Reactive Attachment Disorder
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | طب نفس الأطفال والمراهقين |
| كتاب: | Reactive Attachment Disorder |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:55 AM |
الوصف
"last update: 21 Oct 2025" Download Guideline
- Executive Summary
These guidelines offer evidence-based recommendations on psychotherapeutic and pharmacological interventions of reactive attachment disorder in children. The recommendations are intended to provide psychiatrists and mental health professionals with practical guidance and improve mental health outcomes for children with reactive attachment disorder and their caregivers.
· The most important part of management is to improve the child-carer relationship where this is possible and relevant. Developing a nurturing parent-child relationship is the cornerstone to overcoming the damage caused by severe neglect and abuse. Child individual psychotherapy will help them come to terms with an abusive parent and so improve their attachment security in relation to that person, by enabling them to talk about them in a balanced and coherent way (strong recommendation)
· Parenting skills classes: education for parents and caregivers about attachment styles, attachment disorders as well as other necessary parenting skills. Parent education focuses on developing positive, non-punitive behavior management strategies, ways of responding to nonverbal communication, anticipation and coping strategies for when triggers arise (conditional recommendation).
· Attachment-Based Family Therapy (ABFT): typical therapy for attachment problems includes both children and their caregivers. Therapy often involves fun and rewarding activities that enhance the attachment bond as well as help parents and other children in the family understand the symptoms of the disorder and effective interventions. Implementing ABFT in practice requires a comprehensive understanding of the family's attachment patterns, dynamics, and needs (conditional recommendation).
· Play therapy. Help children to learn appropriate skills for interacting with peers and handling other social situations (conditional recommendation).
· Trauma-Focused Therapies: For children with RAD who have experienced trauma, trauma-focused therapies such as Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) are crucial for processing traumatic memories and promoting healing (conditional recommendation).
· Medication: While there is no specific medication for RAD, psychiatric medication is prescribed to address co-occurring conditions, such as depression or anxiety, if present (Strong recommendation).
- Recommendations
Recommendation 1: Caregivers of children with RAD must be patient, remain positive, and have realistic expectations about what is achievable. It is also important that caregivers take care of their own mental and physical health and seek support from others where necessary.
Strong Recommendation
High Quality Evidence 1
Recommendation 2: The most important part of management is to improve the child-caregiver relationship where this is possible and relevant. Developing a nurturing parent-child relationship is the cornerstone to overcoming the damage caused by severe neglect and abuse. Child individual psychotherapy will help them come to terms with an abusive parent and so improve their attachment security in relation to that person, by enabling them to talk about them in a balanced and coherent way
Strong Recommendation
High Quality Evidence 1,2,4
Recommendation 3: Parenting skills classes: education for parents and caregivers about attachment styles, attachment disorders as well as other necessary parenting skills. Parent education focuses on developing positive, non-punitive behavior management strategies, ways of responding to nonverbal communication, anticipation and coping strategies for when triggers arise.
High Quality Evidence 3,4,5
Recommendation 4: Comprehensive psychiatric evaluation and specific treatment plans developed by professionals including both individual and family interventions
Strong Recommendation
High Quality Evidence 4,5
Recommendation 5: Multi-Disciplinary Approach: Effective treatment often involves a team of professionals, including clinical psychologists, psychiatrists, and social workers.
Conditional Recommendation
Recommendation 6: Child−parent psychotherapy focuses primarily on the caregiver’s and child’s experience of one another and on altering patterns of emotional communication in the dyad to improve the attachment bond. The therapist helps the caregiver to appreciate the emotional experience of the child and its connection to the emotional experience of the caregiver
High Quality Evidence 5
Recommendation 7: Attachment-Based Family Therapy (ABFT): typical therapy for attachment problems includes both children and their caregivers. Therapy often involves fun and rewarding activities that enhance the attachment bond as well as help parents and other children in the family understand the symptoms of the disorder and effective interventions. Implementing ABFT in practice requires a comprehensive understanding of the family's attachment patterns, dynamics, and needs.
Conditional Recommendation
High Quality Evidence 5,6
Recommendation 8: Play therapy. Help children to learn appropriate skills for interacting with peers and handling other social situations.
Conditional Recommendation
Moderate Quality Evidence 9
Recommendation 9: Special education services. Specifically designed programs within your child’s school can help them learn skills required for academic and social success, while also addressing behavioral and emotional difficulties.
