diagnosis and treatment of functional constipation in infants and children
| Site: | EHC | Egyptian Health Council |
| Course: | Pediatrics Guidelines |
| Book: | diagnosis and treatment of functional constipation in infants and children |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:02 AM |
Description
"last update:
28 Oct 2025" Download Guideline
- Executive Summary
➡️Introduction
Functional constipation is a common problem in children. Although some guidelines exist for management of childhood constipation (1) there are no such guidelines for Egyptian children.
Functional constipation constituted 30% of pediatric gastroenterology outpatient practice, 4-5% of all referrals to pediatric gastroenterology tertiary care centers and 0.8-1% of all pediatric cases in medical colleges (1).
Normal stool frequency is; <1-month age: 3-4 times/day; 1 month to 1-year age: 1.5-2 times/day; 1 to 2-year age: 1-2 times/day, mostly formed; older than 2-year age: 1 time/day. While constipation is a delay or difficulty in defecation sufficient to cause significant distress to the patient (3,4).
When the duration of constipation is less than 4 weeks, it is considered as acute constipation and when the duration is more, it is chronic constipation; in addition to two or more of the following criteria: (a) defecation frequency ≤2 times per week, (b) fecal incontinence ≥1 times per week after the acquisition of toileting skills, (c) history of excessive stool retention, (d) history of painful or hard bowel movements, (e) presence of a large mass in the rectum or on per abdomen examination, (f) history of large-diameter stools that may obstruct the toilet (7).
The term “Fecal Incontinence”, currently used instead of the terms soiling or encopresis, is defined as passage of stools in the undergarment and is classified as: (a) Constipation-associated fecal incontinence and (b) non-retentive fecal incontinence: diagnosed only if there is no constipation and normal anal sphincter tone, and symptoms last for more than 2 months in a child with a developmental age of ≥4 years (1).
The term “Refractory constipation” is defined as constipation not responding to optimal conventional treatment for at least 3 months, despite good compliance. These patients should be referred to a pediatric gastroenterologist for evaluation (2).
History and examination are relevant in making a diagnosis of constipation and differentiating functional and organic constipation as follows: Dietary history; like intake of fruits and vegetables and refined foods (e.g., bakery), beverages etc. in older children, nature of feeds (breast vs top feeds) and details of supplementary feeds in younger babies, exclusive and prolonged milk intake with minimal solids in young infants, In addition to evidence of important precipitating factors of functional constipation;, (a) premature initiation of toilet training (normally toilet training should start not before 24 months in a developmentally normal child) (b) drugs and inter-current illnesses, (c) quick and abrupt transition of diet e.g. liquid to solid, breastfeeding to bottle feeding and (d) change in local environment (start of schooling) and psychosocial factors (3,5,6).
Characteristics of functional constipation in infants up to 4 years must include 2 or fewer defecations per week or 1 month of at least 2 of the following: (a) History of excessive stool retention, (b) History of painful or hard bowel movements, (c) History of large-diameter stools, (d) Presence of a large fecal mass in the rectum. While in toilet-trained children, the following additional criteria may be used: (a) At least 1 episode/week of incontinence after the acquisition of toileting skills, (b) History of large-diameter stools that may obstruct the toilet. Children greater than four years must have 2 or more of the following occurring at least once per week for a minimum of 1 month with insufficient criteria for a diagnosis of irritable bowel syndrome: (a) 2 or fewer defecations in the toilet per week in a child of a developmental age of at least 4 years, (b) At least 1 episode of fecal incontinence per week, (c) History of retentive posturing or excessive volitional stool retention, (d) History of painful or hard bowel movements, (e) Presence of a large fecal mass in the rectum, (f) History of large diameter stools that can obstruct the toilet (7).
Organic causes of constipation include; Abnormalities of the colon and rectum (e.g., chronic intestinal pseudo obstruction, anal stenosis, anal/colonic stricture, post NEC/IBD and ectopic anus), Neuropathic lesions (e.g., Hirschsprung disease and intestinal neuronal dysplasia), Spinal cord lesions (e.g., spina bifida, meningomyelocele, sacral agenesis, tethered cord and tumors), Metabolic (e.g., hypothyroidism, hypo/hyper-calcemia, hypokalemia and uremia), Systemic disorders (e.g., celiac disease, cystic fibrosis and diabetes mellitus) and Drugs (e.g., analgesics, anticholinergics, iron, sympathomimetics, psychotropics, NSAIDs and antacids) (6 ).
The aim of this adapted clinical practice guideline (CPG) is to provide evidence-based recommendations for diagnosis and treatment of functional constipation in infants and children. Thise recommendations were adapted from the relevant evaluation and treatment of functional constipation in infants and children: evidence-is based recommendations from ESPGHAN and NASPGHAN: JPGN 2014;58: 258–274 CPG(s) using a formal methodology for CPG adaptation: the Adapted-ADAPTE.
This guideline focuses on diagnosis and treatment of functional constipation.
Disease/Condition:
Guideline Objective(s)
Diagnosis and treatment of functional constipation in infants and children
Health / Clinical Question (PIPOH)
P: Patient (Target Population):
Gender: Both genders
Age group: infants and children from 1-18 years
Disease/condition: functional constipation in infants and children
I: Interventions and Practices Considered / CPG Category:
Clinical: history taking and examination
Laboratory investigations:
• laboratory investigations to diagnose (cow’s milk) allergy, celiac disease, hypothyroidism, and hypercalcemia
• abdominal radiography (use of barium enema to diagnose organic causes such as hd
• colonic transit time (ctt)
• transabdominal rectal ultrasonography
• magnetic resonance imaging (mri) of the spine
• colonic manometry
• anorectal manometry (arm) or rectal suction biopsy to diagnose hd
• colonic full-thickness biopsies
• treatment
P: Professionals (Intended / Target Users or Stakeholders) :
Primary health care physician
General practitioners
Family physician
Pediatrician
Gastroenterologist
O: Major Outcomes Considered:
- Primary outcome: proper diagnosis of functional constipation
- Secondary outcome: proper treatment of functional constipation
H: Healthcare Settings:
Types:
primary, secondary and tertiary healthcare centers.
•governmental healthcare sector:
moh, university, military, health insurance organization
•non-governmental healthcare sector:
private and NGO healthcare centers
Guideline development process and methods
After reviewing all the inclusion and exclusion criteria and quality appraisal results, the GDG/ GAG recommended using the following source original clinical practice guidelines (CPGs):
1- Tabbers MM, DiLorenzo C, Berger MY, Faure C, Langendam MW, Nurko S, Staiano A, Vandenplas Y, and Benninga MA, evaluation and Treatment of Functional Constipation in Infants and Children: Evidence-Based Recommendations from ESPGHAN and NASPGHAN: JPGN 2014;58: 258–274.
We conducted Adolopment for these guidelines: (Adoption, Adaptation, and Development)
- Adoption for most of the guideline recommendations.
