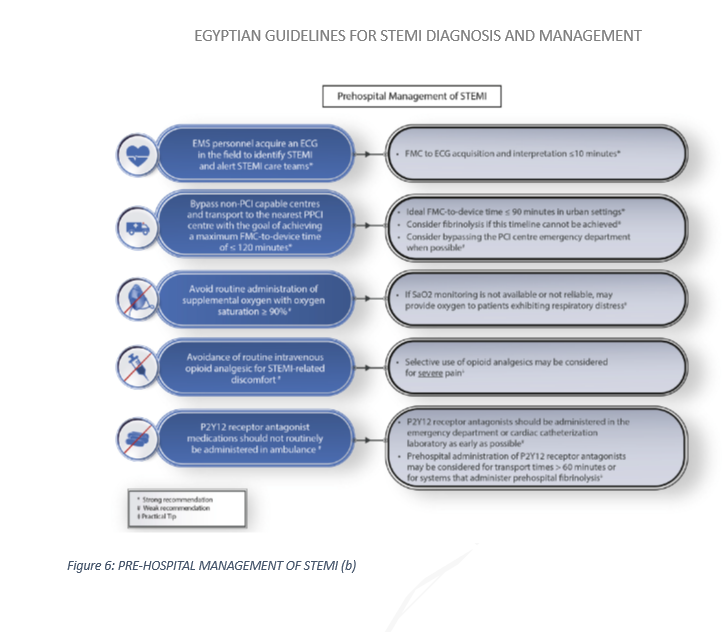
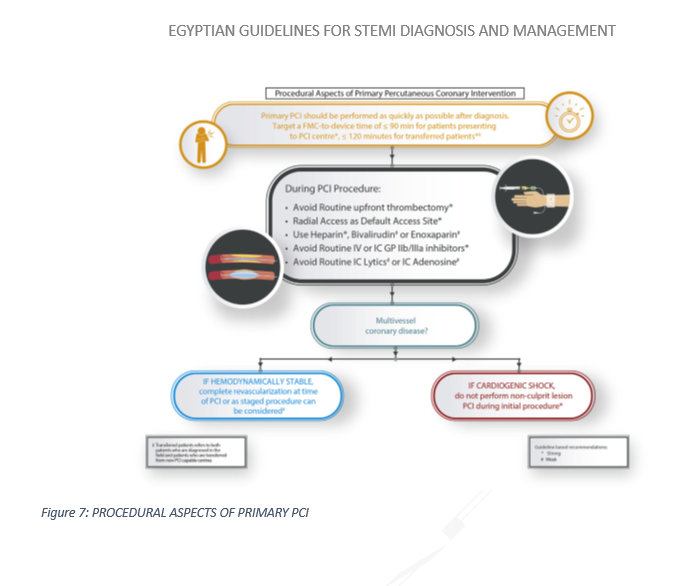
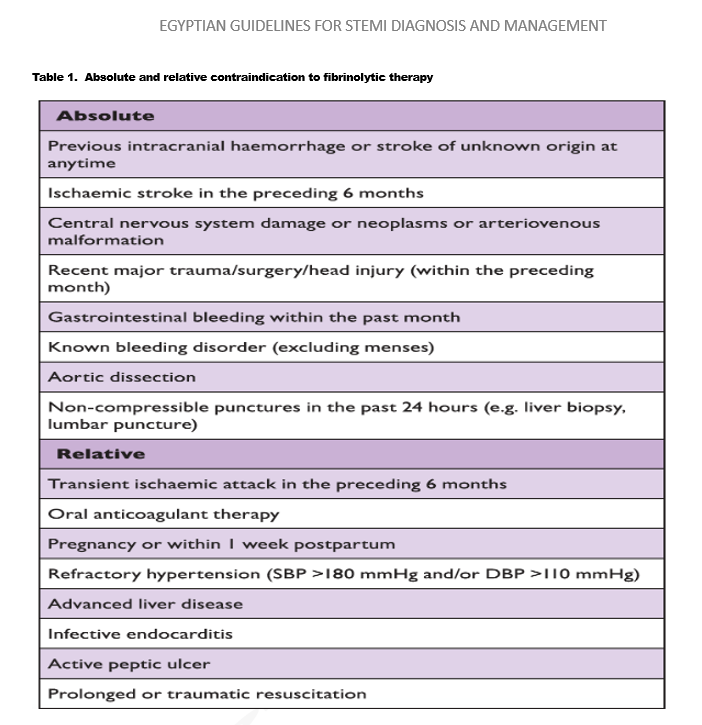
- ANNEXES
List of contributors
|
Name |
Affiliations |
Contribution |
|
1. DR SAMEH SHAHEEN |
Ain Shams University |
Writing and reviewing: STEMI SYSTEMS OF CARE PRE-HOSPITAL MANAGEMENT MANAGEMENT IN PCI CAPABLE HOSPITAL/ PPCI and ADJUNCTIVE THERAPY STEMI MANAGEMENT IN CCU AFTER REPERFUSION SPECIAL STEMI PATIENTS AND COMPLICATIONS |
|
2. DR MOHAMAD SLEEM |
National Heart Institute |
Writing and reviewing: PRE-HOSPITAL MANAGEMENT |
|
3. DR AHMED AL-HABBAA |
Al-Azhar University, Cairo, Egypt |
Writing and reviewing: STEMI SYSTEMS OF CARE SPECIAL STEMI PATIENTS AND COMPLICATIONS |
|
4. DR AHMAD ABDELAZIZ |
National Heart Institute |
Writing and reviewing: MANAGEMENT IN PCI NON-CAPABLE HOSPITAL; FIBRINOLYSIS AND PHARMACOINVASIVE STRATEGY |
|
5. DR MOHAMAD MOSTAFA |
Police Hospital |
Writing and reviewing: PRE-HOSPITAL MANAGEMENT SECONDARY PREVENTION AFTER STEMI |
|
6. DR AHMAD MAGDY |
National Heart Institute |
Reviewing |
|
7. DR HAMZA KABIL |
Damietta University |
Reviewing |
|
8. DR AYMAN KHAIRY |
Assiut University |
Reviewing |
|
9. DR MOHAMAD KABIL |
Suez University |
Reviewing |
- REFERENCES
- Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, Falk V, Filippatos G, Hamm C, Head SJ, Juni P, Kappetein AP, Kastrati A, Knuuti J, Landmesser U, Laufer G, Neumann FJ, Richter DJ, Schauerte P, Sousa Uva M, Stefanini GG, Taggart DP, Torracca L, Valgimigli M, Wijns W, Witkowski A. 2014 ESC/ EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2014;35(37):2541–2619.
- Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, Gencer B, Hasenfuss G, Kjeldsen K, Lancellotti P, Landmesser U, Mehilli J, Mukherjee D, Storey RF, Windecker S, Baumgartner H, Gaemperli O, Achenbach S, Agewall S, Badimon L, Baigent C, Bueno H, Bugiardini R, Carerj S, Casselman F, Cuisset T, Erol C, Fitzsimons D, Halle M, Hamm C, Hildick-Smith D, Huber K, Iliodromitis E, James S, Lewis BS, Lip GY, Piepoli MF, Richter D, Rosemann T, Sechtem U, Steg PG, Vrints C, Luis Zamorano J. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2016;37(3):267–315.
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney MT, Corra U, Cosyns B, Deaton C, Graham I, Hall MS, Hobbs FD, Lochen ML, Lollgen H, Marques-Vidal P, Perk J, Prescott E, Redon J, Richter DJ, Sattar N, Smulders Y, Tiberi M, van der Worp HB, van Dis I, Verschuren WM. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016;37(29):2315–2381.
- Tubaro M, Danchin N, Goldstein P, Filippatos G, Hasin Y, Heras M, Jansky P, Norekval TM, Swahn E, Thygesen K, Vrints C, Zahger D, Arntz HR, Bellou A, De La Coussaye JE, De Luca L, Huber K, Lambert Y, Lettino M, Lindahl B, McLean S, Nibbe L, Peacock WF, Price S, Quinn T, Spaulding C, Tatu-Chitoiu G, Van De Werf F. Pre-hospital treatment of STEMI patients. A scientific statement of the Working Group Acute Cardiac Care of the European Society of Cardiology. Acute Card Care 2011;13(2):56–67.
- Rokos IC, French WJ, Koenig WJ, Stratton SJ, Nighswonger B, Strunk B, Jewell J, Mahmud E, Dunford JV, Hokanson J, Smith SW, Baran KW, Swor R, Berman A, Wilson BH, Aluko AO, Gross BW, Rostykus PS, Salvucci A, Dev V, McNally B, Manoukian SV, King SB, 3rd. Integration of pre-hospital electrocardiograms and ST-elevation myocardial infarction receiving center (SRC) networks: impact on door-to-balloon times across 10 independent regions. JACC Cardiovasc Interv 2009;2(4):339–346.
- Brieger D, Eagle KA, Goodman SG, Steg PG, Budaj A, White K, Montalescot G. Acute coronary syndromes without chest pain, an underdiagnosed and undertreated high-risk group: insights from the Global Registry of Acute Coronary Events. Chest 2004;126(2):461–469.
- Kaul P, Armstrong PW, Sookram S, Leung BK, Brass N, Welsh RC. Temporal trends in patient and treatment delay among men and women presenting with ST-elevation myocardial infarction. Am Heart J 2011;161(1):91–97.
- Diercks DB, Owen KP, Kontos MC, Blomkalns A, Chen AY, Miller C, Wiviott S, Peterson ED. Gender differences in time to presentation for myocardial infarction before and after a national women’s cardiovascular awareness campaign: a temporal analysis from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early Implementation (CRUSADE) and the National Cardiovascular Data Registry Acute Coronary Treatment and Intervention Outcomes Network-Get with the Guidelines (NCDR ACTION Registry-GWTG). Am Heart J 2010;160(1):80–87.e3.
- Kang SH, Suh JW, Yoon CH, Cho MC, Kim YJ, Chae SC, Yoon JH, Gwon HC, Han KR, Kim JH, Ahn YK, Jeong MH, Kim HS, Choi DJ, KAMIR/KorMI Registry. Sex differences in management and mortality of patients with ST-elevation myocardial infarction (from the Korean Acute Myocardial Infarction National Registry). Am J Cardiol 2012;109(6):787–793.
- Kyto V, Sipila J, Rautava P. Gender and in-hospital mortality of ST-segment elevation myocardial infarction (from a multihospital nationwide registry study of 31,689 patients). Am J Cardiol 2015;115(3):303–306.
- Hvelplund A, Galatius S, Madsen M, Rasmussen JN, Rasmussen S, Madsen JK, Sand NP, Tilsted HH, Thayssen P, Sindby E, Hojbjerg S, Abildstrom SZ. Women with acute coronary syndrome are less invasively examined and subsequently less treated than men. Eur Heart J 2010;31(6):684–690.
- Nguyen JT, Berger AK, Duval S, Luepker RV. Gender disparity in cardiac procedures and medication use for acute myocardial infarction. Am Heart J 2008;155(5):862–868.
- de Torbal A, Boersma E, Kors JA, van Herpen G, Deckers JW, van der Kuip DA, Stricker BH, Hofman A, Witteman JC. Incidence of recognized and unrecognized myocardial infarction in men and women aged 55 and older: the Rotterdam Study. Eur Heart J 2006;27(6):729–736.
- Henrikson CA, Howell EE, Bush DE, Miles JS, Meininger GR, Friedlander T, Bushnell AC, Chandra-Strobos N. Chest pain relief by nitroglycerin does not predict active coronary artery disease. Ann Intern Med 2003;139(12):979–986.
- Diercks DB, Peacock WF, Hiestand BC, Chen AY, Pollack CV, Jr, Kirk JD, Smith SC, Jr, Gibler WB, Ohman EM, Blomkalns AL, Newby LK, Hochman JS, Peterson ED, Roe MT. Frequency and consequences of recording an electrocardiogram >10 minutes after arrival in an emergency room in non-ST-segment elevation acute coronary syndromes (from the CRUSADE Initiative). Am J Cardiol 2006;97(4):437–442.