Conditional Recommendation
Moderate Quality Evidence 7
Recommendation 10: Secure Living Situation: Ensuring the child has a consistent and safe home environment is crucial. This may involve placement with foster parents or adoptive parents who can provide a nurturing and predictable environment. Avoiding as much as possible the transit of the child from one placement to another and from one caregiver to another, encouraging the most stable measures possible from the moment the child leaves his or her biological family.
High Quality Evidence 8,10
Recommendation 11: Social Skills Interventions: These interventions help children learn appropriate social behaviors and interactions with peers.
Conditional Recommendation
High Quality Evidence 8,10
Recommendation 12: Trauma-Focused Therapies: For children with RAD who have experienced trauma, trauma-focused therapies such as Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) are crucial for processing traumatic memories and promoting healing.
Conditional Recommendation
High Quality Evidence 11
Recommendation 13: Medication: While there is no specific medication for RAD, psychiatric medication is prescribed to address co-occurring conditions, such as depression or anxiety, if present.
Strong Recommendation
High Quality Evidence 8
- Acknowledgement
We would like to acknowledge the Child and Adolescent Psychiatry Scientific Committee and Egyptian Child and Adolescent Psychiatry Association ECAPA for developing these guidelines.
Chair of the GDG: Suaad Moussa, Prof. of Psychiatry, Cairo University
Members of the Guideline Development Group (GDG):
1. Prof. Azza ElBakry, Professor of Psychiatry, Cairo University.
2. Dr. Aliaa Magdy, Lecturer of Psychiatry, Cairo University.
3. Prof. Aref Khoweiled , Professor of Psychiatry, Cairo University.
4. Dr. Dina Mohamed El-Gabry, Professor of Psychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Ain Shams University.
5. Dr. Dina Massoud, Maamora Psychiatry Hospital
6. Dr. Dina Youssri Afifi, Assistant Prof. of Psychiatry, Cairo University.
7. Dr. Eman Gaber, Psychiatric Consultant, Deputy of Central Administration of General Secretariat of Mental Health GSMHAT.
8. Dr Gellan Karamallah Ramadan Assistant Professor in Neurology and Psychiatry Department, Assuit University.
9. Prof. Hanan Mohamed Ezzeldin Azzam, Professor of Psychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Ain Shams University.
10. Dr. Heba Essam Abou El Wafa, Professor of Psychiatry- Alexandria University.
11. Prof. Heba Hamed Elshahawi, Professor of Psychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department,Ain Shams University.
12. Dr. Helen Soliman, Head of child & Adolescent Psychiatry Unit -Maamora Psychiatry Hospital.
13. Prof. Hisham Salah Zaki, Professor of Psychiatry- Beni-Suef University.
14. Dr. Israa ElSharif, Lecturer of Psychiatry, Cairo University.
15. Prof. Maha Emadeldin, Professor of Psychiatry, Beni-Suef University.
16. Prof. Maha Mohamed Sayed, Professor of Neuropsychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Ain shams University. 2Chi
17. Prof. Manal Omar, Ass. Professor of Psychiatry, Faculty Of Postgraduate Childhood Studies, Ain Shams University.
18. Dr. Mariam Ehab Dawoud, Ass Prof. of Psychiatry Faculty of Medicine Fayoum University.
19. Dr. Marwa Nasr, Maamora Psychiatry Hospital
20. Prof Mahmoud Elwasify Professor of Psychiatry- Mansoura University.
21. Dr. Mohamed Elshiekh, Professor of Psychiatry, Ain Shams University.
22. Prof. Mohamed Nasreldin Sadek, Professor of Psychiatry, Faculty of Medicine Cairo University.
23. Prof Mohammad Abdelhakeem Seleem, Professor of Psychiatry, Tanta University.
24. Dr. Mona Mahmoud El Sheikh, Professor of Neuropsychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Faculty of Medicine, Ain Shams University.
25. Dr. Nahla Radwan, Consultant Psychiatrist, Ministry of Health.
26. Dr. Nermin Mahmoud Shaker, Professor of Psychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Ain Shams University.
27. Dr. Nermin Elsallami, Maamora Psychiatry Hospital
28. Prof. Ola Shaheen, Professor of Psychiatry, Cairo University.
29. Dr. Rana Walid Ibrahim Hamimy, Lecturer of Psychiatry, Cairo University.
30. Prof Salwa Tobar, Prof. of Psychiatry, Mansoura University
31. Dr. Sara Galal, Assistant Lecturer in Medical Department, Faculty of Postgraduate Childhood Studies. Ain Shams University.
