the Management of Skin and Soft Tissue Infections
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | the Management of Skin and Soft Tissue Infections |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:02 AM |
Description
"last update: 8 December 2025" Download Guideline
- Executive summary
Summarized below are the recommendations made in the new guidelines for skin and soft tissue infections (SSTIs), to simplify the management of localized purulent staphylococcal infections such as skin abscesses, furuncles, and carbuncles in the age of methicillin-resistant Staphylococcus aureus (MRSA). In addition, it simplify the approach to patients with surgical site infections. The panel followed a process used in the development of other Infectious Diseases Society of America (IDSA) guidelines, which included a systematic weighting of the strength of recommendation and quality of evidence using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) system.
· Gram stain and culture of pus from carbuncles and abscesses are recommended in atypical cases, but treatment without these studies is reasonable in typical cases, (Strong recommendation).
· We recommend against Gram stain and culture of pus from inflamed epidermoid cysts, (Strong recommendation).
· Incision and drainage is the recommended treatment for inflamed epidermoid cysts, carbuncles, abscesses, and large furuncles, (Strong recommendation).
· The decision to administer antibiotics directed against S. aureus as an adjunct to incision and drainage should be made based upon presence or absence of: systemic inflammatory response syndrome (SIRS), (Strong recommendation).
· An antibiotic active against MRSA is recommended for patients with carbuncles or abscesses who have failed initial antibiotic treatment or have markedly impaired host defenses or in patients with SIRS, (Strong recommendation).
· In case of a recurrent abscess at a site of previous infection, we recommend a search for local causes such as a pilonidal cyst, hidradenitis suppurativa, or foreign material, (Strong recommendation).
· Recurrent abscesses should be drained and cultured early in the course of infection, (Strong recommendation).
· After obtaining cultures of recurrent abscess, we advise to treat it with a 5- to 10-day course of an antibiotic active against the pathogen isolated, (Conditional recommendation).
· For recurrent S. aureus infection, we advise a 5-day decolonization regimen twice daily of intranasal mupirocin, daily chlorhexidine washes, and daily decontamination of personal items such as towels, sheets, and clothes, (Conditional recommendation).
· Adult patients should be evaluated for neutrophil disorders if recurrent abscesses began in early childhood, (Strong recommendation).
· We recommend against routine cultures of blood or cutaneous aspirates, biopsies, or swabs, (Strong recommendation).
· In patients with malignancy on chemotherapy, neutropenia, severe cell-mediated immunodeficiency, immersion injuries, and animal bites, we advise performing cultures and microscopic examination of cutaneous aspirates, biopsies, or swabs, (Conditional recommendation).
· Typical cases of cellulitis without systemic signs of infection should receive an antimicrobial agent that is active against streptococci, (Strong recommendation).
· For cellulitis with systemic signs of infection (moderate non-purulent), we advise prescribing systemic antibiotics. Coverage against methicillin-susceptible S. aureus (MSSA) may be included, (Conditional recommendation).
· For patients whose cellulitis is associated with penetrating trauma, evidence of MRSA infection elsewhere, nasal colonization with MRSA, injection drug use, or SIRS (severe non-purulent), vancomycin or another antimicrobial effective against both MRSA and streptococci is recommended, (Strong recommendation).
· In severely compromised patients as defined in severe non-purulent, we advise prescribing broad-spectrum antimicrobial coverage, (Conditional recommendation).
· Vancomycin plus either piperacillin-tazobactam or imipenem/meropenem is recommended as a reasonable empiric regimen for severe infections, (Strong recommendation).
· The recommended duration of antimicrobial therapy is 5 days, but treatment should be extended if the infection has not improved within this time period, (Strong recommendation).
· Elevation of the affected area and treatment of predisposing factors, such as edema or underlying cutaneous disorders, are recommended, (Strong recommendation).
· In lower-extremity cellulitis, we recommend careful examination of the interdigital toe spaces because treating fissuring, scaling, or maceration may eradicate colonization with pathogens and reduce the incidence of recurrent infection, (Strong recommendation).
· Outpatient therapy is recommended for patients who do not have SIRS, altered mental status, or hemodynamic instability, (mild non-purulent), (Strong recommendation).
