Topogaraphical, clinical and therapeutic ophthalmology
| Site: | EHC | Egyptian Health Council |
| Course: | Veterinary Ophthalmology Guidelines |
| Book: | Topogaraphical, clinical and therapeutic ophthalmology |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:34 AM |
Description
"last update: 20 November 2025" Download Guideline
- Acknowledgement
We would like to acknowledge the committee of National Egyptian Guidelines for Veterinary Medical Interventions, Egyptian Health Council for adapting this guideline.
Executive Chief of the Egyptian Health Council: Prof. Dr Mohamed Mustafa Lotief.
Head of the Committee: Prof. Dr Ahmed M Byomi
The rapporteur of the Committee: Prof. Dr Mohamed Mohamedy Ghanem.
Scientific Group Members: Prof. Dr Nabil Yassien, Prof. Dr Ashraf Aly Eldesoky Shamaa, Prof. Dr Amany Abbas, Prof. Dr Dalia Mansour, Dr Essam Sobhy Dr Mohamed Elsharkawy, Prof. Dr Gamal A. Sosa., Dr Naglaa Radwan, Dr Hend El Sheikh
Scientific Editor/Authors: Prof. Dr Ashraf Aly Eldesoky Shamaa. Dr Mohamed Elsharkawy. Prof. Dr. Mohamed Mostafa Saied Amer, Prof. Dr. Shaaban Mohamed and Dr. Mohamed Moustafa Bahr Moustafa.
- Scope
This guideline Review the common surgical affections of the eye to accustom veterinarian how to pick the principles up to recognize case appraisal, etiology, clinical signs, diagnosis and differential diagnosis, prognosis and different traits used of treatment in different animal species. This guideline to become an effective document, it is important to incorporate the proposed strategies into routine protocols and staff training. The guideline will present the following topics:
1. Ocular anatomy.
2. Examination of the eye.
3. Ocular pharmacology and therapeutics
4. Upper and lower eyelids.
5. Nictitating membrane.
6. Lacrimal System.
7. Anterior uvea.
8. Conjunctiva.
9. Sclera.
10. Cornea.
11. Anterior Chamber.
12. Glaucoma.
13. Orbit and Globe.
14. Lens.
➡️Keywords:
Ophthalmology, topographical anatomy, clinical and therapeutic ophthalmology.
- OCULAR ANATOMY
The eyeball consists of three layers:
1- External fibrous tunic: It is the outer protective layer and consists of a transparent portion (cornea) and opaque portion (sclera).
2- Middle vascular tunic: This layer provides the nourishment for the eyeball and consists of iris, ciliary body and choroid.
3- Internal nervous tunic: This layer is represented by the retina which is really an expansion of the optic nerve.
Adnexal structures of the eyeball:
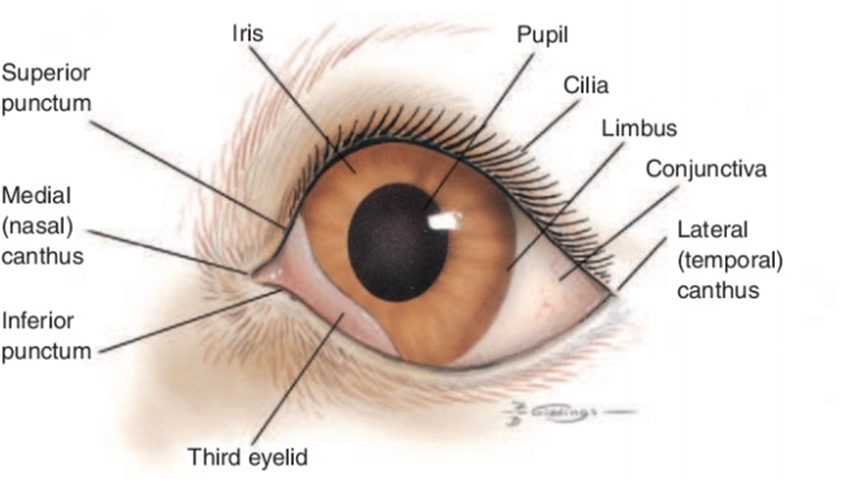
Fig.1: Frontal view of the external structures of the canine eye. Budras KD, et al. (2002):
Structures within the eyeball :
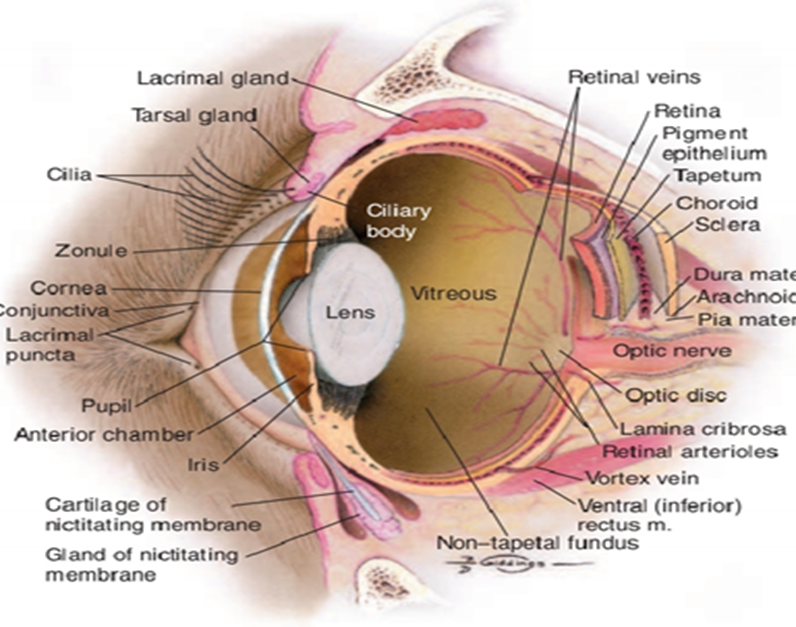
Fig.2: Internal structures of the canine eye. (Budras et al., 2002).
Arterial Supply
The major arterial supply of the eye is from the external ophthalmic artery, a branch of the internal maxillary artery, which arises from the external carotid artery The contribution from the internal carotid artery is small, unlike the situation in primates, and is via an internal ophthalmic artery, which arises from the circle of Willis. The internal ophthalmic artery enters the orbit through the optic canal with the optic nerve. From the external ophthalmic artery, numerous short posterior ciliary arteries arise and penetrate the sclera around the optic nerve head. These arteries supply the retina and choroid.
Venous Drainage
The retina is drained by the retinal veins and venules, which run from the peripheral retina toward the optic nerve head, The venous circle drains posteriorly through the sclera via the posterior ciliary veins to a dilation in the orbital vein, the superior (dorsal) ophthalmic vein.