- Tubaro M, Danchin N, Goldstein P, Filippatos G, Hasin Y, Heras M, Jansky P, Norekval TM, Swahn E, Thygesen K, Vrints C, Zahger D, Arntz HR, Bellou A, De La Coussaye JE, De Luca L, Huber K, Lambert Y, Lettino M, Lindahl B, McLean S, Nibbe L, Peacock WF, Price S, Quinn T, Spaulding C, Tatu-Chitoiu G, Van De Werf F. Pre-hospital treatment of STEMI patients. A scientific statement of the Working Group Acute Cardiac Care of the European Society of Cardiology. Acute Card Care 2011;13(2):56–67.
- Rokos IC, French WJ, Koenig WJ, Stratton SJ, Nighswonger B, Strunk B, Jewell J, Mahmud E, Dunford JV, Hokanson J, Smith SW, Baran KW, Swor R, Berman A, Wilson BH, Aluko AO, Gross BW, Rostykus PS, Salvucci A, Dev V, McNally B, Manoukian SV, King SB, 3rd. Integration of pre-hospital electrocardiograms and ST-elevation myocardial infarction receiving center (SRC) networks: impact on door-to-balloon times across 10 independent regions. JACC Cardiovasc Interv 2009;2(4):339–346.
- Quinn T, Johnsen S, Gale CP, Snooks H, McLean S, Woollard M, Weston C. Effects of prehospital 12-lead ECG on processes of care and mortality in acute coronary syndrome: a linked cohort study from the Myocardial Ischaemia National Audit Project. Heart 2014;100(12):944–950.
- Sorensen JT, Terkelsen CJ, Norgaard BL, Trautner S, Hansen TM, Botker HE, Lassen JF, Andersen HR. Urban and rural implementation of pre-hospital diagnosis and direct referral for primary percutaneous coronary intervention in patients with acute ST-elevation myocardial infarction. Eur Heart J 2011;32(4):430–436.
- Chan AW, Kornder J, Elliott H, Brown RI, Dorval JF, Charania J, Zhang R, Ding L, Lalani A, Kuritzky RA, Simkus GJ. Improved survival associated with prehospital triage strategy in a large regional ST-segment elevation myocardial infarction program. JACC Cardiovasc Interv 2012;5(12):1239–46.
- Dhruva VN, Abdelhadi SI, Anis A, Gluckman W, Hom D, Dougan W, Kaluski E, Haider B, Klapholz M. ST-Segment Analysis Using Wireless Technology in Acute Myocardial Infarction (STAT-MI) trial. J Am Coll Cardiol 2007;50(6):509–513.
- Lopez-Sendon J, Coma-Canella I, Alcasena S, Seoane J, Gamallo C. Electrocardiographic findings in acute right ventricular infarction: sensitivity and specificity of electrocardiographic alterations in right precordial leads V4R, V3R, V1, V2, and V3. J Am Coll Cardiol 1985;6(6):1273–1279.
- O’Doherty M, Tayler DI, Quinn E, Vincent R, Chamberlain DA. Five hundred patients with myocardial infarction monitored within one hour of symptoms. BMJ (Clin Res Ed) 1983;286(6375):1405–1408.
- Mehta RH, Starr AZ, Lopes RD, Hochman JS, Widimsky P, Pieper KS, Armstrong PW, Granger CB. Incidence of and outcomes associated with ventricular tachycardia or fibrillation in patients undergoing primary percutaneous coronary intervention. JAMA 2009;301(17):1779–1789.
- Rokos IC, Farkouh ME, Reiffel J, Dressler O, Mehran R, Stone GW. Correlation between index electrocardiographic patterns and pre-intervention angiographic findings: insights from the HORIZONS-AMI trial. Catheter Cardiovasc Interv 2012;79(7):1092–1098.
- Stribling WK, Kontos MC, Abbate A, Cooke R, Vetrovec GW, Dai D, Honeycutt E, Wang TY, Lotun K. Left circumflex occlusion in acute myocardial infarction (from the National Cardiovascular Data Registry). Am J Cardiol 2011;108(7):959–963.
- Dixon WC, 4th, Wang TY, Dai D, Shunk KA, Peterson ED, Roe MT. Anatomic distribution of the culprit lesion in patients with non-ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention: findings from the National Cardiovascular Data Registry. J Am Coll Cardiol 2008;52(16):1347–1348.
- Pedersen F, Butrymovich V, Kelbaek H, Wachtell K, Helqvist S, Kastrup J, Holmvang L, Clemmensen P, Engstrom T, Grande P, Saunamaki K, Jorgensen E. Short- and long-term cause of death in patients treated with primary PCI for STEMI. J Am Coll Cardiol 2014;64(20):2101–2108.
- Fokkema ML, James SK, Albertsson P, Akerblom A, Calais F, Eriksson P, Jensen J, Nilsson T, de Smet BJ, Sjogren I, Thorvinger B, Lagerqvist B. Population trends in percutaneous coronary intervention: 20-year results from the SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J Am Coll Cardiol 2013;61(12):1222–1230.
- EUGenMed Cardiovascular Clinical Study Group, Regitz-Zagrosek V, OerteltPrigione S, Prescott E, Franconi F, Gerdts E, Foryst-Ludwig A, Maas AH, Kautzky-Willer A, Knappe-Wegner D, Kintscher U, Ladwig KH, SchenckGustafsson K, Stangl V. Gender in cardiovascular diseases: impact on clinical manifestations, management, and outcomes. Eur Heart J 2016;37(1):24–34.
- Priori SG, Blomstrom-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernandez-Madrid A, Nikolaou N, Norekval TM, Spaulding C, Van Veldhuisen DJ. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 2015;36(41):2793–2867.
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, Writing Group on the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction, Thygesen K, Alpert JS, White HD, Jaffe AS, Katus HA, Apple FS, Lindahl B, Morrow DA, Chaitman BA, Clemmensen PM, Johanson P, Hod H, Underwood R, Bax JJ, Bonow RO, Pinto F, Gibbons RJ, Fox KA, Atar D, Newby LK, Galvani M, Hamm CW, Uretsky BF, Steg PG, Wijns W, Bassand JP, Menasche P, Ravkilde J, Ohman EM, Antman EM, Wallentin LC, Armstrong PW, Simoons ML, Januzzi JL, Nieminen MS, Gheorghiade M, Filippatos G, Luepker RV, Fortmann SP, Rosamond WD, Levy D, Wood D, Smith SC, Hu D, Lopez-Sendon JL, Robertson RM, Weaver D, Tendera M, Bove AA, Parkhomenko AN, Vasilieva EJ, Mendis S, ESC Committee for Practice Guidelines. Third universal definition of myocardial infarction. Eur Heart J 2012;33(20):2551–2567.
