the Management of Hiatus Hernia
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | the Management of Hiatus Hernia |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:53 AM |
Description
"last update: 8 December 2025" Download Guideline
- Executive summary
This guideline offers evidence-based recommendations on the targeted levels of Clinical practice guidelines and provide healthcare professionals with practical guidance on the diagnosis and treatment of diverticular disease and its complications.
· Hiatal hernia can be diagnosed by various modalities. Only investigations which will alter the clinical management of the patient should be performed, (Good practice statement).
· We recommend upper endoscopy with or without barium swallow for patients with a hiatal hernia, particularly prior to operative intervention, (Good practice statement).
· Esophageal manometry studies should not be used as a routine investigation for hiatal hernia, (Good practice statement).
· We advise performing computed tomography (CT) scan for patients with suspected complications, (eg. volvulized paraesophageal hernia), (Good practice statement).
· We advise against the use of pH testing for the diagnosis of hiatal hernia except in patients with sliding hiatal hernias that might benefit from antireflux surgery, (Good practice statement).
· We recommend against repair of a type I hernia in the absence of reflux disease, (Strong recommendation).
· We recommend repair of all symptomatic paraesophageal hiatal hernias, particularly those with acute obstructive symptoms or which have undergone volvulus, (Strong recommendation).
· We advise against routine elective repair of completely asymptomatic paraesophageal hernias, (Conditional recommendation).
· For acute gastric volvulus, we recommend reduction of the stomach with limited resection if vascular impairment is suspected, (Strong recommendation).
· Although open surgical repair could be done, we recommend laparoscopic hiatal hernia repair rather than open repair as it has a reduced rate of perioperative morbidity and is associated with shorter hospital stays than open transabdominal repair. It is the preferred approach for the majority of hiatal hernias, (Strong recommendation).
· We recommend dissecting the hernia sac away from mediastinal structures during paraesophageal hiatal hernia repair, (Strong recommendation).
· We advise excision of the hernia sac after its dissection from the mediastinal structures, (Conditional recommendation).
· We recommend the use of mesh for reinforcement of large hiatal hernia repairs to decrease the short term recurrence rates, (Strong recommendation).
· We advise performing fundoplication during repair of a sliding type hiatal hernia to manage reflux. Fundoplication is also advised during para-esophageal hernia repair, (Conditional recommendation).
· We recommend returning the gastroesophageal junction to an infra-diaphragmatic position, as a necessary step of hiatal hernia repair, (Strong recommendation).
· Hernia reduction with gastropexy alone and no hiatal repair may be suggested as a safe alternative in high-risk patients but may be associated with high recurrence rates, (Conditional recommendation).
· In high risk patients, if the circumstances allow, formal repair is preferred, (conditional recommendation).
· We advise repair of all detected hiatal hernias during bariatric operations, (Conditional recommendation).
· We recommend treatment of postoperative nausea and vomiting aggressively to minimize poor outcomes, (Strong recommendation).
· With early postoperative dysphagia, we recommend adequate caloric and nutritional intake, (Strong recommendation).
· We recommend against routine postoperative contrast studies in asymptomatic patients, (Strong recommendation).
· We recommend revisional surgery in presence of experienced surgeons, (Strong recommendation).
· Revisional antireflux surgery is not indicated except in symptomatic cases and in the presence of anatomical cause that could explain patient’s complaint, (Good practice statement).
· Roux-en-Y gastric bypass is a valid option as a revisional antireflux surgery even in non-obese patients, (Good practice statement).
- Recommendations
Section 1:Diagnosis:
· Hiatal hernia can be diagnosed by various modalities. Only investigations which will alter the clinical management of the patient should be performed, (Good practice statement).
· We recommend upper endoscopy with or without barium swallow for patients with a hiatal hernia, particularly prior to operative intervention, (Good practice statement).
· Esophageal manometry studies should not be used as a routine investigation for hiatal hernia, (Good practice statement).
· We advise performing computed tomography (CT) scan for patients with suspected complications, (eg. volvulized paraesophageal hernia), (Good practice statement).
· We advise against the use of pH testing for the diagnosis of hiatal hernia except in patients with sliding hiatal hernias that might benefit from antireflux surgery, (Good practice statement).
Section 2: Indications for surgery:
· We recommend against repair of a type I hernia in the absence of reflux disease, (Strong recommendation, moderate certainty evidence, (1)).
· We recommend repair of all symptomatic paraesophageal hiatal hernias, particularly those with acute obstructive symptoms or which have undergone volvulus, (Strong recommendation, high certainty evidence, (1)).