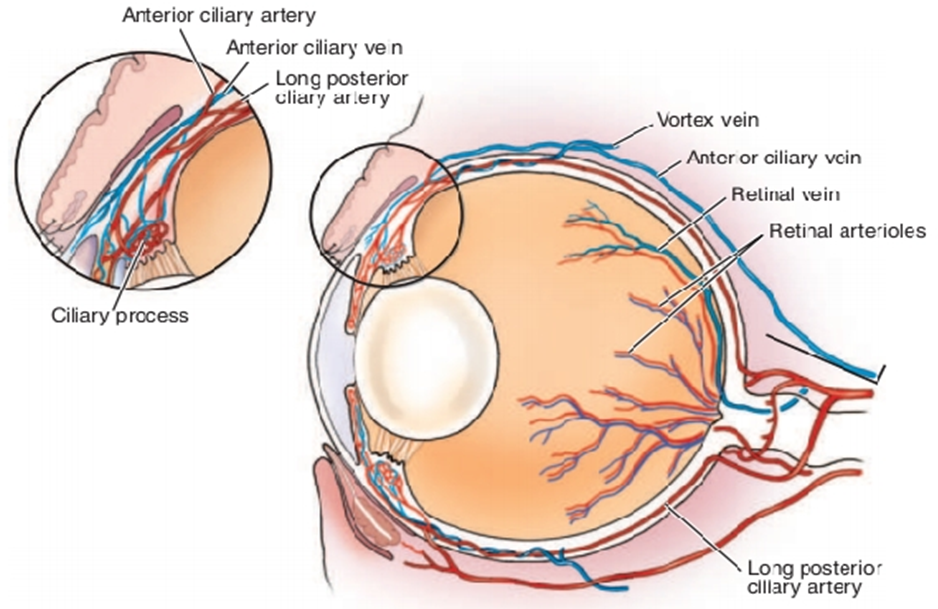
Fig.3: Vascular supply of the canine eye. (Remington , 2005).
Nerve supply:
1- Optic nerve (second cranial nerve)
The optic nerve consists of ganglion cells, whose cell bodies lie in the ganglion cell layer of the retina.
2- Oculomotor nerve(Cranial Nerve III)
The nucleus of the oculomotor nerve lies in the brainstem and has several components serving different extraocular muscles
3- Trochlear nerve (Cranial Nerve IV)
It passes through the fissure with the oculomotor nerve and the ophthalmic branch of the trigeminal nerve. The trochlear nerve innervates the dorsal oblique muscle only.
4- Trigeminal Nerve (Cranial Nerve V)
The nerve has both motor and sensory roots.
5- Abducens nerve (Cranial Nerve VI)
Supply the retractor bulbi and lateral rectus muscles.
6- Facial Nerve (Cranial Nerve VII)
The mixed facial nerve contains somatic motor and parasympathetic fibers, innervating the orbicularis oculi and retractor anguli muscles and the lacrimal gland.
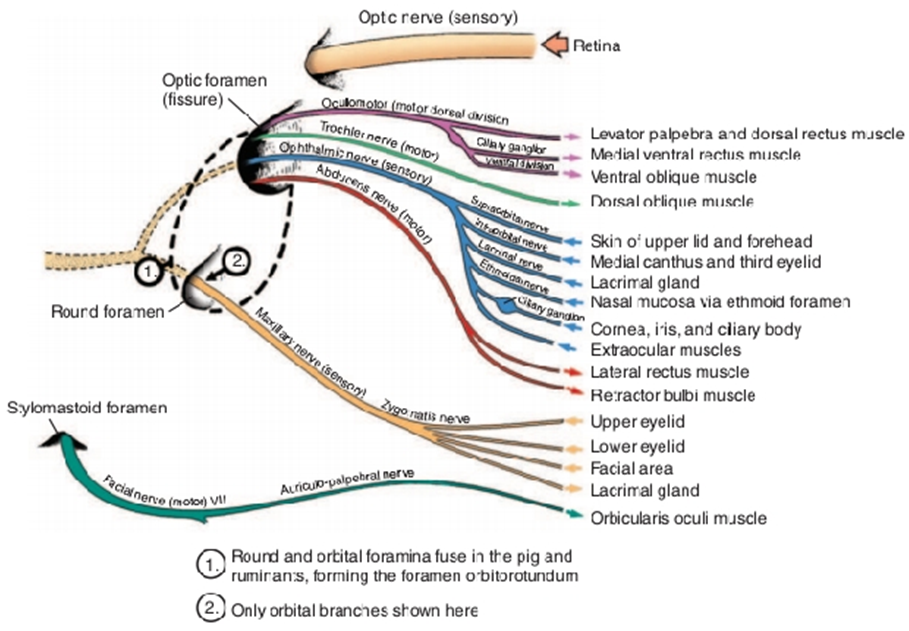
Fig.4: Nerve supply to the eye. (Evans, 1993).
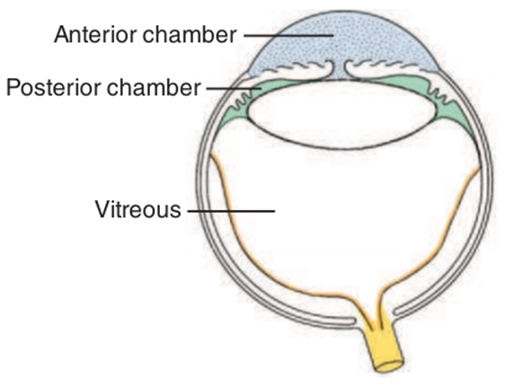
Fig.5: The chambers of the eye. The aqueous compartment is subdivided into two chambers by the iris diaphragm. The anterior chamber is anterior to the plane of the iris and pupil (blue), whereas the posterior chamber (green) is posterior to the iris-pupil plane but anterior to the vitreous (white). The retina and optic nerve are in yellow. (Budras ,2002).
- EXAMINATION OF THE EYE
I- EXTERNAL EXAMINATION OF THE EYEBALL
1- Naked eye examination
Large animals are examined first out-of-doors in day light then indoors in a reduced light. Determine if the lesions are bilateral or unilateral and the normal eye is examined first. The following is determined
a. Lacrimation or abnormal discharge
b. Size of the eye
c. Position of the eye:
d. Endophthalmia
e. Exophthalmia
f. Strabismus
g. Periorbital swellings
2- MICROBIOLOGIC SAMPLING( Corneoconjunctival smears, scrapings and cultures)
- It is used to evaluate the condition of the cornea and conjunctiva for presence of a microbial pathogen by cytological assessment, culture, polymerase chain reaction, or immunofluorescent antibody labeling.
- Microbiologic specimens have been collected with a moist swab. May prefer to collect more cellular specimens from corneal or conjunctival lesions by scraping or with a cytology brush.

Fig.6: Instruments suitable for collecting ocular surface samples for cytologic and microbiologic examination. Left to right, Kimura platinum spatula, handle-end of Bard-Parker scalpel blade, cytology brush. (Bauer , et al.,1996).
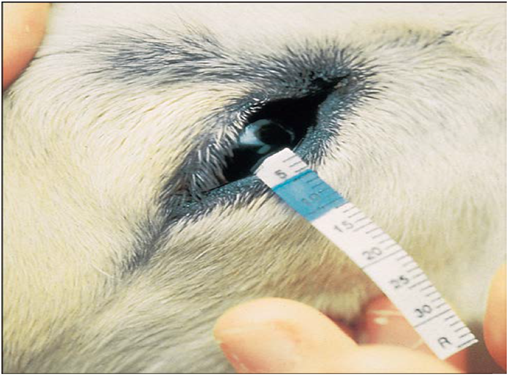
3- Schirmer’s tear test(STT)
- It is a test used to measure the amount of tears produced per one minute.