- Development of Good Practice Statements
Recommendations and Good Practice Statements (GPS)
This version of the CPG includes recommendations and good practice statements on the following four sub-sections:
A. Diagnosis of Functional Constipation
The guideline covers 1 to 18 years old
This guideline emphasis on
B. Management of Functional Constipation
This section includes recommendations and good practice statements on
We can summarize the guidelines’ recommendations for Functional Constipation in the following:
·Based on expert opinion, we recommend the Rome III criteria for the definition of functional constipation for all age groups. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, the diagnosis of functional constipation should be based on history and physical examination. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, use the following alarm signs and symptoms to identify an underlying disease-causing constipation (e.g., onset < 48 h, family history of Hirschsprung disease, ribbon stools, blood without fissures, failure to thrive, bilious vomiting, abnormal anorectal or neurologic findings, sacral dimple, extreme fear during examination, etc.). • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, if only one Rome III criterion is met and diagnosis is uncertain—or if alarm signs or intractable constipation are present—a digital rectal examination is recommended to exclude underlying conditions. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, abdominal radiography is not indicated routinely but may be used when fecal impaction is suspected and physical examination is unreliable or impossible. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, rectal ultrasound is not recommended to diagnose functional constipation. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, routine laboratory testing for cow’s-milk allergy, celiac disease, hypothyroidism, and hypercalcemia is not recommended in children with functional constipation; a 2–4 weeks trial of cow’s-milk protein avoidance may be considered in intractable cases. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, barium enema should not be used as an initial diagnostic tool for organic causes of constipation. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, routine spinal MRI is not recommended in patients with intractable constipation without neurologic abnormalities. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, full-thickness colonic biopsies are not recommended to diagnose colonic neuromuscular disorders in intractable constipation. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, routine colonic scintigraphy is not recommended in children with intractable constipation. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, children with functional constipation should have a normal fiber intake. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, children with functional constipation should have a normal fluid intake. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, children with functional constipation should engage in normal physical activity. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, routine use of prebiotics and probiotics is not recommended in the treatment of childhood constipation. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, intensive behavioral therapy protocols are not recommended; rather, provide demystification, explanation, and toilet-training guidance (for developmental age ≥ 4 years). • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, biofeedback is not recommended as an adjunctive treatment in childhood constipation. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, routine multidisciplinary treatment is not recommended for childhood constipation. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, alternative medicine (acupuncture, homeopathy, mind-body therapy, osteopathic/chiropractic manipulations, yoga) is not recommended in childhood constipation. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, oral polyethylene glycol (PEG) 1–1.5 g/kg/day for 3–6 days is first-line for fecal disimpaction; if PEG is unavailable, daily enemas for 3–6 days are recommended. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, PEG (0.4 g/kg/day, titrate to response) with or without electrolytes is first-line maintenance; lactulose is an alternative if PEG is unavailable; routine chronic enemas are not recommended. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, maintenance therapy should continue for at least 2 months, with all symptoms resolved for ≥ 1 month before tapering; stop medication only after toilet training is achieved. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, transcutaneous nerve stimulation (TNS) is not supported for children with intractable constipation. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, antegrade continence enemas (ACE) are recommended in selected children with intractable constipation. • Quality of evidence: Very Low • Strength of recommendation: Conditional
· Based on expert opinion, approximately 50% of referred children recover without laxatives by 6–12 months, 10% remain well on laxatives, and 40% stay symptomatic; 50% recover by 5 years and 80% by 10 years; delayed treatment (> 3 months) correlates with longer symptom duration. • Quality of evidence: Low • Strength of recommendation: Conditional
· Based on expert opinion, use demographics, clinical history, physical exam, and select ancillary tests to identify prognostic factors for functional constipation—most evidence is limited, though strong evidence exists that sex and family history have no prognostic value. • Quality of evidence: Limited to Strong • Strength of recommendation: Conditiona
➡️Guideline Registration
PREPARE (Practice guideline REgistration for transPAREncy), WHO Collaborating Center for Guideline Implementation and Knowledge Translation, EBM Center, University of Lanzhou, Lanzhou, China. Registration Number: IPGRP-2021CNXXXXXXX. Link: http://www.guidelines-registry.org/- Recommendations
|
Table 3. Recommendations |
|
|
|||
|
A. Prevention and management of functional constipation |
|
|
|||
|
N |
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
A1 |
Q1: What is the definition of functional constipation? |
ESPGHAN |
(1) Based on expert opinion, we recommend the Rome III criteria for the definition of functional constipation for all age groups.
(2) Based on expert opinion, the diagnosis of functional constipation is based on history and physical examination |
Low
Low |
Conditional
Conditional |
|
|
Q2: What are the alarm signs and symptoms that suggest the presence of an underlying disease causing the constipation? |
ESPGHAN |
Based on expert opinion, we recommend using for alarm signs and symptoms and diagnostic clues to identify an underlying disease responsible for the constipation. 1. Constipation starting extremely early in life (48 h 2. Family history of HD 3. Ribbon stools 4. Blood in the stools in the absence of anal fissures 5. Failure to thrive 6. Fever 7. Bilious vomiting 8. Abnormal thyroid gland 9. Severe abdominal distension 10. Perianal fistula 11. Abnormal position of anus 12. Absent anal or cremasteric reflex 13. Decreased lower extremity strength/tone/reflex 14. Tuft of hair on spine Sacral dimple 15. Gluteal cleft deviation 16. Extreme fear during anal inspection Anal scars |
Very Low |
Conditional
|
|
Q3: In the Diagnosis of Functional Constipation in Children, What Is the Diagnostic Value of the Following |
Q 3.1 Digital Rectal Examination |
ESPGHAN |
1. Based on expert opinion, if only 1 of the Rome III criteria is present and the diagnosis of functional constipation is uncertain, a digital examination of the anorectum is recommended. Based on expert opinion, in the presence of alarm signs or symptoms or in patients with intractable constipation, a digital examination of the anorectum is recommended to exclude underlying medical conditions. |
Very Low |
Conditional |
|
|
Q 3.2 Abdominal Radiography
|
ESPGHAN |
The routine uses of an abdominal radiograph to diagnose functional constipation is not indicated.
Based on expert opinion, a plain abdominal radiography may be used in a child in whom fecal impaction is suspected but in whom physical examination is unreliable/not possible. |
Very Low |
Conditional |
|
|
Q3.3 Rectal ultrasound |
ESPGHAN |
Rectal ultrasound is not recommended to diagnose functional constipation |
Very Low |
Conditional |
|
Q4. Which of the following diagnostic tests should be performed in children with constipation to diagnose an underlying disease?
|
4.1 Laboratory Investigations to Diagnose (Cow’s Milk) Allergy, Celiac Disease, Hypothyroidism, and Hypercalcemia? |
ESPGHAN |
1. Routine allergy testing is not recommended to diagnose cow’s-milk allergy in children with functional constipation. 2. Based on expert opinion, a 2- to 4-week trial of avoidance of CMP may be indicated in the child with intractable constipation. Based on expert opinion, we do not recommend routine laboratory testing for hypothyroidism, celiac disease, and hypercalcemia in children with constipation in the absence of alarm symptoms. |
Very Low |
Conditional |
|
|
4.2 Use of Barium Enema to Diagnose Organic Causes Such as HD |
ESPGHAN |
Based on expert opinion, we do not recommend performing barium enema as an initial diagnostic tool for the evaluation of children with constipation. |
Very Low |
Conditional |
|
5- Which of the Following Examinations Should Be Performed in Children With Intractable Constipation to Evaluate Pathophysiology and Diagnose an Underlying Abnormality |
5.1 Magnetic Resonance Imaging (MRI) of the Spine |
ESPGHAN |
The routine use of MRI of the spine is not recommended in patients with intractable constipation without other neurologic abnormalities. |
Very low |
Conditional
|
|
|
5.2 Colonic Full-Thickness Biopsies |
ESPGHAN |
Based on expert opinion, we do not recommend obtaining full-thickness colonic biopsies to diagnose colonic neuromuscular disorders in children with intractable constipation. |
Very low |
Conditional
|
|
|
5.3 Colonic Scintigraphy |
ESPGHAN |
Based on expert opinion we do not recommend routine use of colonic scintigraphy studies in children with intractable constipation |
Low |
Conditional
|
|
6: What Is the Additional Effect of the Following Nonpharmacologic Treatments in Children with Functional Constipation? |
6.1 Fiber
|
ESPGHAN |
A normal fiber intake is recommended in children with constipation. |
Very low |
Conditional
|
|
|
6.2 Fluid |
ESPGHAN |
Based on expert opinion, we recommend a normal fluid intake in children with constipation. |
Low |
Conditional
|
|
|
6.3 Physical activity |
ESPGHAN |
Based on expert opinion, we recommend a normal physical activity in children with constipation. |
Low |
Conditional
|
|
|
6.4 Prebiotics and probiotics |
ESPGHAN |
The routine use of prebiotics and probiotic is not recommended in the treatment of childhood constipation. |
Very low |
Conditional
|
|
|
6.5 Behavioral therapy
|
ESPGHAN |
1. The routine use of an intensive behavioral protocolized therapy program in addition to conventional treatment is not recommended in childhood constipation.
Based on expert opinion, we recommend demystification, explanation, and guidance for toilet training (in children with a developmental age of at least 4 years) in the treatment of childhood constipation |
Low |
Conditional
|
|
|
6.6 Biofeedback
|
ESPGHAN |
The use of biofeedback as additional treatment is not recommended in childhood constipation. |
Low |
Conditional
|
|
|
6.7 multidisciplinary treatment |
ESPGHAN |
Based on expert opinion, we do not recommend the routine use of multidisciplinary treatment in childhood constipation. |
Low |
Conditional
|
|
|
6.8 Alternative medicine (Including Acupuncture, Homeopathy, Mind-Body Therapy, Musculoskeletal Manipulations Such As Osteopathic and Chiropractic and Yoga) |
ESPGHAN |
Based on expert opinion, we do not recommend the use of alternative treatments in childhood constipation. |
Low |
Conditional
|
|
7: What Is the Most Effective and Safest Pharmacologic Treatment in Children with Functional Constipation? |
7.1 Which Pharmacologic Treatment Should Be Given for Dis-impaction? |
ESPGHAN |
The use of PEG with or without electrolytes orally 1 to 1.5 g _ kg_1 _ day_1 for 3 to 6 days is recommended as the first-line treatment for children presenting with fecal impaction.
