UPPER AND LOWER EYELIDS AFFECTION
| Site: | EHC | Egyptian Health Council |
| Course: | Veterinary Ophthalmology Guidelines |
| Book: | UPPER AND LOWER EYELIDS AFFECTION |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:34 AM |
Description
"last update: 7 December 2025" Download Guideline
Table of contents
- - Acknowledgement
- - Structure of the eyelids
- - I.EYELID AGENESIS (COLOBOMA)
- - II-PROMINENT NASAL FOLDS
- - III- DISORDERS OF THE CILIA
- - IV- ENTROPION OF THE EYELID
- - V- Ectropion of the eyelid
- - VI- Blepharitis
- - VII- Ptosis (blepharoptosis)
- - VIII- Traumatic eyelid injuries
- - IX- Eyelid tumors
- - X- Eyelid abscesses
- - XI- Chalazion (Meibomian cyst-Tarsal cyst)
- - XII- Hordeolum (stye) AND MEIBOMIAN ADENITIS
- - XIII- Lagophthalmia
- - References
- Acknowledgement
We would like to acknowledge the committee of National Egyptian Guidelines for Veterinary Medical Interventions, Egyptian Health Council for adapting this guideline.
Executive Chief of the Egyptian Health Council: Prof. Dr Mohamed Mustafa Lotief.
Head of the Committee: Prof. Dr Ahmed M Byomi
The rapporteur of the Committee: Prof. Dr Mohamed Mohamedy Ghanem.
Scientific Group Members: Prof. Dr Nabil Yassien, Prof. Dr Ashraf Aly Eldesoky Shamaa, Prof. Dr Amany Abbas, Prof. Dr Dalia Mansour, Dr Essam Sobhy Dr Mohamed Elsharkawy, Prof. Dr Gamal A. Sosa., Dr Naglaa Radwan, Dr Hend El Sheikh
Scientific Editor/Authors: Prof. Dr Ashraf Aly Eldesoky Shamaa. Dr Mohamed Elsharkawy. Prof. Dr. Mohamed Mostafa Saied Amer, Prof. Dr. Shaaban Mohamed and Dr. Mohamed Moustafa Bahr Moustafa.
- Structure of the eyelids
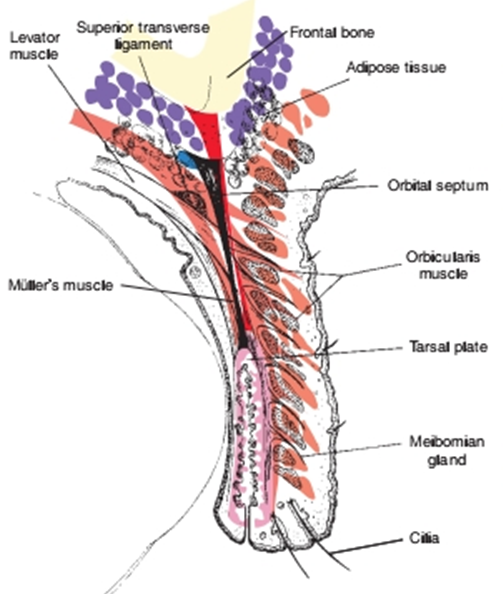
Fig.1:. Structure of the normal eyelid. (Remington, 2005).
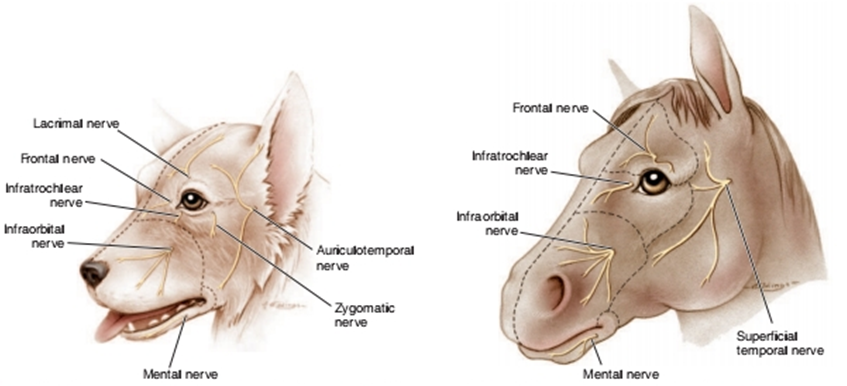
Fig.2: Sensory innervation of the canine periocular area. Fig.3: Sensory innervation of the equine
(Westhues and Fritsch, 1964 periocular area. (Westhues and Fritsch, 1964)
The eyelids protect the eye in the following ways
1. Sensory and protective effects of the cilia and sensory vibrissae surrounding the eye.
2. Secretions of the meibomian glands and conjunctival goblet cells, which contribute to the outer lipid and inner mucopolysaccharide layers of the precorneal tear film, respectively.
3. Physical protection against trauma.
4. Reduction of evaporation of tears.
5. Distribution of the precorneal tear film by eyelid movements.
6. “Pumping” of tears down the nasolacrimal duct, preventing epiphora and promoting a precorneal tear film of uniform thickness and optical properties.
- I.EYELID AGENESIS (COLOBOMA)
It’s a congenital absence of a portion of an eyelid. It can occur in all species but it is most common in cats. It’s a hereditary condition which associated with excessive evaporation and inadequate dispersion of the precorneal tear film, these lead to secondary keratoconjunctivitis, pain, and sometimes corneal ulceration. If the lower eyelid is affected, epiphora may occur owing to escape of tears through the defect.
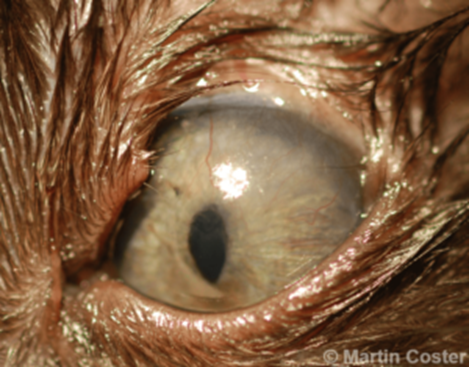
Fig.4: Superior eyelid agenesis in a cat (Belhorn et al, 1971).
Treatment
- Eyelid colobomas are repaired with a blepharoplastic surgery.
- II-PROMINENT NASAL FOLDS
Unusually prominent of the nasal folds in same species like Pekingese, pugs, English bulldogs, Boston terriers, and similar brachycephalic breeds.
If nasal folds are causing keratitis, they should be removed either partially or totally, in partial removing (only the medial portion of the fold is removed, where it touches the cornea, resulting in less alteration from the breed “norm” .