- The test is performed with sterile, individually packaged strips of absorbent paper with a notch 5mm from one end. Each strip is folded at the notch and hooked over the middle to lateral third of the lower lid for 60 seconds.
- The STT measures basal and reflex tearing, including that due to corneal stimulation provided by the test strip itself, it can gently contact the corneal surface if it is placed more medially.
- Each animal had normal values of STT Readings of less. are considered diagnostic for keratoconjunctivitis sicca. particularly if appropriate clinical signs are present.
|
Fig.7: Schirmer tear test being performed on a horse. Note that the strip is placed into The lower lateral conjunctival fornix so that it lightly contacts the lateral cornea. (Abrams et al., 1990). |
II- Systemic examination
- The following structures are examined; eyelids (upper and lower), third eyelid, conjunctiva, sclera, cornea, anterior chamber, iris, lens, vitreous body and pupillary reflexes.
- A dark examination room for small animal and dark stall for large animal is suitable for detection of pupillary reflexes.
A- Pupillary reflexes (PLR) Direct pupillary reflex / Indirect pupillary reflex
- The reflex constriction of the pupil in response to light striking the retina is termed the pupillary light reflex. Its help to assess the pupil size, shape, and symmetry, pupil reactivity.
- Pupil shape and the speed and magnitude of the PLR differ among species.
- In most mammals, constriction of the pupil of the illuminated eye (the direct PLR) is slightly greater than that of the pupil of the contralateral or non-illuminated eye (the indirect or consensual PLR).
- If there is any pathology at any point along the neurologic pathway, iris atrophy (due to age), iris ischemia, (due to acute glaucoma), physical obstruction of the pupil (due to synechia or lens dislocation), prior use of a dilating drug, or high concentrations of circulating epinephrine (i.e., in fearful animals) the PLR may be decreased or absent.
- A positive direct pupillary light reflex is not a reliable indicator of vision or normal retinal function.
- Both the extent and speed of the PLR should be assessed and compared in the two eyes and against what is considered normal for that species.
1- Retroillumination
- Retroillumination is a simple but extremely useful technique for assessment of pupil size, shape, and symmetry. A focal light source (Fin off trans-illuminator or direct ophthalmoscope) is held up to the examiner’s eye and directed over the bridge of the patient’s nose from at least arm’s length from the patient so as to equally illuminate the two pupils and elicit the fundic reflection.
- This reflection is usually gold or green in tapetal animals and red in a tapetal individual.
- Retroillumination used to judge the clarity of all of the transparent ocular media (tear film, cornea, aqueous humor, lens, and vitreous).
- Retroillumination particularly useful for differentiating nuclear sclerosis from cataract.

Fig.8: Retroillumination used to judge the clarity of all of the transparent ocular media (David &Maggs,2022).
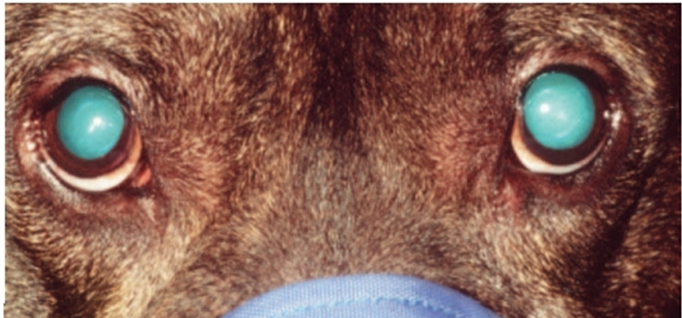
Fig.9: Retroilluminated view of a dog with bilateral nuclear sclerosis (Visible as a translucent ring inside the pupils of both eyes). (David &Maggs,2022).
2- Slit – lamp bio-microscopy
- It is used for examination of the transparent structures of the eye (cornea and lens).
- it’s more sophisticated optical instrument that combines up to 40μ magnification and illumination and can be used to examine many different microscopic and optical features of the patient’s eye such as individual layers of the cornea that normally are invisible to the naked eye of the examiner. As such, it allows pathologic processes to be described more accurately so as to better guide diagnosis, prognosis, and treatment.
|
Fig.10: A slit-lamp bio-microscope in use. (Martin,1969).
Fig.11: portable slit lamp. |


3- Gonioscopy
- It is a procedure used for examination of the anterior chamber angle on gonioscopic findings.
- Gonioscopy describes examination of the iridocorneal or “drainage” angle (the junction between the iris and cornea).
- In the normal eye of most species light rays that are reflected from the drainage angle strike the posterior cornea and undergo total internal reflection as in a prism.
- This occurs because of the difference in refractive index between the cornea and the surrounding air, and the high angle of incidence of the light rays from the drainage angle. By replacing the air surrounding the cornea with a goniolens that has an index of refraction close to that of the cornea, total internal reflection is avoided and light rays from the drainage angle can be viewed directly through the goniolens.
|
Fig.12:Performing gonioscopy in a non-sedated dog utilizing a slit lamp and a Franklin goniolens. (Bedford ,1973). Fig.13: Gonioscopy permits examination of the iridocorneal or “drainage” angle. A, Normally, light rays from the drainage angle undergo total internal reflection at the posterior cornea. B, A direct goniolens refracts light so that the drainage angle may be viewed directly. C, An indirect goniolens refracts light so that the image is viewed in a mirror. (Bedford ;1973). |
|

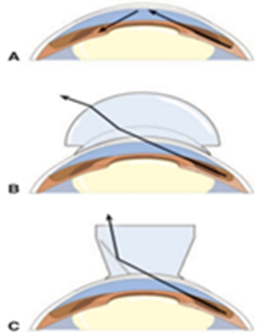
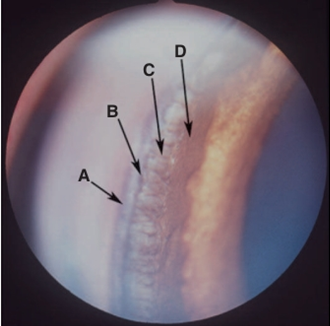
Fig.14: Gonioscopic view of a normal canine iridocorneal (drainage) angle. A, Outer pigment band; B, inner pigment band; C, pectinate ligaments; D, iris root (Martin,1969).
4- Tonometry
- It is the measurement of the intraocular pressure (IOP). It can be performed by three methods; digital tonometry, Schoitz tonometry and Applanation tonometry.
- normal canine and feline IOP is reported as approximately 10 to 20mmHg.
- It is a method of diagnosing anterior uveitis (where IOP is typically reduced) and of confirming the diagnosis of all other causes of reddened eye, such as keratitis, conjunctivitis, scleritis, and orbital cellulitis (in which IOP should be unaffected). Following confirmation of uveitis or glaucoma, tonometry should be an essential and perhaps the most important method of monitoring response to therapy and judging the augmentation of therapy.
- The IOP should be measured in all red, inflamed, or painful eyes to diagnose or eliminate from consideration both glaucoma and uveitis.