An enema once per day for 3 to 6 days is recommended for children with fecal impaction, if PEG is not available. |
Very low |
Conditional
|
|
|
7.2 Which Pharmacologic Treatment Should Be Given for Maintenance Therapy?
|
ESPGHAN
|
1. The use of PEG with (mixed with water) or without (mixed with juice) electrolytes is recommended as the first-line maintenance treatment. A starting dose of 0.4 g _ kg_1 _ day_1 is recommended, and the dose should be adjusted according to the clinical response. 2. The addition of enemas to the chronic use of PEG is not recommended in children with constipation. The use of lactulose as the first-line maintenance treatment is recommended, if PEG is not available. |
Very low |
Conditional
|
|
|
7.3 How Long Should Children Receive Medical Therapy?
|
ESPGHAN |
1. Based on expert opinion, maintenance treatment should continue for at least 2 months. All symptoms of constipation symptoms should be resolved for at least 1 month before discontinuation of treatment. Treatment should be decreased gradually. 2. Based on expert opinion, in the developmental stage of toilet training, medication should only be stopped once toilet training is achieved. |
Low |
Conditional
|
|
Question 8: What Is the Efficacy and Safety of Novel Therapies for Children with Intractable Constipation? |
Q 8.1 Transcutaneous Nerve Stimulation (TNS) |
ESPGHAN |
Based on expert opinion, evidence does not support the use of TNS in children with intractable constipation. |
Low |
Conditional
|
|
|
Q 8.2 Surgery (use of ACE) |
ESPGHAN |
Based on expert opinion, we recommend antegrade enemas in the treatment of selected children with intractable constipation. |
Very low |
Conditional
|
|
|
Question 9.1 What is the prognosis of functional constipation in children? |
ESPGHAN |
· Among patients referred to pediatric gastroenterologists 1. 50% will recover and be without laxatives after 6 to 12 months. 2. 10% are well while taking laxatives. 3. 40% will still be symptomatic despite use of laxatives. · 50% and 80% of the children are recovered after 5 and 10 years, respectively.
delay in initial medical treatment for >3 months from symptom onset correlates with longer duration of symptoms. |
Low |
Conditional
|
|
|
Question 9.2 What are prognostic factors in children with functional constipation? |
ESPGHAN |
Based on expert opinion, we recommend using the following to identify the prognostic factors related to functional constipation. There is limited /insufficient evidence relative to the prognostic value of functional constipation of the following factors 1. Demographics/history: age at presentation, age at onset, duration of symptoms< 3 months before presentation, treatment duration< 2 month before presentation, premature birth, delayed passage of meconium, history of constipation in the first year of life 2. Clinical symptoms: defecation frequency, presence of fecal incontinence, abdominal pain at presentation/history of abdominal pain, large stools, urinary tract infection, nighttime urinary incontinence, stool withholding 3. Physical examination: absence of a rectal or abdominal mass 4. Additional examination: balloon defecation, relaxation of external sphincter, megarectum and/or megacolon at diagnosis
There is limited evidence for a negative prognostic value for Additional examination: prolonged CTT (colonic transit time) There is strong evidence that the following factors have no prognostic value Demographics: sex, positive family history |
Limited evidence in some and Strong evidence for other prognostic factors |
|
➡️Evidence to recommendations: Considerations
The GDG/ GAG was guided by the results of the AGREE II appraisals of the eligible CPGs and thoroughly reviewed the recommendations of the original source WHO CPGs in consideration of local contextual factors related to the national Egyptian health system like burden of the disease, equity, acceptability, feasibility, and other relevant factors. The GDG decided through an informal consensus process to adopt most recommendations however, there was a need to change the strength of 2 recommendations (B2 and B3) as they lack feasibility. Also, GDG/ GAG develops group of good practice statements to improve acceptability and feasibility.
- Acknowledgements
· The GDG/ GAG acknowledge EPG for its help in completing this project.
· We acknowledge ESPGHAN and NASPGHAN: JPGN 2014;58: 258–274 CPGs guidelines (the source original guidelines) for their cooperation in providing the permission for adapting our guidelines.
· Finally, we wish the best for all our patients and their families who inspired us. It is for them this work is being finalized.
Funding
This work is not related to any pharmaceutical or industrial company. The members of the GDG/ GAG and their institutes and universities volunteered their participation and contributions.|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Development/ Adaptation Group (Clinicians subgroup) |
|||||
|
Name |
Affiliation, Area of expertise / Country / Primary location [work] |
Contribution |
|||
|
Prof. Suzan Samir Gad |
Pediatrics Department, Consultant, Suez Canal |
Clinical Chair, GAG |
|||
|
Prof. Ahmed Foad |
Alexandria |
Clinical Expert GAG Member |
|||
|
Prof. Ahmed Hamdy |
Ain Shams |
Clinical Expert GAG Member |
|||
|
Prof. Amal Mahfouz |
Alexandria |
Clinical Expert GAG Member |
|||
|
Prof. Ayman Emil Eskandr |
Cairo |
Clinical Expert GAG Member |
|||
|
Prof. Gihan Bebars |
Minia |
Clinical Expert GAG Member |
|||
|
Prof. Hala Hussien Mansour |
Cairo |
Clinical Expert GAG Member |
|||
|
prof. Maha Abou Zekri |
Cairo |
Clinical expert GAG Member |
|||
|
Prof. Mohamed Ezz |
Mansoura |
Clinical Expert GAG Member |
|||
|
Prof. Naglaa Abu Faddan |
Assuit |
Clinical Expert GAG Member |
|||
|
Prof. Hossam El Saadny |
|
Clinical Expert GAG Member |
|||
|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Development/ Adaptation Group (Guideline Methodologists subgroup) |
|||||
|
Name |
Affiliation, Area of expertise / Country / Primary location [work] |
Contribution |
|||
|
Prof. Ashraf Abdel Baky |
Professor of Pediatrics Ain Shams University, Egypt Founder and Chair of EPG |
Overseeing the adolopment process of the guidelines, training and education of new members, revision of the final draft, and organizing online meetings of GDG |
|||
|
Dr. Yasser Sami Amer |
1. Pediatrics Department and Clinical Practice Guidelines and Quality Research Unit, Quality Management Department, King Saud University Medical City, Riyadh, Saudi Arabia; 2. Research Chair for Evidence-Based Health Care and Knowledge Translation, King Saud University, Riyadh, Saudi Arabia; 3. Chair, Adaptation Working Group, Guidelines International Network (GIN), Perth, Scotland 4. Department of Internal Medicine, Ribeirão Preto Medical School, University of São Paulo (FMRP-USP), Ribeirão Preto, São Paulo, Brazil. |
Overseeing the adolopment process of the guidelines, training and education of new members, participating in writing up the methodology of adaptation process, guideline appraisal, and revision of the final draft |
|||
|
Lecturer of pediatrics, Faculty of Medicine, Modern University for Technology and Information (MTI), Egypt |
Participating in multiple steps of the guideline adaptation process, Writing the methodology of adaptation process and revised the whole document. |
||||
|
External Reviewers Group (ERG) |
|||||
|
External Reviewer(s) for Clinical Content |
|||||
|
|||||
|
International Peer Reviewers |
|||||
|
External Reviewer(s) for methodology |
|||||
|
Prof. Iván D. Flórez |
Department of Pediatrics, University of Antioquia, Medellín, Colombia, Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Canada, Leader, AGREE Collaboration (Appraisal of Guidelines for Research & Evaluation) Director, Cochrane Colombia |
||||
|
Prof. Airton Tetelbom Stein
|
Professor Titular de Saúde Coletiva, Fundação Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), Porto Alegre, Brazil Professor Adjunto, Universidade Luterana do Brasil (Ulbra), Canoas, Brazil Coordenador de Diretrizes Clínicas, Grupo Hospitalar Conceição, Porto Alegre, Brazil 4. Member, Board of Trustees, Guidelines International Network (G-I-N) |
||||
- Abbreviations
|
Adolopment |
Adoption-Adaptation-Development |
||
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation Instrument |
||
|
ARM |
anorectal manometry |
||
|
CTT |
Colonic transit time |
||
|
CPG |
Clinical Practice Guideline |
||
|
DHS |
Demographic and Health Survey |
||
|
EPG |
Egyptian Pediatrics Clinical Practice Guidelines Committee |
||
|
EPG CPG |
EPG Clinical Practice Guideline |
||
|
ERG |
External Review Group |
||
|
GAG |
Guideline Adaptation Group |
||
|
GDG |
Guideline Development Group |
||
|
GPS |
Good Practice Statement |
||
|
GRADE |
Grading of Recommendations Assessment, Development and Evaluation |
||
|
Hd |
Hirschsprung disease |
||
|
MRI |
magnetic resonance imaging |
||
|
PEG |
Polyethlene glycol |
||
|
PICO |
population, intervention, comparison, and outcomes |
||
|
Patient population, intervention, professionals, outcomes, and healthcare context |
||
|
RIGHT |
A Reporting Tool for Practice Guidelines in Health Care |
- Introduction
Functional constipation is a common problem in children. Although some guidelines exist for management of childhood constipation (1) there are no such guidelines for Egyptian children.