Fig.5: A 2 year old male Pug diagnosed and undergoing treatment for a corneal ulcer in his left eye (Rowena et al, 2015).

Fig.6: Crushing of the nasal fold before its excision.
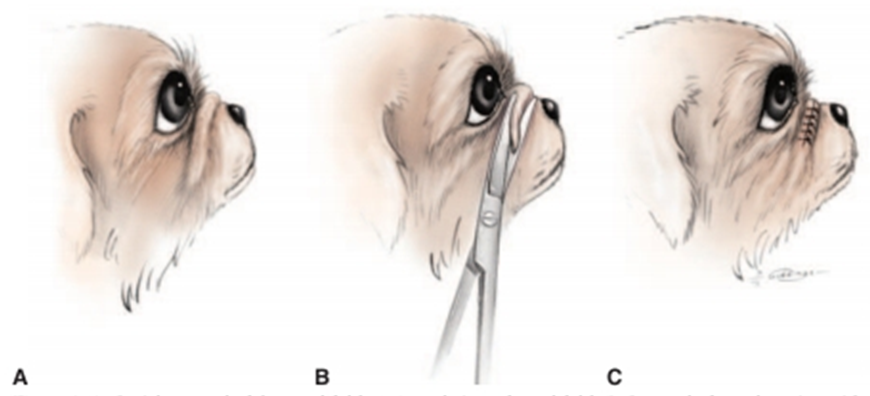
Fig.7: Partial removal of the nasal fold. (Redrawn, 2000).
A- Lateral view of nasal fold.
B- Removal of nasal portion with curved scissors.
C- The sutured wound, the knots are placed on the anterior side
of the incision in order to limit corneal contact.

Fig.8: Total removal of the nasal fold (Redrawn, 2000).
A- Removal of the fold, starting laterally.
B- The fold removed.
C- The fold sutured. The knots are placed on the anterior side of the incision in order to reduce the chance of corneal contact.
- III- DISORDERS OF THE CILIA
Normally positioned cilia emerge from the dermal side of the eyelid margin. Cilia
disorders can be bilateral or unilateral and can affect upper or lower eyelids.
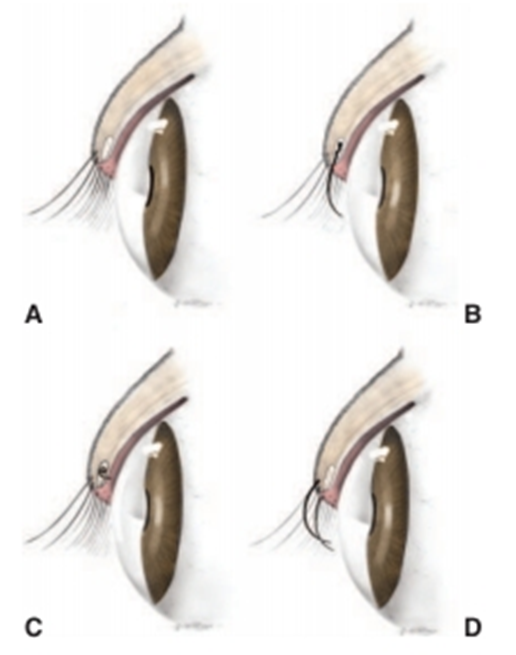
Fig.9: A- Normal eyelid (David et al, 2008).
B- Distichiasis. Cilia emerge from the meibomian gland orifice.
C-Ectopic cilium. The cilium arises from the meibomian gland but emerges
through the palpebral conjunctiva.
A- Trichiasis. Normal cilia or hairs arising from a normal location reach the cornea due to altered facial or eyelid conformation.
Clinical Signs of Cilia Disorders
1- Epiphora: Excess tearing and staining of facial hairs is usually present despite patency of the nasolacrimal apparatus.Purulent discharge is unusual except with corneal ulceration.
2- Blepharospasm: Pain associated with constant irritation and sometimes corneal ulceration is evident as blepharospasm.
3- Chronic conjunctival hyperemia:
4- Corneal ulceration
The three common disorders in which aberrant cilia or hair cause corneoconjunctival irritation are as follows
A- Distichiasis
It means presence of a second abnormal row of eyelashes. The condition is congenital. Without clinical evidence of irritation, they are considered insignificant.