· We advise against routine elective repair of completely asymptomatic paraesophageal hernias, (Conditional recommendation, moderate certainty evidence, (1)).
· For acute gastric volvulus, we recommend reduction of the stomach with limited resection if vascular impairment is suspected, (Strong recommendation, high certainty evidence, (1)).
Section 3: Technical Considerations:
· Although open surgical repair could be done, we recommend laparoscopic hiatal hernia repair rather than open repair as it has a reduced rate of perioperative morbidity and is associated with shorter hospital stays than open transabdominal repair. It is the preferred approach for the majority of hiatal hernias, (Strong recommendation, high certainty evidence, (1)).
· We recommend dissecting the hernia sac away from mediastinal structures during paraesophageal hiatal hernia repair, (Strong recommendation, low certainty evidence, (1)).
· We advise excision of the hernia sac after its dissection from the mediastinal structures, (Conditional recommendation, low certainty evidence, (1)).
· We recommend the use of mesh for reinforcement of large hiatal hernia repairs to decrease the short term recurrence rates, (Strong recommendation, moderate certainty evidence, (1)).
· We advise performing fundoplication during repair of a sliding type hiatal hernia to manage reflux. Fundoplication is also advised during para-esophageal hernia repair, (Conditional recommendation, low certainty evidence, (1)).
· We recommend returning the gastroesophageal junction to an infra-diaphragmatic position, as a necessary step of hiatal hernia repair, (Strong recommendation, moderate certainty evidence, (1)).
· Hernia reduction with gastropexy alone and no hiatal repair may be suggested as a safe alternative in high-risk patients but may be associated with high recurrence rates, (Conditional recommendation, low certainty evidence, (1)).
· In high risk patients, if the circumstances allow, formal repair is preferred, (conditional recommendation, high certainty evidence, (1)).
Section 4: Repair of hiatal hernia during bariatric operations:
· We advise repair of all detected hiatal hernias during bariatric operations, (Conditional recommendation, moderate certainty evidence, (1)).
Section 5: Postoperative Management:
· We recommend treatment of postoperative nausea and vomiting aggressively to minimize poor outcomes, (Strong recommendation, low certainty evidence, (1)).
· With early postoperative dysphagia, we recommend adequate caloric and nutritional intake, (Strong recommendation, very low certainty evidence, (1)).
· We recommend against routine postoperative contrast studies in asymptomatic patients, (Strong recommendation, moderate certainty evidence, (1)).
Section 6: Revisional Surgery:
· We recommend revisional surgery in presence of experienced surgeons, (Strong recommendation, moderate certainty evidence, (1)).
· Revisional antireflux surgery is not indicated except in symptomatic cases and in the presence of anatomical cause that could explain patient’s complaint, (Good practice statement).
· Roux-en-Y gastric bypass is a valid option as a revisional antireflux surgery even in non-obese patients, (Good practice statement).
- Acknowledgement
We would like to acknowledge the Guideline Development Group, (GDG) committee for
developing this guideline.
Chair of GDG: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University.
Moderator of GDG: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University.
Members of GDG (Alphabetically):
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University.
Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University.
Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University.
Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University.
Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University.
Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
BE |
Barrett’s Esophagus |
|
CECT |
Contrast Enhanced Computerized Tomography. |
|
CRP |
C Reactive Protein |
|
CT GDG |
Computerized Tomography. Guideline Development Group. |
|
GEJ |
Gastro-Esophageal Junction. |
|
GERD |
Gastroesophageal Reflux Disease. |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation |
|
HH |
Hiatus Hernia |
|
MRI |
Magnetic Resonance Imaging |
|
PHH |
Paraesophageal Hiatus Hernia |
|
RYGB |
Roux-en-Y Gastric Bypass |
|
WHO |
World Health Organization. |
- Glossary
Types of hiatus hernia:
The current anatomic classification has evolved to include a categorization of hiatal hernias into Types I – IV, (1).
1. Type I hernias are sliding hiatal hernias, where the gastroesophageal junction, (GEJ) migrates above the diaphragm, (2). The stomach remains in its usual longitudinal alignment, (3), and the fundus remains below the gastroesophageal junction.
2. Type II hernias are pure paraesophageal hernias (PEH); the gastroesophageal junction remains in its normal anatomic position but a portion of the fundus herniates through the diaphragmatic hiatus adjacent to the esophagus, (2).