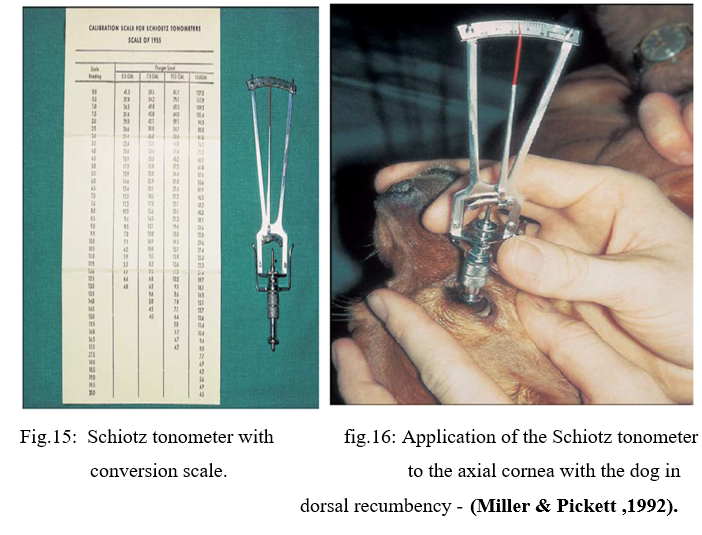
A- Indentation Tonometry
The Schiøtz tonometer relies upon indentation tonometry. In this method, a standard force is applied with a metal rod to the anesthetized cornea.
B- Applanation Tonometry
Unlike indentation tonometry, applanation tonometry using the Tono-Pen , is suitable for large animals, is unaffected by variations in ocular rigidity, requires no conversion tables, and needs no sterilization.
The advantages of the Tono-Pen include the following:
1- It is accurate and easy to use.
2- The animal’s head does not need to be held vertically, although the probe must a planate the corneal surface at right angles.
3- Errors induced by different sizes and curvatures of corneas in different species are less important.
4- Because of the small instrument head, irregular or diseased corneal areas may be avoided, and accurate readings obtained from even small corneas of exotic species.
5- The probe tip is covered with a disposable latex cap, which is changed between uses and prevents transfer of infections.
6- Minimal restraint is required.
7- The pressure is displayed in mm Hg without need for conversion via tables.

Fig.17: Tono-Pen in use by lightly tapping the cornea. (Leiva, et al.,2006).
C- Rebound Tonometry
Rebound (or impact or dynamic) tonometry is a third mechanism by which IOP may be measured and which uses a different mechanical principle. Rebound tonometer eject a small probe (such as a metal pin with a rounded end) at a fixed distance from the cornea and assess the motion of the probe as it strikes the cornea and is returned (rebounds) to the instrument.
|
Fig.18: Rebound tonometry using the TonoVet in a dog ( Görig et al. ,2006). |
. |
|

1-Ophthalmoscopy
- It is the study of the internal structures of the eyeball by ophthalmoscope directly through a widely dilated pupil by aligning the light beam with his/her visual axis and standing a short distance from the patient, as for retro-illumination .
a- Direct ophthalmoscopy
The direct ophthalmoscope directs a beam of light into the patient’s eye and places the observer’s eye in the correct position to view the reflected beam and details of the interior of the eye.
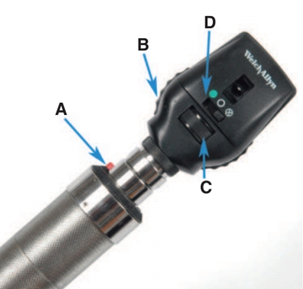
Fig.19: The direct ophthalmoscope. Controls for light intensity (A),
focusing lenses (B), light aperture size and shape (C), and filters (D).
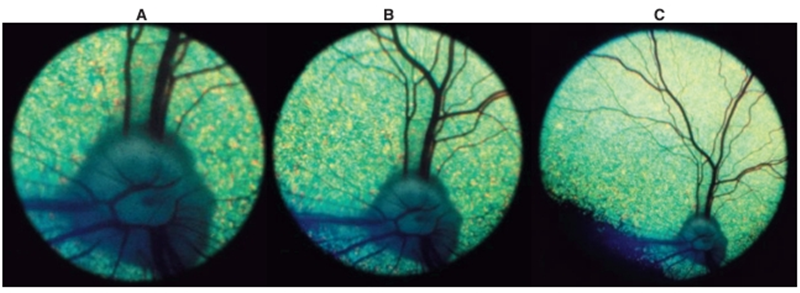
Fig.20: View of a canine fundus as seen through the direct ophthalmoscope (A), the monocular indirect (Panoptic) ophthalmoscope (B), and a 20-D indirect lens (C). Note that as magnification increases, field of view decreases. ( Ramsey et al.,1999).
b- Indirect ophthalmoscopy
Viewing the image of the fundus with a convex lens (typically 20 to 30 D) is placed between the observer’s eye and the patient’s eye and an inverted virtual image is formed between the lens and observer. The magnification and field of view depend on the dioptric power of the lens and on the size of the patient’s eye. However, with the lenses typically used in veterinary medicine, the magnification is always less and the field of view greater than that achieved with use of a direct ophthalmoscope.
|
Fig. 21: The monocular indirect ophthalmoscope (Panoptic) in use. (Moore , 2001) |
Fig.22: Binocular indirect ophthalmoscope. This unit has a rechargeable battery transformer that allows portability.
|


2- Electroretinography (ERG):
- Electroretinography (ERG) is the study of electrical potentials produced by the retina when light strikes it. Light of varying intensity, wavelength, and flash duration is directed onto the retina and the resulting potential differences are detected by electrodes placed around the eye.
- The ERG is performed with the animal under general anesthesia or deep sedation to minimize periocular muscle movements. It is useful in all species. Electroretinography is a test of retinal but not optic nerve or visual function. It is usually available only at specialty ophthalmology practices.
The ERG may be used for the following purposes
1- Preoperative evaluation of retinal function before cataract extraction when fundic examination is not possible.
2- Diagnosis and differentiation of inherited retinal disorders (e.g., rod-cone dysplasias, progressive retinal degeneration, hemeralopia)
3- Investigation of unexplained visual loss (amaurosis) in which retinal lesions are not visible ophthalmoscopically (e.g., sudden acquired retinal degeneration SARD, optic neuritis, CNS disease).

Fig.23: An electroretinogram being performed on a dog. Note the ground and reference (subcutaneous) electrodes as well as the corneal contact lens electrode. (Acland ,1988).
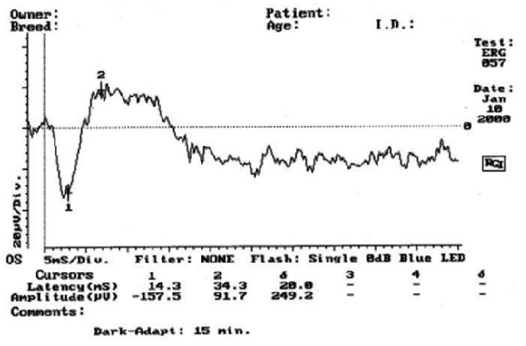
Fig.24: A normal electroretinogram (Acland GM ,1988).
3-Ultrasonography
- In ultrasonography, high-frequency sound waves above the audible range are directed posteriorly through the eye from the cornea, and the echoes are detected.