Fig.10:Marked distichia of both lids, but only visualized
well in the photo of the upper lid of a Shih TzuSymptoms
1. Blepharospasm, conjunctivitis.
2. keratitis and corneal ulceration.
3. Presence of abnormal cilia.
Treatment
1. Manual epilation: by rounded tip epilation forceps.
2. Removal of a V-shaped segment of the tarso-conjunctiva containing distichia.
3. “Eyelid-splitting” and partial tarsal plate excision techniques as postoperative cicatricial entropion, scarring of the eyelid margin, and destruction of the meibomian glands.
4. Cryoepilation or electroepilation
Simple epilation by forceps without adjunctive cryotherapy or application of an electric current is a temporary measure because the cilia regrow within 3 to 4 weeks.
Electroepilation
- For treating a small number of follicles but tends to be less reliable.
- By supplies direct current (1 to 5 mA) to the offending meibomian gland, destroying it by electrolysis.
- A fine needle (25 or 26 gauge) can be used as the applying electrode. It is passed alongside the cilium and into the follicle with use of adequate magnification. Current is applied for 20 to 30 seconds. Easy removal of the cilium, which often adheres to the epilation needle, indicates follicle destruction.
Cryoepilation:
- For treating a large numbers of follicles.
- takes advantage of the selective susceptibility of hair follicles to cold. A nitrous oxide or liquid nitrogen cryoprobe is applied to the conjunctiva overlying the meibomian glands that contain the offending cilia. The ice ball is observed as it advances over the line of gland openings on the eyelid margin. Two rapid freeze–slow thaw cycles are used. Following thawing of the second freeze, a systemically administered corticosteroid or nonsteroidal antiinflammatory drug (NSAID). An oral NSAID may be continued postoperatively for analgesia. An antibiotic-steroid ophthalmic ointment .
A- Ectopic cilia
Ectopic cilia mean single or multiple cilia arise from the meibomian glands emerging from the conjunctival surface of the eyelid, where they cause marked corneal irritation and usually ulceration. The condition is congenital and observed after several months to several years of age. They are visible only with the illumination and magnification provided by a slit-lamp or operating microscope.
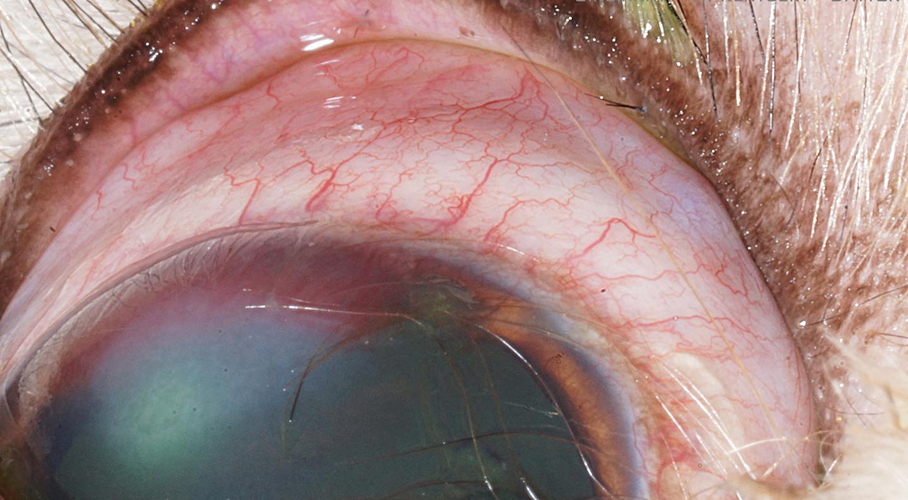
Fig.11: ectopic cilia in upper eye lid of cat (David et al, 2008).
Symptoms
1. Presence of ectopic cilia at the palpebral conjunctiva 2-6 mm from the lid margin.
2. Blepharospasm.
3. epiphora and conjunctivitis especially at the bulbar conjunctiva.
4. Vascularization of adjacent parts of the cornea accompanied by an elongated superficial corneal ulcer.
Treatment
- Electro-epilation of ectopic cilia.
- Surgical removal of the cilia with part of tarso-conjunctiva containing the follicle.
- resection of the affected cilium and meibomian gland under magnification.
- An elliptical Desmarres chalazion clamp with screw lock is placed around the cilium for hemostasis, and the eyelid is everted. A block of tissue containing the offending follicle and meibomian gland is removed with a small (No. 65 Beaver) scalpel blade, leaving the eyelid margin intact. No sutures are placed. Digital pressure for several minutes is sufficient to control hemorrhage.A topical broad-spectrum antibiotic ointment is applied three times daily for 5 to 7 days.
A- Trichiasis
Cilia or adjacent skin hairs arising from a normal location are misdirected so that they touch the cornea which irritates the globe and/or conjunctiva. This may be a primary condition (congenital) but is also a consequence of nasal folds, eyelid coloboma, eyelid agenesis, and entropion.

Fig12:Trichiasis due to prominent nasal folds in a Pekingese dog
Symptoms:
1. Epiphora: Excess tearing and staining of the medial canthal skin is present.
2. Blepharospasm: Pain associated with constant irritation of the cornea and conjunctiva resulting in blepharospasm and rubbing of the eye.
3. Chronic conjunctival erythema: The conjunctival blood vessels are engorged with blood.
4. Corneal ulceration: Ulcers caused by cilia are usually shallow and eccentrically placed on the cornea corresponding to the position of cilia.
5. Presence of abnormally directed cilia towards the eyeball.
Treatment
Depending on location of the offending hairs, is treated with any of the following:
1. Regular trimming of the periocular hairs.
2. Forceps epilation
3. Electro-epilation
4. Cryoepilation of the offending hairs. Especially at the medial canthus when there are a large number of hairs on the inner surface of the canthus and on the medial caruncle.
5. Surgical correction of the deformity causing the trichiasis (e.g., entropion, nasal folds, eyelid coloboma).
6. Surgical removal of dermoids
- IV- ENTROPION OF THE EYELID
-Entropion
Inward rolling of the eyelid margin
Fig.13: Entropion of the lower eyelid in a foal.

Fig.14: Entropion of
the upper eyelid in a goat.
Causes
1- Conformational.
2- Spastic.
3- cicatricial .
4- subsequent to alteration in globe position (enophthalmos) or size (phthisis/microphthalmos).
Clinical Signs of Entropion
1- Rolling in of the eyelid.
2- Blepharospasm with further rolling in of the eyelid (“spastic entropion”).
3- Excoriation and maceration of the eyelid surface from constant contact with tears.
4- Rubbing of the affected area.
5- Corneal ulceration.
6- Corneal melanosis and vascularization in chronic cases.
7- Conjunctival hyperemia.
8- Epiphora or mucoid discharge.
Treatment of Entropion
- The various methods of treating entropion depend on the level of facial maturity, species, severity and position of eyelid abnormality.
- Eliminate other causes of spastic entropion before deciding on the extent of surgical resection.
- entropion progresses or improves with maturity in some animals, permanent surgical correction of entropion is best delayed until facial maturity is reached.
The general principles apply to all surgical techniques are
1- Accurately assess extent of skin resection before induction of anesthesia.
2- Undercorrection, with the need for a second operation, is preferable to overcorrection, which causes cicatricial ectropion.
3- Minimize surgical tissue trauma.
4- It is not necessary to remove orbicularis oculi muscle; doing so increases hemorrhage, operating time, postoperative edema, and risk of infection.
5- Use fine suture material (4/0 or smaller in dogs and cats).
6- Place multiple, closely spaced sutures of small “bites.”
7- Use an Elizabethan collar until 2 to 3 days after suture removal.
8- Provide adequate postoperative analgesia for the first 7 to 10 days.
9- For the first few days after surgery, while the tissues are swollen, the eyelid may appear overcorrected, but as swelling subsides (over 5 to 7 days) the correction can be better evaluated.
The technique of correction Entropion
1- Temporary “Tacking” Techniques ( Stapling technique - Suture technique)
- When surgery should not be performed in patients with a temporary cause of entropion, such as transient enophthalmos due to lack of orbital fat, as in young animals, especially foals.
- surgical staples have been used as they are quicker, less traumatic, and less irritating,
Persist in the tissue longer than sutures, and can be applied without general anesthesia.
- An Elizabethan collar can often be removed a few days after staples are placed.
- A topical antibiotic ointment is used initially.
- The staples are left in place for as long as necessary. In some animals tacking may have to be repeated several times until facial maturity is reached and permanent corrective surgery can be performed.
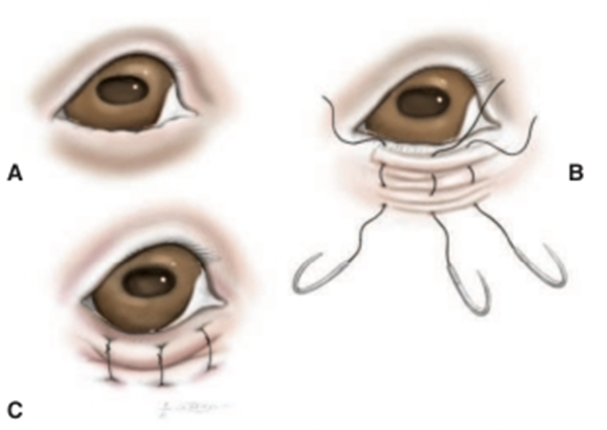
Fig. 15: Temporary “tacking” sutures used to correct entropion in immature animals or animals with a transient cause for Entropion(David et al, 2008).
A- Lower eyelid entropion.
B- Placement of a series of vertical mattress sutures.
- The first bite is taken very close to the eyelid margin, and the second bite is taken a few millimeters distant to the first. A 2/0 or 3/0 nylon suture is recommended.
C- As the suture is tightened a small furrow between the two bites is created and causes the eversion of the eyelid. The sutures are tied with the knots as distant from the eye as possible.