- Gehrie ER, Reynolds HR, Chen AY, Neelon BH, Roe MT, Gibler WB, Ohman EM, Newby LK, Peterson ED, Hochman JS. Characterization and outcomes of women and men with non-ST-segment elevation myocardial infarction and non-obstructive coronary artery disease: results from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) quality improvement initiative. Am Heart J 2009;158(4):688–694.
- Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation 2015;131(10):861–870.
- Niccoli G, Scalone G, Crea F. Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management. Eur Heart J 2015;36(8):475–481.
- Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio AL, De Caterina R, Zimarino M, Roffi M, Kjeldsen K, Atar D, Kaski JC, Sechtem U, Tornvall P, on behalf of the WG on Cardiovascular Pharmacotherapy. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J 2017;38(3):143–153.
- Hartley A, Marshall DC, Salciccioli JD, Sikkel MB, Maruthappu M, Shalhoub J. Trends in mortality from ischemic heart disease and cerebrovascular disease in Europe: 1980 to 2009. Circulation 2016;133(20):1916–1926.
- Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J 2016;37(42):3232–3245.
- Sugiyama T, Hasegawa K, Kobayashi Y, Takahashi O, Fukui T, Tsugawa Y. Differential time trends of outcomes and costs of care for acute myocardial infarction hospitalizations by ST elevation and type of intervention in the United States, 2001-2011. J Am Heart Assoc 2015;4(3):e001445.
- McManus DD, Gore J, Yarzebski J, Spencer F, Lessard D, Goldberg RJ. Recent trends in the incidence, treatment, and outcomes of patients with STEMI and NSTEMI. Am J Med 2011;124(1):40–47.
- Jernberg T. Swedeheart Annual Report 2015. In: Karolinska University Hospital, Huddinge, 14186 Stockholm; 2016.
- Widimsky P, Wijns W, Fajadet J, de Belder M, Knot J, Aaberge L, Andrikopoulos G, Baz JA, Betriu A, Claeys M, Danchin N, Djambazov S, Erne P, Hartikainen J, Huber K, Kala P, Klinceva M, Kristensen SD, Ludman P, Ferre JM, Merkely B, Milicic D, Morais J, Noc M, Opolski G, Ostojic M, Radovanovic D, De Servi S, Stenestrand U, Studencan M, Tubaro M, Vasiljevic Z, Weidinger F, Witkowski A, Zeymer U, European Association for Percutaneous Cardiovascular Interventions. Reperfusion therapy for ST elevation acute myocardial infarction in Europe: description of the current situation in 30 countries. Eur Heart J 2010;31(8):943–957.
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB, American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation 2015;131(4):e29–322.
- Khera S, Kolte D, Gupta T, Subramanian KS, Khanna N, Aronow WS, Ahn C, Timmermans RJ, Cooper HA, Fonarow GC, Frishman WH, Panza JA, Bhatt DL. Temporal trends and sex differences in revascularization and outcomes of st-segment elevation myocardial infarction in younger adults in the United States. J Am Coll Cardiol 2015;66(18):1961–1972.
- Puymirat E, Simon T, Steg PG, Schiele F, Gueret P, Blanchard D, Khalife K, Goldstein P, Cattan S, Vaur L, Cambou JP, Ferrieres J, Danchin N, USIK USIC 2000 Investigators, FAST MI Investigators. Association of changes in clinical characteristics and management with improvement in survival among patients with ST-elevation myocardial infarction. JAMA 2012;308(10):998–1006.
- Gale CP, Allan V, Cattle BA, Hall AS, West RM, Timmis A, Gray HH, Deanfield J, Fox KA, Feltbower R. Trends in hospital treatments, including revascularisation, following acute myocardial infarction, 2003-2010: a multilevel and relative survival analysis for the National Institute for Cardiovascular Outcomes Research (NICOR). Heart 2014;100(7):582–589.
- Kristensen SD, Laut KG, Fajadet J, Kaifoszova Z, Kala P, Di Mario C, Wijns W, Clemmensen P, Agladze V, Antoniades L, Alhabib KF, De Boer MJ, Claeys MJ, Deleanu D, Dudek D, Erglis A, Gilard M, Goktekin O, Guagliumi G, Gudnason T, Hansen KW, Huber K, James S, Janota T, Jennings S, Kajander O, Kanakakis J, Karamfiloff KK, Kedev S, Kornowski R, Ludman PF, Merkely B, Milicic D, Najafov R, Nicolini FA, Noc M, Ostojic M, Pereira H, Radovanovic D, Sabate M, Sobhy M, Sokolov M, Studencan M, Terzic I, Wahler S, Widimsky P, European Association for Percutaneous Cardiovascular Interventions. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: current status in 37 ESC countries. Eur Heart J 2014;35(29):1957–1970.
- Dans AL, Connolly SJ, Wallentin L, Yang S, Nakamya J, Brueckmann M, Ezekowitz M, Oldgren J, Eikelboom JW, Reilly PA, Yusuf S. Concomitant use of antiplatelet therapy with dabigatran or warfarin in the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) trial. Circulation. 2013 Feb 5;127(5):634-40. doi: 10.1161/CIRCULATIONAHA.112.115386. Epub 2012 Dec 27. PMID: 23271794.
- Hansen ML, Sørensen R, Clausen MT, Fog-Petersen ML, Raunsø J, Gadsbøll N, Gislason GH, Folke F, Andersen SS, Schramm TK, Abildstrøm SZ, Poulsen HE, Køber L, Torp-Pedersen C. Risk of bleeding with single, dual, or triple therapy with warfarin, aspirin, and clopidogrel in patients with atrial fibrillation. Arch Intern Med. 2010 Sep 13;170(16):1433-41. doi: 10.1001/archinternmed.2010.271. PMID: 20837828.
- Valgimigli M, Bueno H, Byrne RA, Collet JP, Costa F, Jeppsson A, Jüni P, Kastrati A, Kolh P, Mauri L, Montalescot G, Neumann FJ, Petricevic M, Roffi M, Steg PG, Windecker S, Zamorano JL, Levine GN; ESC Scientific Document Group; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018 Jan 14;39(3):213-260. doi: 10.1093/eurheartj/ehx419. PMID: 28886622.