- Ultrasonography is used to examine the contents of eyes in which opacity of one of the usually clear ocular media (cornea, aqueous humor, lens,or vitreous) prevents visualization of the structures caudal to it. It is also useful to assess orbital structures and to guide fine needle aspiration of intraocular and orbital structures.
Ultrasonography is particularly useful for the following
- Detection of retinal detachment.
- Detection of lens dislocation or rupture.
- Detection of vitreous degeneration
- Detection of intraocular tumors or foreign bodies
- Characterization of retrobulbar disease
- Guidance of fine-needle aspirates of orbital and ocular lesions.
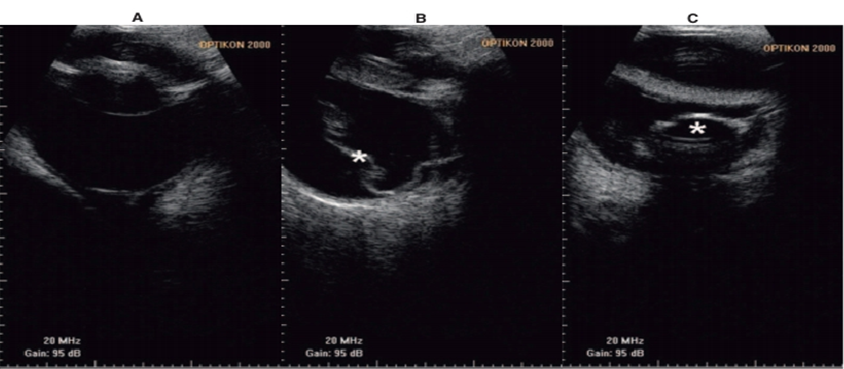
Fig.25: B-mode ultrasound images of A, a normal globe; B, a detached retina (*); C, a posteriorly luxated lens (Cottrill et al., 1989).
|
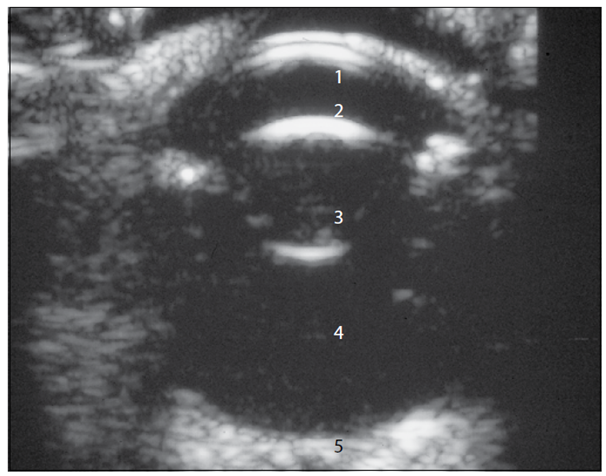
Fig.26: B-mode ultrasound image of a normal 11-year-old dog with a 10-MHz probe and direct contact with the cornea. (1: Cornea; 2: Anterior chamber; 3: Lens; 4: Vitreous; 5: Optic nerve (Cottrill et al., 1989). |
5- Anterior chamber paracentesis
- It is the collection of a sample of aqueous humour. The anterior chamber is entered at the limbus and is indicated in cases of hypopyon, chronic uveitis, malignant glaucoma, prior to surgery and diagnosis of anterior segment diseases.
- A 30-gauge needle has been inserted at the dorsolateral limbus and directed in a plane parallel to the iris. No syringe is attached, and aqueous humor is allowed to passively fill the needle hub. In this procedure, care should be taken not to touch the corneal endothelium, the iris, or the lens with the needle tip.
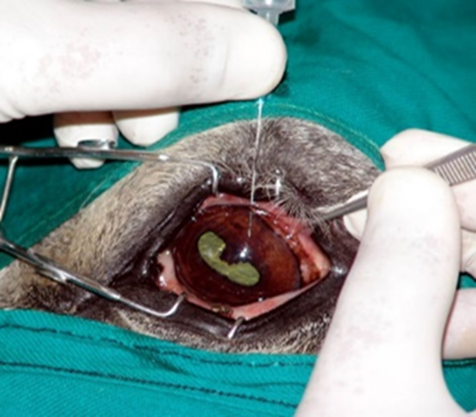
Fig.27: Anterior chamber paracentesis from a cat with uveitis. (Hamor ,2001)
6- Vitreous paracentesis
Vitreous paracentesis (hyalocentesis) in dogs is a procedure to collect small amount of vitreous fluid for diagnostic analysis, performed under general anesthesia after dilating the pupil and disinfecting the eye. The needle is carefully inserted through the sclera and pars plana ciliaris to avoid complications like retinal punctures or significant intraocular hemorrhage.

Fig.28: Vitreous centesis of a cat eye. Special care should be taken to avoid the lens (Hamor,2001)
6- Computed Tomography and Magnetic Resonance Imaging
- CT and MRI provide superb detail for localization of orbital lesions.
- Contrast sialography and dacryocystorhinography are as applicable to CT as they are to radiography and provide superior detail.
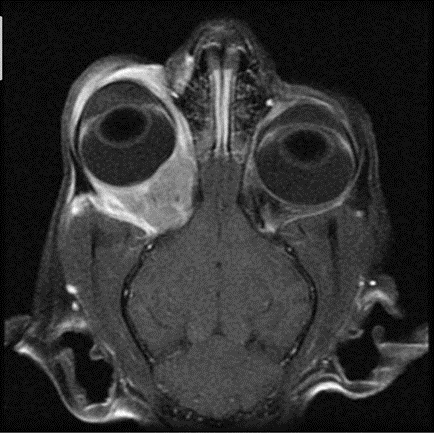
Fig.39: T1-weighted, post–contrast injection, frontal magnetic resonance image of a cat with a space-occupying mass behind the right eye. Cytology and culture testing performed on material aspirated from this mass permitted diagnosis of a bacterial retrobulbar abscess/cellulitis that responded well to antibiotic therapy (Calia et al., 1994).
- OCULAR PHARMACOLOGY AND THERAPEUTICS
I- ROUTES OF ADMINISTRATION OF OCULAR DRUGS
The main factors governing choice of the route of administration are as follows
1- Inherent properties of the drug.
2- Site of desired action (surface or intraocular structures.
3- Frequency of administration possible.
4- Drug concentration required at target tissue.
5- Vascularity of the target tissue.
Sites of drug administration
1- Topically applied ointments
Suspensions and solutions achieve high drug concentrations on the corneal and conjunctival surface.
2- Subconjunctival injections
Facilitate high drug concentrations at the ocular surface and provide a variable-duration depot effect.
3- Intraocular (intracameral or intravitreal)
Injection of drugs is used rarely because general anesthesia is needed, serious ocular risks are associated with this route of therapy.
4- Systemically administered drugs (oral or parenteral)
Reach all vascular ocular structures but are not delivered in useful concentration.