Fig.16: Lower eyelid entropion in a Labrador retriever puppy that
temporarily everted with surgical staples (David et al, 2008).
1- Injection Technique in Lambs
- entropion in lambs has been treated with subcutaneous injection of a liquid to physically alter lid alignment.
- Various fluids have been injected to evert the lower eyelid. A subcutaneous injection of Injection of procaine penicillin or long-acting tetracycline , also sterile air (5-15 ml) is effective in many cases.
2- Wedge Resection
- If the cause of entropion is euryblepharon (elongated eyelids), the lower eyelid can be shortened by resection of a full-thickness wedge from its lateral end.
- If the entropion is associated with a “notch” deformity, the wedge can be repositioned to remove the deformed tissue. As with all incisions that involve the eyelid margin, accurate apposition with a two-layer closure is essential.
|
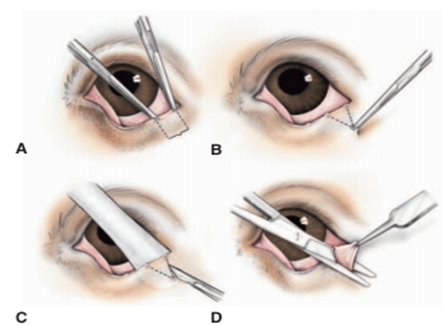
Fig.17: Eyelid wedge resection (David et al, 2008). A- The extent of eyelid margin resected with hemostats or with a dermatologic marker pen. B- The apex of the triangle or “wedge”resected in a similar manner. Usually the height of this triangle is approximately twice its base. C- The skin incision is made with a No. 15 Bard-Parker scalpel while the eyelid is supported by a Jaeger lidplate. D- The subcutis and conjunctiva are cut with straight Mayo or Stevens’s tenotomy scissors, so that the tissue wedge is completely resected.
|
|
Fig.18: Standard two-layer closure technique (David et al, 2008). A- This technique is used for all eyelid wounds that involve the eyelid margin. B- A buried 3/0 to 5/0 absorbable horizontal mattress suture without penetrating the skin, the margin itself, or the conjunctiva. Suture is placed so that the appositional forces are at the margin, but the knot is distal from it so as to avoid corneal contact ,from the eyelid margin to the apex of the incision so as to close the sub cutis. C- The skin is closed using a figure-of-eight suture of 3/0 or 4/0 silk or braided nylon. Both suture ends are left long at this stage. D- The rest of the skin incision is closed with a series of closely spaced simple interrupted sutures. The ends of the figure-of-eight suture are incorporated into the knot of the firs simple interrupted suture so that they are directed away from the eye. |
1- Hotz-Celsus Procedure
- If the cases are simple, breed-related or conformational entropion can be using a Hotz-Celsus procedure.
- The initial incision parallel to the eyelid margin should be made at the haired-non haired border.
- The length of this first incision is dictated by the length (extent) of inverted eyelid.
- Gentle pressure with the thumb on the lower lid at the point of entropion until the eyelid margin (meibomian gland orifices) can be seen along the whole length will assist with outlining the full lateral and medial extent of entropion.
- The tendency is to make this incision too.
- The real “art” of entropion surgery is in deciding on the amount of tissue to be resected at the widest point.
- The most important point is to ensure that the
- Use of calipers or some other simple method of measurement may assist in resection of a symmetric portion of the contralateral eyelid if that is required.
- The skin incisions are best made with a No. 15 Bard-Parker or No. 64 Beaver scalpel blade.
- The eyelid tissue is then best resected with a small pair of tenotomy scissors such that it has a V-shaped or boat keel–shaped profile.
- The wound is then closed with multiple, small, closely spaced, simple interrupted sutures of 3/0 or 4/0 braided nylon or silk.
- Sutures should be placed perpendicular to the eyelid margin.
- It is easily performed by placement of the first suture centrally (at the widest point of resection) and placement of each subsequent suture such that it bisects the distance still to be sutured.
- Topical antibiotic ointment, an Elizabethan collar, and a systemically administered NSAID for analgesia. Systemic antibiotics are not necessary. Sutures can be removed approximately 10 days postoperatively.
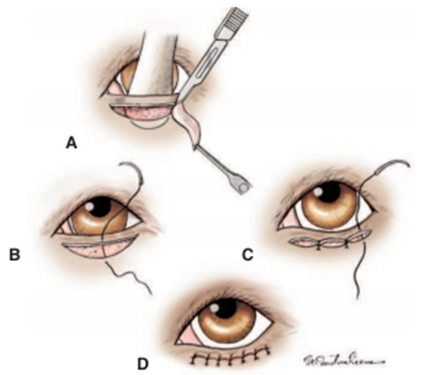
Fig.19: Hotz-Celsus procedure for correction of Entropion (Moore and Constantinescu,1997)
A- A Jaeger lid plate is inserted into the conjunctival fornix to provide support for the incisions.
- The initial incision is made parallel to the eyelid margin at the haired-nonhaired border.
- A second incision is made that arcs between the ends of the first incision.
- The width of the skin to be removed determines the extent of eversion this procedure will create.
B- The defect is closed with a series of simple interrupted skin sutures.
- The first suture placed should be at the widest point of the resected tissue.
C- Each of the following sutures is then placed so as to bisect the space remaining.
D- Final appearance.
1- Medial Canthoplasty
In brachycephalic dogs a syndrome of eyelid, conjunctival, and corneal lesions is seen commonly which called brachycephalic ocular syndrome characterized by :
a- Lower medial Entropion.
b- Breed-related exophthalmos (shallow orbits)
c- Macropalpebral fissure (evident as excessive limbal or scleral exposure)
d- Lagophthalmos (and/or sleeping with the eyelids incompletely closed)
e- Medial caruncular trichiasis
f- Nasal fold trichiasis
g- Pigmentary keratitis
h- Epiphora due to “kinking” of the nasolacrimal canaliculi and obscuring of the puncta.
Aim of surgery
E- To provides a way to neatly correct many of the contributing features of this syndrome, by:
1- shortening the lower and upper eyelids.
2- removing the medial caruncle, and everting the lower medial Entropion.
F- thereby reducing corneal exposure, frictional irritation, and functional nasolacrimal apparatus obstruction.
G- It is recommended for dogs with progressive corneal lesions.
H- It is also suitable for patients with postproptosis exophthalmos that does not resolve and causes lagophthalmos and secondary corneal lesions.
The surgical technique
I- The animal placed in dorsal recumbency with the neck ventroflexed or may be placed in sternal recumbency with the head elevated.
J- Important features of the procedure are avoidance of the lacrimal puncta, meticulous removal of all hair follicles from the medial caruncle and conjunctiva, careful incision of the eyelids, perfect realignment of the eyelid margin, and appropriate postoperative management as for other eyelid procedures.
K- In very severe cases, medial and lateral canthoplasties may be required.
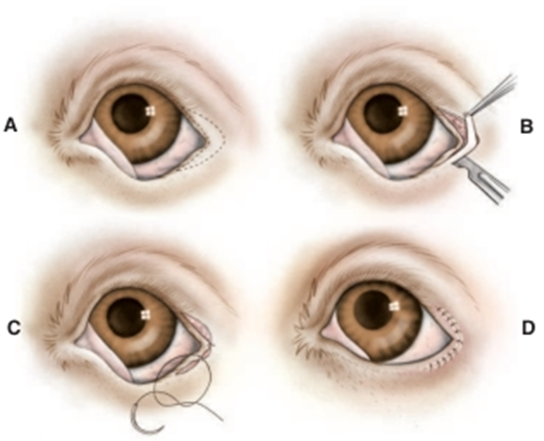
Fig.20: Lateral arrowhead procedure for entropion of the lateral
aspects of the upper and lower eyelids and the lateral canthus (Moore and Constantinescu,1997).
(This isusually performed after a lateral canthal tenotomy).
A- An arrowheadshaped section of tissue to be removed is outlined surrounding the lateral canthus.
- Its dimensions are dictated by the severity and extent of the entropion and may be asymmetric.
B- The tissue is resected with a scalpel blade and tenotomy scissors.
C- The incisions are closed using the rule of bisection, beginning with a suture placed at the lateracanthus.
D- All sutures must be placed perpendicular to the eyelid margin if maximal eversion is to be achieved.
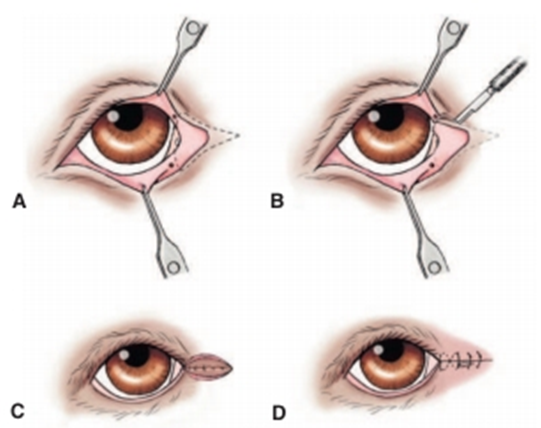
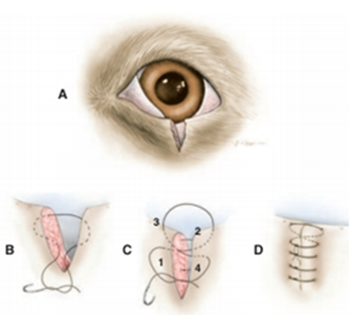
Fig.21: Medial canthoplasty(Moore and Constantinescu,1997).
A- The area to be resected is outlined and should include approximately the medial one fourth of the upper and lower eyelid margins, the medial caruncle, and a section medial to the medial canthus.
- Care is taken to not resect the nasolacrimal puncta.
B- The outlined tissue is resected using a No. 64 Beaver blade.
- The incisions should be perpendicular to the upper and lower eyelid margins where they cross them.
C- A buried mattress suture is used to appose the fresh edges of the canthus, continued as a series of mattress
sutures if required.
D- The skin is closed with a figure-of-eight suture at the new canthus with a series of simple interrupted sutures.
- V- Ectropion of the eyelid
Ectropion is an eversion or turning out of the eyelid margin.