- Gibson CM, Mehran R, Bode C, Halperin J, Verheugt FW, Wildgoose P, Birmingham M, Ianus J, Burton P, van Eickels M, Korjian S, Daaboul Y, Lip GY, Cohen M, Husted S, Peterson ED, Fox KA. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N Engl J Med. 2016 Dec 22;375(25):2423-2434. doi: 10.1056/NEJMoa1611594. Epub 2016 Nov 14. PMID: 27959713.
- Brieger D, Eagle KA, Goodman SG, Steg PG, Budaj A, White K, Montalescot G; GRACE Investigators. Acute coronary syndromes without chest pain, an underdiagnosed and undertreated high-risk group: insights from the Global Registry of Acute Coronary Events. Chest. 2004 Aug;126(2):461-9. doi: 10.1378/chest.126.2.461. PMID: 15302732.
- Malkin CJ, Prakash R, Chew DP. The impact of increased age on outcome from a strategy of early invasive management and revascularisation in patients with acute coronary syndromes: retrospective analysis study from the ACACIA registry. BMJ Open. 2012 Feb 16;2(1):e000540. doi: 10.1136/bmjopen-2011-000540. PMID: 22344538; PMCID: PMC3282292.
- Toleva O, Ibrahim Q, Brass N, Sookram S, Welsh R. Treatment choices in elderly patients with ST: elevation myocardial infarction-insights from the Vital Heart Response registry. Open Heart. 2015 Jun 24;2(1):e000235. doi: 10.1136/openhrt-2014-000235. PMID: 26196017; PMCID: PMC4488892.
- Alexander KP, Chen AY, Roe MT, Newby LK, Gibson CM, Allen-LaPointe NM, Pollack C, Gibler WB, Ohman EM, Peterson ED; CRUSADE Investigators. Excess dosing of antiplatelet and antithrombin agents in the treatment of non-ST-segment elevation acute coronary syndromes. JAMA. 2005 Dec 28;294(24):3108-16. doi: 10.1001/jama.294.24.3108. Erratum in: JAMA. 2006 Feb 8;295(6):628. PMID: 16380591.
- Bueno H, Betriu A, Heras M, Alonso JJ, Cequier A, García EJ, López-Sendón JL, Macaya C, Hernández-Antolín R; TRIANA Investigators. Primary angioplasty vs. fibrinolysis in very old patients with acute myocardial infarction: TRIANA (TRatamiento del Infarto Agudo de miocardio eN Ancianos) randomized trial and pooled analysis with previous studies. Eur Heart J. 2011 Jan;32(1):51-60. doi: 10.1093/eurheartj/ehq375. Epub 2010 Oct 22. PMID: 20971744; PMCID: PMC3013200.
- Timmer JR, Ottervanger JP, de Boer MJ, Boersma E, Grines CL, Westerhout CM, Simes RJ, Granger CB, Zijlstra F; Primary Coronary Angioplasty vs Thrombolysis-2 Trialists Collaborators Group. Primary percutaneous coronary intervention compared with fibrinolysis for myocardial infarction in diabetes mellitus: results from the Primary Coronary Angioplasty vs Thrombolysis-2 trial. Arch Intern Med. 2007 Jul 9;167(13):1353-9. doi: 10.1001/archinte.167.13.1353. PMID: 17620527.
- James S, Angiolillo DJ, Cornel JH, Erlinge D, Husted S, Kontny F, Maya J, Nicolau JC, Spinar J, Storey RF, Stevens SR, Wallentin L; PLATO Study Group. Ticagrelor vs. clopidogrel in patients with acute coronary syndromes and diabetes: a substudy from the PLATelet inhibition and patient Outcomes (PLATO) trial. Eur Heart J. 2010 Dec;31(24):3006-16. doi: 10.1093/eurheartj/ehq325. Epub 2010 Aug 29. PMID: 20802246; PMCID: PMC3001588.
- NICE-SUGAR Study Investigators; Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Henderson WR, Hébert PC, Heritier S, Heyland DK, McArthur C, McDonald E, Mitchell I, Myburgh JA, Norton R, Potter J, Robinson BG, Ronco JJ. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009 Mar 26;360(13):1283-97. doi: 10.1056/NEJMoa0810625. Epub 2009 Mar 24. PMID: 19318384.
- Senthinathan A, Kelly V, Dzingina M, Jones D, Baker M, Longson D; Guideline Development Group. Hyperglycaemia in acute coronary syndromes: summary of NICE guidance. BMJ. 2011 Oct 26;343:d6646. doi: 10.1136/bmj.d6646. PMID: 22031910.
- Szummer K, Lundman P, Jacobson SH, Schön S, Lindbäck J, Stenestrand U, Wallentin L, Jernberg T; SWEDEHEART. Relation between renal function, presentation, use of therapies and in-hospital complications in acute coronary syndrome: data from the SWEDEHEART register. J Intern Med. 2010 Jul;268(1):40-9. doi: 10.1111/j.1365-2796.2009.02204.x. Epub 2009 Dec 3. PMID: 20210836.
- Authors/Task Force members; Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, Falk V, Filippatos G, Hamm C, Head SJ, Jüni P, Kappetein AP, Kastrati A, Knuuti J, Landmesser U, Laufer G, Neumann FJ, Richter DJ, Schauerte P, Sousa Uva M, Stefanini GG, Taggart DP, Torracca L, Valgimigli M, Wijns W, Witkowski A. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014 Oct 1;35(37):2541-619. doi: 10.1093/eurheartj/ehu278. Epub 2014 Aug 29. PMID: 25173339.
- Gierlotka M, Gasior M, Wilczek K, Hawranek M, Szkodzinski J, Paczek P, Lekston A, Kalarus Z, Zembala M, Polonski L. Reperfusion by primary percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction within 12 to 24 hours of the onset of symptoms (from a prospective national observational study [PL-ACS]). Am J Cardiol. 2011 Feb 15;107(4):501-8. doi: 10.1016/j.amjcard.2010.10.008. Epub 2010 Dec 31. PMID: 21195380.