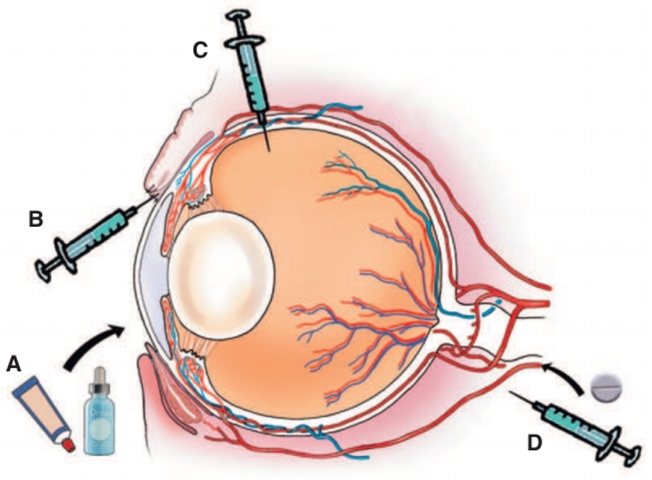
Fig.31: Sites of drug administration. A, Topically applied ointments, B, Subconjunctival C, Intraocular (intracameral or intravitreal) injection. D, Systemically administered drugs (oral or parenteral). (Budras et al.,2002).
- Frequency of administration
1- Periodic administration
2- Continuous or Intermittent Ocular Surface Lavage Systems
- In patient with painful eyes, a lavage system allows medications to be conveniently, safely, and frequently delivered into the conjunctival sac.
- Systems were placed within the nasolacrimal duct and medications were instilled in a retrograde fashion.
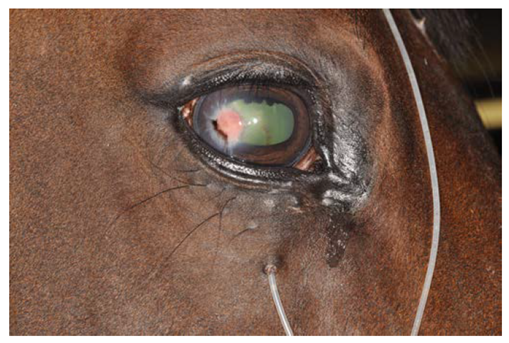
Subpalpebral administration to treat equine and feline:
- Subpalpebral lavage systems placed in the medial aspect of the lower lid are associated with less common and less severe ocular complications than those placed centrally and dorsally, even when left in place and used by owners for up to 55 days later.
- The lavage tube leads back to the shoulder, where it is secured at the mane and where drugs can be administered with less risk of injury to the eye or the operator.
- Drugs are injected into the tube and either slowly propelled to the eye with a gently administered bolus of air from a syringe or continuously propelled by a gravity-fed bottle or small mechanical infusion pump connected to the tube.
- This method of therapy is usually reserved for horses with severe corneal or uveal disease.
- A protective eyecup can be applied over the lavage tube for protection of the eye and apparatus. Ointments (and some more viscous suspensions) cannot be applied through lavage systems.

Fig.32: Placement of a subpalpebral lavage system in the medial aspect of a horse’s lower eyelid. A, A local (subcutaneous) injection of lidocaine is administered. B, The palpebral and fornicial conjunctival surfaces are anesthetized with proparacaine-soaked cotton-tipped applicators held in place for 1 or 2 minutes. C, A trocar is used to penetrate the lower lid from the conjunctival fornix, and the lavage tube is threaded through it. D, The trocar is removed, and the lavage tube is pulled down until it lies snugly in the ventral conjunctival fornix between the third eyelid and lower lid. (Budras et al.,2002).
|
Fig.33: Right eye of a horse with a subpalpebral lavage system inserted through the inferior eyelid. The footplate of the tube rests between palpebral conjunctiva and third eyelid to avoid corneal irritation (Budras et al.,2002). |
- OPHTHALMIC THERAPEUTIC AGENTS
1. Cleansing solutions
Sterile eye wash is used for removal of purulent exudates, foreign bodies, and irritants from the eyelids and conjunctival sac.
- Normal saline solution (NaCl solution 0.9%).
- B.S.S. (Balanced salt solution) and boric acid solution 2%.
2- Astringents and Cauterants
Identification and removal of the cause or more modern medical and surgical approaches usually achieve a better result in a more controlled manner, and astringents and cauterants are no longer recommended for ocular use.
- Astringents are locally acting protein precipitants.
- Cauterants are severe protein-precipitating agents that cause local tissue destruction.
Astringents as
- Zinc sulphate.
- Silver nitrate solution (1%).
- Copper sulphate .
- Yellow mercuric oxide (golden eye ointment).
.Cauterants as
- Carbolic acid (phenol.
- Tincture of iodine.
- Silver nitrate sticks
4. Mydriatics
They are drugs that dilate the pupil by stimulate the contraction of the iris dilator muscle or relax the iris sphincter muscle. they are used To make it easier to examine the retina and internal structures of the eye, treat inflammatory conditions like iritis and relieve spasms of the ciliary muscle , they can cause blurred vision, photophobia (light sensitivity), and dry eyes.
Example
• Atropine.
• Tropicamide (1% solution).
• Scopolamine (0.3 - 0.5%) solution.
• Epinephrine (Adrenalin).
• Phenylepherine.
5. Miotics
Miotics are drugs that constrict the pupil by stimulate the contraction of the iris sphincter muscle or cause the relaxation of the iris dilator muscle they are used to treat open-angle glaucoma by increasing the outflow of aqueous humor, help with presbyopia (age-related farsightedness) and to reverse the effects of mydriatics. Side effects can include eye discomfort and headache.
Example
- Pilocarpine 1-4%.
- Carbachol 1%.
- Eserine 0.25%.
6. LOCAL ANESTHETICS
a- Topical (local) anesthetics are used for ocular examinations and minor manipulative and surgical procedures, but never for therapeutic purposes. The effect on corneal sensation of a single drop of proparacaine or 2 drops separated by 1 minute.
b- Injectable analgesics
xylocaine (lidocaine) 1 - 2%, procaine (Novocaine) 1%, carbocaine (Mepivacaine HCL) 1-3%, marcaine (Bupivacaine HCL) 0.25–0.75% and duranest (Etidocaine HCL) 1%.
7. Antibiotics
The factors must be considered in the selection of an antibiotic
• The offending organism and its sensitivity.
• Location of the organism.
• Penetration of available drugs to that site.
• Pharmacokinetics of the available drugs
• Spectrum of activity of available drugs
•Toxicity of available drugs
The antibiotics used commonly in veterinary ophthalmology
- Penicillins
a large family of natural and synthetic derivatives of 6-aminopenicillanic acid that range considerably in stability, solubility, spectrum of activity, ocular penetration, and resistance to β-lactamase.
- Cephalosporins
They are generally similar to the penicillins in mechanism of action and pharmacology but are less susceptible to staphylococcal b-lactamases. A type of b-lactamase (cephalosporinase) produced by some Gram-negative organisms may inactivate them, also very useful for bacterial blepharitis. Cefazolin is the antibiotic of choice for perioperative antimicrobial prophylaxis in small animal surgery.
