Dissociative Disorders
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | طب نفس الأطفال والمراهقين |
| كتاب: | Dissociative Disorders |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:02 AM |
الوصف
"last update: 20 November 2025" Download Guideline
- Executive Summary
These guidelines provide evidence-based recommendations for the assessment and management of dissociative disorders in children and adolescents. Dissociative disorders (DDs) are often misunderstood, underdiagnosed, and stigmatized, leading to delayed care and unnecessary suffering.
The recommendations emphasize:
- Exclusion of medical/neurological conditions before psychiatric diagnosis.
- Comprehensive psychiatric assessment incorporating trauma history, family context, and developmental needs.
- Psychotherapy as first-line treatment, delivered within a trauma-informed, family-inclusive framework.
- Cautious use of medication only for comorbidities such as depression or anxiety.
- System-level supports including anti-stigma interventions, psychoeducation, and clinician training.
The ultimate goal is to standardize care, reduce misdiagnosis, and improve outcomes for children and families across Egypt and similar contexts.
▪️ Comprehensive Medical and Neurological Assessment:
Children and adolescents presenting with dissociative symptoms must undergo a comprehensive medical and neurological evaluation to exclude organic causes such as epilepsy, syncope, metabolic disorders, migraines, and central nervous system pathology. This step is essential to prevent misdiagnosis and inappropriate psychiatric labelling. (Strong Recommendation)
▪️Comprehensive Psychiatric Assessment: Following medical clearance, children and adolescents with suspected dissociative disorders should receive a comprehensive developmentally informed psychiatric assessment. This should integrate information from multiple sources (child, caregivers, teachers), include trauma and attachment history, family context, and comorbid psychiatric conditions. (Strong Recommendation)
▪️Psychotherapy as First-Line: The first-line treatment for dissociative disorders in children and adolescents is psychotherapy. Individual psychotherapy should be developmentally tailored and trauma-informed, incorporating techniques from cognitive-behavioral therapy (CBT), dialectical behavior therapy (DBT) skills adapted for youth, psychodynamic therapy, and/or attachment-focused interventions. Family therapy should also be integrated to strengthen caregiver and relational support. Psychoeducation for the child, caregivers, and schools is essential to reduce stigma and improve coping. (Strong Recommendation)
Acute
Stress and Conversion Symptoms (First Month Post-Trauma):
For children and adolescents
presenting with symptoms of dissociative (conversion) disorders within the
first month after exposure to a potentially traumatic event, clinicians are not
advised to initiate specialized psychological interventions, as evidence does
not support their effectiveness. Instead, we
advise that early management includes the following:
-Exclusion of physical and neurological causes
-Provision of Psychological First Aid (PFA) focusing on comfort, stabilization, and safety
-Psychoeducation for the child and caregivers, explaining that symptoms may occur after extreme stress
-Respectful, culturally appropriate engagement, including safe collaboration with traditional/community supports
-Avoidance of reinforcing secondary gain from symptoms. (Conditional Recommendation)
▪️ Pharmacological Management: Pharmacological treatment is not indicated for dissociation itself in children and adolescents. Medications should only be considered for comorbid conditions such as depression, anxiety, or severe behavioral dysregulation. Benzodiazepines should be avoided, as they may worsen dissociative symptoms. (Strong Recommendation)
- Recommendations
• Comprehensive Medical and Neurological Assessment:
Children and adolescents presenting with dissociative symptoms must undergo a comprehensive medical and neurological evaluation to exclude organic causes such as epilepsy, syncope, metabolic disorders, migraines, and central nervous system pathology. This step is essential to prevent misdiagnosis and inappropriate psychiatric labelling.
Strong Recommendation
High Quality Evidence 2,4,5
• Comprehensive Psychiatric Assessment
Following medical clearance, children and adolescents with suspected dissociative disorders should receive a comprehensive developmentally informed psychiatric assessment. This should integrate information from multiple sources (child, caregivers, teachers), include trauma and attachment history, family context, and comorbid psychiatric conditions.