· Hospitalization is recommended if there is concern for a deeper or necrotizing infection, for patients with poor adherence to therapy, for infection in a severely immunocompromised patient, or if outpatient treatment is failing, (moderate or severe non-purulent), (Strong recommendation).
· Identifying and treating predisposing conditions for recurrent cellulitis is recommended, (Strong recommendation).
· We advise administration of prophylactic antibiotics in patients who have 3–4 episodes of cellulitis per year despite attempts to treat or control predisposing factors, (Conditional recommendation).
· We recommend suture removal plus incision and drainage for surgical site infections, (Strong recommendation).
· We advise against routine adjunctive systemic antimicrobial therapy in SSI, except in the presence of manifestations of SIRS, (Conditional recommendation).
· A brief course of systemic antimicrobial therapy is recommended in patients with surgical site infections following clean operations on the trunk, head and neck, or extremities that also have systemic signs of infection, (Strong recommendation).
· Prophylactic antibiotic is recommended before the operation according to the type of operation, (Strong recommendation).
· Prompt surgical intervention is recommended for patients with aggressive infections associated with signs of systemic toxicity or suspicion of necrotizing fasciitis or gas gangrene (severe non-purulent), (Strong recommendation).
· Empiric antibiotic treatment should be broad, (Strong recommendation).
· Penicillin plus clindamycin is recommended for treatment of documented group A streptococcal necrotizing fasciitis, (Strong recommendation).
· We recommend performing imaging studies for diagnosis of pyomyositis, (Strong recommendation).
· We recommend cultures of blood and abscess, followed by administration of initial empirical therapy in patients with pyomyositis, (Strong recommendation).
· We recommend early drainage of purulent material in pyomyositis, (Strong recommendation).
· We recommend repeating imaging studies in the patient with persistent bacteremia to identify undrained foci of infection, (Strong recommendation).
· Antibiotics should be administered intravenously initially, but once the patient is clinically improved, oral antibiotics are appropriate, (Strong recommendation).
· We recommend urgent surgical exploration of the suspected gas gangrene site and surgical debridement of involved tissue, (severe non-purulent), (Strong recommendation).
· In the absence of a definitive etiologic diagnosis, we recommend administration of broad-spectrum antibiotic, (Strong recommendation).
· We recommend against hyperbaric oxygen (HBO) therapy, because it has not been proven as a benefit to the patient and may delay resuscitation and surgical debridement, (Strong recommendation).
- Recommendations
Section 1: Evaluation and treatment for purulent SSTIs (cutaneous abscesses, furuncles, carbuncles, and inflamed epidermoid cysts):
· Gram stain and culture of pus from carbuncles and abscesses are recommended in atypical cases, but treatment without these studies is reasonable in typical cases, (Strong recommendation, moderate certainty evidence, (3)).
· We recommend against Gram stain and culture of pus from inflamed epidermoid cysts, (Strong recommendation, moderate certainty evidence, (3)).
· Incision and drainage is the recommended treatment for inflamed epidermoid cysts, carbuncles, abscesses, and large furuncles, (Strong recommendation, high certainty evidence, (3)).
· The decision to administer antibiotics directed against S. aureus as an adjunct to incision and drainage should be made based upon presence or absence of: systemic inflammatory response syndrome (SIRS), (Strong recommendation, low certainty evidence, (3)).
· An antibiotic active against MRSA is recommended for patients with carbuncles or abscesses who have failed initial antibiotic treatment or have markedly impaired host defenses or in patients with SIRS, (Strong recommendation, low certainty evidence, (3)).
Section 2: Treatment of recurrent skin abscess:
· In case of a recurrent abscess at a site of previous infection, we recommend a search for local causes such as a pilonidal cyst, hidradenitis suppurativa, or foreign material, (Strong recommendation, moderate certainty evidence, (3)).
· Recurrent abscesses should be drained and cultured early in the course of infection, (Strong recommendation, moderate certainty evidence, (3)).
· After obtaining cultures of recurrent abscess, we advise to treat it with a 5- to 10-day course of an antibiotic active against the pathogen isolated, (Conditional recommendation, low certainty evidence, (3)).