32. Prof. Soha Abdel Latif Ghobashy, Professor of Psychiatry Alexandria University.
33. Dr. Walaa Fakher, Associate Professor of Psychiatry, Cairo University.
34. Dr. Walaa Hussny Elsaied, Consultant of Psychiatry- Head of Child & Adolescent Psychiatric Administration GSMHAT-Ministry of Health.
35. Prof. Yomna Sabry, Professor of Psychiatry Mansoura University
We would like to acknowledge the efforts of
Supervisor of the EHA Pediatric Protocols General Doctor/ Mourad Alfy Ramzy Tadros
• MD, FRCPCH(UK), MRCPI(Dublin)
• Consultant Paediatrician of Egyptian Military Medical Services.
• Professors of Paediatrics Military Medical Academy
• Head of Training Committee of Paediatrics of Egyptian Military Medical Board
• Consultant Paediatrician of the Medical Advisory Council of Egypt Healthcare
Authority (EHA).
Coordinators & Editing Supervisors
1. Dr. Hala Adel: Pediatric Consultant, Moderator & coordinator of Medical
Advisory Council of Egypt Healthcare Authority (EHA)
2. Dr. Huda Karam: Pediatric Specialist, Moderator & coordinator of Medical
Advisory Council of Egypt Healthcare Authority (EHA)
Cover Designed & Edited By
- Mr. Bassam Sayed: Technical Officer at Medical Advisory Council of Egypt
- Abbreviations
AACAP: American Academy of Child and Adolescent Psychiatry
(ABFT): Attachment-Based Family Therapy
DSM-5: Diagnostic and Statistical Sanual for Sental Disorders, 5th Edition
ECAPA: Egyptian Child and Adolescent Psychiatry Association
GDG: Guideline Development Group
GRADE: Grading of Recommendations, Assessment, Development and Evaluation
ICD-11: The International Classification of Diseases 11th edition
NGOs: Non -Governmental Organizations
NICE: National Institute for Health and Care Excellence
RAD: Reactive Attachment Disorder
TF-CBT: Trauma-Focused Cognitive Behavioral Therapy
- Glossary
Attachment-Based Interventions
These therapies aim to strengthen the bond between child and caregiver by promoting positive interactions, play, and nurturing touch to build trust and safety.
Attachment disorders in children
These disorders are characterized by difficulties in forming healthy emotional bonds with caregivers, stemming from early experiences of neglect, abuse, or inconsistent care.
Dyad
Refers to parent/caregiver – infant interaction
Reactive Attachment Disorder (RAD)
It's characterized by difficulties in forming secure attachments, experiencing positive emotions, and seeking or accepting comfort.
Trauma and stress-related disorders
A group of emotional and behavioral problems that may result from childhood traumatic and stressful experiences. These traumatic and stressful experiences can include exposure to physical or emotional violence or pain, including abuse, neglect or family conflict.
Trauma-focused therapy
It's a specialized form of psychotherapy designed to help individuals process and recover from the emotional and psychological effects of traumatic experiences.
- Introduction
The International Classification of Diseases 11th edition (ICD-11) classifies reactive attachment disorder and disinhibited social engagement disorder as two of the disorders specifically associated with stress, with onset in childhood. However, The Diagnostic and Statistical Manual 5th Edition (DSM-5) classifies reactive attachment disorder (RAD) as a trauma- and stress-related condition of early childhood caused by social neglect or maltreatment. 12, 13
Children with reactive attachment disorder show a consistent pattern of inhibited, emotionally withdrawn behavior towards adult caregivers. The child rarely or minimally seeks comfort when distressed, and rarely or minimally responds to comfort when distressed. There is minimal social and emotional responsiveness to others, episodes of unexplained irritability, sadness, or fearfulness that are evident even during non-threatening interaction with adult caregivers. 4
The child has typically experienced a pattern of extremes of insufficient care, such as social neglect or deprivation with persistent lack of basic emotional needs for comfort, stimulation, and affection met by caregiving adults. There may be a history of repeated changes of primary caregivers that limit opportunities to form stable attachments or rearing in unusual settings that severely limit opportunities to form selective attachments.4
- Scope and Purpose
This chapter provides guidance on psychotherapeutic interventions for reactive attachment disorder in children to be used by policymakers, mental health professionals and primary health care providers to offer better treatment strategies.