Strong Recommendation
Moderate Quality Evidence 2,4,5
• Psychotherapy as First-Line: The first-line treatment for dissociative disorders in children and adolescents is psychotherapy. Individual psychotherapy should be developmentally tailored and trauma-informed, incorporating techniques from cognitive-behavioural therapy (CBT), dialectical behaviour therapy (DBT) skills adapted for youth, psychodynamic therapy, and/or attachment-focused interventions. Family therapy should also be integrated to strengthen caregiver and relational support. Psychoeducation for the child, caregivers, and schools is essential to reduce stigma and improve coping
Strong Recommendation
High Quality Evidence 2,4,6
· Acute Stress and Conversion Symptoms (First
Month Post-Trauma):
For children and adolescents
presenting with symptoms of dissociative (conversion) disorders within the
first month after exposure to a potentially traumatic event, clinicians are not
advised to initiate specialized psychological interventions, as evidence does
not support their effectiveness. Instead, we
advise that early management includes the following:
-Exclusion of physical and neurological causes.
-Provision of Psychological First Aid (PFA)focusing on comfort, stabilization, and safety.
-Psychoeducation for the child and caregivers, explaining that symptoms may occur after extreme stress.
-Respectful, culturally appropriate engagement, including safe collaboration with traditional/community supports
-Avoidance of reinforcing secondary gain from symptoms.
Conditional Recommendation
Very Low-Quality Evidence 7
Pharmacological treatment is not indicated for dissociation itself in children and adolescents. Medications should only be considered for comorbid conditions such as depression, anxiety, or severe behavioural dysregulation. Benzodiazepines should be avoided, as they may worsen dissociative symptoms.
Strong
Recommendation
Moderate Quality Evidence 2,6
- Acknowledgement
We would like to acknowledge the Child and Adolescent Psychiatry Scientific Committee and Egyptian Child and Adolescent Psychiatry Association ECAPA for developing these guidelines.
Chair of the GDG: Suaad Moussa, Prof. of Psychiatry, Cairo University
Members of the Guideline Development Group (GDG):
1. Prof. Azza ElBakry, Professor of Psychiatry, Cairo University.
2. Dr. Aliaa Magdy, Lecturer of Psychiatry, Cairo University.
3. Prof. Aref Khoweiled , Professor of Psychiatry, Cairo University.
4. Prof Dina Mohamed El-Gabry, Professor of Psychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Ain Shams University.
5. Dr. Dina Massoud, Maamora Psychiatry Hospital
6. Dr. Dina Youssri Afifi, Assistant Prof. of Psychiatry, Cairo University.
7. Dr. Eman Gaber, Psychiatric Consultant, Deputy of Central Administration of General Secretariat of Mental Health GSMHAT.
8. Dr Gellan Karamallah Ramadan Assistant Professor in Neurology and Psychiatry Department, Assuit University.
9. Prof. Hanan Mohamed Ezzeldin Azzam, Professor of Psychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Ain Shams University.
10. Dr. Heba Essam Abou El Wafa, Professor of Psychiatry- Alexandria University.
11. Prof. Heba Hamed Elshahawi, Professor of Psychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department,Ain Shams University.
12. Dr. Helen Soliman, Head of child & Adolescent Psychiatry Unit -Maamora Psychiatry Hospital.
13. Prof. Hisham Salah Zaki, Professor of Psychiatry- Beni-Suef University.
14. Dr. Israa ElSharif, Lecturer of Psychiatry, Cairo University.
15. Prof. Maha Emadeldin, Professor of Psychiatry, Beni-Suef University.
16. Prof. Maha Mohamed Sayed, Professor of Neuropsychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Ain shams University. 2Chi
17. Prof. Manal Omar, Ass. Professor of Psychiatry, Faculty Of Postgraduate Childhood Studies, Ain Shams University.
18. Dr. Mariam Ehab Dawoud, Ass Prof. of Psychiatry Faculty of Medicine Fayoum University.
19. Dr. Marwa Nasr, Maamora Psychiatry Hospital
20. Prof Mahmoud Elwasify Professor of Psychiatry- Mansoura University.
21. Dr. Mohamed Elshiekh, Professor of Psychiatry, Ain Shams University.
22. Prof. Mohamed Nasreldin Sadek, Professor of Psychiatry, Faculty of Medicine Cairo University.
23. Prof Mohammad Abdelhakeem Seleem, Professor of Psychiatry, Tanta University.
24. Dr. Mona Mahmoud El Sheikh, Professor of Neuropsychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Faculty of Medicine, Ain Shams University.