· For recurrent S. aureus infection, we advise a 5-day decolonization regimen twice daily of intranasal mupirocin, daily chlorhexidine washes, and daily decontamination of personal items such as towels, sheets, and clothes, (Conditional recommendation, low certainty evidence, (3)).
· Adult patients should be evaluated for neutrophil disorders if recurrent abscesses began in early childhood, (Strong recommendation, moderate certainty evidence, (3)).
Section 3: Evaluation and treatment of erysipelas and cellulitis:
· We recommend against routine cultures of blood or cutaneous aspirates, biopsies, or swabs, (Strong recommendation, moderate certainty evidence, (3)).
· In patients with malignancy on chemotherapy, neutropenia, severe cell-mediated immunodeficiency, immersion injuries, and animal bites, we advise performing cultures and microscopic examination of cutaneous aspirates, biopsies, or swabs, (Conditional recommendation, moderate certainty evidence, (3)).
· Typical cases of cellulitis without systemic signs of infection should receive an antimicrobial agent that is active against streptococci, (Strong recommendation, moderate certainty evidence, (3)).
· For cellulitis with systemic signs of infection (moderate non-purulent), we advise prescribing systemic antibiotics. Coverage against methicillin-susceptible S. aureus (MSSA) may be included, (Conditional recommendation, low certainty evidence, (3)).
· For patients whose cellulitis is associated with penetrating trauma, evidence of MRSA infection elsewhere, nasal colonization with MRSA, injection drug use, or SIRS (severe non-purulent), vancomycin or another antimicrobial effective against both MRSA and streptococci is recommended, (Strong recommendation, moderate certainty evidence, (3)).
· In severely compromised patients as defined in severe non-purulent, we advise prescribing broad-spectrum antimicrobial coverage, (Conditional recommendation, moderate certainty evidence, (3)).
· Vancomycin plus either piperacillin-tazobactam or imipenem/meropenem is recommended as a reasonable empiric regimen for severe infections, (Strong recommendation, moderate certainty evidence, (3)).
· The recommended duration of antimicrobial therapy is 5 days, but treatment should be extended if the infection has not improved within this time period, (Strong recommendation, high certainty evidence, (3)).
· Elevation of the affected area and treatment of predisposing factors, such as edema or underlying cutaneous disorders, are recommended, (Strong recommendation, moderate certainty evidence, (3)).
· In lower-extremity cellulitis, we recommend careful examination of the interdigital toe spaces because treating fissuring, scaling, or maceration may eradicate colonization with pathogens and reduce the incidence of recurrent infection, (Strong recommendation, moderate certainty evidence, (3)).
· Outpatient therapy is recommended for patients who do not have SIRS, altered mental status, or hemodynamic instability, (mild non-purulent), (Strong recommendation, moderate certainty evidence, (3)).
· Hospitalization is recommended if there is concern for a deeper or necrotizing infection, for patients with poor adherence to therapy, for infection in a severely immunocompromised patient, or if outpatient treatment is failing, (moderate or severe non-purulent), (Strong recommendation, moderate certainty evidence, (3)).
Section 4: Evaluation and management of patients with recurrent cellulitis:
· Identifying and treating predisposing conditions for recurrent cellulitis is recommended, (Strong recommendation, moderate certainty evidence, (3)).
· We advise administration of prophylactic antibiotics in patients who have 3–4 episodes of cellulitis per year despite attempts to treat or control predisposing factors, (Conditional recommendation, moderate certainty evidence, (3)).
Section 5: Management of surgical site infections:
· We recommend suture removal plus incision and drainage for surgical site infections, (Strong recommendation, low certainty evidence, (3)).
· We advise against routine adjunctive systemic antimicrobial therapy in SSI, except in the presence of manifestations of SIRS, (Conditional recommendation, low certainty evidence, (3)).
· A brief course of systemic antimicrobial therapy is recommended in patients with surgical site infections following clean operations on the trunk, head and neck, or extremities that also have systemic signs of infection, (Strong recommendation, low certainty evidence, (3)).