Functional constipation constituted 30% of pediatric gastroenterology outpatient practice, 4-5% of all referrals to pediatric gastroenterology tertiary care centers and 0.8-1% of all pediatric cases in medical colleges (1).
Normal stool frequency is; <1-month age: 3-4 times/day; 1 month to 1-year age: 1.5-2 times/day; 1 to 2-year age: 1-2 times/day, mostly formed; older than 2-year age: 1 time/day. While constipation is a delay or difficulty in defecation sufficient to cause significant distress to the patient (3,4).
When the duration of constipation is less than 4 weeks, it is considered as acute constipation and when the duration is more, it is chronic constipation; in addition to two or more of the following criteria: (a) defecation frequency ≤2 times per week, (b) fecal incontinence ≥1 times per week after the acquisition of toileting skills, (c) history of excessive stool retention, (d) history of painful or hard bowel movements, (e) presence of a large mass in the rectum or on per abdomen examination, (f) history of large-diameter stools that may obstruct the toilet (7).
The term “Fecal Incontinence”, currently used instead of the terms soiling or encopresis, is defined as passage of stools in the undergarment and is classified as: (a) Constipation-associated fecal incontinence and (b) non-retentive fecal incontinence: diagnosed only if there is no constipation and normal anal sphincter tone, and symptoms last for more than 2 months in a child with a developmental age of ≥4 years (1).
The term “Refractory constipation” is defined as constipation not responding to optimal conventional treatment for at least 3 months, despite good compliance. These patients should be referred to a pediatric gastroenterologist for evaluation (2).
History and examination are relevant in making a diagnosis of constipation and differentiating functional and organic constipation as follows: Dietary history; like intake of fruits and vegetables and refined foods (e.g., bakery), beverages etc. in older children, nature of feeds (breast vs top feeds) and details of supplementary feeds in younger babies, exclusive and prolonged milk intake with minimal solids in young infants, In addition to evidence of important precipitating factors of functional constipation;, (a) premature initiation of toilet training (normally toilet training should start not before 24 months in a developmentally normal child) (b) drugs and inter-current illnesses, (c) quick and abrupt transition of diet e.g. liquid to solid, breastfeeding to bottle feeding and (d) change in local environment (start of schooling) and psychosocial factors (3,5,6).
Characteristics of functional constipation in infants up to 4 years must include 2 or fewer defecations per week or 1 month of at least 2 of the following: (a) History of excessive stool retention, (b) History of painful or hard bowel movements, (c) History of large-diameter stools, (d) Presence of a large fecal mass in the rectum. While in toilet-trained children, the following additional criteria may be used: (a) At least 1 episode/week of incontinence after the acquisition of toileting skills, (b) History of large-diameter stools that may obstruct the toilet. Children greater than four years must have 2 or more of the following occurring at least once per week for a minimum of 1 month with insufficient criteria for a diagnosis of irritable bowel syndrome: (a) 2 or fewer defecations in the toilet per week in a child of a developmental age of at least 4 years, (b) At least 1 episode of fecal incontinence per week, (c) History of retentive posturing or excessive volitional stool retention, (d) History of painful or hard bowel movements, (e) Presence of a large fecal mass in the rectum, (f) History of large diameter stools that can obstruct the toilet (7).
Organic causes of constipation include; Abnormalities of the colon and rectum (e.g., chronic intestinal pseudoobstruction, anal stenosis, anal/colonic stricture, post NEC/IBD and ectopic anus), Neuropathic lesions (e.g., Hirschsprung disease and intestinal neuronal dysplasia), Spinal cord lesions (e.g., spina bifida, meningomyelocele, sacral agenesis, tethered cord and tumors), Metabolic (e.g., hypothyroidism, hypo/hyper-calcemia, hypokalemia and uremia), Systemic disorders (e.g., celiac disease, cystic fibrosis and diabetes mellitus) and Drugs (e.g., analgesics, anticholinergics, iron, sympathomimetics, psychotropics, NSAIDs and antacids) (6 ).
The aim of this adapted clinical practice guideline (CPG) is to provide evidence-based recommendations for for diagnosis and treatment of functional constipation in infants and children.These recommendations were adapted from the relevant evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN: JPGN 2014;58: 258–274 CPG(s) using a formal methodology for CPG adaptation: the Adapted-ADAPTE.
- Purpose and Scope
These guidelines have been developed to standardize the delivery of services and to implement the guidance on the prevention, diagnosis and management of Functional Constipation. It provides guidance to primary health care providers, pediatricians and specially trained nurses.
The guidelines aimed to diagnose and treat functional constipation in infants and young children.
This version of the guideline includes recommendations and good practice statements for functional constipation in infants and young children.
Disease/Condition:
Guideline Objective(s)
Diagnosis and treatment of functional constipation in infants and children
Health / Clinical Question (PIPOH)
P: Patient (Target Population):
Gender: Both genders
Age group: infants and children from 1-18 years
Disease/condition: functional constipation in infants and children
I: Interventions and Practices Considered / CPG Category:
Clinical: history taking and examination
Laboratory investigations:
• laboratory investigations to diagnose (cow’s milk) allergy, celiac disease, hypothyroidism, and hypercalcemia
• abdominal radiography (use of barium enema to diagnose organic causes such as hd
• colonic transit time (ctt)
• transabdominal rectal ultrasonography
• magnetic resonance imaging (mri) of the spine
• colonic manometry
• anorectal manometry (arm) or rectal suction biopsy to diagnose hd
• colonic full-thickness biopsies
• treatment
P: Professionals (Intended / Target Users or Stakeholders) :
Primary health care physician
General practitioners
Family physician
Pediatrician
Gastroenterologist
O: Major Outcomes Considered:
Primary outcome: proper diagnosis of functional constipation
Secondary outcome: proper treatment of functional constipation
H: Healthcare Settings:
Types:
primary, secondary and tertiary healthcare centers.
•governmental healthcare sector:
moh, university, military, health insurance organization
•non-governmental healthcare sector:
private and NGO healthcare centers.
- Methods
➡️Methods of search:
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation. Keywords used for search are: functional constipation, Hirschsprung disease, infants, young children.
Inclusion / exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on methodology of development including the systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated 2013 and later or the last 5 years)
• Selecting peer-reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author
➡️The following three categories of databases and websites were searched:
1. CPG databases and libraries (e.g., GIN, ECRI, SIGN, DynaMed, BIGG-REC PAHO)
2. Bibliographic databases (e.g., PubMed, Google Scholar)
3. Specialized professional societies (related to the pediatric subspecialty)
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least two members. The panel decided a cut-off point or rank the guidelines (any guideline scoring above 60% on the rigor dimension was retained)
After reviewing all the previous criteria, the GDG/ GAG recommended using 1 guideline:
1- Evidence-Based Recommendations from ESPGHAN and NASPGHAN: JPGN 2014
We did Adolopment for these guidelines: (Adoption, Adaptation, and Development)
- Adoption for most of the guideline recommendations.
- Development of Good Practice Statement
➡️Contributors to the guideline development process:
Guideline Development Group (GDG)/ Guideline Adaptation Group (GAG):
The GDG/ GAG included two subgroups; the clinicians/ healthcare providers subgroup and the guideline methodologists’ subgroup.
➡️Clinicians Subgroups
The clinicians’ subgroup or clinical panel for this guideline included experts with a range of knowledge, technical skills and diverse perspectives in the field of functional constipation
The main functions of the clinical panel were adolopment of Evidence-Based Recommendations from ESPGHAN and NASPGHAN: JPGN 2014. Guidelines, determining the scope of the guideline and guideline, reviewing the evidence, and formulating evidence-informed recommendations in case of changing strength of recommendations.