- Chloramphenicol
Is a broad-spectrum bacteriostatic antibiotic effective against a wide range of Gram-positive and Gram-negative organisms, Rickettsia, spirochetes, and Chlamydophila spp. However, Pseudomonas aeruginosa is often resistant. Because of its lipid solubility, Chloramphenicol may be administered orally, intramuscularly, subcutaneously, intravenously, subconjunctivally, or topically. Because absorption after oral administration results in high blood concentrations, this is the route of choice for infections in the posterior globe and orbit.
- Neomycin
Useful bactericidal agent for ocular use and is active against Gram-positive and Gram-negative bacteria, including Staphylococcus aureus and highly effective against Proteus vulgaris.
- Gentamicin
a topical agent of first choice for bacterial prophylaxis, relatively narrow against Gram-negative organisms, the value of gentamicin for treatment of more resistant organisms strains of S. aureus, Pseudomonas spp., E. coli, Aerobacter, Klebsiella spp., and Proteus spp. Topical application does not result in high intraocular concentrations, and although some drug enters the eye after subconjunctival or intravenous injection, vitreous penetration is poor regardless of route of administration. Long-term systemic therapy is limited by ototoxicity and nephrotoxicity. Gentamicin causes cataract and severe retinal degeneration when injected intraocularly.
- Tobramycin
Is effective againstβ-lactamase–producing staphylococci, resistance to tobramycin is less frequent, probably because of its more recent introduction. It is also ototoxic and nephrotoxic when given systemically but may be administered topically. or by administered via subconjunctival injection.
- Tetracyclines
broad-spectrum bacteriostatic antibiotics; however, Staphylococcus, Pseudomonas, and Proteus spp. are usually resistant. Tetracyclines are useful in treatment of infections with Chlamydophila and Mycoplasma spp. in cats. Systemic administration to dogs affected with periocular staining from pigments in the tears results in a decrease in staining, tetracycline preparations are effective for treatment of Moraxella bovis infection in cattle.
7.Antiviral drugs (DNA-synthesis inhibitors)
The use of antiviral drugs in veterinary ophthalmology is restricted to treatment of herpetic keratoconjunctivitis due to feline herpesvirus (FHV-1) in cats or, occasionally, equine herpesvirus (EHV-2) in horses.
Agents commonly used for treatment of patients with viral infection
- Idoxuridine
Idoxuridine is of the constituents of nucleic acids, which it replaces during DNA synthesis, thereby inhibiting viral replication. Can be compounded as a 0.1% solution or 0.5% ointment. It penetrates the intact cornea poorly after topical application but is generally well tolerated by cats. It must be applied at least 5 times daily.
- Vidarabine
Vidarabine interferes with viral DNA synthesis, and is moderately active against FHV-1 replication in vitro. It is usually well tolerated when applied topically as an ointment.
- Acyclovir and Valacyclovir
Acyclovir is widely available as a systemic drug, also available in a topical (ophthalmic) preparation. The efficacy of acyclovir against FHV-1 is low; cats receiving acyclovir sometimes show toxic adverse effects.
8.Antifungal agents
Important ophthalmic fungal infections may be considered in the following three categories
a- Infections of the eyelids and surrounding skin.
b- Intraocular infection (usually endophthalmitis) associated with penetrating foreign bodies or systemic mycoses, such as Cryptococcosis, Blastomycosis, Histoplasmosis, and Coccidioidomycosis.
c- Mycotic keratitis following corneal penetration or ulceration.
Agents commonly used for treatment of patients with fungal endophthalmitis orb keratitis are
- Natamycin
Natamycin is antifungal agent available as a 5% ophthalmic suspension, which is viscous but will pass through ocular lavage systems in the horse without causing obstruction. It is effective against a broad variety of fungi, including Candida, Aspergillus, Cephalosporium, Fusarium, and Penicillium spp.
- Azoles
Itraconazole, ketoconazole, fluconazole, voriconazole, clotrimazole, and miconazole are members of the azole group.They are especially useful for the treatment of systemic and ocular Cryptococcus spp. and Coccidioides immitis infections. Side effects in dogs include inappetence, pruritus, alopecia, and reversible lightening of the hair coat. In cats, anorexia, fever, depression, and diarrhea may occur. Long-term therapy, up to 6 months or longer, may be necessary because the drugs are fungistatic. Most azoles do not cross the blood-ocular barriers well.
10.Anti-inflammatory
I- Corticosteroids
The most useful and powerful drugs as anti-inflammatory agent. The following are good general rules to help govern ophthalmic use of corticosteroids:
a- Corticosteroids must not be used topically or subconjunctivally when fluorescein indicates a corneal epithelial defect.
b- Every “red” eye should be stained with fluorescein and its IOP should be measured before indiscriminate therapy with corticosteroids is initiated.
c- For non-ulcerative corneal disease or intraocular disease, a penetrating topical corticosteroid such as prednisolone or dexamethasone must be administered. Hydrocortisone does not penetrate the cornea.
d- For inflammatory disorders of the eyelids, posterior segment, optic nerve, or orbit, corticosteroids must be administered systemically, not topically.
Uses of corticosteroids:
1- Immune-mediated ocular disorders (seasonal allergic conjunctivitis, drug and contact allergies, chronic superficial keratitis or “pannus,” eosinophilic keratoconjunctivitis, episcleritis, some cases of keratoconjunctivitis sicca, lensinduced uveitis, uveodermatologic (VKH-like) syndrome, etc.)
2- Traumatic conditions resulting in severe inflammation (proptosis of the globe, contusion with hyphema).
3- Anterior uveitis
4- Postoperative immunomodulation (e.g., after corneal transplant or cataract extraction)
5- Reduction of postoperative swelling and inflammation after cryosurgery (e.g., cyclocryotherapy or cryoepilation for distichiasis or eyelid tumors)
Methods of corticosteroid application and indications are
a) Topical.
b) subconjunctival injections.
c) Systemic administration.
Corticosteroids are contraindicated in the following conditions
• Epithelial lesions of the cornea.
• Viral, mycotic and bacterial infections.
• Glaucoma.
II- Non-steroidal anti-inflammatory drugs (NSAIDs)
Such as acetylsalicylic acid 10-25 mg/kg 3 times daily.
I- Antihistamines
Antihistamine solution is very effective topically Premedication with systemic antihistamine 20–30min before intraocular surgery as
- Sodium cromoglycate.
- Olopatadine.
- Lodoxamide.
12.Carbonic anhydrase inhibitors
The enzyme carbonic anhydrase is present in ciliary body epithelium, where it is responsible, in part, for aqueous humor production. The enzyme carbonic anhydrase inhibitors decreased intraocular pressure. Carbonic anhydrase inhibitors as
- Acetazolamide (Diamox) 0.5 – 2.5 mg/ kg. b.w.
- Methazolamide (Neptazane) 1 - 2 mg/kg b.w.
13- Antiparasitic Agents
Ivermectin is now used, almost to the exclusion of all older parasiticides, for treatment of parasitism such as Habronemiasis and onchocerciasis in horses and ocular filariasis in small animals.
14.Osmotic diuretics
Osmotic drugs are applied topically to clear or reduce corneal edema ,osmotic diuretics used in acute glaucoma, prior to intraocular surgery, traumatic proptosis of the globe, and clearing of corneal edema as
- Mannitol (Osmitrol).
- glycerol (Osmoglyn).
- urea (ureaphil) .