25. Dr. Nahla Radwan, Consultant Psychiatrist, Ministry of Health.
26. Dr. Nermin Mahmoud Shaker, Professor of Psychiatry, Okasha Institute of Psychiatry, Neuropsychiatry Department, Ain Shams University.
27.Dr. Nermin Elsallami, Maamora Psychiatry Hospital
28. Prof. Ola Shaheen, Professor of Psychiatry, Cairo University.
29. Dr. Rana Walid Ibrahim Hamimy, Lecturer of Psychiatry, Cairo University.
30. Prof Salwa Tobar, Prof. of Psychiatry, Mansoura University
31. Dr. Sara Galal, Assistant Lecturer in Medical Department, Faculty of Postgraduate Childhood Studies. Ain Shams University.
32. Prof. Soha Abdel Latif Ghobashy, Professor of Psychiatry Alexandria University.
33. Dr. Walaa Fakher, Associate Professor of Psychiatry, Cairo University.
34. Dr. Walaa Hussny Elsaied, Consultant of Psychiatry- Head of Child & Adolescent Psychiatric Administration GSMHAT-Ministry of Health.
35. Prof. Yomna Sabry, Professor of Psychiatry Mansoura University
We would like to acknowledge the efforts of
Supervisor of the EHA Pediatric Protocols General Doctor/ Mourad Alfy Ramzy Tadros
• MD, FRCPCH(UK), MRCPI(Dublin)
• Consultant Paediatrician of Egyptian Military Medical Services.
• Professors of Paediatrics Military Medical Academy
• Head of Training Committee of Paediatrics of Egyptian Military Medical Board
• Consultant Paediatrician of the Medical Advisory Council of Egypt Healthcare
Authority (EHA).
Coordinators & Editing Supervisors
1. Dr. Hala Adel: Pediatric Consultant, Moderator & coordinator of Medical
Advisory Council of Egypt Healthcare Authority (EHA)
2. Dr. Huda Karam: Pediatric Specialist, Moderator & coordinator of Medical
Advisory Council of Egypt Healthcare Authority (EHA)
Cover Designed & Edited By
- Mr. Bassam Sayed: Technical Officer at Medical Advisory Council of Egypt
- Abbreviations
AACAP: American Academy of Child and Adolescent Psychiatry
CBT: Cognitive Behavioural Therapy
DBT: Dialectical Behaviour Therapy
DD: Dissociative Disorders
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition
ECAPA: Egyptian Child and Adolescent Psychiatry Association
EMDR: Eye Movement Desensitization and Reprocessing
GDG: Guideline Development Group
GRADE: Grading of Recommendations, Assessment, Development and Evaluation
ICD-11: International Classification of Diseases, 11th Edition
ISSTD: International Society for the Study of Trauma and Dissociation
NGOs: Non-Governmental Organizations
PFA: Psychological First Aid
PTSD: Post-Traumatic Stress Disorder
TF-CBT: Trauma-Focused Cognitive Behavioural Therapy
WHO: World Health Organization.
- Glossary
Dissociation: Disruptions in consciousness, memory, identity, or perception, often in response to trauma or overwhelming stress.
Conversion Symptoms: Neurological-like symptoms (e.g., paralysis, seizures) without a medical basis, arising from psychological stress.
Trauma-Informed Care: An approach that emphasizes safety, trust, and avoidance of re-traumatization while recognizing the impact of trauma on behaviour and emotions.
Psychological First Aid (PFA): Immediate, supportive, non-intrusive care offered after traumatic events to promote safety, stabilization, and coping.