➡️Guideline Methodologists Subgroup
There were 7 guideline methodologists with expertise in guidelines development, adaptation, GRADE and translation of evidence into recommendations. Methodologists provided orientation and overview of evidence-informed guideline development processes using the GRADE approach, guideline adaptation using the Adapted ADAPTE, provided AGREE II assessment of the source guidelines in collaboration with the clinician’s subgroup, generation of the EtD frameworks whenever applicable.
➡️External Review Group:
The External Review Group for this guideline comprises 3 clinical national experts who have interest and expertise in as well as eminent international reviewers.
They were identified by Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) as people who can provide valuable insights during the guideline development process.
The External Review Group was asked to comment on (peer review) the final guideline to identify any criticism on the content and to comment on clarity and applicability as well as issues relating to implementation, dissemination, ethics, regulations, or monitoring, but not to change the recommendations formulated by the GDG/ GAG. The members of the External Review Group were required to submit declarations of interest before the peer review process.
➡️Guideline Development/ Adaptation Group meetings:
GDG/ GAG meetings were organized virtually (weekly/bimonthly). Due to the extensive scope of
the guideline, EPG was responsible for overseeing the adolopment process. the timetable and objectives of each meeting. GDG/ GAG meetings were also attended by members of the methodologists. Working rules for each contributor type were outlined by the chair at the start of each meeting, covering aspects such as vocal rights, voting, and evidence to decision and recommendation formulating processes.
➡️Declarations of interests:
Prospective members of the GDG/ GAG were asked to fill in and sign the standard WHO declaration of interest and confidentiality undertaking forms. All guideline members and methodologists were also asked to fill in and sign the standard WHO declaration-of-interests.
Members of the external review group will be asked to fill in and sign the standard WHO declaration-of-interests form before the peer review process.
- Evidence for the guideline
We used the GRADE system (Grading of Recommendations, Assessment, Development and Evaluation) for assigning the quality of evidence and strength of recommendations that includes the following definitions [13]. Informed by the evidence required for the GRADE Evidence to Decision (EtD) framework(s) was(were) done while considering changing strength of recommendations according to availability of some resources in the recommendations.
Description of the interpretation of the GRADE four levels of certainty of evidence:
Table 1. Classification of the Quality of Evidence
|
High |
We are very confident that the true effect lies close to that of the estimate of the effect. |
|
Moderate |
We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. |
|
Low |
Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. |
|
Very Low |
We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of the effect. |
GRADE EtD’s contextual factors, criteria and considerations that link to the strength of recommendations:
Criteria and Considerations:
1. Benefits and harms: When a new recommendation is developed, desirable effects (benefits) need to be weighed against undesirable effects (risks/harms), considering any previous recommendation or another alternative. The larger the gap or gradient in favor of the desirable effects over the undesirable effects, the more likely that a strong recommendation will be made.
2. Certainty of the evidence about the effects: The higher the certainty of the scientific evidence base, the more likely that a strong will be made.
3. Values and preferences: If there is no important uncertainty or variability in how much people value the main outcomes, it is likely that a strong recommendation will be made. Uncertainty or variability around these values that could likely lead to different decisions, is more likely to lead to a conditional recommendation.
4. Economic implications: Lower costs (monetary, infrastructure, equipment or human resources) or greater cost-effectiveness are more likely to support a strong recommendation.
5. Equity and human rights: If an intervention will reduce inequities, improve equity or contribute to the realization of human rights, the greater the likelihood of a strong recommendation.
6. Feasibility: The greater the feasibility of an intervention to all stakeholders, the greater the likelihood of a strong recommendation.
7. Acceptability: If a recommendation is widely supported by health workers and program managers and there is widespread acceptance for implementation within the health service, the likelihood of a strong recommendation is greater.
Table 2. Classification of the Strengths of Recommendations
|
Strong |
The desirable effects of an intervention clearly outweigh the undesirable effects (or vice versa), so most patients should receive the recommended course of action. |
|
Conditional |
There is uncertainty about the trade-offs. The clinician and patient need to discuss the patient's values and preferences, and the decision should be individualized. |
Developing good practice statements:
The GDG/ GAG also developed good practice statements for this guideline, which are actionable messages relevant to the guideline questions. The justification for each good practice statement was carefully considered by the GDG/ GAG with an emphasis that they are clearly needed. Good practice statements were developed, guided by the following GRADE criteria:
1- Message is really necessary with regard to actual healthcare practice
2- Have large net positive consequence (relevant outcomes and downstream consequences) (GRADE EtD domains)
3- Collecting and summarizing the evidence is a poor use of time and resources
4- Include a well-documented, clear rationale connecting indirect evidence
5- Are clear and actionable statements.
The GDG/ GAG collectively drafted and finalized good practice statements with relevant justifications and remarks to help with their interpretation, with close support and input from the consultant and guideline methodologists.
We have used the Reporting Items for Practice Guidelines in Healthcare (RIGHT) extension for adapted guidelines (RIGHT-Ad@pt Tool) as a reporting checklist for this guideline adaptation process as recommended by the EQUATOR network.
- Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing functional constipation diagnosis, treatment, and prevention strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of nutritional care delivery, care gaps and current needs.
1. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
2. Identify barriers to, and facilitators of implementation.
3. Select an implementation framework and its component strategies.
4. Develop a step-by-step implementation plan:
· Select the target populations and evaluate the outcome.
· Identify the local resources to support the implementation.
· Set timelines.
· Distribute the tasks to the members.
· Evaluate the outcomes.
5. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
· Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
· Educational materials: printed or electronic information (software).
·Web-based education: computer-based educational activities.
· A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
· Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
· Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
· Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
· Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
· Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behaviors.
· Mass media campaigns.
3. For Nurses
· Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
· Educational materials: printed.
· A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
· Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
· Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
· Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
· Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
· Administrative policies and procedures.
· Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
· International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
· Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
➡️Guideline Implementation Tools
Educational materials based on this Adapted CPG for treatment of CAP in children have been made available in several forms including:
1. Manual for physician for diagnosis and algorithm for management of acute malnutrition
3. Arabic Educational materials for nurses and mothers
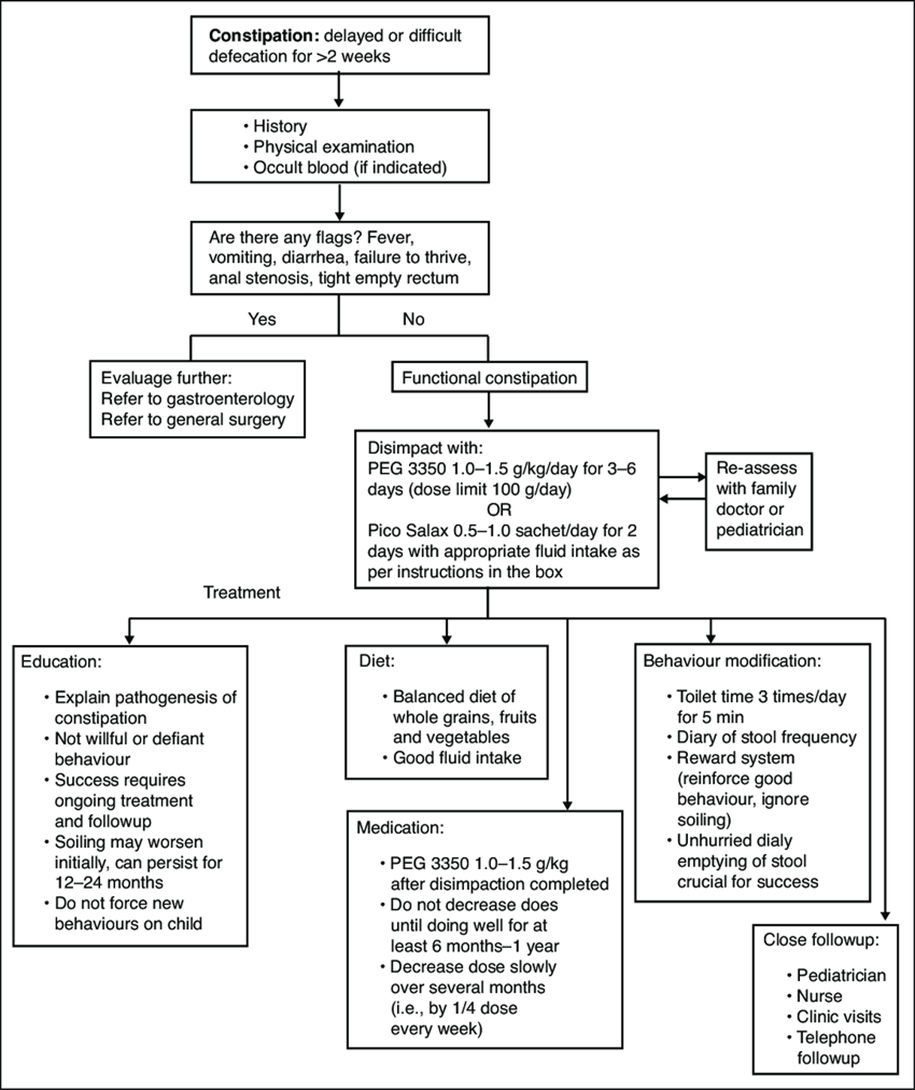
The CPG adaptation group decided to adopt all of the CPG implementation tools proposed by member group including the following: -
Constipation treatment algorithm. Adapted from The Hospital for Sick Children constipation fluxogram 2013.