· Prophylactic antibiotic is recommended before the operation according to the type of operation, (Strong recommendation, low certainty evidence, (3)).
Section 6: Evaluation and treatment of necrotizing fasciitis, including Fournier gangrene:
· Prompt surgical intervention is recommended for patients with aggressive infections associated with signs of systemic toxicity or suspicion of necrotizing fasciitis or gas gangrene (severe non-purulent), (Strong recommendation, low certainty evidence, (3)).
· Empiric antibiotic treatment should be broad, (Strong recommendation, low certainty evidence, (3)).
· Penicillin plus clindamycin is recommended for treatment of documented group A streptococcal necrotizing fasciitis, (Strong recommendation, low certainty evidence, (3)).
Section 7: Management of pyomyositis:
· We recommend performing imaging studies for diagnosis of pyomyositis, (Strong recommendation, moderate certainty evidence, (3)).
· We recommend cultures of blood and abscess, followed by administration of initial empirical therapy in patients with pyomyositis, (Strong recommendation, moderate certainty evidence, (3)).
· We recommend early drainage of purulent material in pyomyositis, (Strong recommendation, high certainty evidence, (3)).
· We recommend repeating imaging studies in the patient with persistent bacteremia to identify undrained foci of infection, (Strong recommendation, low certainty evidence, (3)).
· Antibiotics should be administered intravenously initially, but once the patient is clinically improved, oral antibiotics are appropriate, (Strong recommendation, low certainty evidence, (3)).
Section 8: Evaluation and treatment of clostridial gas gangrene or myonecrosis:
· We recommend urgent surgical exploration of the suspected gas gangrene site and surgical debridement of involved tissue, (severe non-purulent), (Strong recommendation, moderate certainty evidence, (3)).
· In the absence of a definitive etiologic diagnosis, we recommend administration of broad-spectrum antibiotic, (Strong recommendation, low certainty evidence, (3)).
· We recommend against hyperbaric oxygen (HBO) therapy, because it has not been proven as a benefit to the patient and may delay resuscitation and surgical debridement, (Strong recommendation, low certainty evidence, (3)).
- Acknowledgement
We would like to acknowledge the Guideline Development Group, (GDG) committee for developing this guideline.
Chair of GDG: Mostafa Abdel Hamed Soliman; professor of surgery, Cairo university.
Moderator of GDG: Mohamed Ali Mohamed Nada, professor of surgery, Ain Shams University.
Members of GDG (Alphabetically):
Abel Motey Hussein Aly; professor of surgery, Cairo university.
Abdelwahab Mohamed Ezzat; professor of surgery, Ain Shams university.
Ahmed Abdel Raouf Elgeidie; professor of digestive surgery, Mansoura university.
Alaa Abdallah; professor of surgery, Ain Shams university.
Atef Abdelghani Salem; professor of surgery, Benha university.
Hesham Abdel Raouf Elakad; professor of surgery, Ain Shams university.
Khaled Abdallah Elfiky; professor of surgery, Ain Shams university.
Khaled Amer; professor of surgery, Military medical academy.
Khaled Safwat; professor of surgical oncology and endoscopy, Zagazig university.
Ibrahim Elzayat; head of surgery department, Aswan university.
Mohamed Ibrahim Abdel Hamed Alsaid, professor of surgery, Zagazig University.
Tarek Ibrahim; professor of surgery, National liver institute Menofia university.
- Abbreviations
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
C & S |
Culture and Sensitivity. |
|
GDG |
Guideline Development Group. |
|
GRADE |
Grading of Recommendations Assessment, Development, and Evaluation. |
|
HBO |
Hyperbaric Oxygen. |
|
I&D |
Incision and Drainage |
|
IDSA |
Infectious Diseases Society of America. |
|
MSSA |
Methicillin-Susceptible Staphylococcus Aureus. |
|
MRI |
Magnetic Resonance Imaging. |
|
MRSA |
Methicillin-Resistant Staphylococcus Aureus. |
|
SIRS SSI |
Systemic Inflammatory Response Syndrome. Surgical Site Infection. |
|
SSTIs |
Skin And Soft Tissue Infections. |
|
US |
Ultrasonography. |
|
WBC |
White Blood Cell Count. |
|
WHO |
World Health Organization |
- Introduction
This practice guideline provides recommendations for the diagnosis and management of skin and soft tissue infections (SSTIs) in all age groups. These recommendations take on new importance because of a dramatic increase in the frequency and severity of infections and the emergence of resistance to many of the antimicrobial agents commonly used to treat SSTIs in the past, (1).