The objective of this chapter is to standardize practice to decrease variation of practice and improve outcome
- Target Audience
This guideline targets child and adolescent psychiatrists, psychiatrists, mental health professionals (clinical psychologists, social workers) family physicians, pediatricians, policy makers, as well as non-governmental organizations (NGOs) and other stakeholders to offer the most appropriate treatment guidelines for children with reactive attachment disorder.
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt the NICE and American (AACAP) standard of care for reactive attachment disorder. 1, 10
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of
Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
• GRADE working group:https://www.gradeworkinggroup.org
• GRADE online training modules: http://cebgrade.mcmaster.ca/
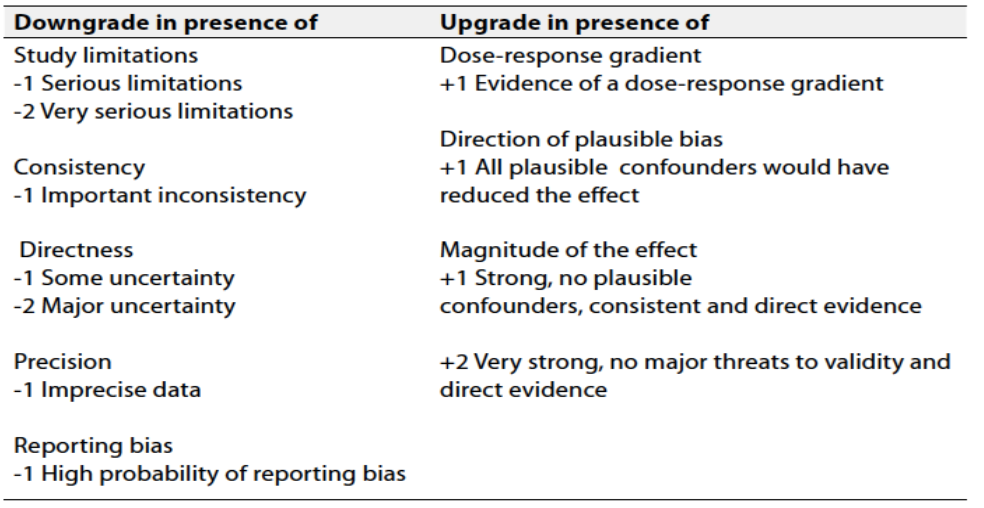
Table 1 Quality and Significance of the four levels of evidence in GRADE:
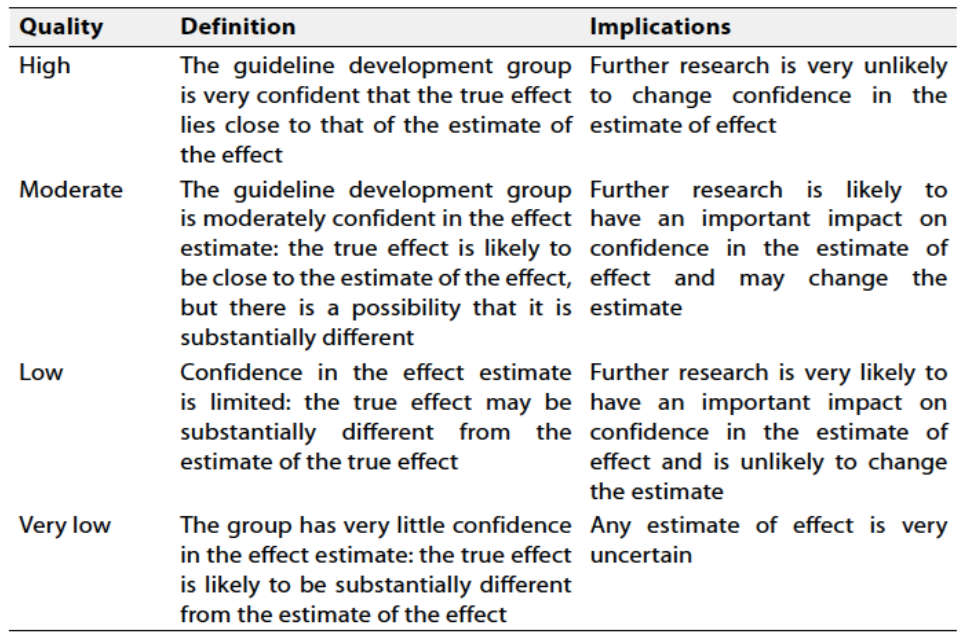
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
➡️The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation should account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Implementation Considerations
Several factors (barriers) may hinder the effective implementation and scale-up of the recommendations in this guideline. These factors may be related to the negative attitude of families, cultural beliefs towards mental disorders, inadequate resources, lack of trained mental healthcare professionals and limited financial resources. By addressing these challenges and implementing targeted strategies, Egypt can improve the implementation of treatment guidelines, ultimately enhancing the quality and equity of healthcare services for all children.