Parent and carer health educational guide (in Arabic) ازاي تعرفي أن ابنك عنده امساك ؟- لو بيعمل براز أقل من ٣ مرات في الأسبوع أو لو البراز ناشف جدا أو لو بيتالم أو يبكي أثناء التبرز
· ده معناه ايه ؟ انك لازم تتابعي عملية التبرز و خصوصا .لما يكبر شوية و يبدأ يدخل الحمام لوحده اوقات كتير تيجي الام تشتكي من طفلها عنده مغص و الام مستمرة في البطن و لما نسأل عن التفاصيل نلاقي أن الطفل عنده امساك بيعمل حمام كل ٣-٤ ايام و الام .فاكرة أن دي طبيعته عادي
· ٣ مراحل مهمة في حياة الطفل يكثر فيها حدوث - : الإمساك لازم تاخدي بالك منهم
١ -عند سن ٦ شهور مع ادخال طعام الفطام
٢ -عند سن ٥.٢-٣ سنوات مع تدريب الطفل علي استعمال الپوتي أو التواليت حيث يبدأ في رفض التدريب في البداية
٣ -عند دخول المدرسة حيث يبدأ الطفل في رفض استعمال حمام المدرسة في كل مرحلة لازم نخلي بالنا .
· عند ادخال طعام الفطام لازم اهتم بوجود عناصر غذائية ملينة زي الكوسة و . القرع و الفاكهة الملينة سواء عنب أو كونتالوب مثلا و في المرحلة التانية لابد من الصبر علي الطفل أثناء عملية التدريب و إعطاؤه الوقت الكافي للتدريب و برضه الحفاظ علي نوعية الطعام زي ما قلنا سابقا . و في المرحلة دي انواع الاطعمة بتزيد . يعني مثلا بدل ما يتعود ياكل عيش فينو طول الوقت
· لازم يتعود ياكل عيش بلدي المحتوي علي الردة و هي ألياف هامة .
· لازم يتعود ياكل خيار او طماطم او خس ... يا منفردة يا في صورة سلطة .
· برجاء عدم إدخال عصائر السوبرماركت و شيبسي و خلافه و كيك و بسكوتات....
· و هكذا في المرحلة التالثة لازم تشجعه أنه يدخل حمام المدرسة حين يشعر أنه يحتاج الي دخول الحمام و اعطيه مطهر و مناديل ورقية و قاعدة حمام بلاستيكية و اعلمه كيفية التعامل مع الحمامات العامة في البيت
· لازم اعود طفلي أنه يدخل الحمام ٣ مرات في اليوم بعد الاكل حتي لو لم يكن يرغب في الدخول لمدة ١٠ دقائق و إذا شعر في اي وقت بالرغبة في دخول الحمام يدخل فورا لان الاحساس بالرغبة في التبرز يختفي بعد قليل و إذا تكرر الأمر فيحدث ما نسميه امساك تعودي
· لازم برضه نخلي بالنا أن الأطفال لاترغب في ترك اللعب مع الاخوات و الأقارب و الاصدقاء و حاليا في اللعب بالاجهزة الإلكترونية لتضيع وقتها في دخول الحمام فلابد من ملاحظة ذلك
· و طبعا التوجه للطبيب ضروري في أي مرحلة لان هناك بعض الأمراض تبدأ بالامساك و قد يضطر لإعطاء الطفل بعض الأدوية لتسهيل عملية التبرز و برجاء عدم ايقاف الأدوية الا تحت إشراف الطبيب حيث أن الامساك قد يحتاج لفترات طويلة لعلاجه.
Rome III diagnostic criteria for functional constipation
In the absence of organic pathology, >2 of the following must occur
For a child with a developmental age <4 years*
1. <2 defecations per week
2. At least 1 episode of incontinence per week after the acquisition of toileting skills
3. History of excessive stool retention
4. History of painful or hard bowel movements
5. Presence of a large fecal mass in the rectum
6. History of large-diameter stools that may obstruct the toilet
· Accompanying symptoms may include irritability, decreased appetite, and/or early satiety, which may disappear immediately following passage of a large stool
For a child with a developmental age >4 years with insufficient criteria for irritable bowel syndrome #
1. <2 defecations in the toilet per week
2. At least 1 episode of fecal incontinence per week
3. History of retentive posturing or excessive volitional stool retention
4. History of painful or hard bowel movements
5. Presence of a large fecal mass in the rectum
6. History of large-diameter stools that may obstruct the toilet.
*Criteria fulfilled for at least 1 month. Adapted from Hyman et al (12)
#Criteria fulfilled at least once per week for at least 2 months before diagnosis. Adapted from Rasquin et al (13)
- Limitations and suggestions for further research needs
Future research recommendations for the management of functional constipation in children the Egyptian context could include:
· Epidemiological studies regarding functional constipation on Egyptian children
These recommendations aim to address specific challenges and characteristics of the Egyptian context, potentially leading to more effective prevention and management strategies for functional constipation in children.
➡️Challenges
· Most of the recommendations depend on the clinical experience of the clinician to make a decision
· Patients need a long term follow up for functional constipation as recovery is achieved after a very long time.
· Strengthen the evidence base of the next update of this guideline by generating GRADE summary of finding tables, evidence profiles, and EtD frameworks.
Monitoring and evaluating the impact of the guideline.
The following are three performance measures or indicators for implementing this adapted CPG for functional constipation in children:
1. Adherence to functional constipation Guidelines
· Numerator: Number of children with functional constipation who received treatment as per guideline recommendations.
· Denominator: Total number of children diagnosed with functional constipation
· Data Source: Hospital or clinic patient records.
2. Duration of Hospital Stay
· Numerator: Total number of hospitals stay days for children with functional constipation
· Denominator: Total number of children admitted with functional constipation
· Data Source: Hospital admission and discharge records.
These key performance indicators are designed to measure the effectiveness and adherence to the guidelines, the efficiency of the treatment in terms of resource utilization (hospital stay), and the success of the treatment in preventing further complications (readmissions).
- Updating of the guideline
The EPG functional constipation GAG has decided to conduct the next review of this adapted CPG for updates after five years. This should be carried out in 2029 after checking for updates in the source CPGs, consultation of expert opinion on the changes needed for updating according to the newest evidence and recommendations published in this area and the clinical audit and feedback from implementation efforts in the aforementioned local healthcare settings except if any breakthrough evidence- based recommendations are published before that date. The process will be guided by the Checklist for the Reporting of Updated Guidelines (CheckUp) Tool that is freely provided by the AGREE Enterprise and by the Reporting Items for Practice Guidelines in Healthcare (RIGHT) extension for adapted guidelines RIGHT-Ad@pt Checklist.
- References
- Yachha SK, Srivastava A, Mohan N, Bharadia L, Sarma MS. Management of childhood functional constipation: consensus practice guidelines of Indian Society of Pediatric Gastroenterology, Hepatology and Nutrition and Pediatric Gastroenterology Chapter of Indian Academy of Pediatrics. Indian Pediatr. 2018 Oct 15;55(10):885-892.
- Tabbers MM, DiLorenzo C, Berger MY, Faure C, Langen-dam MW, Nurko S, et al. Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr. 2014;58:258-74.
- Sujatha B, Velayutham DR, Deivamani N, Bavanandam S. Normal bowel pattern in children and dietary and other precipitating factors in functional constipation. J Clin Diag Res. 2015;9:SC12-5.
- Yadav M, Singh PK, Mittal SK. Variation in bowel habits of healthy Indian children aged up to two years. Indian J Pediatr. 2014;81:446-9.