- Schömig A, Mehilli J, Antoniucci D, Ndrepepa G, Markwardt C, Di Pede F, Nekolla SG, Schlotterbeck K, Schühlen H, Pache J, Seyfarth M, Martinoff S, Benzer W, Schmitt C, Dirschinger J, Schwaiger M, Kastrati A; Beyond 12 hours Reperfusion AlternatiVe Evaluation (BRAVE-2) Trial Investigators. Mechanical reperfusion in patients with acute myocardial infarction presenting more than 12 hours from symptom onset: a randomized controlled trial. JAMA. 2005 Jun 15;293(23):2865-72. doi: 10.1001/jama.293.23.2865. PMID: 15956631.
- Busk M, Kaltoft A, Nielsen SS, Bøttcher M, Rehling M, Thuesen L, Bøtker HE, Lassen JF, Christiansen EH, Krusell LR, Andersen HR, Nielsen TT, Kristensen SD. Infarct size and myocardial salvage after primary angioplasty in patients presenting with symptoms for <12 h vs. 12-72 h. Eur Heart J. 2009 Jun;30(11):1322-30. doi: 10.1093/eurheartj/ehp113. Epub 2009 Apr 8. PMID: 19357105.
- Hochman JS, Lamas GA, Buller CE, Dzavik V, Reynolds HR, Abramsky SJ, Forman S, Ruzyllo W, Maggioni AP, White H, Sadowski Z, Carvalho AC, Rankin JM, Renkin JP, Steg PG, Mascette AM, Sopko G, Pfisterer ME, Leor J, Fridrich V, Mark DB, Knatterud GL; Occluded Artery Trial Investigators. Coronary intervention for persistent occlusion after myocardial infarction. N Engl J Med. 2006 Dec 7;355(23):2395-407. doi: 10.1056/NEJMoa066139. Epub 2006 Nov 14. PMID: 17105759; PMCID: PMC1995554.
- Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H, Held C, Horrow J, Husted S, James S, Katus H, Mahaffey KW, Scirica BM, Skene A, Steg PG, Storey RF, Harrington RA; PLATO Investigators; Freij A, Thorsén M. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009 Sep 10;361(11):1045-57. doi: 10.1056/NEJMoa0904327. Epub 2009 Aug 30. PMID: 19717846.
- Chen ZM, Jiang LX, Chen YP, Xie JX, Pan HC, Peto R, Collins R, Liu LS; COMMIT (ClOpidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet. 2005 Nov 5;366(9497):1607-21. doi: 10.1016/S0140-6736(05)67660-X. PMID: 16271642.
- Yusuf S, Mehta SR, Chrolavicius S, Afzal R, Pogue J, Granger CB, Budaj A, Peters RJ, Bassand JP, Wallentin L, Joyner C, Fox KA; OASIS-6 Trial Group. Effects of fondaparinux on mortality and reinfarction in patients with acute ST-segment elevation myocardial infarction: the OASIS-6 randomized trial. JAMA. 2006 Apr 5;295(13):1519-30. doi: 10.1001/jama.295.13.joc60038. Epub 2006 Mar 14. PMID: 16537725.
- Peacock WF, Hollander JE, Diercks DB, Lopatin M, Fonarow G, Emerman CL. Morphine and outcomes in acute decompensated heart failure: an ADHERE analysis. Emerg Med J. 2008 Apr;25(4):205-9. doi: 10.1136/emj.2007.050419. PMID: 18356349.
- Weng CL, Zhao YT, Liu QH, Fu CJ, Sun F, Ma YL, Chen YW, He QY. Meta-analysis: Noninvasive ventilation in acute cardiogenic pulmonary edema. Ann Intern Med. 2010 May 4;152(9):590-600. doi: 10.7326/0003-4819-152-9-201005040-00009. Erratum in: Ann Intern Med. 2010 Aug 17;153(4):280. Erratum in: Ann Intern Med. 2010 Jul 6;153(1):67. PMID: 20439577.
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016 Jul 14;37(27):2129-2200. doi: 10.1093/eurheartj/ehw128. Epub 2016 May 20. Erratum in: Eur Heart J. 2016 Dec 30;: PMID: 27206819.
- Udell J, Jones W, Petrie M, et al. Sodium Glucose Cotransporter-2 Inhibition for Acute Myocardial Infarction. J Am Coll Cardiol. 2022 May, 79 (20) 2058–2068.
- Paolisso P, Bergamaschi L, Gragnano F, Gallinoro E, Cesaro A, Sardu C, Mileva N, Foà A, Armillotta M, Sansonetti A, Amicone S, Impellizzeri A, Esposito G, Morici N, Andrea OJ, Casella G, Mauro C, Vassilev D, Galie N, Santulli G, Marfella R, Calabrò P, Pizzi C, Barbato E. Outcomes in diabetic patients treated with SGLT2-Inhibitors with acute myocardial infarction undergoing PCI: The SGLT2-I AMI PROTECT Registry. Pharmacol Res. 2023 Jan;187:106597. doi: 10.1016/j.phrs.2022.106597. Epub 2022 Dec 5. PMID: 36470546; PMCID: PMC9946774.
- Dong Y, Xu Y, Ding C, Yu Z, Yu Z, Xia X, Chen Y, Jiang X. Comparing the efficacy of angiotensin receptor-neprilysin inhibitor and enalapril in acute anterior STEMI patients after primary percutaneous coronary intervention: a prospective randomized trial. Cardiovasc Diagn Ther. 2022 Feb;12(1):42-54. doi: 10.21037/cdt-21-386. PMID: 35282662; PMCID: PMC8898690.
- Pfeffer MA, Claggett B, Lewis EF, Granger CB, Køber L, Maggioni AP, Mann DL, McMurray JJV, Rouleau JL, Solomon SD, Steg PG, Berwanger O, Cikes M, De Pasquale CG, East C, Fernandez A, Jering K, Landmesser U, Mehran R, Merkely B, Vaghaiwalla Mody F, Petrie MC, Petrov I, Schou M, Senni M, Sim D, van der Meer P, Lefkowitz M, Zhou Y, Gong J, Braunwald E; PARADISE-MI Investigators and Committees. Angiotensin Receptor-Neprilysin Inhibition in Acute Myocardial Infarction. N Engl J Med. 2021 Nov 11;385(20):1845-1855. doi: 10.1056/NEJMoa2104508. Erratum in: N Engl J Med. 2021 Dec 30;385(27):2592. PMID: 34758252.