Stigma: Negative social attitudes or beliefs toward individuals with dissociative symptoms, leading to discrimination or treatment delays.
Regression: A return to earlier developmental behaviors (e.g., bedwetting, baby talk, clinging) in response to psychological stress or trauma, commonly observed in younger children with dissociative symptoms.
Trance-like State: An altered state of consciousness characterized by unresponsiveness to the external environment, fixed staring, or automatic behaviors, often observed in dissociative presentations or after traumatic events.
- Introduction
Dissociative disorders (DD) in children and adolescents are a complex group of psychiatric conditions marked by disruptions in consciousness, memory, identity, perception, and behaviour. These symptoms often develop as involuntary coping mechanisms in response to trauma or overwhelming stress, and they frequently impair a child’s social, academic, and emotional functioning (1, 2). Although primarily psychological, dissociative symptoms may resemble or coexist with neurological or developmental conditions, making careful assessment and exclusion of physiological causes essential (2).
DDs may present early in life, sometimes from the age of three, and their manifestations can vary widely across developmental stages. In young children, symptoms may take the form of regression, trance-like episodes, or imaginary companions that appear unusually vivid or controlling. In school-aged children, dissociation may emerge through unexplained amnesia, abrupt changes in behaviour or identity, or somatic complaints without a medical basis. During adolescence, presentations often become more structured, with clearer episodes of amnesia, identity disturbance, depersonalization, derealization, or trance states (2, 3). Because presentation may overlap with normal developmental behaviour, careful attention to features that are inconsistent with developmental expectations—such as loss of control, memory gaps, or functional impairment—is essential for timely recognition. The ICD-11 framework identifies Dissociative Identity Disorder, Dissociative Amnesia, Depersonalization-Derealization Disorder, and trance or possession states as part of this spectrum (1).
These Egyptian Guidelines aim to provide practical recommendations for doctors working with children and adolescents. They recommend evidence-based and culturally appropriate interventions, with particular focus on early recognition, accurate differentiation, and trauma-informed care. In Egypt, where family bonds and community traditions strongly shape children’s development, clinicians should consider cultural meanings of distress and use family-engaged, school-linked pathways to ensure care that is both effective and respectful.
- Scope and Purpose
This chapter provides guidance on psychotherapeutic interventions for Dissociative disorders in children and adolescents to be used by policymakers, mental health professionals, and primary health care providers to offer better treatment strategies.