- Chen SL, Cai SR, Deng L, Zhang XH, Luo TD, Peng JJ, et al. Efficacy and complications of polyethylene glycols for treatment of constipation in children: A meta-analysis. Medicine (Baltimore). 2014;93:e65.
- Bardisa-Ezcurra L, Ullman R, Gordon J. Diagnosis and management of idiopathic childhood constipation: Summary of NICE Guidance. BMJ. 2010;340:c2585.
- Zeevenhooven J, Koppen IJ, Benninga MA. The New Rome IV Criteria for Functional Gastrointestinal Disorders in Infants and Toddlers. Pediatr Gastroenterol Hepatol Nutr.
2017;20(1):1-13
12. Abdel Baky A, Omar TEI, Amer YS; Egyptian Pediatric Clinical Practice Guidelines Committee (EPG). Adapting global evidence-based practice guidelines to the Egyptian healthcare context: the Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) initiative. Bull Natl Res Cent. 2023;47(1):88. https://doi.org/10.1186%2Fs42269-023-01059-0
13. Alshehri A, Almazrou S, Amer Y. Methodological frameworks for adapting global practice guidelines to national context in the Eastern Mediterranean Region. Eastern Mediterranean Health Journal. 2023 Jul 1;29(7). https://www.emro.who.int/emhj-volume-29-2023/volume-29-issue-7/methodological-frameworks-for-adapting-global-practice-guidelines-to-national-context-in-the-eastern-mediterranean-region.html
14. Schünemann H, Brozek J, Guyatt G, Oxman A (editors). GRADE handbook: handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group; 2013 (Online updated version: https://gdt.gradepro.org/app/handbook/handbook.html Accessed 16/8/2024)
15. Klugar M, Lotfi T, Darzi AJ, et al. GRADE Guidance 39: Using GRADE-ADOLOPMENT to adopt, adapt or create contextualized recommendations from source guidelines and evidence syntheses. Journal of Clinical Epidemiology. 2024 Aug 6:111494. https://doi.org/10.1016/j.jclinepi.2024.111494 (in press)
16. Amer YS, Elzalabany MM, Omar TI, Ibrahim AG, Dowidar NL. The ‘Adapted ADAPTE’: an approach to improve utilization of the ADAPTE guideline adaptation resource toolkit in the A lexandria C enter for E vidence‐B ased C linical P ractice G uidelines. Journal of evaluation in clinical practice. 2015 Dec;21(6):1095-106. https://doi.org/10.1111/jep.12479
17. Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. https://doi.org/10.1503%2Fcmaj.090449
18. Agree II (2022) AGREE Enterprise website. Available at: https://www.agreetrust.org/resource-centre/agree-ii/ (Accessed: 16/8/2024).
19. Song Y, Alonso-Coello P, Ballesteros M, et al. A Reporting Tool for Adapted Guidelines in Health Care: The RIGHT-Ad@pt Checklist[J]. Annals of Internal Medicine, 2022, 175(5):710-719. https://doi.org/10.7326/M21-4352 (Official RIGHT Statement Website: http://www.right-statement.org/extensions/13 Accessed 16/8/2024)
- Annexes
Annex Table 1.
Declaration of Conflict of Interests
The members of the guideline development/ adaptation group and the external review group have no academic, financial, or competing interests to declare and none of them were involved in the development of the original source guideline(s).
Any identified potential COI has been reported below.
|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Development/ Adaptation Group (Clinicians subgroup) |
|||||
|
Name |
Affiliation, Area of expertise / Country / Primary location [work] |
Contribution |
|||
|
Prof. Suzan Samir Gad |
Pediatrics Department, Consultant, Suez Canal |
Clinical Chair, GAG |
|||
|
Prof. Ahmed Foad |
Alexandria |
Clinical Expert GAG Member |
|||
|
Prof. Ahmed Hamdy |
Ain Shams |
Clinical Expert GAG Member |
|||
|
Prof. Amal Mahfouz |
Alexandria |
Clinical Expert GAG Member |
|||
|
Prof. Ayman Emil Eskandr |
Cairo |
Clinical Expert GAG Member |
|||
|
Prof. Gihan Bebars |
Minia |
Clinical Expert GAG Member |
|||
|
Prof. Hala Hussien Mansour |
Cairo |
Clinical Expert GAG Member |
|||
|
prof. Maha Abou Zekri |
Cairo |
Clinical expert GAG Member |
|||
|
Prof. Mohamed Ezz |
Mansoura |
Clinical Expert GAG Member |
|||
|
Prof. Naglaa Abu Faddan |
Assuit |
Clinical Expert GAG Member |
|||
|
Prof. Hossam El Saadny |
|
Clinical Expert GAG Member |
|||
|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Development/ Adaptation Group (Guideline Methodologists subgroup) |
|||||
|
Name |
Affiliation, Area of expertise / Country / Primary location [work] |
Contribution |
|||
|
Prof. Ashraf Abdel Baky |
Professor of Pediatrics Ain Shams University, Egypt Founder and Chair of EPG |
Overseeing the adolopment process of the guidelines, training and education of new members, revision of the final draft, and organizing online meetings of GDG |
|||
|
Dr. Yasser Sami Amer |
1. Pediatrics Department and Clinical Practice Guidelines and Quality Research Unit, Quality Management Department, King Saud University Medical City, Riyadh, Saudi Arabia; 2. Research Chair for Evidence-Based Health Care and Knowledge Translation, King Saud University, Riyadh, Saudi Arabia; 3. Chair, Adaptation Working Group, Guidelines International Network (GIN), Perth, Scotland 4. Department of Internal Medicine, Ribeirão Preto Medical School, University of São Paulo (FMRP-USP), Ribeirão Preto, São Paulo, Brazil. |
Overseeing the adolopment process of the guidelines, training and education of new members, participating in writing up the methodology of adaptation process, guideline appraisal, and revision of the final draft |
|||
|
Dr. Nahla Gamaleldin |
Lecturer of pediatrics, Faculty of Medicine, Modern University for Technology and Information (MTI), Egypt |
Participating in multiple steps of the guideline adaptation process, Writing the methodology of adaptation process and revised the whole document. |
|||
|
External Reviewers Group (ERG) |
|||||
|
External Reviewer(s) for Clinical Content |
|||||
|
|||||
|
International Peer Reviewers |
|||||
|
External Reviewer(s) for methodology |
|||||
|
Prof. Iván D. Flórez |
Department of Pediatrics, University of Antioquia, Medellín, Colombia, Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Canada, Leader, AGREE Collaboration (Appraisal of Guidelines for Research & Evaluation) Director, Cochrane Colombia |
||||
|
Prof. Airton Tetelbom Stein
|
Professor Titular de Saúde Coletiva, Fundação Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), Porto Alegre, Brazil Professor Adjunto, Universidade Luterana do Brasil (Ulbra), Canoas, Brazil Coordenador de Diretrizes Clínicas, Grupo Hospitalar Conceição, Porto Alegre, Brazil 4. Member, Board of Trustees, Guidelines International Network (G-I-N) |
||||
Web annexes
The following annexes can be added as a package of standalone supplementary documents.
Keywords: The MeSH terms for "Guideline for the diagnosis and treatment of functional constipation in infants and children
on PubMed are: functional, constipation, infants, young children, Hirschsprung disease
Appendix Table 2. AGREE II assessment results and the standardized domain scores for the one ESPGHAN and NASPGHAN: JPGN 2014 included CPG
|
CPGs AGREE II DOMAINS |
CPG1 |
|
D1: Scope & Purpose |
93% |
|
D2: Stakeholder Involvement |
82.5% |
|
D3: Rigour of Development |
83.7% |
|
D4: Clarity & Presentation |
90.5% |
|
D5: Applicability |
83.6% |
|
D6: Editorial Independence |
88% |
|
OA 1 |
80% |
|
OA 2 (Recommend for use) |
Yes (all) |
This table uses the AGREE II Domain Score Color codes (< 40% red; > 41 – 70% yellow; > 71 % green)
Based on the results of the AGREE II assessment, the GAG decided to adapt/ adopt all of the recommendations from the XXXXXXXXXXXXXXXXXX CPG.