- Picard MH, Davidoff R, Sleeper LA, Mendes LA, Thompson CR, Dzavik V, Steingart R, Gin K, White HD, Hochman JS; SHOCK Trial. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK. Echocardiographic predictors of survival and response to early revascularization in cardiogenic shock. Circulation. 2003 Jan 21;107(2):279-84. doi: 10.1161/01.cir.0000045667.11911.f6. PMID: 12538428.
- Lancellotti P, Price S, Edvardsen T, Cosyns B, Neskovic AN, Dulgheru R, Flachskampf FA, Hassager C, Pasquet A, Gargani L, Galderisi M, Cardim N, Haugaa KH, Ancion A, Zamorano JL, Donal E, Bueno H, Habib G. The use of echocardiography in acute cardiovascular care: recommendations of the European Association of Cardiovascular Imaging and the Acute Cardiovascular Care Association. Eur Heart J Acute Cardiovasc Care. 2015 Feb;4(1):3-5. doi: 10.1177/2048872614568073. Epub 2015 Jan 29. PMID: 25635106.
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeJemtel TH. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999 Aug 26;341(9):625-34. doi: 10.1056/NEJM199908263410901. PMID: 10460813.
- De Backer D, Biston P, Devriendt J, Madl C, Chochrad D, Aldecoa C, Brasseur A, Defrance P, Gottignies P, Vincent JL; SOAP II Investigators. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med. 2010 Mar 4;362(9):779-89. doi: 10.1056/NEJMoa0907118. PMID: 20200382.
- Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, Richardt G, Hennersdorf M, Empen K, Fuernau G, Desch S, Eitel I, Hambrecht R, Fuhrmann J, Böhm M, Ebelt H, Schneider S, Schuler G, Werdan K; IABP-SHOCK II Trial Investigators. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med. 2012 Oct 4;367(14):1287-96. doi: 10.1056/NEJMoa1208410. Epub 2012 Aug 26. PMID: 22920912.
- Patel MR, Smalling RW, Thiele H, Barnhart HX, Zhou Y, Chandra P, Chew D, Cohen M, French J, Perera D, Ohman EM. Intra-aortic balloon counterpulsation and infarct size in patients with acute anterior myocardial infarction without shock: the CRISP AMI randomized trial. JAMA. 2011 Sep 28;306(12):1329-37. doi: 10.1001/jama.2011.1280. Epub 2011 Aug 29. PMID: 21878431.
- Ouweneel DM, Eriksen E, Sjauw KD, van Dongen IM, Hirsch A, Packer EJ, Vis MM, Wykrzykowska JJ, Koch KT, Baan J, de Winter RJ, Piek JJ, Lagrand WK, de Mol BA, Tijssen JG, Henriques JP. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump in Cardiogenic Shock After Acute Myocardial Infarction. J Am Coll Cardiol. 2017 Jan 24;69(3):278-287. doi: 10.1016/j.jacc.2016.10.022. Epub 2016 Oct 31. PMID: 27810347.
- Cheng JM, den Uil CA, Hoeks SE, van der Ent M, Jewbali LS, van Domburg RT, Serruys PW. Percutaneous left ventricular assist devices vs. intra-aortic balloon pump counterpulsation for treatment of cardiogenic shock: a meta-analysis of controlled trials. Eur Heart J. 2009 Sep;30(17):2102-8. doi: 10.1093/eurheartj/ehp292. Epub 2009 Jul 18. PMID: 19617601.
- Sheu JJ, Tsai TH, Lee FY, Fang HY, Sun CK, Leu S, Yang CH, Chen SM, Hang CL, Hsieh YK, Chen CJ, Wu CJ, Yip HK. Early extracorporeal membrane oxygenator-assisted primary percutaneous coronary intervention improved 30-day clinical outcomes in patients with ST-segment elevation myocardial infarction complicated with profound cardiogenic shock. Crit Care Med. 2010 Sep;38(9):1810-7. doi: 10.1097/CCM.0b013e3181e8acf7. PMID: 20543669.
- Starling RC, Naka Y, Boyle AJ, Gonzalez-Stawinski G, John R, Jorde U, Russell SD, Conte JV, Aaronson KD, McGee EC Jr, Cotts WG, DeNofrio D, Pham DT, Farrar DJ, Pagani FD. Results of the post-U.S. Food and Drug Administration-approval study with a continuous flow left ventricular assist device as a bridge to heart transplantation: a prospective study using the INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support). J Am Coll Cardiol. 2011 May 10;57(19):1890-8. doi: 10.1016/j.jacc.2010.10.062. Erratum in: J Am Coll Cardiol. 2011 Nov 8;58(20):2142. PMID: 21545946.
- Schmitt J, Duray G, Gersh BJ, Hohnloser SH. Atrial fibrillation in acute myocardial infarction: a systematic review of the incidence, clinical features and prognostic implications. Eur Heart J. 2009 May;30(9):1038-45. doi: 10.1093/eurheartj/ehn579. Epub 2008 Dec 24. PMID: 19109347.
- Kirchhof P, Benussi S, Kotec ha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P; ESC Scientific Document Group. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016 Oct 7;37(38):2893-2962. doi: 10.1093/eurheartj/ehw210. Epub 2016 Aug 27. PMID: 27567408.
- Gorenek B, Blomström Lundqvist C, Brugada Terradellas J, Camm AJ, Hindricks G, Huber K, Kirchhof P, Kuck KH, Kudaiberdieva G, Lin T, Raviele A, Santini M, Tilz RR, Valgimigli M, Vos MA, Vrints C, Zeymer U, Lip GY, Potpara T, Fauchier L, Sticherling C, Roffi M, Widimsky P, Mehilli J, Lettino M, Schiele F, Sinnaeve P, Boriani G, Lane D, Savelieva I. Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and EAPCI task force. Europace. 2014 Nov;16(11):1655-73. doi: 10.1093/europace/euu208. Epub 2014 Aug 29. Erratum in: Europace. 2019 Oct 1;21(10):1518. PMID: 25172845.
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Van Veldhuisen DJ; ESC Scientific Document Group. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015 Nov 1;36(41):2793-2867. doi: 10.1093/eurheartj/ehv316. Epub 2015 Aug 29. PMID: 26320108.