The objective of this chapter is to standardize practice to decrease variation of practice and improve outcomes for affected children and their families.
- Target Audience
This guideline targets child and adolescent psychiatrists, psychiatrists, general practitioners, mental health professionals (clinical psychologists, social workers), family physicians, pediatricians, policy makers, as well as non-governmental organizations (NGOs) and other stakeholders to offer the most appropriate treatment guidelines for children with reactive attachment disorder.
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria were followed in the search and retrieval of guidelines to be adapted:
- Selecting only evidence-based guidelines (guidelines must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines
· Selecting peer-reviewed publications only
· Selecting guidelines written in the English language
· Excluding guidelines written by a single author, not on behalf of an organization, to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references, as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt the Guidelines for the management of conditions specifically related to stress by the WHO and the Guidelines of the International Society for the Study of Trauma and Dissociation (ISSTD) . 4,7
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of
Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because they represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
Table 1 Quality and Significance of the four levels of evidence in GRADE:
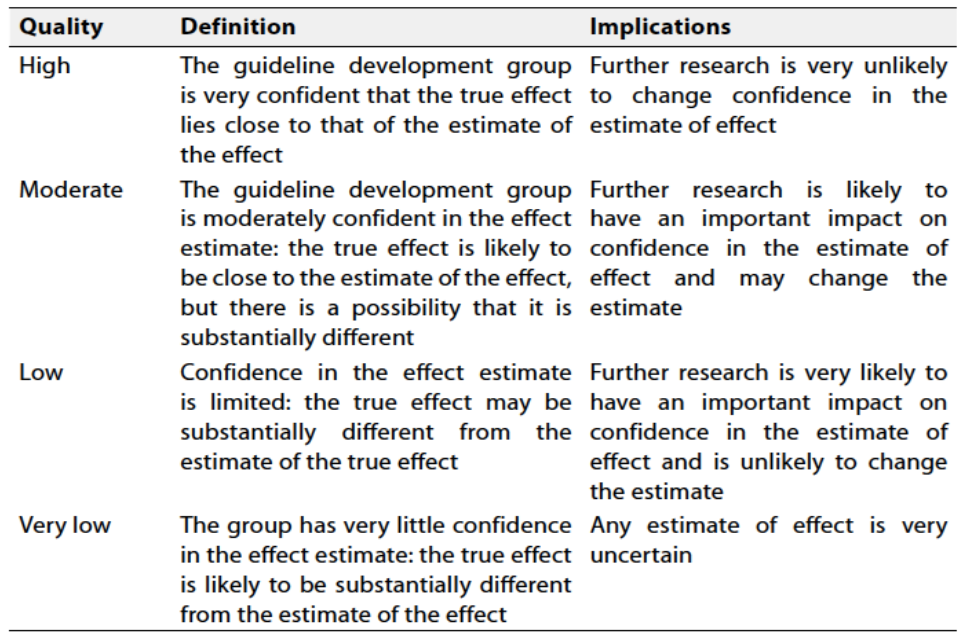
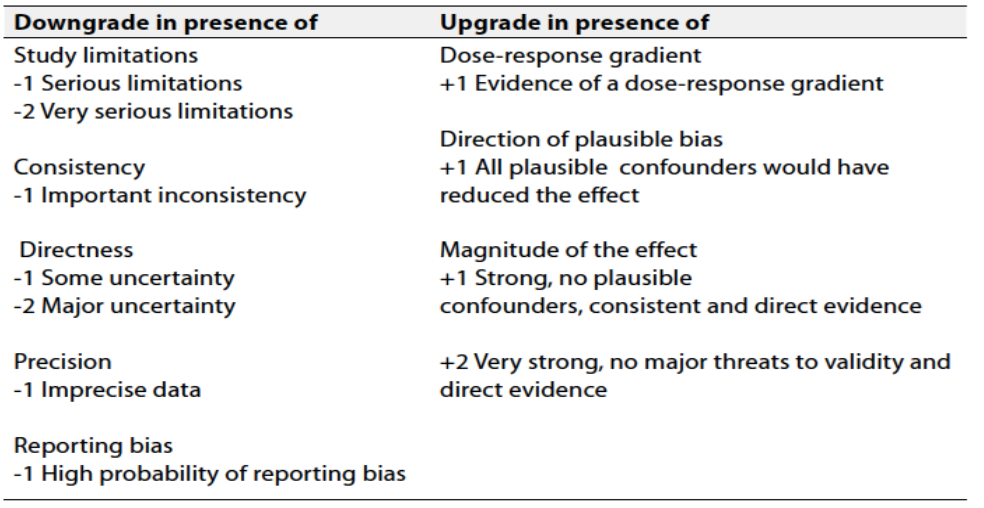
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation should account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Implementation Considerations
Several barriers may hinder the effective implementation and scale-up of these recommendations for dissociative disorders in children and adolescents:
- Stigma and misinterpretation: Families and schools may mislabel dissociative symptoms as behavioural problems or attention-seeking, which delays care.
- Cultural beliefs: In many settings, dissociation may be explained through spiritual or supernatural frameworks, leading families to seek non-medical care first.
- Resource limitations: There is a shortage of trained child psychiatrists, psychologists, and allied professionals skilled in trauma and dissociation.
- Access inequities: Rural areas and refugee populations often lack specialized services.
- Financial constraints: Psychotherapy and long-term care may not be accessible due to cost and specialized training gaps.
By addressing these barriers through awareness campaigns, training programs, tele-supervision, and integration of dissociation management into national child mental health policies, implementation can be strengthened.