Appendix Table 3. Currency survey of the CPG developer
|
1. Are you aware of any new evidence relevant to this CPG statement? Yes/ No |
|
2. Is there any new evidence to invalidate any of the recommendations comprising the CPG? Yes/ No |
|
3. Are there any plans to update the CPG in the near future? Yes/ No |
|
4. When the CPG was last updated? XX/XX/XXXX What is the citation for the latest version? See Reference XXXXXXXXXX |
Annex Table 3. Annex Nurses and Parents Educational Guide in Arabic
Appendix Table 4. Decision Support for EPG Adaptation Working Group for CPG for ‘Management of diagnosis and treatment of functional constipation in infant and children. Chairperson: Dr. suzan samer gad
|
PHASE |
MODULE |
STEP |
TOOL |
DECISION |
REASON (if not utilized) |
||||
|
Utilized |
Not utilized |
||||||||
|
ONE: SET-UP |
1.1. Preparation |
1 |
1 |
√ |
|
|
|||
|
2 |
√ |
|
|
||||||
|
2 |
|
√ |
|
|
|||||
|
3 |
|
√ |
|
|
|||||
|
4 |
|
√ |
|
|
|||||
|
5 |
3 |
√ |
|
|
|||||
|
4 |
√ |
|
|
||||||
|
1 |
√ |
|
|
||||||
|
6 |
5 |
√ |
|
|
|||||
|
|
|||||||||
|
TWO: ADAPTATION |
2.1. Scope and Purpose |
7 |
6 |
√ |
|
|
|||
|
2.2. Search and Screen |
8 |
2 |
√ |
|
|
||||
|
7 |
√ |
|
|
||||||
|
9 |
8 |
√ |
|
|
|||||
|
10 |
9 |
|
√ |
Decided to rely on inclusion/ exclusion criteria (filters) & PIPOH compatibility |
|||||
|
10 |
√ |
||||||||
|
2.3. Assessment |
11 |
9 |
√ |
|
|
||||
|
10 |
√ |
|
|
||||||
|
12 |
11 |
√ |
|
|
|||||
|
13 |
12 |
|
√ |
Decided to select NICU (Rs) of the XXXXXXXXXXXXXXXXXXXXXXXXXXXXX CPG |
|||||
|
14 |
13 |
|
√ |
Decided to rely on D3 Scores of AGREE II |
|||||
|
14 |
|
√ |
|||||||
|
15 |
15 |
|
√ |
Decided to rely on D5, D2 Scores of AGREE II |
|||||
|
2.4. Decision and Selection |
16 |
Table |
√ |
|
|
||||
|
17 |
Decision making and selection |
√ |
|
|
|||||
|
|
2.5. Customization |
18 |
16 |
√ |
|
|
|||
|
|
|||||||||
|
THREE: FINALIZATION |
3.1. External Review and Acknowledgment Module |
19 |
17 |
√ |
|
|
|||
|
20 |
|
√ |
|
|
|||||
|
21 |
|
√ |
|
|
|||||
|
22 |
|
√ |
|
|
|||||
|
3.2. Aftercare Planning |
23 |
18 |
√ |
|
|
||||
|
3.3. Final Production |
24 |
|
√ |
|
|
||||
Appendix Table 4. The RIGHT-Ad@pt checklist |
|||||
|
7 sections, 27 topics, and 34 items |
Assessment |
Page(s)* |
Note(s) |
||
|
BASIC INFORMATION |
|||||
|
Title/subtitle |
|||||
|
1 |
Identify the report as an adaptation of practice guideline(s), that is include "guideline adaptation", "adapting", "adapted guideline/recommendation(s)", or similar terminology in the title/subtitle. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
2 |
Describe the topic/focus/scope of the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Cover/first page |
|||||
|
3 |
Report the respective dates of publication and the literature search of the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
4 |
Describe the developer and country/region of the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Executive summary/abstract |
|||||
|
5 |
Provide a summary of the recommendations contained in the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Abbreviations and acronyms |
|||||
|
6 |
Define key terms and provide a list of abbreviations and acronyms (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Contact information of the guideline adaptation group |
|||||
|
7 |
Report the contact information of the developer of the adapted guideline. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
SCOPE |
|||||
|
Source guideline(s) |
|||||
|
8 |
Report the name and year of publication of the source guideline(s), provide the citation(s), and whether source authors were contacted. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Brief description of the health problem(s) |
|||||
|
9 |
Provide the basic epidemiological information about the problem (including the associated burden), health systems relevant issues, and note any relevant differences compared to the source guideline(s).
|
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Aim(s) and specific objectives |
|||||
|
10 |
Describe the aim(s) of the adapted guideline and specific objectives, and note any relevant differences compared to the source guideline(s). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Target population(s) |
|||||
|
11 |
Describe the target population(s) and subgroup(s) (if applicable) to which the recommendation(s) is addressed in the adapted guideline, and note any relevant differences compared to the source guideline(s). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
End-users and settings |
|||||
|
12 |
Describe the intended target users of the adapted guideline, and note any relevant differences compared to the source guideline(s). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
13 |
Describe the setting(s) for which the adapted guideline is intended, and note any relevant differences compared to the source guideline(s). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
RIGOR OF DEVELOPMENT |
|||||
|
Guideline adaptation group |
|||||
|
14 |
List all contributors to the guideline adaptation process and describe their selection process and responsibilities. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Adaptation framework/methodology |
|||||
|
15 |
Report which framework or methodology was used in the guideline adaptation process. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Source guideline(s) |
|||||
|
16 |
Describe how the specific source guideline(s) was(were) selected. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Key questions |
|||||
|
17 |
State the key questions of the adapted guideline using a structured format, such as PICO (population, intervention, comparator, and outcome), or another format as appropriate. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
18 |
Describe how the key questions were developed/modified, and/or prioritized. |
☐ Yes ☒ No ☐ Unclear |
|
|
|
|
Source recommendation(s) |
|||||
|
19 |
Describe how the recommendation(s) from the source guideline(s) was(were) assessed with respect to the evidence considered for the different criteria, the judgements and considerations made by the original panel. |
☐ Yes ☒ No ☐ Unclear |
|
|
|
|
Evidence synthesis |
|||||
|
20 |
Indicate whether the adapted recommendation(s) is/are based on existing evidence from the source guideline(s), and/or additional evidence. |
☐ Yes ☒ No ☐ Unclear |
|
|
|
|
21 |
If new research evidence was used, describe how it was identified and assessed. |
☐ Yes ☒ No ☐ Unclear |
NA |
|
|
|
Assessment of the certainty of the body of evidence and strength of recommendation |
|||||
|
22 |
Describe the approach used to assess the certainty/quality of the body/ies of evidence and the strength of recommendations in the adapted guideline and note any differences (if applicable) compared to the source guideline(s). |
☐ Yes ☒ No ☐ Unclear |
NA |
|
|
|
Decision-making processes |
|||||
|
23 |
Describe the processes used by the guideline adaptation group to make decisions, particularly the formulation of recommendations.
|
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
RECOMMENDATIONS |
|||||
|
Recommendations |
|||||
|
24 |
Report recommendations and indicate whether they were adapted, adopted, or de novo. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
25 |
Indicate the direction and strength of the recommendations and the certainty/quality of the supporting evidence and note any differences compared to the source recommendations(s) (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
26 |
Present separate recommendations for important subgroups if the evidence suggests important differences in factors influencing recommendations and note any differences compared to the source recommendations(s) (If applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Rationale/explanation for recommendations |
|||||
|
27 |
Describe the criteria/factors that were considered to formulate the recommendations or note any relevant differences compared to the source guideline(s) (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
EXTERNAL REVIEW AND QUALITY ASSURANCE |
|||||
|
External review |
|||||
|
28 |
Indicate whether the adapted guideline underwent an independent external review. If yes, describe the process. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Organizational approval |
|||||
|
29 |
Indicate whether the adapted guideline obtained organizational approval. If yes, describe the process. |
☒ Yes ☐ No ☐ Unclear |
SNS & NEBMC |
|
|
|
FUNDING, DECLARATION, AND MANAGEMENT OF INTEREST |
|||||
|
Funding source(s) and funder role(s) |
|||||
|
30 |
Report all sources of funding for the adapted guideline and source guideline(s), and the role of the funders. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Declaration and management of interests |
|||||
|
31 |
Report all conflicts of interest of the adapted and the source guideline(s) panels, and how they were evaluated and managed. |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
OTHER INFORMATION |
|||||
|
Implementation |
|||||
|
32 |
Describe the potential barriers and strategies for implementing the recommendations (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Update |
|||||
|
33 |
Briefly describe the strategy for updating the adapted guideline (if applicable). |
☒ Yes ☐ No ☐ Unclear |
|
|
|
|
Limitations and suggestions for further research |
|||||
|
34 |
Describe the challenges of the adaptation process, the limitations of the evidence, and provide suggestions for future research. |
☐ Yes ☒ No ☐ Unclear |
-- |
|
|