Fig.22:
Bilateral ectropion in a young Labrador retriever (David et al, 2008).
Causes
Ectropion is classified according to the cause into:
1- Congenital ectropion
2- Acquired ectropion
a) Senile ectropion
b) Cicatrical ectropion
c) Intermittent ectropion
d) ectropion may result in severe secondary corneoconjunctival lesions if severe
enough and left untreated.
Treatment
A- Surgical correction when it causes conjunctivitis, keratitis, or exfoliative blepharitis due to epiphora or when it exacerbates keratoconjunctivitis sicca.
B- Correction is required much less frequently than for entropion.
Techniques used to correct different types of ectropion
1- Wedge Resection
A- The lower eyelid can be shortened by resection of a full-thickness wedge from the lateral end of the lower eyelid.
B- A standard two-layer closure is then used to perfectly appose the sides of the eyelid margin.
C- For ectropion due to either focal cicatricial contraction or a “notch” deformity in the lower eyelid, the wedge should be repositioned to remove the deformed or scarred tissue, the medial canthal area and nasolacrimal apparatus must be avoided.
2- “V-to-Y” Blepharoplasty
A- For cicatricial ectropion and in cases in which a small wedge resection is insufficient The V-to-Y (Wharton-Jones) blepharoplasty procedure is used.
B- It is particularly well suited to correction of ectropion due to a broad, contracted scar.
C- The V-to-Y blepharoplasty is begun with outlining of a triangular piece of skin with the base parallel and equal in length to the affected eyelid margin.
D- A skin incision is made along the two lower sides of the triangle, and the skin between them is undermined to elevate a V-shaped flap.
E- Scar tissue beneath the flap is excised.
F- The ventral ends of the incisions then are sutured together with simple interrupted sutures of 3/0 to 5/0 braided nylon or silk to form a vertical line perpendicular to the eyelid margin.
G- This vertical portion forces the triangle and eyelid margin superiorly.
H- The length of the vertical portion depends on how much elevation/inversion of the eyelid margin is required to return it to its normal position.
I- To allow for subsequent wound contraction, it should be about 2 to 3 mm longer than required.
J- The remaining parts of the two incisions are sutured to the free edges of the flap so that the sutured skin forms a Y.
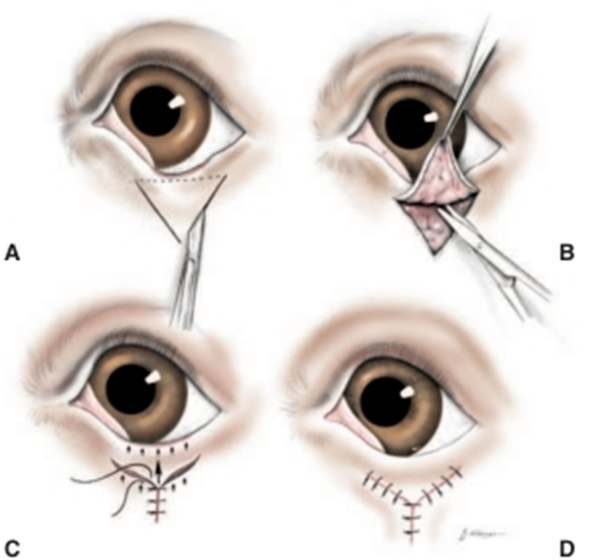
Fig.23:V-to-Y (Wharton-Jones) blepharoplasty (Moore and Constantinescu,1997).
A- A triangle of skin is outlined.
- The base is determined by the extent (width) of the lid margin affected by ectropion.
- The height of the triangle is determined by the extent of eversion to be corrected.
- A scalpel is used to incise the skin along the two sides but not the base of the triangle.
A- The skin flap created is elevated and undermined, along with any scar tissue.
B- The two sides of the triangle are sutured together to form the vertical portion of the Y.
- The length of the vertical portion of the wound is determined by the extent of eyelid eversion. Arrows show the tissue forces created.
C- The incisions are closed so as to form the two arms of the Y.
- VI- Blepharitis
Blepharitis is an inflammation of the eyelids.
Symptoms:
1- Pain is manifested by blepharospasm.
2- Hyperemia and swelling of the eyelid due to edema or inflammatory cell infiltration.
3- Alopecia, Scaliness, pruritis and epiphora.
4- Serous or purulent exudation.
5- Ulceration and fibrosis especially in chronic cases.