- Topical NaCl 5% ointment is used in corneal edema.
15.Vitamins
Various vitamins have been advocated for their supposed therapeutic efficacy in the treatment of ocular disorders of animals. In the absence of a specific vitamin deficiency (e.g., vitamin A deficiency causing nyctalopia in cattle or conjunctivitis in turtles) there usually is little to be gained from such local therapy. The exception is systemic and ocular signs of warfarin Poisoning which are treated with vitamin K and its analogues, Vitamin C and Riboflavin (B2).
16. Enzymes
- Fibrinolysin is used to remove clotted blood from the anterior chamber in traumatic hyphema.
- Alpha chymotrypsin (Alphapsin) is useful for absorption of intraocular debris in cases of hypopyon.
- Alpha chymotrypsin is a proteolytic enzyme used for removal of the lens by intracapsular extraction in cases of cataract.
17.Ophthalmic stains
Ophthalmic stains are used commonly as diagnostic aids in diseases of anterior and posterior segment and nasolacrimal system.
a) Fluorescein dyes: Fluorescein is available as solution of 0.5-2.0%. Filter paper strips impregnated with fluorescein may be placed in the conjunctival sac until moistened by tears. It is readily soluble in water produces a bright green fluorescent color. It is used in the following conditions
• An indicator dye for corneal epithelial defects.
• Detection of the patency of the nasolacrimal duct.
• Detection of the lesions of the retinal and uveal vasculature.
b) Rose Bengal: It stains devitalized cells and their nuclei of the cornea and conjunctiva.

Fig.34: Corneal ulcer in horse note the Fluorescein dyes stained the dead tissue not the life tissue.

Fig.35: Corneal ulcer in horse note the Rose Bengal dyes stained the life tissue not the dead tissue.
18. Artificial tears
Artificial tear preparations are used when the normal tear quality or quantity is altered or when loss of tears is increased due to evaporation, or, in some cases, primary corneal pathology. These agents are lacrimomimetic and are not to be confused with lacrimogenic agents, such as cyclosporine. The production of endogenous tears is always preferred over the replacement of tears with “artificial” tears.
Indications for tear replacement preparations are as follows
1- For treatment of keratoconjunctivitis sicca (“dry eye”).
2- For treatment of exposure keratitis (e.g., facial nerve paralysis, buphthalmos, breed-associated lagophthalmos).
3- In patients with abnormal tear film breakup time (qualitative tear film disturbances)
4- During and after general anesthesia to prevent corneoconjunctival desiccation
5- As a lubricant, refractive/electroconductive, and cushioning solution during gonioscopy and electroretinography
6- As a diluent for compounding of some ophthalmic solutions
7- In patients with primary corneal disease, such as feline corneal sequestration and canine superficial punctate keratitis.
19. Vasoconstrictors and decongestants
Vasoconstrictor and decongestant eye drops that work by narrowing the blood vessels in the eye which activate alpha-adrenergic receptors in the small blood vessels (arterioles) of the eye's outer layer (conjunctiva) to reduce redness and congestion. These drops are effective for temporary relief of symptoms like redness and irritation but can lead to a "rebound" effect, making the eyes redder if used too frequently or over the long term
Example
- Ephedrine 0.15%.
- Phenylephrine 0.15%.
20. Corneal dehydrating agents:
Corneal dehydrating agents for corneal edema and to preserve corneal tissue for transplantation. Hypertonic drops work by drawing water out of the cornea, while preservation agents are used to dry and store donor tissue, often maintaining its properties for later use.
For treatment of corneal edema
- Hypertonic saline 2-5%: Typically used as an ophthalmic solution or ointment, 5% sodium chloride draws water from the cornea to reduce swelling.
- Glycerin: A highly concentrated solution that can rapidly dehydrate the cornea, but it is often unsuitable for routine use due to burning and photophobia.
For preserving corneal tissue
- Silica gel: A common agent for preserving corneal tissue, it is particularly good at maintaining optical transmittance.
- Silicone oil: A novel agent being explored for its stability, low toxicity, and high hydrophobicity, which may be useful for corneal tissue storage.
- Polyethylene glycol (PEG): Used to dehydrate anterior corneal grafts to a normal thickness and restore transparency before procedures
- References
- Abrams K, et al. (1990): Evaluation of the Schirmer tear test in clinically normal rabbits. Am J Vet Res 51:1912.
- Acland GM (1988): Diagnosis and differentiation of retinal disease in small animals by electroretinography. Semin Vet Med Surg 3:15.
- Bauer GA, et al. (1996): Exfoliative cytology of conjunctiva and cornea in domestic animals: a comparison of four collecting techniques. Vet Comp Ophthalmol 6:181.
- Bedford PGC (1973): A practical method of gonioscopy and goniophotography in the dog and cat. J Small Anim Pract 14:601.
- Budras KD, et al. (2002): Anatomy of the Dog: An Illustrated Text. Schlütersche, Hannover, Germany.
- Calia CM, et al. (1994): The use of computed tomography scan for the evaluation of orbital disease in cats and dogs. Vet Comp Ophthalmol 4:24.
- Carastro SM (2004): Equine ocular anatomy and ophthalmic examination.Vet Clin North Am Equine Pract 20:285.
- Cottrill 1, W J Banks, R D Pechman 1989: Ultrasonographic and biometric evaluation of the eye and orbit of dogs Am J Vet Res 1989 Jun;50(6):898-903.
- Cottrill NB, et al. (1989): Ultrasonographic and biometric evaluation of the eye and orbit of dogs. Am J Vet Res 50:898.
- Duke-Elder S (1958, 1968): System of Ophthalmology: Vol. 1: The Eye in Evolution, and Vol. IV: Physiology of the Eye and of Vision. Henry Kimpton, London, pp. 605-706.
- Evans HE (1993): Miller’s Anatomy of the Dog, 3rd ed. Saunders, Philadelphia.
- Görig C, et al. (2006): Comparison of the use of new handheld tonometers and established applanation tonometers in dogs. Am J Vet Res 67:134.
- Hamor RE (2001): Techniques for collection and interpretation of tissue samples in ocular disease. Clin Tech Small Anim Pract 16:17.
- Karpinski LG (2004): The prepurchase examination. Vet Clin North Am Equine Pract 20:459.
- Leiva M, et al. (2006): Comparison of the rebound tonometer (ICare) to the applanation tonometer (Tonopen XL) in normotensive dogs. Vet Ophthalmol 9:17.
- Martin CL (1969): Gonioscopy and anatomical correlations of the drainage angle of the dog. J Sm Anim Pract 10:171.
- Martin CL (1969): Slit lamp examination of the normal canine anterior ocular segment part III: discussion and summary. J Small Anim Pract 10:163.
- Miller PE, Pickett JP (1992): Comparison of the human and canine Schiøtz tonometry conversion tables in clinically normal cats. J Am Vet Med Assoc 201:1017.
- Moore PA (2001): Examination techniques and interpretation of ophthalmic findings. Clin Tech Small Anim Pract 16:1.
- Ramsey DT, Ewart SL, Render JA, Cook CS, Latimer CA. Congenital ocular abnormalities of Rocky Mountain horses. Vet Ophthalmol 1999;2(1):47-59.