These factors were identified from case studies and systematic reviews exploring factors affecting the implementation of interventions to prevent /reduce complications rates. Additional barriers were identified from qualitative reviews undertaken for this guideline and Cochrane overviews of reviews of health system implementation, care delivery arrangements and financial strategies.
- Research Needs
During the review of evidence and the development of recommendations, several research gaps were identified regarding Egyptian population. Addressing these will help inform revision of these guidelines.
1. Long-Term Effectiveness: follow up studies should be done to evaluate the long-term effectiveness of psychotherapeutic programs (trauma-focused therapy, play therapy, and parenting. and attachment-based therapy.,,etc).
2. Tailoring Interventions: Investigate the effectiveness of personalized or modified psychotherapeutic and family intervention programs. Explore how personal and temperamental traits, cultural factors, socioeconomic status, mental health literacy, and stigma of mental illness influence program outcomes and identify strategies for optimizing prescription customization.
3. Cost-Effectiveness Analysis: Conduct cost-effectiveness analyses of psychotherapeutic intervention programs to assess the economic impact of these interventions. Evaluate the balance between costs, health outcomes, and potential healthcare savings to inform policy decisions and resource allocation.
- Monitoring and Evaluating the Impact of the Guideline
There are potential indicators that can be used to evaluate the success of the psychotherapeutic programs in treating reactive attachment disorder
1. Observing changes in the child's social interactions, emotional regulation, and overall behavior patterns.
2. Changes in the child's ability to form secure attachments, regulate emotions, and respond appropriately to caregivers
3. Development of healthy peer relationships and decreased social isolation.
4. Increased self-esteem and confidence, reduced feelings of guilt, and greater sense of hope and optimism about the future.
5. Program Engagement and Participation: Evaluate the level of engagement and participation of the target audience, including attendance rates for educational sessions, participation, and utilization of support resources. Higher engagement indicates increased program reach and potential effectiveness.
6. Cost-effectiveness: Assess the cost-effectiveness of the different treatment strategies
7. Patient Satisfaction and Feedback: Collect feedback from children and their families through surveys or interviews to evaluate their satisfaction with the program, perceived benefits, and suggestions for improvement. Positive satisfaction of children and their families indicates a well-received and impactful program.
- Update of the Guideline
This guideline will be updated whenever there is new evidence.
- References
1. National Collaborating Centre for Mental Health (UK). Children's Attachment: Attachment in Children and Young People Who Are Adopted from Care, in Care or at High Risk of Going into Care. London: National Institute for Health and Care Excellence (NICE); 2015 Nov. (NICE Guideline, No. 26.) 2, Introduction to children's attachment. Available from: https://www.ncbi.nlm.nih.gov/books/NBK356196/
2. Joseph MA, O'Connor TG, Briskman JA, et al; The formation of secure new attachments by children who were maltreated: an observational study of adolescents in foster care. Dev Psychopathol. 2014 Feb;26(1):67-80. doi: 10.1017/S0954579413000540. Epub 2013 Oct 29.
3. Winokur M, Holtan A, Batchelder KE; Kinship care for the safety, permanency, and well-being of children removed from the home for maltreatment. Cochrane Database Syst Rev. 2014 Jan 31;1:CD006546. doi:10.1002/14651858.CD006546.pub3.
4. Ellis EE, Yilanli M, Saadabadi A. Reactive Attachment Disorder. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537155/
5. Zeanah CH, Chesher T, Boris NW., American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI). Practice Parameter for the Assessment and Treatment of Children and Adolescents with Reactive Attachment Disorder and Disinhibited Social Engagement Disorder. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):990-1003. [PubMed].
6. Diamond G, Diamond GM, Levy S. Attachment-based family therapy: Theory, clinical model, outcomes, and process research. J Affect Disord. 2021 Nov 1;294:286-295. doi: 10.1016/j.jad.2021.07.005. Epub 2021 Jul 16. PMID: 34304083; PMCID: PMC8489519.