3. Type III hernias are a combination of Types I and II, with both the gastroesophageal junction and the fundus herniating through the hiatus. The fundus lies above the gastroesophageal junction, (2).
4. Type IV hiatal hernias are characterized by the presence of a structure other than stomach, such as the omentum, colon or small bowel within the hernia sac, (2).
- Introduction
Hiatal hernia is a common disorder, (4 & 5). It is characterized by a protrusion of any abdominal structure other than the esophagus into the thoracic cavity through a widening of the hiatus of the diaphragm.
Attempts began early in the last century to classify hiatal hernia into four subtypes, (1).
Greater than 95% of hiatal hernias are Type I. Types II – IV hernias as a group are referred to as paraesophageal hernias (PEH), and are differentiated from Type I hernias by relative preservation of posterolateral phrenoesophageal attachments around the gastroesophageal junction, (6). Of the paraesophageal hernias, more than 90% are Type III, and the least common is Type II, (3). The term “giant” paraesophageal hernia appears frequently in the literature, though its definition is inconsistent. Various authors have suggested giant paraesophageal hernias be defined as all type III and IV hernias , but most limit this term to those paraesophageal hernias having greater than one third to one half of the stomach in the chest, (7- 9). These guidelines are specific for each type of hiatal hernia since the implications of a hiatal hernia and the indications for repair differ between the sliding (Type I) hernias and for the paraesophageal hernias (Type II, III and IV). Cephalad migration of the gastroesophageal junction may result from weakening of the phrenoesophageal ligament. Depletion of elastin fibers leads to stretching of the ligament and proximal displacement of the gastroesophageal junction, (10).
Most cases of hiatal hernia are acquired rather than congenital. Other diaphragmatic hernias exist but are not included in this review. These include acquired hernias such as traumatic diaphragmatic hernias; the rare parahiatal hernias in which the hernia defect arises lateral to the crural musculature and not through the esophageal hiatus itself; iatrogenic diaphragmatic hernias such as those that misguided chest tubes or after thoracoabdominal incisions in which the diaphragm is taken down, (3); and congenital diaphragmatic defects such as posterolateral Bochdalek hernias and retrosternal Morgagni hernias.
Management is complex and based on multiple factors including size and type of hiatal hernia, degree of symptoms, and associated failure of symptom control by non-surgical means. Deciding whether to proceed with surgical repair of an asymptomatic hiatal hernia can be difficult, (1). These guidelines aim to provide recommendations on the aforementioned dilemmas.
- Scope and Purpose
The scope of these guidelines is to diagnose hiatus hernia and its complications and to manage these problems accurately and without any hesitation.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target Audience
The principle targeted audiences are the practicing surgeons, however, gastroenterologists, ICU specialists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation. Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines
· Specific range of dates for publication (using Guidelines published or updated in 2013 and later)
· Selecting peer reviewed publications only
· Selecting guidelines written in English language
· Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt the Guidelines for the management of hiatal hernia, (2013).
- Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org
· GRADE online training modules: http://cebgrade.mcmaster.ca/
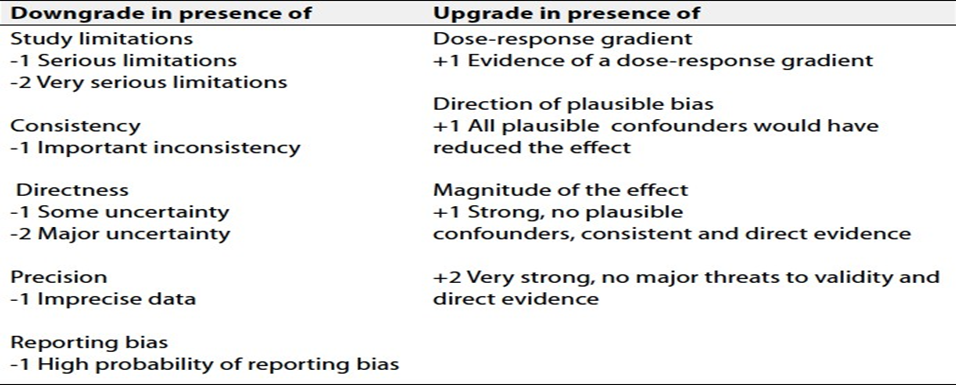
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (tables 1& 2).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research needs
1. Evaluating the role of autologous tissue reinforcement (eg. Falciform ligament) for management of wide hiatal opening.