Fig.24: Chronic blepharitis in a cat.
Treatment
1- Careful cleaning of the lid margins and removal of purulent exudates with cotton soaked with worm normal saline or 2% sodium bicarbonate solution.
2- Topical application of antibiotic ointments to the outer and inner lid margin.
3- Topical fungicide is used in cases of fungal blepharitis.
4- A protective ointment is applied to the lid in parasitic blepharitis.
1- Corticosteroids and antihistamines are indicated in cases of allergic blepharitis.
- VII- Ptosis (blepharoptosis)
It means drooping of the upper eyelid. Classified according to the cause into:
1- Congenital ptosis
2- Acquired ptosis
a) False ptosis: It occurs as a result of trauma of the eyelid, abscess or tumor of the eyelid or fracture of the supra-orbital process.
b) True ptosis: It may be central as a result of cerebral or cerebellar tumor or peripheral due to paralysis of the nerve supply of the levators of the eyelid.
Treatment:
1-Resection of the levator muscles of the upper eyelid.
1- Removal of an elliptical piece of skin or trephination of a circular disc and suturing the wound horizontally.
- VIII- Traumatic eyelid injuries
The eyelids have an excellent blood supply, and injuries to them heal rapidly when repaired correctly.
The considerations to ensure an optimal outcome
1. The eyelids are susceptible to severe edema and distortion after even relatively minor injury
2. preferable to treat eyelid injuries as soon as possible.
3. When an eyelid injury complete examination for concurrent injuries to the cornea, sclera, and nasolacrimal apparatus in particular, and to the globe as a whole.
4. the nasolacrimal puncta should be identified and cannulated, and the nasolacrimal apparatus flushed to ensure patency.
5. Sutures in the eyelids must be kept away from the globe
6. The margin should always be accurately reapposed with a
standard two-layer closure .
7. Bacterial flora in the conjunctival sac and surrounding area
may readily invade this area a course of systemic antibiotics with good spectrum of activity against grampositive organisms (such as amoxicillin-clavulanic acid or a cephalosporin) is instituted.
8. Severe pruritus and self-trauma may occur during wound healing, an Elizabethan collar and postoperative use of warm packs and analgesics will minimize this problem and are essential.

Fig.25: Flap wound of the upper eyelid in a donkey.
Treatment
1- Copious irrigation and cleaning of the wound with boric acid solution 2% or warm normal saline.
1- Removal of any blood coagulum or foreign body.
2- Minimal debridement of the wound.
3- Suturing of the wound to restore the anatomic and functional
4- Surgical preparation and clipping should be gentle to prevent further edema.
5- A standard two-layer closure with soft, braided suture can then be used to close the eyelid laceration as for all other incisions involving the eyelid margin .
6- Systemic and topical antibiotics should be used perioperatively. Postoperatively, an ophthalmic ointment is preferred as it provides lubrication and protects the cornea during wound healing.
7- Topical corticosteroids are usually unnecessary and should be avoided if there is coincident corneal ulceration.
8- Systemically administered NSAIDs and application of warm packs may minimize pain and swelling, and an Elizabethan collar is essential to prevent self-trauma.
9- effort should be made to repair damage to the nasolacrimal apparatus as soon as possible after injury.
- IX- Eyelid tumors
Eyelid tumors are relatively common in all domestic species. the most common eyelid neoplasms vary by species, that the disease is virus induced. It has a “wart” like appearance or can also be ulcerative and granulomatous.
Dog: meibomian adenoma, papilloma, histiocytoma, melanoma .
• Cat: squamous cell carcinoma
• Horse: squamous cell carcinoma, equine sarcoid, melanoma
• Cattle: squamous cell carcinoma