These infections have diverse etiologies that depend, in part, on different epidemiological settings. As a result, obtaining a careful history that includes information about the patient's immune status, geographic locale, travel history, recent trauma or surgery, previous antimicrobial therapy, lifestyle, hobbies, is essential when developing an adequate differential diagnosis and an appropriate index of suspicion for specific etiological agents. In some cases, this information is insufficient and biopsy or aspiration of tissue may be necessary. In addition, radiographic procedures may be critical in a small subset of patients to determine the level of infection and the presence of gas, abscess, or a necrotizing process. Last, surgical exploration or debridement is an important diagnostic, as well as therapeutic, procedure in patients with necrotizing infections or myonecrosis and may be important for selected immunocompromised hosts, (2).
- Glossary
Purulent skin and soft tissue infections (SSTIs):
Mild infection: for purulent SSTI, in whom incision and drainage, (I&D) is indicated.
· Moderate infection: patients with purulent infection with systemic signs of infection.
· Severe infection: patients who have failed incision and drainage plus oral antibiotics or those with systemic signs of infection such as temperature >38°C, tachycardia (heart rate >90 beats per minute), tachypnea (respiratory rate >24 breaths per minute) or abnormal white blood cell count (<12 000 or <400 cells/µL), or immunocompromised patients..
B) Non-purulent SSTIs:
· Mild infection: typical cellulitis/erysipelas with no focus of purulence.
· Moderate infection: typical cellulitis/erysipelas with systemic signs of infection.
· Severe infection: patients who have failed oral antibiotic treatment or those with systemic signs of infection (as defined above under purulent infection), or those who are immunocompromised, or those with clinical signs of deeper infection such as bullae, skin sloughing, hypotension, or evidence of organ dysfunction.
- Scope and purpose
The scope of this guideline is who to prevent, diagnose and treat soft tissue infection and how to manage their complications.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target audience
The principle targeted audiences are the practicing surgeons, however, ICU specialists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines
· Specific range of dates for publication (using Guidelines published or updated in 2014 and later)
· Selecting peer reviewed publications only
· Selecting guidelines written in English language
· Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014.
- Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: https://www.gradeworkinggroup.org
· GRADE online training modules: http://cebgrade.mcmaster.ca/
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1& 2).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research needs
1. Clinical trials should be performed that include patients with severe soft tissue infections (eg, necrotizing fasciitis and gas gangrene) and immunocompromised patients.
2. Investigations should determine host and pathogen factors that result in recurrent cellulitis.
3. Larger clinical trials should determine if anti-inflammatory agents are useful or detrimental in the treatment of cellulitis and erysipelas.
- Clinical indicators for monitoring
1. Documentation of the vital signs and manifestation of SIRS.
2. Documentation of the type and site of infection.
3. Laboratory investigations, (CBC, CRP, C &S etc.).
4. Imaging, (US, MRI).
- Updating of the guideline
The GDG committee for guidelines development is responsible for the continuous evaluation of evidence available about skin and soft tissue infection.