7. Bosmans G, Verschueren K, Cuyvers B, Minnis H. Current Perspectives on the Management of Reactive Attachment Disorder in Early Education. Psychol Res Behav Manag. 2020 Dec 18; 13:1235-1246. doi: 10.2147/PRBM.S264148. PMID: 33376419; PMCID: PMC7755333.
8. Talmón-Knuser F, González-Sala F, Lacomba-Trejo L, Samper-García P. Reactive Attachment Disorder and Its Relationship to Psychopathology: A Systematic Review. Children (Basel). 2023 Dec 6;10(12):1892. doi: 10.3390/children10121892. PMID: 38136094; PMCID: PMC10741566
9. Nasrin Zamani, Mehdi Tavallaei, Somaieh Kahdouei. Cognitive-behavioral play therapy in children with reactive attachment disorder: help reduce anxiety, impulsivity, bullying and antisocial behaviors. J Adv Pharm Edu Res 2020;10(S4):115-122. Source of Support: Nil, Conflict of Interest: None declared.
10. American Academy of Child & Adolescent Psychiatry. Attachment Disorders (https://www.aacap.org/aacap/Families_and_Youth/Facts_for_Families/FFF-Guide/Attachment-Disorders-085.aspx). Accessed 2/21/2022.
11. de Arellano MA, Lyman DR, Jobe-Shields L, George P, Dougherty RH, Daniels AS, Ghose SS, Huang L, Delphin-Rittmon ME. Trauma-focused cognitive-behavioral therapy for children and adolescents: assessing the evidence. Psychiatr Serv. 2014 May 1;65(5):591-602. doi: 10.1176/appi.ps.201300255. PMID: 24638076; PMCID: PMC4396183.
12. International Classification of Diseases 11th Revision; World Health Organization, 2019/2021.
13. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
- Annexes
Table 1: Reactive Attachment Disorder (DSM-5 criteria).
|
Diagnostic Criteria: 313.89 (F94.1) A. A consistent pattern of inhibited, emotionally withdrawn behavior toward adult caregivers, manifested by both of the following: 1. Rarely or minimally seeks comfort when distressed 2. Rarely or minimally responds to comfort offered when distressed B. A persistent social and emotional disturbance characterized by at least 2 of the following: 1. Minimal social and emotional responsiveness to others 2. Limited positive affect 3. Episodes of unexplained irritability, sadness, or fearfulness which are evident during non-threatening interactions with adult caregiver C. Child has experienced a pattern of extremes of insufficient care (pathogenic care) as evidenced by at least one of the following: 1.Social neglect or deprivation in the form of persistent lack of having basic emotional needs for comfort, stimulation, and affection met by caregiving adults 2. Repeated changes of primary caregiver that limit opportunities to form stable attachments (e.g., frequent changes in foster care) 3. Rearing in unusual settings that severely limit opportunities to form selective attachments (e.g. institutions with high child-to-caregiver ratios) D. The care in Criterion C is presumed to be responsible for the disturbed behavior in Criterion A (e.g. the disturbances in criterion A began following lack of adequate care in Criterion C) E. The criteria are not met for autism spectrum disorder F. Disturbance is evident before age 5 G. The child has a developmental age of at least 9
months Specify if: Persistent: The disorder has been present for more than 12 months Specify current severity: Reactive Attachment Disorder is specified as severe when a child exhibits all symptoms of the disorder, with each symptom manifesting at relatively high levels. |
Adapted from: American Psychiatric Association, (2013).13
Table 2: Reactive Attachment Disorder (ICD-11 criteria).
|
6B44: Reactive Attachment Disorder Reactive attachment disorder is characterized by grossly abnormal attachment behaviors in early childhood, occurring in the context of a history of grossly inadequate, childcare (e.g. severe neglect, multi treatment, institutional deprivation). Even when an adequate primary caregiver is newly available, the child does not turn into the primary caregiver for comfort, support, and nurture rarely displays security seeking behaviors towards any other and does not respond when comfort is offered. Reactive attachment disorder can only be diagnosed in children, and features of the disorder develop within the first five years of life. However, the disorder cannot be diagnosed before the age of one year (or developmental age of less than nine months, when the capacity for selective attachments may not be fully developed, or in the context of spectrum disorder. Exclusions: Asperger syndrome (coded as 6A02) and inhibited attachment disorder of childhood (coded as 6B 45) |
Adapted from: International Classification of Diseases 11th Revision, (2019/2021).12