Fig.26: Basal cell carcinoma at the lower eyelid in a cat. Fig.27: Fibropapilloma at the eyelid in a cow calf.
A- Squamous Cell Carcinoma
Squamous cell carcinoma may involve the eyelids of all species especially common in poorly pigmented areas of the eyelids in horses, cattle, and cats. The tumor is associated with exposure to ultraviolet light.
The pathogenesis of eyelid squamous cell carcinoma is may metastasize to regional lymph nodes and eventually to the lungs.
Clinical signs
Chronic purulent ocular discharge, which may be temporarily or partially responsive to antibiotics. Periocular excoriation, chronic conjunctivitis, and encrusted or hemorrhagic lesions of the eyelids are common.
Diagnosis
Is confirmed with cytologic assessment of scrapings or by biopsy.
B- Meibomian Adenoma
- The most common eyelid tumor in dogs, occurring most frequently after middle age.
- The tumors originate in the meibomian glands, and although many grow rapidly and sometimes appear histologically malignant, they are usually clinically benign.
- appear as proliferative masses appearing from the meibomian gland orifice .
- Enlargement of the gland itself is often visible, especially when viewed from the conjunctival surface, be associated with glandular enlargement due to retained secretions and associated lipogranuloma formation (chalazion), may cause frictional keratoconjunctivitis and should be removed as soon as the diagnosis is made.
- Simple removal of the section of the mass protruding from the eyelid margin is inadequate, because the tumor arises from the meibomian gland and will recur if not totally removed.
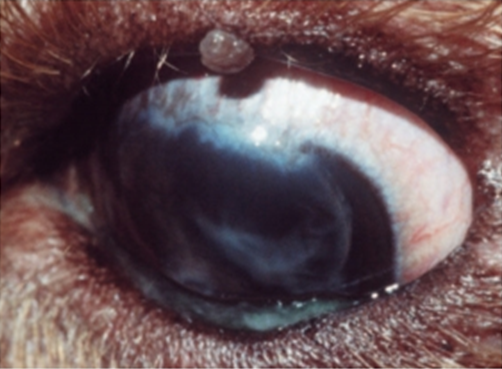
Fig.28: Upper eyelid meibomian adenoma in a dog(David et al, 2008).
A- Equine Sarcoid
- Equine sarcoid or fibrosarcoma is the second most common tumor of the equine eyelid,may be present elsewhere on the face and body.
- Sarcoids are nodular masses usually beneath intact skin and firmly adherent to the overlying dermis and subcutaneous tissues.
- Occasionally they can be ulcerated and must be distinguished from the eyelid lesions of habronemiasisin endemic areas.
- complete surgical excision of sarcoids is difficult and recurrence is likely. If surgical excision is used, a wide surrounding margin of normal tissue should be removed with reconstruction via a preplanned method.

Fig.29: Equine sarcoid at the medial canthus of the right eye(David et al, 2008).
A- Viral Papillomatosis
- Viral papillomas of the eyelids and conjunctiva occur in young dogs and cattle as part of oral or generalized papillomatosis.
- When continually moistened by tears, the tumors are grayish white and soft. The disease is often self limiting.

Fig.30: Lower eyelid papilloma in a dog (David et al, 2008).
A- Histiocytoma
Histiocytic masses involving the eyelids occur occasionally in dogs. may occur as single or multiple eyelid lesions
The tumors vary from benign lesions that regress spontaneously to tumors that are metastatic from or to the eyelids and therefore may involve regional lymph nodes or
other organ systems. Histiocytomas involving the eyelid typically appear as
tan to pink, somewhat alopecic masses that may grow relatively
quickly and may ulcerate quickly .
All eyelid tumors are regarded as malignant until proved otherwise by biopsy examination.
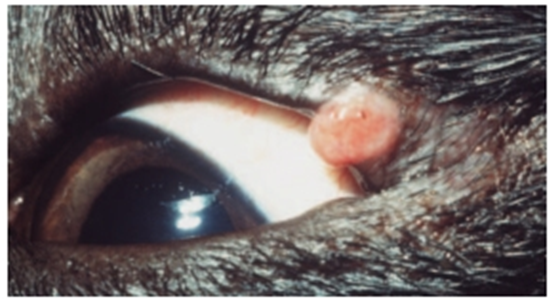
Fig.31: Solitary histiocytoma of the upper eyelid of a young dog (David et al, 2008).
Treatment
The best treatment is combination therapy of two or more of the following methods:
1- Surgical excision
- For smaller tumors involving one third or less of the eyelid margin, a simple, full-thickness wedge resection with two-layer closure.
- For more than one third of the eyelid length must be removed, total excision is usually not possible without some sort of blepharoplastic procedure, and referral may be indicated. One of the more straightforward blepharoplastic procedures is the H-plasty or full-thickness advancement flap.
2- Cryotherapy
Cryotherapy is particularly useful for eyelid lesions, as most eyelid tissues (including the nasolacrimal apparatus) are relatively resistant to the effects of cryotherapy and the lid retains function after cryonecrosis sufficient to produce tumor cell death. Cryotherapy is particularly useful for small or early tumors, especially in elderly or debilitated patients.
3- Radiation therapy
Chemotherapy- X- Eyelid abscesses
Eyelid abscesses are mostly subconjunctival and in some cases they are subcutaneous. The cause may be penetrating wound, embedded foreign body or hordeolum. Subconjunctival abscesses are present at the lateral canthus, upper eyelid and lower eyelid. The conjunctival abscess swelling extends over the eyeball and protrudes through the palpebral fissure preventing closure of the eyelids. Subcutaneous lid abscess leads to swelling of the eyelid preventing opening of the eyeball. Subconjunctival abscess at the lateral canthus in a cow

Fig.32: Subconjunctival abscess at the lateral canthus in a cow.
Treatment
Evacuation of pus is performed through a conjunctival incision. After squeezing and flushing of the abscess cavity, antibiotic eye ointment is applied. Subcutaneous lid abscess is drained through a skin incision.
- XI- Chalazion (Meibomian cyst-Tarsal cyst)
A chalazion is a nonneoplastic enlargement of the meibomian gland caused by blockage of its duct and inspissation of its secretory products.