2. Long term studies on a larger population to assess the outcome of RYGB as a revisional antireflux surgery.
3. Defining the best therapeutic option in the management of short esophagus.
- Clinical indicators of monitoring
1. Documentation of the clinical symptoms and signs.
2. Documentation of the type of hiatus hernia.
3. Upper endoscopy.
4. Imaging studies
5. Documentation of the type of treatment.
- Updating of the guidelines
The GDG committee for guidelines development is responsible for the continuous evaluation of evidence available about hiatus hernia. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1. Quality and Significance of the four levels of evidence in GRADE:
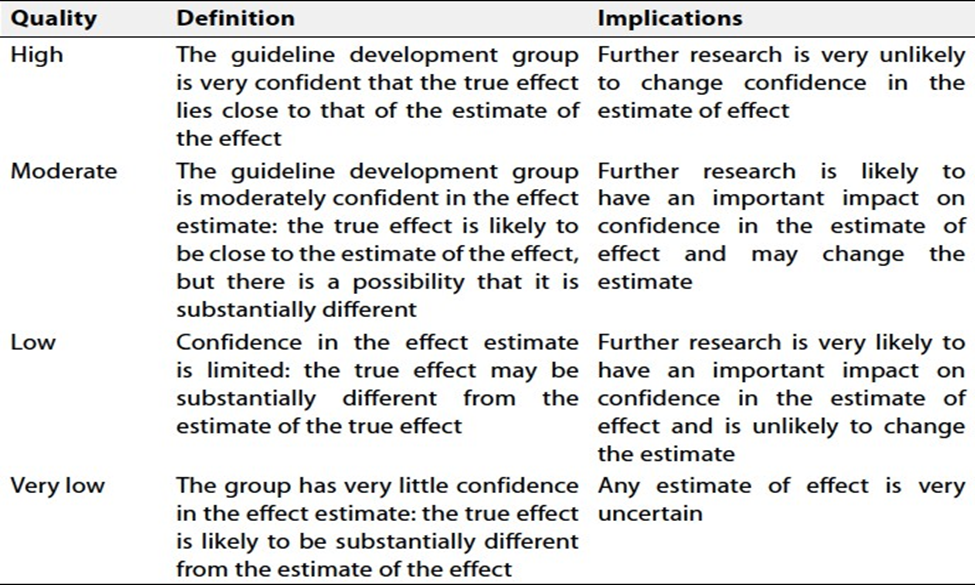
Table 2. Factors that determine How to upgrade or downgrade the quality of evidence.
- References
1. Kohn GP, Price RR, DeMeester SR, Zehetner J, Muensterer OJ, Awad Z, Mittal SK, Richardson WS, Stefanidis D, Fanelli RD (2013). Guidelines for the management of hiatal hernia . Surg Endosc 27:4409-4428.
2. Kavic SM, Segan RD, George IM, Turner PL, Roth JS, Park A (2006). Classification of hiatal hernias using dynamic three-dimensional reconstruction. Surgical innovation 13:49-52.
3. Hutter MM, Rattner DW (2007). Paraesophageal and other complex diaphragmatic hernias. In: Yeo CJ (ed) Shackelford's Surgery of the Alimentary Tract Saunders Elsevier, Philadelphia, pp 549-562.
4. Altorki NK, Yankelevitz D, Skinner DB (1998). Massive hiatal hernias: the anatomic basis of repair. J Thorac Cardiovasc Surg 115:828-835.
5. Andujar JJ, Papasavas PK, Birdas T, Robke J, Raftopoulos Y, Gagne DJ, Caushaj PF, Landreneau RJ, Keenan RJ (2004). Laparoscopic repair of large paraesophageal hernia is associated with a low incidence of recurrence and reoperation. Surg Endosc 18:444-447.
6. Landreneau RJ, Del Pino M, Santos R (2005). Management of paraesophageal hernias. The Surgical clinics of North America 85:411-432.
7. Awais O, Luketich JD (2009). Management of giant paraesophageal hernia. Minerva Chir 64:159-168.
8. 8.Litle VR, Buenaventura PO, Luketich JD (2001). Laparoscopic repair of giant paraesophageal hernia. Adv Surg 35:21-38.
9. Mitiek MO, Andrade RS (2010) Giant hiatal hernia. Ann Thorac Surg 89:S2168-2173.
10. Curci JA, Melman LM, Thompson RW, Soper NJ, Matthews BD (2008) Elastic fiber depletion in the supporting ligaments of the gastroesophageal junction: a structural basis for the development of hiatal hernia. J Am Coll Surg 207:191-196.