- Research Needs
During the review of evidence and development of recommendations, several research gaps were identified for dissociative disorders in children and adolescents:
- Long-Term Effectiveness: Conduct follow-up studies to evaluate the long-term outcomes of trauma-focused therapy, play therapy, family interventions, and attachment-based approaches.
- Tailoring Interventions: Examine how personal traits (e.g., temperament), cultural factors, socioeconomic status, mental health literacy, and stigma influence treatment outcomes.
- Cost-Effectiveness: Assess the economic impact of psychotherapeutic and adjunctive programs, weighing cost against clinical and functional improvements.
- Service Delivery Models: Evaluate the effectiveness of tele-mental health and task-sharing models for dissociative disorders in resource-limited settings.
- Monitoring and Evaluating the Impact of the Guideline
Potential indicators for evaluating the success of dissociative disorder interventions include:1. Early Identification: Equip GPs and non-specialist clinicians with the tools and confidence to recognize dissociative symptoms.
2. Appropriate Referral Pathways: Encourage timely referrals to specialized services, reducing delays in treatment.
3. Reduction in Misdiagnosis: Differentiate dissociative symptoms from other psychiatric or neurological conditions (e.g., epilepsy, psychosis, ADHD).
4. Integrated Care: Promote collaboration between GPs, psychiatrists, psychologists, pediatricians, and educators.
5. Reducing Stigma
Raise awareness and provide education to reduce fear, shame, or misunderstanding about dissociative disorders. Reducing stigma helps people feel safer asking for help and improves their recovery.
- Update of the Guideline
This guideline will be updated whenever there is new evidence
- References
- International Classification of Diseases 11th Revision; World Health Organization, 2019/2021
2. Agarwal V, Sitholey P, Srivastava C. Clinical practice guidelines for the management of dissociative disorders in children and adolescents. Indian J Psychiatry. 2019;61(Suppl 2):247-53. doi: 10.4103/psychiatry.IndianJPsychiatry_493_18
3. Nowak M, Szyszka M, Lewicka W. Dissociative disorders in children—literature review. Pediatr Pol. 2023;98(3):223-8. doi: 10.5114/polp.2023.130988
4. International Society for the Study of Trauma and Dissociation. Guidelines for the evaluation and treatment of dissociative symptoms in children and adolescents. J Trauma Dissociation. 2003;4(4):109-53. doi: 10.1300/J229v05n03_09
5. Kedare JS, Baliga SP, Kadiani AM. Clinical practice guidelines for assessment and management of dissociative disorders presenting as psychiatric emergencies. Indian J Psychiatry. 2023 Jan 30;65(2):186-95. doi:10.4103/indianjpsychiatry.indianjpsychiatry_493_22
7. World Health Organization. Guidelines for the management of conditions specifically related to stress. Geneva: World Health Organization; 2013.
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
- Annex
Annex: Dissociative Disorders – DSM-5 and ICD-11 Criteria
Table 1: DSM-5 Dissociative Disorders (core criteria, summarized)
|
1. Dissociative Identity Disorder (DID) Code 300.14
2. Dissociative Amnesia Code 300.12
3. Depersonalization/Derealization Disorder Code 300.6
4. Other Specified Dissociative Disorder (OSDD) Code 300.16
5. Unspecified Dissociative Disorder (UDD) Code 300.15
|
Adapted from: American Psychiatric Association (8).
Table 2: ICD-11 Dissociative Disorders (6B codes)
|
6B64 Dissociative Identity Disorder
6B61 Dissociative Amnesia
6B66 Depersonalization-Derealization Disorder
6B60 Dissociative Neurological Symptom Disorder (Functional Neurological Disorder)
6B6Y Other Specified Dissociative Disorder
6B6Z Dissociative Disorder, unspecified
6B62 Trance Disorder · Characterized by trance states in which there is marked alteration in the individual's state of consciousness or a loss of the individual's customary sense of personal identity, in which the individual experiences a narrowing of immediate surroundings or unusual narrowing or selective focus on environmental stimuli. The trance state is involuntary and unwanted and is not accepted as a part of collective or religious practice. |
Adapted from: International Classification of Diseases 11th Revision (1).