Fig.33: Chalazion of one of the meibomian gland of the upper eyelid in a dog.
Symptoms
1. Localized painless swelling, yellow-white in color when viewed through the palpebral conjunctiva. The size of the swelling varies between pea-like swellings in dogs to hazel-nut in horses.
2. if the gland ruptures, lipid-laden sebaceous material escapes into the eyelid stroma and causes a lipogranuloma that may become quite inflamed.
3. Chalazion is few millimeters from the lid margin.
4. Chalazion bulges the skin over it but still the skin is freely movable.
5. The conjunctiva over the chalazion is reddened and elevated.
6. The contents are usually cheesy inspissated oily secretion.
Treatment
· Chalazion clamp is applied to the eyelid and then everted.
· Incision is made through the conjunctiva over the swelling.
· The contents are squeezed and the wall of the chalazion is thoroughly curetted.
· The clamp is removed and antibiotic ointment is applied for several days.
- XII- Hordeolum (stye) AND MEIBOMIAN ADENITIS
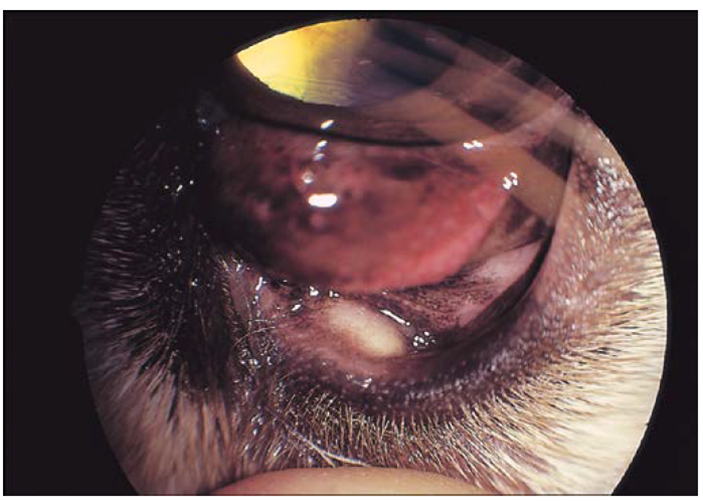
Fig.34:Internal hordeolum (stye) in a dog.
It is a small acute abscess of the meibomian glands.Hordeolum is an acute localized suppurative inflammation of the glands of Zies and glands of Moll belonging to the follicle of the eyelashes. Hordeolum affecting glands of Zies and Moll usually termed external hordeolum, while that affecting meibomian gland (meibomitis) is termed as internal hordeolum, Involvement of multiple glands is common The microorganism is usually Staphylococcus aureus. Termed meibomitis, meibomian or tarsal adenitis, or marginal blepharitis
Symptoms
1- Small solitary abscess or multiple abscesses at the lid margin. The infection will “point” and may erupt spontaneously.
2- variable erythema and swelling of the eyelid margins, pruritus, pain, chemosis, and purulent conjunctivitis
3- Blepharitis, blepharospasm and epiphora.
4- Internal hordeolum is characterized by presence of small painful abscess at the inner surface of the eyelid near the lid margin.
Treatment
1. Pulling of the offending eyelash (epilation) which present at the apex of the swelling.
2. Softening of the skin over the abscess by warm compresses contains sodium bicarbonate.
3. Incision of the abscess and evacuation of its content.
4. Rubbing of antibiotic ointment to the lid margin.
5. Systemic antibiotic therapy and topical antibiotic-corticosteroid administration are required. Without culture and sensitivity data or while waitingfor these results, administration of amoxicillin-clavulanic acid, doxycycline, or a cephalosporin
6. If there are recurrences, injection of staphylococcus toxoid is of value.
- XIII- Lagophthalmia
It means inability to close the eyelids. It may be a result of facial nerve paralysis
Symptoms
It predisposes to exposure corneal desiccation resulting in vascularization, granulation, pigmentation and sequestration.
Treatment
- The condition is treated medically as in cases of KCS.
- Temporary tarsorrhaphy.
- Medial
- References
- Belhorn RW, Barnett KC, Henkind P. Ocular colobomas in domestic cats. J Am Vet Med Assoc. 1971 Oct 15;159(8):1015-21.
- David J. Maggs, Paul E.Miller and Ron Ofri 2008 : SLATTER’S FUNDAMENTALS OF VETERINARY OPHTHALMOLOGY 11830 Westline Industrial Drive St. Louis, Missouri 63146.
- Donaldson D, et al. (2005): Surgical management of cicatricial ectropion following scarring dermatopathies in two dogs. Vet Ophthalmol 8:361.
- Gross TL, et al. (2005): Skin Diseases of the Dog and Cat: Clinical and Histopathologic Diagnosis, 2nd ed. Blackwell Science, Oxford, England.
- Lewin G (2003): Eyelid reconstruction in seven dogs using a split eyelid flap. J Small Anim Pract 44:346.
- Moore CP, Constantinescu GM [1997]: Surgery of the adnexa. Vet Clin North Am Small Anim Pract 27:1011.
- R W Belhorn, K C Barnett, P Henkind. 1971: Animals; Cat Diseases* / pathology . 1971 Oct 15; 159(8):1015-21.
- Redrawn from Severin GA [2000]: Severin’s Veterinary Ophthalmology Notes, 3rd ed. Severin, Ft. Collins, CO.
- Remington LA (2005): Clinical Anatomy of the Visual System, 2nd ed. Butterworth-Heinemann,
- Rowena M A Packer 1, Anke Hendricks 1, Charlotte C Burn 2 2015: Impact of facial conformation on canine health: corneal ulceration DOI: 10.1371/journal.pone.0123827.
- Rowena M. A. Packer1, Anke Hendricks1, Charlotte C. Burn2. Impact of Facial Conformation on CanineHealth: Corneal Ulceration May 201510(5):e0123827
- St. Louis.
- Westhues M, Fritsch R [1964]: Animal Anaesthesia, Vol 1: Local Anaesthesia. Oliver & Boyd, London.
- Withrow SJ, Vail DM (2007): Withrow & MacEwen’s Small Animal Clinical Oncology, 4th ed. Saunders, St. Louis.
- Wolfer JC (2002): Correction of eyelid coloboma in four cats using subdermal collagen and a modified Stades technique. Vet Ophthalmol 5:269.