The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Quality and Significance of the four levels of evidence in GRADE:
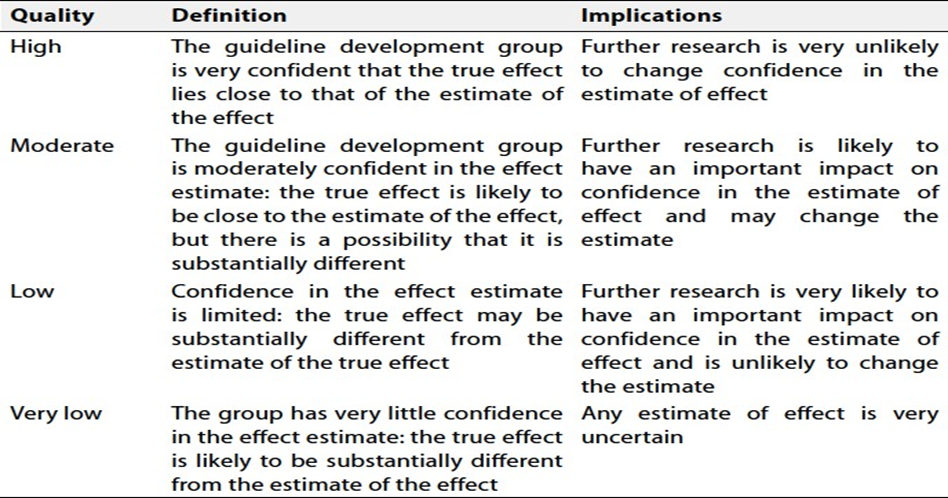
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
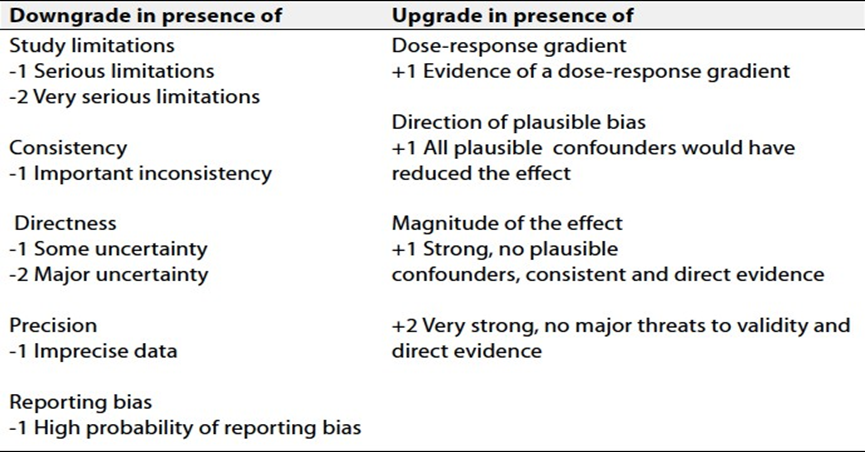
Table (3): Surgery of intestinal or genitourinary tract.
|
Silngle-drug regimens |
· Tetracillin-clavulanate 3.1 g/6h IV · Piperacillin-tazobactum 4.375 g/6h or 4.5 g/8h IV · Imipenem-cilastatin 500 mg/6h IV · Meropenem 1 g/8h IV · Ertapenem 1 g/24h IV |
|
Combination regimen |
· Ceftriaxone 1 g/24h + metronidazole 500 mg/8h IV · Ciprofloxacin 400 mg IV/12 h or 750 mg po/12 h + metronidazole 500 mg/8h IV · Levofloxacin 750 mg IV/24h + metronidazole 500 mg/8h IV · Ampicillin-salbactum 4 g/6 h + gentamicin or tobramycin 5 mg/kg/24h IV |
Table (4): Surgery of Axilla or Perineum.
|
· metronidazole 500 mg/8h IV + Ciprofloxacin 400 mg IV/12 h or 750 mg po/12 h · Levofloxacin 750 mg/24h IV po Ceftriaxone 1 g/24h
|
- References
1. Edelsberg J; Taneja C; Zervos M et al. Trends in US hospital admissions for skin and soft tissue infections Emerg Infect Dis 2009;15:1516-18.
2. 2. Pallin DJ; Egan DJ; Pelletier AJ; Espinola JA; Hooper DC; and Camargo CA Jr . Increased US emergency department visits for skin and soft tissue infections, and changes in antibiotic choices, during the emergence of community-associated methicillin-resistant Staphylococcus aureus. Ann Emerg Med 2008;51 ;291-8.
3. Stevens AL; Bisno AL; Dellinger EP et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 Update by the Infectious Diseases Society of America, Clinical infectious diseases, Vol.59, Issue 2, 15 July 2014, P. e10- e52,https;//doi.org/10,1093/cid/ciu296.