- Piccini JP, Schulte PJ, Pieper KS, Mehta RH, White HD, Van de Werf F, Ardissino D, Califf RM, Granger CB, Ohman EM, Alexander JH. Antiarrhythmic drug therapy for sustained ventricular arrhythmias complicating acute myocardial infarction. Crit Care Med. 2011 Jan;39(1):78-83. doi: 10.1097/CCM.0b013e3181fd6ad7. PMID: 20959785; PMCID: PMC3010352.
- Chatterjee S, Chaudhuri D, Vedanthan R, Fuster V, Ibanez B, Bangalore S, Mukherjee D. Early intravenous beta-blockers in patients with acute coronary syndrome--a meta-analysis of randomized trials. Int J Cardiol. 2013 Sep 30;168(2):915-21. doi: 10.1016/j.ijcard.2012.10.050. Epub 2012 Nov 17. PMID: 23168009; PMCID: PMC4104797.
- Piccini JP, Schulte PJ, Pieper KS, Mehta RH, White HD, Van de Werf F, Ardissino D, Califf RM, Granger CB, Ohman EM, Alexander JH. Antiarrhythmic drug therapy for sustained ventricular arrhythmias complicating acute myocardial infarction. Crit Care Med. 2011 Jan;39(1):78-83. doi: 10.1097/CCM.0b013e3181fd6ad7. PMID: 20959785; PMCID: PMC3010352.
- Masuda M, Nakatani D, Hikoso S, Suna S, Usami M, Matsumoto S, Kitamura T, Minamiguchi H, Okuyama Y, Uematsu M, Yamada T, Iwakura K, Hamasaki T, Sakata Y, Sato H, Nanto S, Hori M, Komuro I, Sakata Y; OACIS investigators. Clinical Impact of Ventricular Tachycardia and/or Fibrillation During the Acute Phase of Acute Myocardial Infarction on In-Hospital and 5-Year Mortality Rates in the Percutaneous Coronary Intervention Era. Circ J. 2016 Jun 24;80(7):1539-47. doi: 10.1253/circj.CJ-16-0183. Epub 2016 May 24. PMID: 27238618.
- Chen A, Ashburn MA. Cardiac Effects of Opioid Therapy. Pain Med. 2015 Oct;16 Suppl 1:S27-31. doi: 10.1111/pme.12915. PMID: 26461073.
- Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, Cleland J, Deharo JC, Delgado V, Elliott PM, Gorenek B, Israel CW, Leclercq C, Linde C, Mont L, Padeletti L, Sutton R, Vardas PE; ESC Committee for Practice Guidelines (CPG); Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S; Document Reviewers; Kirchhof P, Blomstrom-Lundqvist C, Badano LP, Aliyev F, Bänsch D, Baumgartner H, Bsata W, Buser P, Charron P, Daubert JC, Dobreanu D, Faerestrand S, Hasdai D, Hoes AW, Le Heuzey JY, Mavrakis H, McDonagh T, Merino JL, Nawar MM, Nielsen JC, Pieske B, Poposka L, Ruschitzka F, Tendera M, Van Gelder IC, Wilson CM. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013 Aug;34(29):2281-329. doi: 10.1093/eurheartj/eht150. Epub 2013 Jun 24. PMID: 23801822.
- Larsen JM, Ravkilde J. Acute coronary angiography in patients resuscitated from out-of-hospital cardiac arrest--a systematic review and meta-analysis. Resuscitation. 2012 Dec;83(12):1427-33. doi: 10.1016/j.resuscitation.2012.08.337. Epub 2012 Sep 7. PMID: 22960567.
- Garot P, Lefevre T, Eltchaninoff H, Morice MC, Tamion F, Abry B, Lesault PF, Le Tarnec JY, Pouges C, Margenet A, Monchi M, Laurent I, Dumas P, Garot J, Louvard Y. Six-month outcome of emergency percutaneous coronary intervention in resuscitated patients after cardiac arrest complicating ST-elevation myocardial infarction. Circulation. 2007 Mar 20;115(11):1354-62. doi: 10.1161/CIRCULATIONAHA.106.657619. Epub 2007 Mar 12. PMID: 17353440.
- Noc M, Fajadet J, Lassen JF, Kala P, MacCarthy P, Olivecrona GK, Windecker S, Spaulding C; European Association for Percutaneous Cardiovascular Interventions (EAPCI); Stent for Life (SFL) Group. Invasive coronary treatment strategies for out-of-hospital cardiac arrest: a consensus statement from the European association for percutaneous cardiovascular interventions (EAPCI)/stent for life (SFL) groups. EuroIntervention. 2014 May;10(1):31-7. doi: 10.4244/EIJV10I1A7. PMID: 24832635.
- Reynolds JC, Frisch A, Rittenberger JC, Callaway CW. Duration of resuscitation efforts and functional outcome after out-of-hospital cardiac arrest: when should we change to novel therapies? Circulation. 2013 Dec 3;128(23):2488-94. doi: 10.1161/CIRCULATIONAHA.113.002408. Epub 2013 Nov 17. PMID: 24243885; PMCID: PMC4004337.
- Moulaert VR, Verbunt JA, van Heugten CM, Wade DT. Cognitive impairments in survivors of out-of-hospital cardiac arrest: a systematic review. Resuscitation. 2009 Mar;80(3):297-305. doi: 10.1016/j.resuscitation.2008.10.034. Epub 2008 Dec 30. PMID: 19117659.
- Monsieurs KG, Nolan JP, Bossaert LL, Greif R, Maconochie IK, Nikolaou NI, Perkins GD, Soar J, Truhlář A, Wyllie J, Zideman DA; ERC Guidelines 2015 Writing Group. European Resuscitation Council Guidelines for Resuscitation 2015: Section 1. Executive summary. Resuscitation. 2015 Oct;95:1-80. doi: 10.1016/j.resuscitation.2015.07.038. Epub 2015 Oct 15. PMID: 26477410.
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, Hindricks G, Kastrati A, Lenzen MJ, Prescott E, Roffi M, Valgimigli M, Varenhorst C, Vranckx P, Widimský P; ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018 Jan 7;39(2):119-177. doi: 10.1093/eurheartj/ehx393. PMID: 28886621.